
Abstract
Objective
This study identified patient clinical and sociodemographic characteristics, and, more originally, service use patterns as predictors of death from physical illness or accidental/intentional causes.
Methods
A cohort of 19,015 patients with substance-related disorders (SRD) from 14 addiction treatment centers was investigated using Quebec (Canada) health administrative databases. Death was studied over a 3-year period (April 1, 2013, to March 31, 2016), and most predictors from 4 years to 12 months prior to the time of death, using multinomial logistic regression.
Results
Frequent emergency department (ED) use strongly predicted both causes of death, suggesting that outpatient care responded inadequately to patient needs. Only receipt of specialized SRD and psychiatric care significantly decreased the risk of death from physical illness, with trends toward significance for accidental/intentional death. Hospitalization, greater material deprivation and having SRD-chronic physical illnesses or alcohol-related disorders most strongly predicted risk of death from physical illness. Sociodemographic characteristics, mainly social deprivation, were more likely to predict accidental/intentional death.
Conclusions
Outpatient services could be improved by increasing outreach and motivational interventions and, for ED and hospital units, better screening, brief intervention, and referral to treatment, particularly for men and socially deprived patients at high risk of accidental/intentional death. Patients with more severe health conditions, notably older or materially deprived men at higher risk of death from physical illness, could benefit from programs like assertive community treatment or intensive case management that respond well to diverse and continuous patient needs. Collaborative care between SRD and health services could also be improved.
Introduction
Substance-related disorders (SRD) are the main cause of death worldwide.1,2 Estimates of potential life lost were 21.6 years for individuals with SRD and 23.2 years for those with cooccurring SRD-mental disorders (MD) in a 2010 to 2017 US study, 3 and 24 to 28 years for individuals with alcohol-related disorders in a 1987 to 2006 study conducted in Nordic countries. 4 European patients treated for SRD in 2012−2013 had a 10 to 20 times higher risk of death than the general population, controlling for age and sex. 5 Patients treated for opioids, cocaine, cannabis, or alcohol-related disorders were identified as having a much greater risk of death, that is, 15 to 20,5,6 six, 7 five, 8 and four times higher, respectively, 9 compared to patients without SRD. SRD also increased the risks for chronic physical illnesses, including cancer, cardiovascular or respiratory diseases, and HIV/AIDS. 5 A 2014 systematic review and meta-analysis found that patients with alcohol-related disorders had a 10 times greater risk of dying from cirrhosis of the liver and twice the risk for cancer or cardiovascular diseases than the general population. 10 SRD also increased the risk of accidental death (e.g., car accidents and drowning) or intentional death (e.g., suicide and self-harm). 5 Death by suicide is reportedly high among patients with SRD.11,12 Despite their elevated risk of premature death, most patients with SRD (fewer than 20% in the US 13 ) lacked access to specialized treatment.9,14
Several studies have assessed death among patients with SRD over a period ranging from 215-17 to 42 years. 18 Most focused on specific substances, mainly opioids,15,19-21 but also alcohol, 10 cocaine, 22 and cannabis-related disorders. 8 These studies investigated death from any cause16,19,23 or by overdose/intoxication15,17,24 or suicide,25-27 whereas few assessed death due to overdose/intoxication versus physical illness.15,18 Previous hospitalization was associated with both death from any cause 19 and overdose/intoxication more specifically, 24 while having chronic physical illnesses 23 and older age 15 increased the overall risk of death from physical illness. Having polysubstance-related disorders17,18 was associated with death by overdose/intoxication and physical illness. The number of years with SRD 23 related to death overall, whereas younger age related to death by overdose/intoxication 18 and suicide. 25 Living alone, 24 injection drug use, 24 previous nonfatal overdose, 17 and co-occurring SRD-MD 18 were mainly associated with death by overdose/intoxication, whereas retention in SRD treatment 21 decreased this risk. Disrupted relationships, unemployment, childhood abuse, previous suicide attempts, 27 chronic alcohol and opioid-related disorders,25,26 and MD 27 were mainly linked to death by suicide.
This study is original as it examines death in a large cohort of patients with SRD who used addiction treatment centers and compares predictors of death from physical illness and accidental/intentional death. In Quebec, addiction treatment centers serve roughly 10% of the population with SRD, 28 representing highly vulnerable patients. Particular attention was given to patient service use patterns up to the time of death, as service use has rarely been explored as a predictor of death. Considering that adverse outcomes vary over time and according to SRD, we hypothesized that death from physical illness would be more strongly predicted by severe health conditions among patients than accidental/intentional death. We also hypothesized that more adequate outpatient service use would protect against both deaths from physical illness and accidental/intentional causes. This study thus aimed to identify patient clinical and sociodemographic characteristics, and their service use patterns predicting death from physical illness or accidental/intentional death, compared to patients with SRD who did not die during the study period. More comprehensive identification of predictors of death from physical illness versus accidental/intentional death could help strengthen targeted interventions to reduce the overall risk of death among patients with SRD.
Methods
Study Context
Quebec addiction treatment centers are specialized regional organizations offering SRD programs like detoxification, substitution treatment and rehabilitation, including brief intervention units, accessible through self-referral, referral from primary care or court order. Addiction treatment centers are complementary to primary care provided by general practitioners (GP), most of whom work in family medicine groups, or by psychosocial teams operating in community healthcare centers. Family medicine groups include psychosocial staff (e.g., social workers), require patient registration and provide extended medical coverage, aiming to ensure continuity of patient care.
Study Sample, Sources, and Design
Data were collected in the financial year 2012–2013 (April 1−March 31) for a cohort of 19,099 patients who used one of 14 (out of 16) Quebec addiction treatment centers. Patients had to be Quebec residents, 12 + years old, registered in the addiction treatment center database (SIC-SRD), and eligible for the Quebec Health Insurance Plan (Régie de l’assurance maladie du Québec, RAMQ) between 1996−1997 and 2015−2016. Patients were excluded if they died during 2012−2013, or if their cause of death was unknown. Data from SIC-SRD included patient sociodemographic characteristics, type of SRD and services received in these centers. The RAMQ integrated billing systems of physician services, except for 6% of services occurring outside the public system. 29 The RAMQ also included various subdatabases concerning hospitalization, emergency department (ED) use, psychosocial interventions in community healthcare centers and causes of death. Diagnostic codes from RAMQ were framed by the International Classification of Diseases, Ninth and Tenth Revisions (Appendix 1). The SIC-SRD integrated standardized instruments which measured the presence of SRD (yes/no), based on the Addiction Severity Index 30,31 or the Global Appraisal of Individual Needs. 32
Death was measured for a 3-year period, from 2013−2014 to 2015−2016. Predictors of death included patient clinical characteristics measured from 2012−2013 to 2015−2016 or to the time of death, except for the number of years with SRD measured from 1996−1997 to 2015−2016 or to the time of death. Patient sociodemographic characteristics were measured in the year of death and services use 12 months prior to death, except for the variables on criminal history or history of homelessness, measured from 2009–2010 to 2015−2016 or to time of death. For these measures, a case-control design was used: each living patient was allocated an exposure window in the same way as a randomly selected patient of the same age and sex who died between 2013−2014 and 2015−2016. Figure 1, the study framework, identifies all databases linked to each study variable, including their measurement intervals. Data from all the databases were merged yearly, for each patient, through a unique RAMQ identifier matched with the SIC-SRD database (100% data linkage). Access to the databases was granted by the Quebec Commission for Access to Information, and the ethics review board of the Integrated University Health and Social Services Center of the South-Central Island of Montreal approved the study protocol.
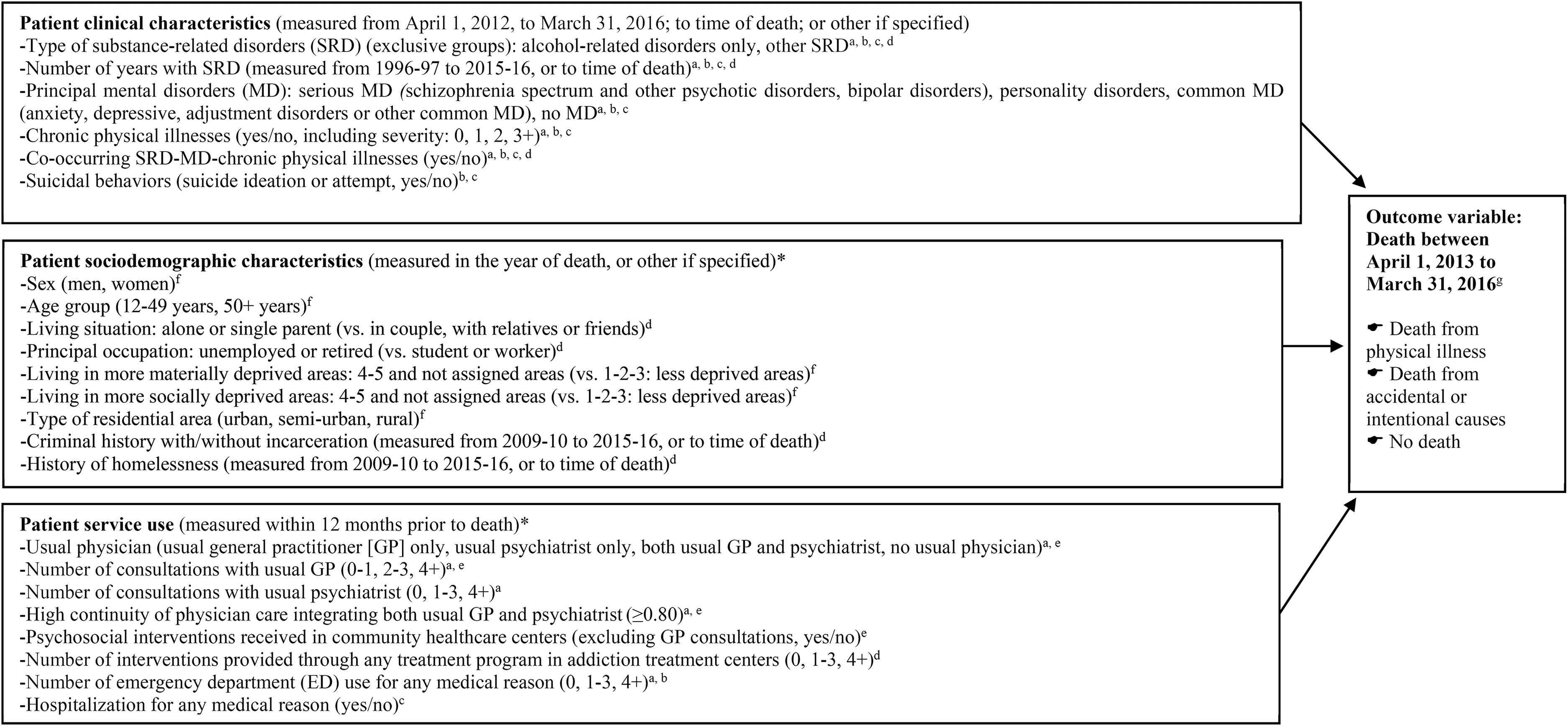
Framework: predictors of death from physical illness or accidental/intentional causes among patients with substance-related disorders.
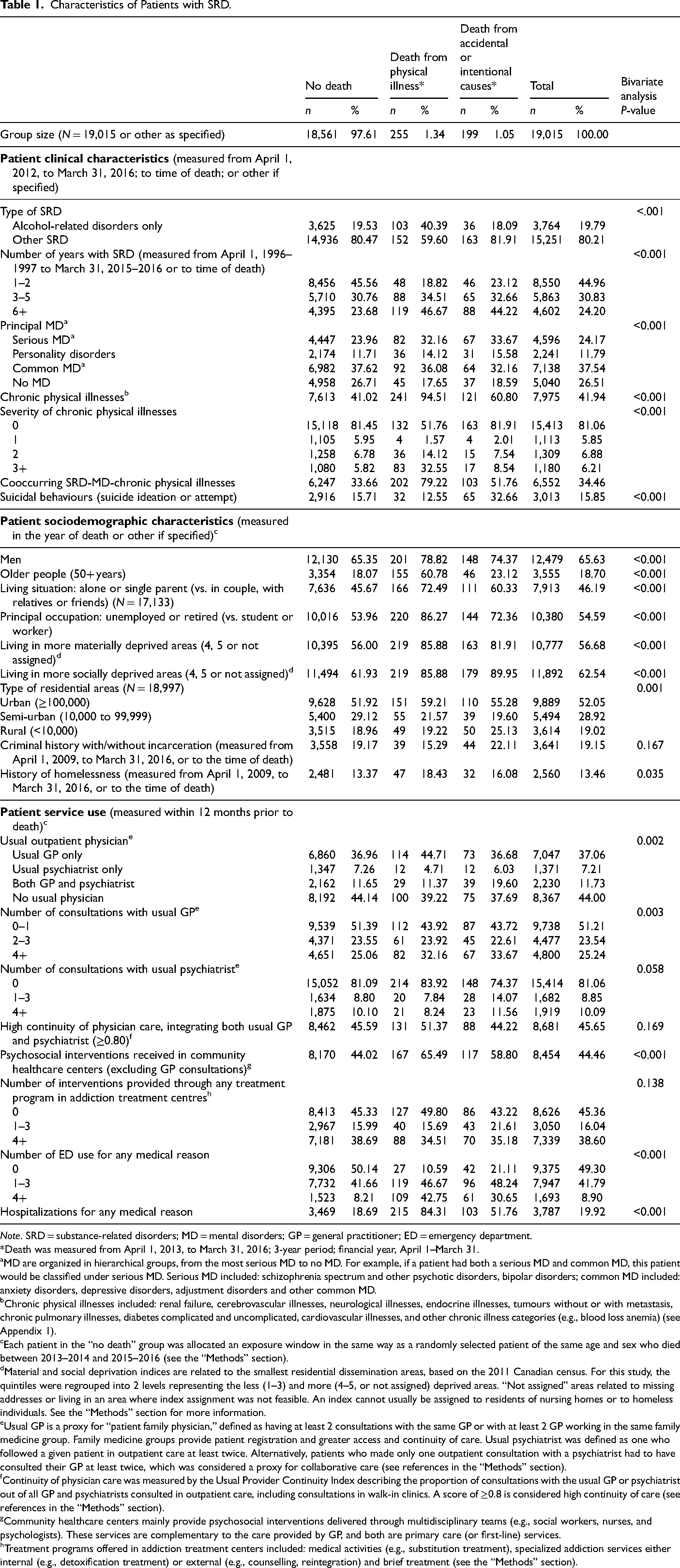
Characteristics of Patients with SRD.
Note. SRD = substance-related disorders; MD = mental disorders; GP = general practitioner; ED = emergency department.
*Death was measured from April 1, 2013, to March 31, 2016; 3-year period; financial year, April 1–March 31.
MD are organized in hierarchical groups, from the most serious MD to no MD. For example, if a patient had both a serious MD and common MD, this patient would be classified under serious MD. Serious MD included: schizophrenia spectrum and other psychotic disorders, bipolar disorders; common MD included: anxiety disorders, depressive disorders, adjustment disorders and other common MD.
Chronic physical illnesses included: renal failure, cerebrovascular illnesses, neurological illnesses, endocrine illnesses, tumours without or with metastasis, chronic pulmonary illnesses, diabetes complicated and uncomplicated, cardiovascular illnesses, and other chronic illness categories (e.g., blood loss anemia) (see Appendix 1).
Each patient in the “no death” group was allocated an exposure window in the same way as a randomly selected patient of the same age and sex who died between 2013–2014 and 2015–2016 (see the “Methods” section).
Material and social deprivation indices are related to the smallest residential dissemination areas, based on the 2011 Canadian census. For this study, the quintiles were regrouped into 2 levels representing the less (1–3) and more (4–5, or not assigned) deprived areas. “Not assigned” areas related to missing addresses or living in an area where index assignment was not feasible. An index cannot usually be assigned to residents of nursing homes or to homeless individuals. See the “Methods” section for more information.
Usual GP is a proxy for “patient family physician,” defined as having at least 2 consultations with the same GP or with at least 2 GP working in the same family medicine group. Family medicine groups provide patient registration and greater access and continuity of care. Usual psychiatrist was defined as one who followed a given patient in outpatient care at least twice. Alternatively, patients who made only one outpatient consultation with a psychiatrist had to have consulted their GP at least twice, which was considered a proxy for collaborative care (see references in the “Methods” section).
Continuity of physician care was measured by the Usual Provider Continuity Index describing the proportion of consultations with the usual GP or psychiatrist out of all GP and psychiatrists consulted in outpatient care, including consultations in walk-in clinics. A score of ≥0.8 is considered high continuity of care (see references in the “Methods” section).
Community healthcare centers mainly provide psychosocial interventions delivered through multidisciplinary teams (e.g., social workers, nurses, and psychologists). These services are complementary to the care provided by GP, and both are primary care (or first-line) services.
Treatment programs offered in addiction treatment centers included: medical activities (e.g., substitution treatment), specialized addiction services either internal (e.g., detoxification treatment) or external (e.g., counselling, reintegration) and brief treatment (see the “Methods” section).
Variables
Three groups were compared on the outcome variable: death from physical illness (e.g., cancer and cardiovascular diseases), accidental death (e.g., motor vehicle accident and falls) or intentional death (e.g., self-harm and suicide—see Appendix 1), and “no death” used as the reference group. Patient clinical characteristics included type of SRD, number of years with SRD, principal MD, chronic physical illnesses (yes/no; severity), cooccurring SRD-MD-chronic physical illnesses, and suicidal behaviours (suicide ideation and attempt). SRD referred to alcohol and drug use disorders, intoxication, induced disorders, and withdrawal. Type of SRD included alcohol-related disorders only, and other SRD. Alcohol-related disorders only were distinguished from other SRD, as being the most prevalent substance in the US 33 and often used without drugs. 34 Principal MD included serious MD (schizophrenia spectrum and other psychotic disorders, bipolar disorders), personality disorders, and common MD (e.g., anxiety and depressive disorders). Chronic physical illnesses, based on an adapted version of the integrated Elixhauser and Charlson Comorbidity Indexes, 35 comprised the number and level of illness severity per patient from 0 to 3+.
Patient sociodemographic characteristics encompassed sex, age group (˂50, 50+ years), living situation (e.g., alone or single parent), principal occupation (e.g., student or worker), material and social deprivation, type of residential area (e.g., urban), criminal history, and history of homelessness. The 50-year threshold was determined based on an adult's developmental perspective, where middle-aged adulthood (50 to 64 years old) usually begins.36,37 This period also coincides with menopause in women, and a higher prevalence of chronic illnesses, especially cardiovascular illnesses.38,39 The Material Deprivation Index, based on the smallest dissemination areas established for the 2011 Canadian census, integrated ratios of population employment, average income, and education levels lower than high school, while the Social Deprivation Index included proportions of patients living alone, those whose civil status is “single,” and single-parent families. 40 Both indexes were classified in quintiles but were regrouped for this study as less deprived (1 to 3) and more deprived (4 to 5 and not assigned—e.g., homelessness) areas.
Patient service use variables included usual outpatient physician (usual GP or psychiatrist only, both usual GP and psychiatrist), number of consultations with usual GP or psychiatrist, high continuity of physician care, psychosocial interventions received in community healthcare centers, number of interventions provided for any SRD in addiction treatment centers, frequent ED use and hospitalization for any medical reason. Usual GP, a proxy for family doctor, was defined as having at least 2 consultations with the same GP working in a private clinic or community healthcare center, or with at least 2 GP working in the same family medicine group. Usual psychiatrist was defined as one who followed a patient in outpatient care at least twice. Alternatively, patients who made only 1 consultation with a psychiatrist had to have consulted their GP at least twice, which was a proxy for collaborative care. 41 Highest frequency of care was defined as receiving at least 4+ consultations or interventions/year.42-44 Continuity of physician care was measured with the Usual Provider Continuity Index, describing the proportion of consultations with the usual GP or psychiatrist of all GP and psychiatrists consulted in outpatient care, including consultations in walk-in clinics. A score of ≥0.80 is considered high continuity of care. 45 Frequent ED use was defined as 4+ visits/year, which is a minimum standard.46,47
Analyses
As missing values were <1%, a complete case analysis was used. 48 Descriptive analyses followed by bivariate multinomial logistic regressions were produced, the latter testing associations between each independent variable and the outcome variable (death). As the intraclass correlation coefficient was small (0.02), indicating low shared variance among patients from the 14 addiction treatment centers, multilevel analysis was not required, but is usually recommended for 50+ level 2 analysis units.49,50 Predictors identified as significant in bivariate analyses (Alpha: 0.20) 51 were entered with the forward stepwise model selection into the multivariable multinomial logistic regression model, with “no death” as the reference group. This model was justified considering the low number of death events, despite the large study sample. The Akaike Information Criterion (AIC) 52 was used to select the final multivariate model, including the smallest AIC. Variance inflation factor (VIF) was also tested, and small VIF values (<3) indicate a low correlation among variables. 53 Relative risk ratio (RRR) and 95% confidence interval (CI) were calculated in the final model. Statistical analyses were performed using Stata 17. 54
Results
Of the 19,099 patients with SRD, 74 deceased in 2012−2013 and 10 died of unknown causes from 2013−2014 to 2015−2016, who were excluded. Of the final 19,015-patient sample, 255 (1.3%) died from physical illness and 199 (1.1%) of accidental/intentional causes from 2013−2014 to 2015−2016. Patients included 20% with alcohol-related disorders only, 73% had MD (38% common MD and 24% serious MD), 42% chronic physical illnesses, 34% cooccurring SRD-MD-chronic physical illnesses, and 16% suicidal behaviours (Table 1). The majority (66%) were men, 19% were 50+ years, 55% were unemployed or retired, 46% lived alone, 57% and 52% were in more materially or socially deprived areas, and 52% were in urban areas. Within the 12-month period prior to death, 44% of patients were without a usual physician, 49% consulted their usual GP and 19% their usual psychiatrist, with 46% receiving high continuity of physician care; 44% were provided with psychosocial interventions in community healthcare centers, and 55% services from addiction treatment centers. About half (51%) used ED, including 9% who were frequent ED users, and 20% were hospitalized.
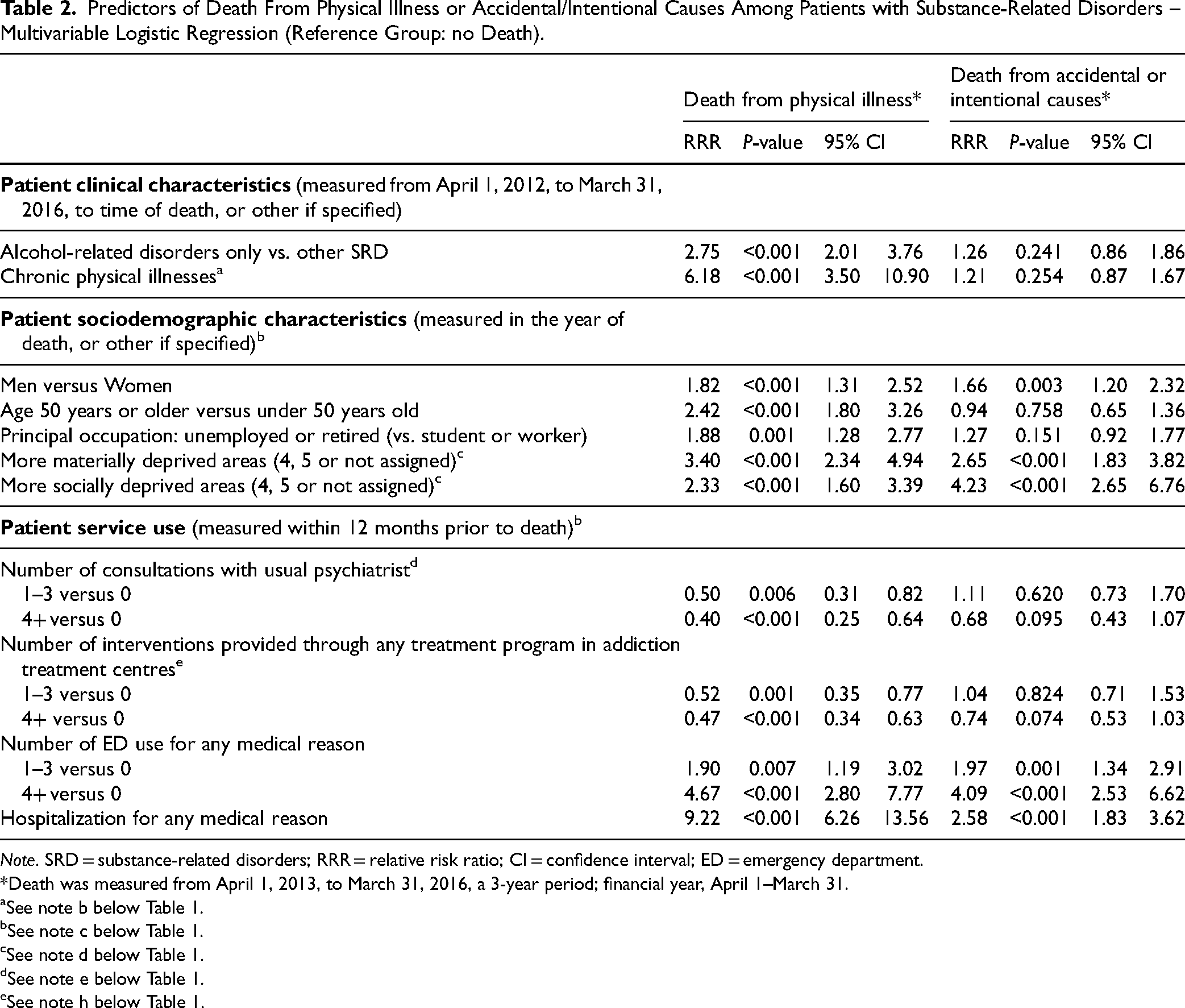
Patients with alcohol-related disorders only and those with SRD-chronic physical illnesses, respectively, had a 1.75 and 5.18 times higher risk of death from a physical illness compared to patients with other SRD or those without chronic physical illness (Table 2). Compared to women, men were 82% more likely to die from physical illness and 66% more likely to die of accidental/intentional causes. Patients living in more materially deprived areas had a 2.40 times higher risk of death from physical illness and 1.65 times higher risk of accidental/intentional death, while those in socially deprived areas had a 1.33 times higher risk of death from physical illness and 3.23 times higher risk of accidental/intentional death. Patients 50+ years of age or unemployed had a 1.42 times or 88% higher risk of death from a physical illness compared with younger or worker/student patients.
Predictors of Death From Physical Illness or Accidental/Intentional Causes Among Patients with Substance-Related Disorders – Multivariable Logistic Regression (Reference Group: no Death).
Note. SRD = substance-related disorders; RRR = relative risk ratio; CI = confidence interval; ED = emergency department.
*Death was measured from April 1, 2013, to March 31, 2016, a 3-year period; financial year, April 1–March 31.
See note b below Table 1.
See note c below Table 1.
See note d below Table 1.
See note e below Table 1.
See note h below Table 1.
Compared to patients with no psychiatric consultations, those who received 1 to 3 or 4+ psychiatric consultations were 50% and 60% less likely to die from physical illness. Receiving 4+ consultations suggested a 32% statistical trend toward a lower risk of accidental/intentional death. Patients who received 1 to 3 or 4+ interventions in addiction treatment centers were 48% or 53% less likely to die from physical illness than those without SRD interventions, while receiving 4+ interventions also related to a 26% statistical trend toward a lower risk of accidental/intentional death. Patients who used ED 1 to 3 times and frequent ED users had a 90% or 3.67 times higher risk of death from physical illness, as well as 3.09 times (97%) higher risk of accidental/intentional death than those who did not use ED. Previously hospitalized patients were at 8.22 times higher risk of death from physical illness and at 1.58 times more risk for accidental/intentional death.
Discussion
This study identified patient sociodemographic, clinical, and service use characteristics that predicted death from physical illness or accidental/intentional causes. The study death rate from 2013−2014 to 2015−2016 (2.4%) was higher than in the Quebec general population for this period, with an average near 0.6%/year. 55 The findings confirmed the first hypothesis that severe health conditions would be the strongest predictors of death from physical illness. The risk of death for patients previously hospitalized, reporting SRD-chronic physical illnesses, with previous frequent ED use, or with alcohol-related disorders only were 8, 5, 4, and 2 times greater than that of patients without these conditions. SRD, and alcohol-related disorders more specifically, are known to contribute to the development of several chronic physical illnesses like cancer, liver, and cardiovascular diseases 56 often associated with death.10,57 These patients usually require hospitalization as well, testifying to the severity of these health conditions. Hospitalization was the study variable most strongly linked to death from physical illness, with higher risk also identified among patients 50+ years old. That older age increases both the risk of chronic physical illnesses and death is well-known. 23
Being a frequent ED user is a key indicator of adverse outcomes for patients.58,59 Frequent ED use often translates into inappropriate provision or quality of outpatient care for patients with diverse needs. 60 Studies show that patients with SRD have some of the highest rates of ED use and hospitalization, which might be explained by their usually low rates of outpatient service use 61 and high dropout from services. 62 Roughly half of the patients in this study lacked a usual physician, high continuity of physician care, and had received no treatment from addiction treatment centers or community healthcare centers in the 12-month follow-up period before death. Considering that three-quarters of patients had cooccurring MD, nearly half with chronic physical illnesses, and more than one-third with SRD-MD-chronic physical illnesses, this low level of outpatient service use might explain the high study rates of frequent ED use and hospitalization. Both adverse outcomes, frequent ED use and hospitalization, predicted accidental/intentional death and death from physical illness among hospitalized patients, whose risk for accidental/intentional death, however, was 4 times lower than death from physical illness.
Accidental/intentional death was explained more by sociodemographic characteristics than other patient characteristics. Notably, patients living in more socially deprived areas were twice as likely to die of accidental/intentional causes than from physical illness, making social deprivation the strongest predictor of accidental/intentional death. It is possible that patients without social support were at higher risk for suicide or self-harm and were possibly more victimized by aggression or prone to risky behaviours leading to accidental death. By contrast, a good social network might encourage patients to seek help for SRD and to complete treatment. 63 Living in more materially deprived areas was also strongly associated with both death from physical illness and accidental/intentional death. Poverty has often been associated in previous research with a greater risk of death, due to poor lifestyle habits leading to more chronic physical illnesses and associated difficulties.64,65 However, in this study being unemployed or retired was associated with death from physical illness only, perhaps due to the more severe health conditions and older age of this group that may prevent them to work. Finally, being male increases the risk of both death from physical illness and accidental/intentional death. Men usually seek less help than women 66 and tend to use specialized services rather than primary care, 67 as they often seek help as a last resort when their health conditions become intolerable 68 —another possible explanation for the higher risk of death. However, the literature shows mixed results on risk of death according to sex, with studies finding higher risk among women,69,70 higher among men, 56 or no differences between them. 71
The second study hypothesis, which states that more adequate outpatient service use would protect against both death from physical illness and accidental/intentional causes, was partially confirmed. Findings showed that receiving at least 1 intervention from a usual psychiatrist or addiction treatment center protected against death from physical illness. However, the findings for accidental/intentional death reflected only statistical trends. Patients with more complex health problems were perhaps more likely to adhere to their psychiatric or SRD treatments, which may have helped reduce their risk of death from physical illness. Moreover, outpatient services provided by hospital psychosocial teams, crisis or suicide prevention centers might have safeguarded patients against the risk of death by accidental/intentional causes better than physician care or services for SRD, but this data was not available to the study. The results might also reflect the uncaptured severity or poor self-management of health conditions. As well, the study found small associations between a higher intensity of care provided to patients and death. Study results on the appropriate intensity of care for patients with SRD are mixed 72 and may fluctuate according to patient needs. The intensity of services is only 1 dimension of quality of care, 73 while adequacy of services for responding to the diversity of patient needs and deployment of best practices may be more key for protecting patients against adverse events. In this study, both the provision of high continuity physician care and care from a usual GP did not protect against death. According to the literature, GP greatly underdetect and undertreat patients with SRD and cooccurring SRD-MD, as they are often uncomfortable with these patients.74,75 This might explain the finding that these two variables did not protect against death.
Limitations
First, SRD other than alcohol only were combined in a single category. The database did not make it possible to identify specific SRD (e.g., opioid-related disorders) that could be more strongly associated with death from physical illness or accidental/intentional death. Second, it was not possible to distinguish accidental from intentional death in the database. These categories were thus integrated, even though they may have been related to distinct predictors. Third, services like crisis centers, suicide prevention centers, Alcoholics Anonymous, or hospital psychosocial care that could help prevent death were not included in the study database. Fourth, a longer follow-up period might have helped better identify patient characteristics related to death. Finally, results may not be generalizable to patients with SRD not using addiction treatment centers, or to countries without public healthcare insurance for this population.
Conclusion
This study found that the severity of patient conditions, mainly among hospitalized patients, those with SRD-chronic physical illnesses, alcohol-related disorders, or more materially deprived, most strongly predicted death from physical illness. Patient sociodemographic characteristics were more strongly linked to accidental/intentional death, especially for those living in more socially deprived areas. However, previous hospitalization also predicted accidental/intentional death. Being a frequent ED user predicted both deaths from physical illness and accidental/intentional causes, suggesting that outpatient care was highly inappropriate for responding to patients with diverse needs. Only specialized SRD and psychiatric care decreased the risk of death from physical illness. However, study patients used few outpatient services overall despite dealing with multiple health issues. Outpatient services could thus be greatly improved by increasing outreach and motivational interventions, and in ED and hospital units through particular attention to screening, brief intervention, and treatment referral including information on and prevention of risky behaviours, especially for patients at high risk of accidental/intentional death. Patients with more severe health conditions, those materially deprived, and especially older men at higher risk of death from physical illness could benefit from programs like assertive community treatment or intensive case management that respond well to patient needs. Collaborative care between SRD, physical and mental health services, including increased training for GP on treatment for patients with SRD, could further promote improved overall care, more specifically for patients at high risk of death from physical illness.
Footnotes
Acknowledgements
We gratefully acknowledge the support of the Substance Use and Addiction Program of Health Canada, the Quebec Ministère de la santé et des services sociaux (Ministry of Health and Social Services0 and the University Institute on Addictions (IUD), as well as the Quebec Network on Suicide, Mood Disorders and Associated Disorders.
Availability of Data
In accordance with the applicable ethics regulations for the province of Quebec, the principal investigator is responsible for keeping data confidential.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Substance Use and Addiction Program of Health Canada, Québec Ministère de la santé et des services sociaux (Ministry of Health and Social Services), grant numbers 8400886 and 8400993.
Appendix
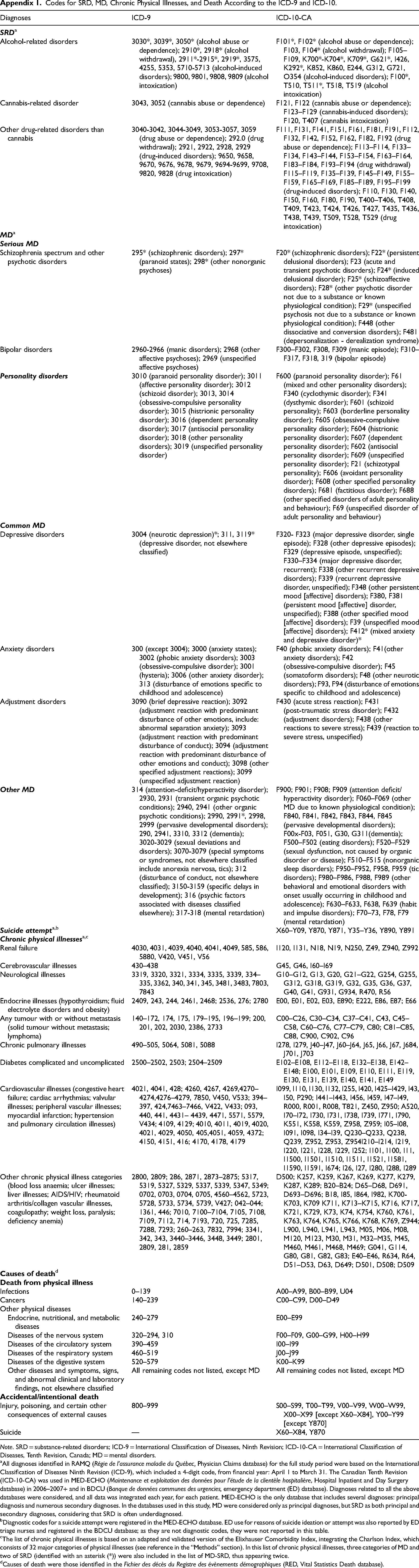
Codes for SRD, MD, Chronic Physical Illnesses, and Death According to the ICD-9 and ICD-10.
| Diagnoses | ICD-9 | ICD-10-CA |
|---|---|---|
|
|
||
| Alcohol-related disorders | 3030*, 3039*, 3050* (alcohol abuse or dependence); 2910*, 2918* (alcohol withdrawal), 2911*-2915*, 2919*, 3575, 4255, 5353, 5710-5713 (alcohol-induced disorders); 9800, 9801, 9808, 9809 (alcohol intoxication) | F101*, F102* (alcohol abuse or dependence); F103, F104* (alcohol withdrawal); F105–F109, K700*-K704*, K709*, G621*, I426, K292*, K852, K860, E244, G312, G721, O354 (alcohol-induced disorders); F100*, T510, T511*, T518, T519 (alcohol intoxication) |
| Cannabis-related disorder | 3043, 3052 (cannabis abuse or dependence) | F121, F122 (cannabis abuse or dependence); F123–F129 (cannabis-induced disorders); F120, T407 (cannabis intoxication) |
| Other drug-related disorders than cannabis | 3040-3042, 3044-3049, 3053-3057, 3059 (drug abuse or dependence); 292.0 (drug withdrawal); 2921, 2922, 2928, 2929 (drug-induced disorders); 9650, 9658, 9670, 9676, 9678, 9679, 9694-9699, 9708, 9820, 9828 (drug intoxication) | F111, F131, F141, F151, F161, F181, F191, F112, F132, F142, F152, F162, F182, F192 (drug abuse or dependence); F113–F114, F133–F134, F143–F144, F153–F154, F163–F164, F183–F184, F193–F194 (drug withdrawal) F115–F119, F135–F139, F145–F149, F155–F159, F165–F169, F185–F189, F195–F199 (drug-induced disorders); F110, F130, F140, F150, F160, F180, F190, T400–T406, T408, T409, T423, T424, T426, T427, T435, T436, T438, T439, T509, T528, T529 (drug intoxication) |
|
|
||
|
|
||
| Schizophrenia spectrum and other psychotic disorders | 295* (schizophrenic disorders); 297* (paranoid states); 298* (other nonorganic psychoses) | F20* (schizophrenic disorders); F22* (persistent delusional disorders); F23 (acute and transient psychotic disorders); F24* (induced delusional disorder); F25* (schizoaffective disorders); F28* (other psychotic disorder not due to a substance or known physiological condition); F29* (unspecified psychosis not due to a substance or known physiological condition); F448 (other dissociative and conversion disorders); F481 (depersonalization - derealization syndrome) |
| Bipolar disorders | 2960-2966 (manic disorders); 2968 (other affective psychoses); 2969 (unspecified affective psychoses) | F300–F302, F308, F309 (manic episode); F310–F317, F318, 319 (bipolar episode) |
|
|
3010 (paranoid personality disorder); 3011 (affective personality disorder); 3012 (schizoid disorder); 3013, 3014 (obsessive-compulsive personality disorder); 3015 (histrionic personality disorder); 3016 (dependent personality disorder); 3017 (antisocial personality disorder); 3018 (other personality disorders); 3019 (unspecified personality disorder) | F600 (paranoid personality disorder); F61 (mixed and other personality disorders); F340 (cyclothymic disorder); F341 (dysthymic disorder); F601 (schizoid personality); F603 (borderline personality disorder); F605 (obsessive-compulsive personality disorder); F604 (histrionic personality disorder); F607 (dependent personality disorder); F602 (antisocial personality disorder); F609 (unspecified personality disorder); F21 (schizotypal personality); F606 (avoidant personality disorder); F608 (other specified personality disorders); F681 (factitious disorder); F688 (other specified disorders of adult personality and behaviour); F69 (unspecified disorder of adult personality and behaviour) |
|
|
||
| Depressive disorders | 3004 (neurotic depression)*; 311, 3119* (depressive disorder, not elsewhere classified) | F320- F323 (major depressive disorder, single episode); F328 (other depressive episodes); F329 (depressive episode, unspecified); F330–F334 (major depressive disorder, recurrent); F338 (other recurrent depressive disorders); F339 (recurrent depressive disorder, unspecified); F348 (other persistent mood [affective] disorders); F380, F381 (persistent mood [affective] disorder, unspecified); F388 (other specified mood [affective] disorders); F39 (unspecified mood [affective] disorders); F412* (mixed anxiety and depressive disorder)* |
| Anxiety disorders | 300 (except 3004); 3000 (anxiety states); 3002 (phobic anxiety disorders); 3003 (obsessive-compulsive disorder); 3001 (hysteria); 3006 (other anxiety disorder); 313 (disturbance of emotions specific to childhood and adolescence) | F40 (phobic anxiety disorders); F41(other anxiety disorders); F42 (obsessive-compulsive disorder); F45 (somatoform disorders); F48 (other neurotic disorders); F93, F94 (disturbance of emotions specific to childhood and adolescence) |
| Adjustment disorders | 3090 (brief depressive reaction); 3092 (adjustment reaction with predominant disturbance of other emotions, include: abnormal separation anxiety); 3093 (adjustment reaction with predominant disturbance of conduct); 3094 (adjustment reaction with predominant disturbance of other emotions and conduct); 3098 (other specified adjustment reactions); 3099 (unspecified adjustment reaction) | F430 (acute stress reaction); F431 (post-traumatic stress disorder); F432 (adjustment disorders); F438 (other reactions to severe stress); F439 (reaction to severe stress, unspecified) |
|
|
314 (attention-deficit/hyperactivity disorder); 2930, 2931 (transient organic psychotic conditions); 2940, 2941 (other organic psychotic conditions); 2990, 2991*, 2998, 2999 (pervasive developmental disorders); 290, 2941, 3310, 3312 (dementia); 3020-3029 (sexual deviations and disorders); 3070-3079 (special symptoms or syndromes, not elsewhere classified include anorexia nervosa, tics); 312 (disturbance of conduct, not elsewhere classified); 3150-3159 (specific delays in development); 316 (psychic factors associated with diseases classified elsewhere); 317-318 (mental retardation) | F900; F901; F908; F909 (attention deficit/hyperactivity disorder); F060–F069 (other MD due to known physiological condition); F840, F841, F842, F843, F844, F845 (pervasive developmental disorders); F00x-F03, F051, G30, G311(dementia); F500–F502 (eating disorders); F520–F529 (sexual dysfunction, not caused by organic disorder or disease); F510–F515 (nonorganic sleep disorders); F950–F952, F958, F959 (tic disorders); F980–F986, F988, F989 (other behavioral and emotional disorders with onset usually occurring in childhood and adolescence); F630–F633, F638, F639 (habit and impulse disorders); F70–73, F78, F79 (mental retardation) |
|
|
X60–Y09, Y870, Y871, Y35–Y36, Y890, Y891 | |
|
|
||
| Renal failure | 4030, 4031, 4039, 4040, 4041, 4049, 585, 586, 5880, V420, V451, V56 | I120, I131, N18, N19, N250, Z49, Z940, Z992 |
| Cerebrovascular illnesses | 430–438 | G45, G46, I60–I69 |
| Neurological illnesses | 3319, 3320, 3321, 3334, 3335, 3339, 334–335, 3362, 340, 341, 345, 3481, 3483, 7803, 7843 | G10–G12, G13, G20, G21–G22, G254, G255, G312, G318, G319, G32, G35, G36, G37, G40, G41, G931, G934, R470, R56 |
| Endocrine illnesses (hypothyroidism; fluid electrolyte disorders and obesity) | 2409, 243, 244, 2461, 2468; 2536, 276; 2780 | E00, E01, E02, E03, E890; E222, E86, E87; E66 |
| Any tumour with or without metastasis (solid tumour without metastasis; lymphoma) | 140–172, 174, 175, 179–195, 196–199; 200, 201, 202, 2030, 2386, 2733 | C00–C26, C30–C34, C37–C41, C43, C45–C58, C60–C76, C77–C79, C80; C81–C85, C88, C900, C902, C96 |
| Chronic pulmonary illnesses | 490–505, 5064, 5081, 5088 | I278, I279, J40–J47, J60–J64, J65, J66, J67, J684, J701, J703 |
| Diabetes complicated and uncomplicated | 2500–2502, 2503; 2504–2509 | E102–E108, E112–E118, E132–E138, E142–E148; E100, E101, E109, E110, E111, E119, E130, E131, E139, E140, E141, E149 |
| Cardiovascular illnesses (congestive heart failure; cardiac arrhythmias; valvular illnesses; peripheral vascular illnesses; myocardial infarction; hypertension and pulmonary circulation illnesses) | 4021, 4041, 428; 4260, 4267, 4269,4270–4274,4276–4279, 7850, V450, V533; 394–397, 424,7463–7466, V422, V433; 093, 440, 441, 4431– 4439, 4471, 5571, 5579, V434; 4109, 4129; 4010, 4011, 4019, 4020, 4021, 4029, 4050, 405,4051, 4059, 4372; 4150, 4151, 416; 4170, 4178, 4179 | I099, I110, I130, I132, I255, I420, I425–I429, I43, I50, P290; I441–I443, I456, I459, I47–I49, R000, R001, R008, T821, Z450, Z950; A520, I70–I72, I730, I731, I738, I739, I771, I790, K551, K558, K559, Z958, Z959; I05–I08, I091, I098, I34–I39, Q230–Q233, Q238, Q239, Z952, Z953, Z954I210–I214, I219, I220, I221, I228, I229, I252; I101, I100, I11, I1500, I1501, I1510, I1511, I1521, I1581, I1590, I1591, I674; I26, I27, I280, I288, I289 |
| Other chronic physical illness categories (blood loss anaemia; ulcer illnesses; liver illnesses; AIDS/HIV; rheumatoid arthritis/collagen vascular illnesses, coagulopathy; weight loss, paralysis; deficiency anemia) | 2800, 2809; 286, 2871, 2873–2875; 5317, 5319, 5327, 5329, 5337, 5339, 5347, 5349; 0702, 0703, 0704, 0705, 4560–4562, 5723, 5728, 5733, 5734, 5739, V427; 042–044; 1361, 446; 7010, 7100–7104, 7105, 7108, 7109, 7112, 714, 7193, 720, 725, 7285, 7288, 7293; 260–263, 7832, 7994; 3341, 342, 343, 3440–3446, 3448, 3449; 2801, 2809, 281, 2859 | D500; K257, K259, K267, K269, K277, K279, K287, K289; B20–B24; D65–D68, D691, D693–D696; B18, I85, I864, I982, K700- K703, K709 K711, K713–K715, K716, K717, K721, K729, K73, K74, K754, K760, K761, K763, K764, K765, K766, K768, K769, Z944; L900, L940, L941, L943, M05, M06, M08, M120, M123, M30, M31, M32–M35, M45, M460, M461, M468, M469; G041, G114, G80, G81, G82, G83; E40–E46, R634, R64, D51–D53, D63, D649; D501, D508; D509 |
|
|
||
|
|
||
| Infections | 0–139 | A00–A99, B00–B99, U04 |
| Cancers | 140–239 | C00–C99, D00–D49 |
| Other physical diseases | ||
| Endocrine, nutritional, and metabolic diseases | 240–279 | E00–E99 |
| Diseases of the nervous system | 320–294, 310 | F00–F09, G00–G99, H00–H99 |
| Diseases of the circulatory system | 390–459 | I00–I99 |
| Diseases of the respiratory system | 460–519 | J00–J99 |
| Diseases of the digestive system | 520–579 | K00–K99 |
| Other diseases and symptoms, signs, and abnormal clinical and laboratory findings, not elsewhere classified | All remaining codes not listed, except MD | All remaining codes not listed, except MD |
|
|
||
| Injury, poisoning, and certain other consequences of external causes | 800–999 | S00–S99, T00–T99, V00–V99, W00–W99, X00–X99 [except X60–X84], Y00–Y99 [except Y870] |
| Suicide | — | X60–X84, Y870 |
Note. SRD = substance-related disorders; ICD-9 = International Classification of Diseases, Ninth Revision; ICD-10-CA = International Classification of Diseases, Tenth Revision, Canada; MD = mental disorders.
All diagnoses identified in RAMQ (Régie de l’assurance maladie du Québec, Physician Claims database) for the full study period were based on the International Classification of Diseases Ninth Revision (ICD-9), which included a 4-digit code, from financial year: April 1 to March 31. The Canadian Tenth Revision (ICD-10-CA) was used in MED-ECHO (Maintenance et exploitation des données pour l’étude de la clientèle hospitalière, Hospital Inpatient and Day Surgery database) in 2006–2007+ and in BDCU (Banque de données communes des urgencies, emergency department (ED) database). Diagnoses related to all the above databases were considered, and all data was integrated each year, for each patient. MED-ECHO is the only database that includes several diagnoses: principal diagnosis and numerous secondary diagnoses. In the databases used in this study, MD were considered only as principal diagnoses, but SRD as both principal and secondary diagnoses, considering that SRD is often underdiagnosed.
Diagnostic codes for a suicide attempt were registered in the MED-ECHO database. ED use for reasons of suicide ideation or attempt was also reported by ED triage nurses and registered in the BDCU database; as they are not diagnostic codes, they were not reported in this table.
The list of chronic physical illnesses is based on an adapted and validated version of the Elixhauser Comorbidity Index, integrating the Charlson Index, which consists of 32 major categories of physical illnesses (see reference in the “Methods” section). In this list of chronic physical illnesses, three categories of MD and two of SRD (identified with an asterisk (*)) were also included in the list of MD-SRD, thus appearing twice.
Causes of death were those identified in the Fichier des décès du Registre des évènements démographiques (RED, Vital Statistics Death database).