
Abstract
Objective
Neuropsychiatric symptoms (NPS) are prevalent in neurodegenerative disorders, however, their frequency and impact on function across different disorders is not well understood. We compared the frequency and severity of NPS across Alzheimer's disease (AD) (either with mild cognitive impairment or dementia), Cerebrovascular disease (CVD), Parkinson's disease (PD), frontotemporal dementia (FTD), and amyotrophic lateral sclerosis (ALS), and explored the association between NPS burden and function.
Methods
We obtained data from Ontario Neurodegenerative Disease Research Initiative (ONDRI) that included following cohorts: AD (N = 111), CVD (N = 148), PD (N = 136), FTD (N = 50) and ALS (N = 36). We compared the frequency and severity of individual NPS (assessed by the neuropsychiatric inventory questionnaire) across cohorts using generalized estimating equations and analysis of variance. Second, we assessed the relationship of NPS burden with instrumental (iADLs) and basic (ADLs) activities of living across cohorts using multivariate linear regression while adjusting for relevant demographic and clinical covariates.
Results
Frequency of NPS varied across cohorts (χ2(4) = 34.4, p < .001), with post-hoc tests showing that FTD had the greatest frequency as compared to all other cohorts. The FTD cohort also had the greatest severity of NPS (H(4) = 34.5, p < .001). Further, there were differences among cohorts in terms of the association between NPS burden and ADLs (F(4,461) = 3.1, p = 0.02). Post-hoc comparisons suggested that this finding was driven by the FTD group, however, the differences did not remain significant following Bonferroni correction. There were no differences among cohorts in terms of the association between NPS burden and IADLs.
Conclusions
NPS frequency and severity are markedly greater in FTD as compared to other neurodegenerative diseases. Further, NPS burden appears to be associated differently with function across neurodegenerative disorders, highlighting the need for individualized clinical interventions.
Introduction
Neuropsychiatric symptoms (NPS) constitute a major challenge for patients with Alzheimer's disease (AD), cerebrovascular disease (CVD), Parkinson's disease (PD), frontotemporal dementia (FTD), and amyotrophic lateral sclerosis (ALS).1,5 NPS commonly include apathy, depression, anxiety, irritability, agitation, aggression, delusions, hallucinations, as well as sleep and appetite disturbances.1,5 NPS occur almost invariably at some point during the course of neurodegenerative illness. Among patients with dementia, the 5-year period prevalence of at least one symptom has been estimated to be up to 97%, with the most common being depression, anxiety, and apathy. 6 Moreover, the presence of these symptoms has been associated with accelerated disease progression, reduced quality of life, and greater disability.1,7
Interestingly, the prevalence of particular neuropsychiatric symptoms differs between specific neurodegenerative disease cohorts.2,8,9 Varied symptom presentations across cohorts also pose a significant challenge in the evaluation and management of NPS, as treatment needs to be individualized. 10 Importantly, NPS has been associated with cognitive impairment, with a higher symptom burden predictive of poorer cognitive function.11,12 Specifically, depression and sleep disturbances in AD, while delusions and abnormal eating behaviours in FTD, were negatively associated with cognition. 12 Moreover, NPS in patients with AD and CVD have been associated with impairments in activities of daily living (ADLs).8,13,14 However, most studies lack participant stratification into specific neurodegenerative disease cohorts. 13 Thus, data assessing NPS and their association with function across diverse, well-defined neurodegenerative disease cohorts is needed to better understand this relationship. 15
The primary objective of this study was to compare the burden of NPS among AD, CVD, PD, FTD, and ALS cohorts. We hypothesized that these groups will have distinct NPS frequency and severity. We further aimed to explore the association between NPS and function in each cohort while adjusting for demographic and other clinical factors.
Methods
Data used in this study are from Phase 1 of the Ontario Neurodegenerative Disease Research Initiative (ONDRI) – a longitudinal observational cohort study addressing the phenotypic sequelae of degenerative cognitive impairment. The sample included participants with AD (mild cognitive impairment (MCI) or dementia due to AD), CVD, PD, FTD, or ALS. Detailed inclusion/exclusion criteria of ONDRI participants were reported previously.16,17 For MCI, participants with MCI only due to AD were included and they met the National Institute on Aging-Alzheimer's Association (NIA-AA) core clinical criteria for amnestic single or multiple domain mild cognitive impairment. 18 Other causes of cognitive impairment were ruled out by standardized work up, including brain imaging. 16 All participants underwent comprehensive evaluations to assess cognition, function, and neuropsychiatric symptoms. Of the enrolled participants, only those providing neuropsychiatric symptom score, and one of either basic or instrumental activities of daily living score described below were included in analyses.
Neuropsychiatric Symptoms and Cognition
The neuropsychiatric inventory questionnaire (NPI-Q) was used to assess neuropsychiatric symptoms. 19 Study partners of participants reported on the presence and severity of 12 neuropsychiatric symptoms including delusions, hallucinations, agitation/aggression, depression/dysphoria, anxiety, elation/euphoria, apathy/indifference, disinhibition, irritability/lability, motor disturbances, nighttime behaviours, and appetite/eating. Total scores for symptom severity (maximum of 36) and partner distress (maximum of 60) were computed by adding the individual symptom scores. 20 Montreal cognitive assessment (MoCA) was used to assess cognition. 21
Function
Lawton–Brody instrumental activities of daily living (iADL) scale was used to measure participants’ ability to function independently on instrumental activities of daily living. Study partners rated the participants’ ability across eight iADL tasks, ranging from totally independent to totally dependent, including telephone use, shopping, food preparation, housekeeping, laundering, use of transportation, managing medications, and financial management, for a maximum possible total score of 23. 22 In the event that a given participant did not engage in an activity pre-morbidly, the activity's score was deducted from that participant's total possible score (maximum of 23). This produced a modified total score for each participant, by which each participant's score was divided to compute an iADL percent score.
The physical self-maintenance scale was used to measure participants’ ability to function independently on basic activities of daily living (ADLs). Study partners rated the participants’ ability to function independently across six basic ADLs: feeding, dressing, grooming, ambulation, bathing, and toileting, for a maximum possible total score of 24. 23 ADL percent scores were computed for each participant by dividing their total score by 24.
Motor Function
The ALS functional rating scale-revised (ALSFRS-R) was used in the ALS cohort, 24 and the Unified Parkinson's Disease Rating Scale (MDS-UPDRS, part III) was used in the PD cohort to assess motor symptoms. 25
Statistical Analyses
Statistical analyses were performed using SPSS (IBM Corp, SPSS v25). Chi-square or Fisher's exact test (expected cell count less than five) were used to compare categorical measures among cohorts. Standardized residuals (z scores) were evaluated for significant outcomes. For all continuous outcomes, means and standard deviations were computed, normality was assessed using the Shapiro–Wilk test and by visual inspection of data histograms and quantile–quantile plots. Generalized estimating equations (GEE) were used to compare NPS frequency among cohorts, by evaluating binary outcomes (presence of individual NPI-Q symptoms) for individuals within each cohort while accounting for correlation of multiple symptoms measure from the same individual. The GEE covariance structure was specified as “unstructured” as the structure of the within-subject covariance was unknown. One-way analysis of variance (ANOVA) was used to compare NPS severity among cohorts. As applicable, Kruskal–Wallis test was used for non-normally distributed continuous data. Post hoc analyses were completed using Bonferroni testing. To investigate the relationships among NPI-Q total score, MoCA and ADL/iADL scores, correlations were computed using Pearson's or Spearman's correlation coefficient as appropriate, first across combined patient cohorts and further within each cohort. To explore whether the dependence of ADL and iADL percent scores on NPI-Q differed between cohorts, we carried out multivariable linear regression with ADL or iADL score as the dependent variable, NPI-Q and cohort membership as the independent variables with an interaction term, and with age, education, and MoCA as additional independent variables. Subsequently, to explore the association between NPS and function within each cohort, independent of demographic variables and cognition, linear regression was performed with total ADL or iADL percent scores as the dependent variables and NPI-Q total score, age, education, and MoCA scores as the independent variables. AD cohort participants were divided into two groups (MCI or dementia) and analyzed according to diagnosis at the time of study initiation. ALSFRS-R and MDS-UPDRS were included as covariates to control for motor disease burden in ALS and PD cohorts. Bootstrapping using 1,000 samples was performed with all linear regressions to improve interpretability independent of distribution assumptions. Only participants with complete data across measures of interest were included in regressions. Statistical significance was set at α = 0.05.
Results
ONDRI participant cohorts included AD (n = 126), CVD (n = 161), PD (n = 140), FTD (n = 53), and ALS (n = 40). In the AD cohort, 85 (67.4%) participants were diagnosed with MCI while 41 (32.5%) were diagnosed with dementia. In the FTD cohort, 22 (41.5%) were diagnosed with
Of the total sample, 111 (88%) of AD participants, 148 (92%) of CVD participants, 136 (97%) of PD participants, 50 (94%) of FTD participants, and 37 (93%) of ALS participants provided sufficient data for inclusion in this study. Of the 38 excluded participants, 36 were missing NPI-Q scores, and two were missing functional outcomes measures (both basic and instrumental activities of daily living). Of the missing data, three participants (7.8%) had missing data due to verbal refusal to provide data. The remainder of the missing data was for unspecified reasons (i.e., not related to an administrative error, technical challenges, or otherwise). The demographics for included participants are presented in Table 1.
Baseline Clinical and Demographic Characteristics of Participants in Each Cohort (AD, ALS, FTD, PD, and CVD).
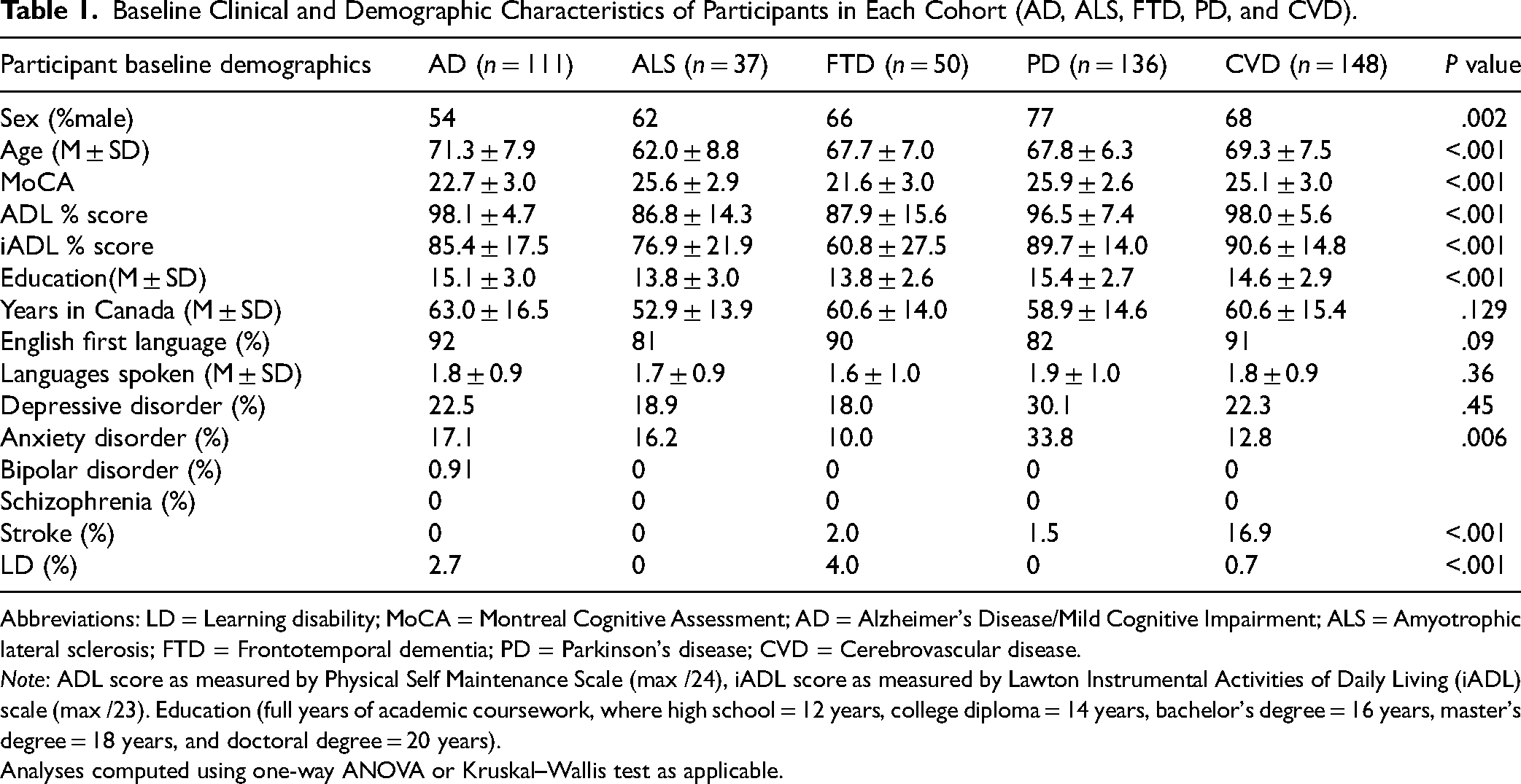
Abbreviations: LD = Learning disability; MoCA = Montreal Cognitive Assessment; AD = Alzheimer's Disease/Mild Cognitive Impairment; ALS = Amyotrophic lateral sclerosis; FTD = Frontotemporal dementia; PD = Parkinson's disease; CVD = Cerebrovascular disease.
Note: ADL score as measured by Physical Self Maintenance Scale (max /24), iADL score as measured by Lawton Instrumental Activities of Daily Living (iADL) scale (max /23). Education (full years of academic coursework, where high school = 12 years, college diploma = 14 years, bachelor's degree = 16 years, master's degree = 18 years, and doctoral degree = 20 years).
Analyses computed using one-way ANOVA or Kruskal–Wallis test as applicable.
Neuropsychiatric Symptoms
There were significant differences in the NPS frequency among cohorts (χ2(4) = 34.4, p < .001). Post-hoc, Bonferroni-corrected, pairwise analyses demonstrated that the symptom profile among the FTD cohort differed significantly when compared to AD (χ2 = 18.1, p < .001), ALS (χ2 = 12.7, p < .001), CVD (χ2 = 17.4, p < .001), and PD (χ2 = 33.8, p < .001) cohorts. Frequencies of individual NPS for each cohort and their comparison across cohorts are shown in Table 2.
Percentage of Participants in Each Cohort (AD, ALS, FTD, PD, and CVD) Showing Symptoms (Mild, Moderate, or Severe) Evaluated on the NPI-Q.

*P values derived from chi-squared tests.
Abbreviations: NPI-Q = Neuropsychiatric Inventory Questionnaire; AD = Alzheimer's Disease/Mild Cognitive Impairment; ALS = Amyotrophic lateral sclerosis; FTD = Frontotemporal dementia; PD = Parkinson's disease; CVD = Cerebrovascular disease.
Participants with FTD suffered from the greatest frequency of aggression, anxiety, apathy, disinhibition, irritability, euphoria, appetite changes, and motor disturbances. FTD and PD participants showed the greatest frequency of abnormal night-time behaviours. Notably, there were no significant differences among cohorts with respect to the frequency of depression, hallucinations, or delusions. Further details, with included participant counts, are provided in Supplementary Table 1. Participants in the FTD cohort also experienced the greatest overall NPS severity (mean (SD) NPI-Q severity score, AD = 3.7 (4.0), ALS = 3.1 (3.7), FTD = 8.2 (6.2), PD = 3.5 (3.9), CVD = 3.1 (3.9); H(4) = 34.5, p < .001). Further, partners of participants with FTD reported the greatest degree of overall partner distress (mean (SD) NPI-Q distress score, AD = 4.12 (5.0), ALS = 3.7 (5.3), FTD = 9.1 (9.1), PD = 4.1 (5.7); CVD = 3.5 (5.2), H(4) = 21.0, p < .001).
Function
For iADL function, 113 (90%) of AD participants, 40 (100%) of ALS participants, 51 (96%) of FTD participants, 133 (95%) of PD participants, and 149 (93%) of CVD participants were included. There were significant differences among the cohorts on iADL percent scores (mean percent (SD) scores AD = 85.3 (17), ALS = 78.3 (22), FTD = 61.5 (28), PD = 89.7 (14), CVD = 90.8 (14.7); H(4) = 69.4, p < .001). Post-hoc pairwise comparisons revealed that participants with FTD exhibited greater impairment in iADL scores compared to all cohorts other than ALS (p < .001 for all pairwise comparisons).
For ADL function, 115 (91%) of AD participants, 39 (98%) of ALS participants, 52 (98%) of FTD participants, 137 (98%) of PD participants, and 152 (94%) of CVD participants were included. There were significant differences among the cohorts on ADL scores (mean percent (SD) scores, AD = 98.2 (4.6), ALS = 87.5 (14), FTD = 87.8 (16), PD = 96.5(7.3), CVD = 98.1(6), H(4) = 94.8, p < .001). Post-hoc pairwise comparisons revealed that ALS and FTD cohorts had significantly greater impairment in ADL scores compared to all other cohorts (p < .001 for all pairwise comparisons among both groups).
Relationship between NPS and Function
Across combined participant samples, NPI-Q demonstrated significant negative correlation with MoCA scores (rs = −0.15, p = .001). NPI-Q scores were also negatively correlated with iADL percent scores in AD (rs = −0.45, p < .001), ALS (rs = −0.52, p = .001), FTD (rs = −0.51, p < .001), PD (rs = −0.38, p < .001), and CVD participants (rs = −0.24, p < .01). Further, NPI-Q total score was negatively correlated with ADL percent scores in AD (rs = −.32, p = .001), FTD (rs = −0.35, p = .01), PD (rs = −0.39, p < .001), and CVD (rs = −0.26, p = .002) participants. Among ALS participants, there was no significant correlation between NPI-Q and ADL percent score. Summary correlation data and number of included participants from each cohort are presented in Table 3.
Correlation Matrix Between NPI-Q Total Score with Functional Performance and MoCA Scores Across Cohorts.

*Note: Significant after Bonferonni correctin.
ADL score as measured by Physical Self Maintenance Scale (max /24), iADL score as measured by Lawton Instrumental Activities of Daily Living (iADL) scale (max /23).
Abbreviations: NPI-Q = Neuropsychiatric Inventory Questionnaire; AD = Alzheimer's Disease/Mild Cognitive Impairment; ALS = Amyotrophic lateral sclerosis; FTD = Frontotemporal dementia; PD = Parkinson's disease; CVD = Cerebrovascular disease.
With respect to the dependence of iADL on NPI-Q across cohorts, multivariable linear regression did not reveal statistically significant differences (F(4,456) = 1.59, p = 0.18). Full results of cohort-specific linear regression are presented in Supplementary Tables 2 and 3. Partial plots of NPI-Q residuals against iADL percent scores are shown in Figure 1. In the AD cohort, NPI-Q MoCA, and age contributed to the model (F(4,103) = 15.8, R2 = .36, p < .001). Within the AD cohort, in participants with MCI, MoCA, and age contributed (F(4,64) = 6.80, R2 = .25, p < .001), while in participants with dementia, NPI-Q alone contributed to the model (F(4,29) = 4.25, R2 = 0.28, p = .008). In the PD cohort, NPI-Q and age contributed to the model (F(5,126) = 12.2, R2 = .30, p < .001). In the FTD cohort, NPI-Q alone contributed to the model (F(4,45) = 4.3, R2 = .21, p < .01). Similarly, in the CVD cohort, NPI alone contributed to the model (F(4,138) = 2.9, R2 = .05, p = .03). In the ALS cohort, FRS-R scores alone contributed to the model (F(5,30) = 3.0, R2 = 0.22, p = .03).

Partial regression plots with y-axis representing residuals* from regressing iADL percent score against education, age, and moCA and x-axis representing residuals from regressing NPI-Q score against education, age, and MoCA. UPDRS (part 3) residuals are included for the PD cohort. 95% confidence intervals are represented by dotted blue lines and 95% prediction intervals are represented by dotted green lines. The line of best fit shows the strength of the linear relationship between NPI-Q and iADL score among each of the cohorts (AD, FTD, CVD, and PD). *Note. Difference between the observed value of the response variable (iADL score) and the measured value of the response variable predicted from the regression line. iADL score as measured by Lawton instrumental activities of daily living (iADL) scale (max/23). Abbreviations: MoCA = Montreal Cognitive Assessment; NPI-Q = Neuropsychiatric Inventory Questionnaire; FRSR = ALS functional rating scale-revised; UPDRS = Unified Parkinson's Disease Rating Scale; AD = Alzheimer's Disease; ALS = Amyotrophic lateral sclerosis; FTD = Frontotemporal dementia; PD = Parkinson's disease; CVD = Cerebrovascular disease.
With respect to the dependence of ADLs on NPI-Q across cohorts, multivariable linear regression revealed significant differences (F(4,461) = 3.1, p = .02). Post-hoc pairwise comparisons demonstrated significant differences between the FTD, and ALS (t = 2.0, p = .03) and CVD (t = 2.7, p < .01) cohorts. As well, we observed differences between the CVD and PD cohorts (t = −2.5, p = .01). However, these comparisons did not remain significant following Bonferroni adjustment. Cohort-specific regressions for ADL score revealed significant multivariable models among the AD, FTD, and PD cohorts. Partial plots of NPI-Q residuals against ADL percent score are shown in Figure 2. In the AD cohort, both NPI-Q and age contributed to the model (F(4,104) = 4.6, R2 = .12, p = .002). Within the AD cohort, in participants with MCI, NPI-Q alone contributed to the model (F(4,65) = 3.4, R2 = .12, p = .02). Similarly, in the FTD cohort, NPI-Q alone contributed to the model (F(4,45) = 3.1, R2 = .14, p = .026). In the PD cohort, both NPI-Q and UPDRS contributed to the model (F(5,129) = 15.0, R2 = .34, p < .001). In the ALS cohort, FRS-R alone contributed to the model (F(5,29) = 5.6, R2 = 0.40, p = .001).
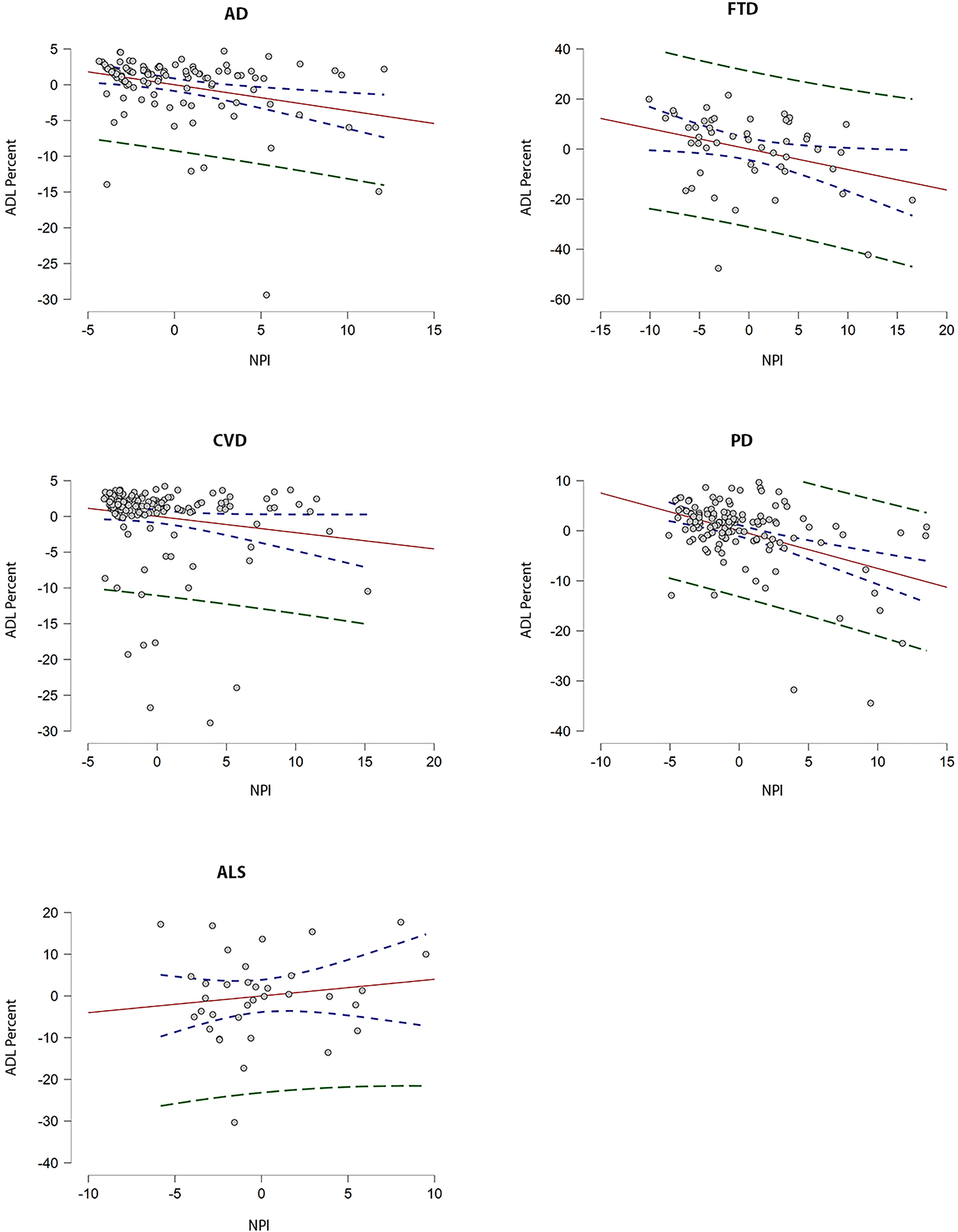
Partial regression plots with y-axis representing residuals* from regressing ADL precent score against education, age, and moCA and x-axis representing residuals from regressing NPI-Q score against education, age, and MoCA. UPDRS (part 3) residuals are included for the PD cohort. 95% confidence intervals are represented by dotted blue lines and 95% prediction intervals represented by dotted green lines. The line of best fit shows the strength of the linear relationship between NPI-Q and ADL score among each of the cohorts (AD, FTD, CVD, and PD). *Note. Difference between the observed value of the response variable (ADL score) and the measured value of the response variable predicted from the regression line. ADL score as measured by Lawton Instrumental Activities of Daily Living (ADL) scale (max/23). Abbreviations: MoCA = Montreal Cognitive Assessment; NPI-Q = Neuropsychiatric Inventory Questionnaire; FRSR = ALS functional rating scale-revised; UPDRS = Unified Parkinson's Disease Rating Scale; AD = Alzheimer's Disease; ALS = Amyotrophic lateral sclerosis; FTD = Frontotemporal dementia; PD = Parkinson's disease; CVD = Cerebrovascular disease.
Discussion
This study conducted a comprehensive evaluation of NPS and their association with function in large, well-defined cohorts of patients across a wide spectrum of neurodegenerative disorders. As hypothesized, we found that the frequency of NPS differed significantly between cohorts, with FTD demonstrating the greatest frequency of NPS. The FTD cohort also had the greatest severity of NPS. Further, there were differences between cohorts in terms of the association between NPS burden and ADLs, and this finding seemed to be largely driven by the FTD cohort. Cohort-stratified analyses revealed a significant association between NPS and activities of living (both basic and instrumental) in AD, FTD, PD, and CVD cohorts. When examined in the presence of covariates (age, education, cognition, and motor function), NPS alone was associated with iADLs in FTD and CVD, whereas NPS, age, and cognition were associated with iADLs in AD. NPS and age were together associated with iADLs in PD. Furthermore, NPS alone were associated with ADLs in FTD and CVD, and together with motor disease burden in PD. Motor disease burden alone was associated with ADLs in ALS. NPS and age were together associated with ADLs in AD.
In line with our work, previous studies have revealed differences in the frequency and severity of NPS among neurodegenerative disease cohorts. In one observational study, participants with FTD had more frequent appetite disturbances, disinhibition, and abnormal motor behaviours as compared to AD and CVD. 26 This finding is consistent with our data, and in addition, we observed higher frequencies of nearly all other NPS in our FTD cohort as compared to other cohorts. Notably, the previous study had a smaller sample size and higher frequency of overall NPS relative to our sample. 26 In another large study, FTD was associated with greater overall NPS burden when compared to AD, CVD, and DLB cohorts. 27 While the authors did not present the frequency of individual NPS within each cohort at baseline, 27 these findings parallel the results observed in our data. Of note, the behavioural variant subtype was disproportionally represented in our FTD cohort, likely accounting for some of these differences, as previously suggested.3,27
Relationship Between NPS and Function
Interestingly, our data suggested that the dependence of ADL scores on NPS differed significantly between cohorts. While pairwise comparisons did not remain significant after correction, these data support the notion that with greater disease burden, as ADLs become affected, the relationship between NPS and function becomes increasingly clinically relevant. The most notable group differences were observed when comparing FTD cohort to ALS and CVD cohorts.
While cohort-level analyses demonstrated associations between NPS with iADL and ADL across all cohorts, this was not observed in the ALS cohort, possibly due to partial confounding by motor disturbance, consistent with previous data. 28 Further, our finding in the AD cohort that NPS, cognition, and age together were associated with iADL score, while NPS alone predicted ADL score, suggests that NPS are more closely linked with functional ability at more advanced stages of illness, when basic ADLs become compromised. Additionally, the association of NPS alone with function for both iADL and ADLs in FTD suggests that NPS are the main drivers of functional impairment in FTD throughout the duration of illness. Among PD participants, motor symptom severity demonstrated a significant relationship with ADL scores, but not with iADL scores, suggesting that motor symptoms play a greater role in functional outcomes as disease burden progresses and basic ADLs become compromised. Taken together, these results highlight the need for developing effective clinical interventions for patients experiencing NPS due to neurodegenerative disorders. These should include improved use of existing non-pharmacological and pharmacological approaches, and development of novel therapeutics to improve care for NPS.1,29,33
Limitations
The present study has several limitations. First, this present study was cross-sectional, and we are thus unable to draw conclusions about longitudinal predictions based on our models. Second, the FTD group included participants with bvFTD, PPA, CBS, and PSP, and stratified analyses by these subtypes was not completed due to limited sample sizes. This should be investigated in future studies with larger cohorts. Third, while our diagnostic assessment for patients included standardized criteria and neuroimaging, assessment of biomarkers was not incorporated. Fourth, patients recruited into the study were those with mild-to-moderate illness, potentially reducing the observed range of functional impairment and NPS severity. Therefore, the generalizability of our findings is limited to patients in early or mid-stages of disease. Fifth, unequal cohort sizes included in our data may have resulted in reduced statistical power.
Conclusion
The present study demonstrates significant differences in the frequency and severity of neuropsychiatric symptoms across neurodegenerative disease cohorts, with the greatest frequency and severity of NPS observed in FTD. Further, NPS burden appears to be associated differently with function across neurodegenerative disorders. These findings elucidate the importance of NPS and their impact on function across the spectrum of neurodegenerative disorders. Considering the irreversibility of cognitive decline, the effective and individualized management of NPS may improve function and other clinical outcomes such as patient and caregiver quality of life. 34
Supplemental Material
sj-pdf-1-cpa-10.1177_07067437221147443 - Supplemental material for Neuropsychiatric Symptom Burden across Neurodegenerative Disorders and its Association with Function
Supplemental material, sj-pdf-1-cpa-10.1177_07067437221147443 for Neuropsychiatric Symptom Burden across Neurodegenerative Disorders and its Association with Function by Daniel Kapustin, Shadi Zarei, Wei Wang, Malcolm A. Binns, Paula M. McLaughlin, Agessandro Abrahao, Sandra E. Black, Michael Borrie, David Breen, Leanna Casaubon, Dar Dowlatshahi, Elizabeth Finger, Corinne E Fischer, Andrew Frank, Morris Freedman, David Grimes, Ayman Hassan, Mandar Jog, Donna Kwan, Anthony Lang, Brian Levine, Jennifer Mandzia, Connie Marras, Mario Masellis, Joseph B. Orange, Stephen Pasternak, Alicia Peltsch, Bruce G. Pollock, Tarek K. Rajji, Angela Roberts, Demetrios Sahlas, Gustavo Saposnik, Dallas Seitz, Christen Shoesmith, Alisia Southwell, Thomas D.L. Steeves, Kelly Sunderland, Richard H Swartz, Brian Tan, David F. Tang-Wai, Maria Carmela Tartaglia, Angela Troyer, John Turnbull, Lorne Zinman, and Sanjeev Kumar in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-2-cpa-10.1177_07067437221147443 - Supplemental material for Neuropsychiatric Symptom Burden across Neurodegenerative Disorders and its Association with Function
Supplemental material, sj-docx-2-cpa-10.1177_07067437221147443 for Neuropsychiatric Symptom Burden across Neurodegenerative Disorders and its Association with Function by Daniel Kapustin, Shadi Zarei, Wei Wang, Malcolm A. Binns, Paula M. McLaughlin, Agessandro Abrahao, Sandra E. Black, Michael Borrie, David Breen, Leanna Casaubon, Dar Dowlatshahi, Elizabeth Finger, Corinne E Fischer, Andrew Frank, Morris Freedman, David Grimes, Ayman Hassan, Mandar Jog, Donna Kwan, Anthony Lang, Brian Levine, Jennifer Mandzia, Connie Marras, Mario Masellis, Joseph B. Orange, Stephen Pasternak, Alicia Peltsch, Bruce G. Pollock, Tarek K. Rajji, Angela Roberts, Demetrios Sahlas, Gustavo Saposnik, Dallas Seitz, Christen Shoesmith, Alisia Southwell, Thomas D.L. Steeves, Kelly Sunderland, Richard H Swartz, Brian Tan, David F. Tang-Wai, Maria Carmela Tartaglia, Angela Troyer, John Turnbull, Lorne Zinman, and Sanjeev Kumar in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-3-cpa-10.1177_07067437221147443 - Supplemental material for Neuropsychiatric Symptom Burden across Neurodegenerative Disorders and its Association with Function
Supplemental material, sj-docx-3-cpa-10.1177_07067437221147443 for Neuropsychiatric Symptom Burden across Neurodegenerative Disorders and its Association with Function by Daniel Kapustin, Shadi Zarei, Wei Wang, Malcolm A. Binns, Paula M. McLaughlin, Agessandro Abrahao, Sandra E. Black, Michael Borrie, David Breen, Leanna Casaubon, Dar Dowlatshahi, Elizabeth Finger, Corinne E Fischer, Andrew Frank, Morris Freedman, David Grimes, Ayman Hassan, Mandar Jog, Donna Kwan, Anthony Lang, Brian Levine, Jennifer Mandzia, Connie Marras, Mario Masellis, Joseph B. Orange, Stephen Pasternak, Alicia Peltsch, Bruce G. Pollock, Tarek K. Rajji, Angela Roberts, Demetrios Sahlas, Gustavo Saposnik, Dallas Seitz, Christen Shoesmith, Alisia Southwell, Thomas D.L. Steeves, Kelly Sunderland, Richard H Swartz, Brian Tan, David F. Tang-Wai, Maria Carmela Tartaglia, Angela Troyer, John Turnbull, Lorne Zinman, and Sanjeev Kumar in The Canadian Journal of Psychiatry
Footnotes
Author Contributions
S.K. has received research support the Brain and Behavior Foundation, US National institute on Aging, BrightFocus Foundation, Brain Canada, Canadian Institutes of Health Research, Canadian Consortium on Neurodegeneration in Aging, Centre for Ageing and Brain Health Innovation, Centre for Addiction and Mental Health, and an Academic Scholars Award from the Department of Psychiatry, Temerty Faculty of Medicine, University of Toronto. He has also received equipment support from Soterix Medical. B.P. holds and receives support from the Peter and Shelagh Godsoe Endowed Chair in Late-Life Mental Health, Centre for Addiction and Mental Health. Dr. Pollock's research is supported by the National Institute of Aging, Brain Canada, the Canadian Institutes of Health Research, the Alzheimer's Drug Discovery Foundation, the Ontario Brain Institute, the Centre for Aging and Brain Health Innovation, Alzheimer's Society of Canada, the W. Garfield Weston Foundation, the Weston Brain Institute, the Canadian Consortium on Neurodegeneration in Aging and Genome Canada. B.P. receives honoraria from the American Geriatrics Society and holds United States Provisional Patent No. 16/490,680 and Canadian Provisional Patent No. 3,054,093 for a cell-based assay and kits for assessing serum anticholinergic activity. T.R has received research support from Brain Canada, Brain and Behavior Research Foundation, BrightFocus Foundation, Canada Foundation for Innovation, Canada Research Chair, Canadian Institutes of Health Research, Centre for Aging and Brain Health Innovation, National Institutes of Health, Ontario Ministry of Health and Long-Term Care, Ontario Ministry of Research and Innovation, and the Weston Brain Institute. He also received in-kind equipment support for an investigator-initiated study from Magstim, and in-kind research accounts from Scientific Brain Training Pro. He participated in 2021 in an advisory board for Biogen Canada Inc. E.F. has received personal compensation for serving on a PSP scientific advisory board for Biogen, for serving as a section editor for NeuroImage Clinical, and for serving as a course director for the AAN annual meeting. M.F. is listed on a patent related to methods and kits for differential diagnosis of Alzheimer disease vs frontotemporal dementia using blood biomarkers. D.G. reports honorariums from Sunovion and Paladin Labs Inc. as well as clinical trials with CIHR, Genzyme Corporation/Sanofi Canada, and Eli Lilly and Company. A.E.L. reports consultancy support from Abbvie, Acorda, AFFiRis, Biogen, Denali, Janssen, Intracellular, Kallyope, Lundbeck, Paladin, Retrophin, Roche, Sun Pharma, Theravance, and Corticobasal Degeneration Solutions; advisory board support form Jazz Pharma, PhotoPharmics, Sunovion; other honoraria from Sun Pharma, AbbVie, Sunovion, American Academy of Neurology and the International Parkinson and Movement Disorder Society; grants from Brain Canada, Canadian Institutes of Health Research, Corticobasal Degeneration Solutions, Edmond J Safra Philanthropic Foundation, Michael J. Fox Foundation, the Ontario Brain Institute, Parkinson Foundation, Parkinson Canada, and W. Garfield Weston Foundation and royalties from Elsevier, Saunders, Wiley-Blackwell, Johns Hopkins Press, and Cambridge University Press. M.M. receives salary support from the Department of Medicine at Sunnybrook Health Sciences Centre, the University of Toronto, and the Sunnybrook Research Institute, as well as advisory board support from Arkuda Therapeutics, Ionis Pharmaceuticals, Alector and Wave Life Sciences; royalties from Henry Stewart Talks Ltd; grants paid to institution from Weston Brain Institute, Ontario Brain Institute, Washington University and Canadian Institutes of Health Research outside the submitted work; and clinical trials support from Roche and Alector. G.S. is the Editor-in-Chief of the World Stroke Academy for the World Stroke Organization and receives CME honorarium from Servier and Roche, as well as grants from Roche. M.C.T. receives consultancy support from Biogen and Hoffman-La Roche and is a board member of Alzheimer's Society of Toronto. SS is the Chief Scientific Officer of ADMdx, a medical diagnostics company specializing in neuroimaging of neurodegenerative disorders. M.F. received support from the Saul A. Silverman Family Foundation as a Canada International Scientific Exchange Program (MF), and Morris Kerzner Memorial Fund. M.F. is listed on a patent related to methods and kits for differential diagnosis of Alzheimer disease vs frontotemporal dementia using blood biomarkers. The remaining authors declare no competing interests. CEF has grant funding from Hoffman La Roche, Vielight Inc, Cortexyme, the Weston Foundation, Brian Canada and NIH. MB has received research support from CIHR/CCNA, NIH/ADNI. MB has been principal investigator for pharma-sponsored clinical trials, with contract funding paid to Lawson Research Institute, from Pfizer, Genentech, Alector, Transtech, Forum, Abbvie and Eisai. He has received honoraria for participating in scientific boards and for continuing medical education paid by Pfizer, Janssen, Novartis, Merck, Roche, Lundbeck, Eli Lily, and Biogen.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was conducted with support from the Ontario Neurodegenerative Disease Research Initiative through the Ontario Brain Institute, an independent non-profit corporation, funded partially by the Ontario government. The opinions, results and conclusions are those of the authors and no endorsement by the Ontario Brain Institute is intended or should be inferred. Matching funds provided by participating hospital and research institute foundations, including the Baycrest Foundation, Bruyère Research Institute, Centre for Addiction and Mental Health Foundation, London Health Sciences Foundation, McMaster University Faculty of Health Sciences, Ottawa Brain and Mind Research Institute, Queen's University Faculty of Health Sciences, Providence Care (Kingston), Sunnybrook Health Sciences Foundation, St. Michael's Hospital, the Thunder Bay Regional Health Sciences Centre, the University of Ottawa Faculty of Medicine, and the Windsor/Essex County ALS Association. This study was also funded in part by an Academic Scholars Award from the Department of Psychiatry, Temerty Faculty of Medicine, University of Toronto to SK.
Ethics Statement
All participating institutions obtained ethics approval and informed consent was obtained from all participants before carrying out any study procedures. Ethics approval was obtained from the Toronto Academic Health Sciences Network (TAHSN) and the Research Ethics Board of Sunnybrook Health Sciences Centre (Project ID 013-2014).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.