
Abstract
Objective
In 2018, the sale of non-medical cannabis was authorized in the province of Quebec in Canada, within a public monopoly under the Société Québécoise du Cannabis (SQDC). The objective of this study was to offer a description of the cannabis-using population regarding the sources of cannabis supply and to explore whether at-risk individuals are purchasing cannabis at SQDC.
Method
We used data from a cross-sectional, representative population survey (age >18 years, n = 1799), the Enquête Québécoise sur le Cannabis, which was completed between February and June 2019. Analyses involved adjusted binary logistic regressions, incorporating population weights, to assess 7 potential indicators of harm.
Results
The vulnerability profiles of SQDC consumers (47.8%) and those acquiring their cannabis elsewhere (52.2%) were similar in terms of frequency of cannabis use (adjusted odds ratio [aOR] = 0.46; 95% confidence interval [CI] = 0.12-1.67), motivation to use (aOR = 0.62; 95% CI = 0.16-2.46), concomitant consumption of other substances (aOR = 0.80; 95% CI = 0.14-4.75), cannabis-impaired driving behaviours (aOR = 0.93; 95% CI = 0.26-3.36), psychological distress (aOR = 0.99; 95% CI = 0.26-3.79), and problematic cannabis use (aOR = 0.46; 95% CI = 0.13-1.64). However, SQDC consumers were more likely to be aware of the cannabinoid content of the product purchased compared to those who acquired their cannabis from other sources (aOR = 4.12; 95% CI = 1.10-15.40).
Conclusions
No association was detected between the source of cannabis supply and potential vulnerability indicators of cannabis-related harms, but SQDC consumers were more aware of the cannabinoid content of the products purchased. These results suggest that the regulated government supply in Quebec is reaching a substantial portion of those with potential high vulnerability to harm. Whether this knowledge translates into a reduction in the negative consequences related to consumption is still to be determined.
Introduction
Cannabis is one of the most commonly used psychoactive substances with an estimated 200 million consumers worldwide. 1 There has been an increasing awareness of the significance and scope of the burden of disease and mortality associated with cannabis.2,3 The harms attributable to cannabis consumption include respiratory diseases, such as chronic bronchitis,4,5 and higher prevalence of mood and other psychiatric disorders.3,5 Cannabis-impaired driving is estimated to elevate the risk of being involved in a motor vehicle accident 2- to 3-fold 6 and represents the leading cause of cannabis-attributable mortality.7,8 Specific patterns of use have been linked to an increased risk of negative consequences. Heavy use of cannabis, defined as daily to almost daily cannabis use, is a key predictor of most cannabis-related harms. 9 Adolescents and youth are more susceptible to the adverse effects of chronic cannabis use, such as impaired neural development,10,11 cognitive impairment, 12 and lower life satisfaction and achievement. 5 Individuals with a high frequency of consumption are also more likely to transition toward problematic use, 9 or cannabis use disorder (CUD), 13 which is estimated to affect ∼13 million individuals worldwide 3 and is characterized by a loss of control over consumption, neurobiological changes due to cannabis exposure, and negative consequences on the individual's activities and functioning.9,14 Finally, new conditions, such as hyperemesis syndrome, 15 are being associated with possible physiological effects of cannabis. 10
In 2018, Canada legalized the non-medical use of cannabis with a public health-driven objective of reorienting consumers toward a new legal market. 16 Cannabis legalization was based on public health protection principles 17 and the premise that adverse consequences of cannabis use can be reduced through product regulation, retail within a “safer” legal market, and targeted information to consumers.18,19 Overall, there are 3 modality models observed across Canada: strictly government-run in-person and online stores, strictly privately licensed retailers, and a combination of private retailers and online government-run sales. The sale of cannabis in a regulated setting can offer on-site health and prevention information directly to consumers. 20 A public health-focused framework can notably prohibit advertising campaigns and limit youth-oriented marketing and products that may encourage consumption patterns leading to problematic use. 21 Price regulation has also been historically employed to reduce accessibility to substances with addictive potential such as tobacco 22 and alcohol. 23 It has, however, been suggested that the public health outcomes of legalization depend on the regulation modalities of sale and distribution, 24 particularly whether individuals at-risk of cannabis-related harms are reached by distribution modalities. It is therefore essential to develop in-depth knowledge of consumer characteristics based on their source of cannabis supply, which remains largely unknown in the context of recent cannabis legalization in Canada.
In Québec, as of October 2018, the sale of non-medical cannabis has been authorized strictly within a public monopoly of government-run online and in-person retail named the Société Québécoise du Cannabis (SQDC). The purpose of this study was to offer a description of the cannabis-using population with regard to their source of cannabis supply and to explore whether at-risk individuals are purchasing cannabis at SQDC. Specifically, we assessed whether the source of cannabis supply is associated with a core set of potential risk indicators of interest for public health25–27: frequency of use, content of cannabis product, motives for using, concomitant use of other substances with cannabis, drug-impaired driving behaviours, psychological distress, and problematic use.
Materials and Methods
Study Design
Data from a 2019 Québec population survey, the Enquête Québécoise sur le cannabis 2019 (EQC), 28 were accessed for secondary analysis. The EQC is a provincial cross-sectional study created in 2018, following the federal policy change, by the Institut de la Statistique du Québec (ISQ). The purpose of the survey was to monitor annual variables of interest for cannabis consumption and related behaviours in Québec. The EQC 2019 was conducted between February 11, 2019, and June 9, 2019. The EQC 2019 data were the most recent available to date, since the 2020 edition was interrupted due to the COVID-19 pandemic. The complete methodology and population characteristics of the survey have been described elsewhere. 29
Participants
Participants were Quebecers aged 15 years and older selected from the Régie de l’Assurance Maladie du Québec, a population-based database of Québec residents covered by the provincial universal health insurance program. Specifically, 16,329 individuals were approached to participate, of whom 10,192 completed the survey (65.8% response rate). The present study sample was restricted to respondents aged 18 years who reported using cannabis in the 12 months preceding the survey (n = 1834). Among the defined study population, 1.6% did not declare the source of supply and were excluded from subsequent analysis (n = 1799). The study was approved by the research ethics committee of the Ethical Board of the Research Centre of Centre Hospitalier de l’Université de Montréal (CÉR CHUM #20.168).
Measures
The independent variable was the source of supply used in the last 12 months as reported by participants. Participants could declare using more than 1 source of supply from the following options: “Cultivated by me or for me,” “From a third party (friends, family members or acquaintance),” “From SQDC online or in store,” “From an official retailer in another province of Canada,” “Directly, from a licensed Health Canada producer,” “From a medical dispensary,” “From an illegal supplier in person or online,” and “Other.” Each choice option was treated into several binary variables (Yes/No). This outcome treatment allowed us to preserve a maximum of study sample participants. Exposition outcome was derived from the “Yes” answers for “From SQDC online or in store,” “Yes” representing respondents who reported any purchases at SQDC since its opening, and “No” representing those reporting not ever purchasing at SQDC.
The 7 dependent variables, or vulnerability indicators for cannabis-related harms, were defined as follows.
Statistical Analyses
First, the sociodemographic characteristics of groups and missing data were described and inspected, as well as the description of the distribution of other sources of cannabis supply used by participants. Then, 7 weighted binary logistic regression models were created, 1 for each potential indicator of cannabis-related harms. Additional missing data for each dependent outcome varied from 0.5% to 3.1% and were considered missing at random. All regression models used “Yes” for retailer sourcing as a reference for exposition groups and lower risk threshold as a reference for outcome groups. Sensitivity analyses were further performed to determine whether the associations with problematic cannabis use would change if the ASSIST outcome was considered as a continuous score. Further analyses were carried out to determine whether the associations with vulnerability markers differed across different thresholds for the proportion of cannabis bought from retailers (partial supply [1%–99%] and exclusive supply [100%]). All models were adjusted for confounding variables including sex, age, education level, and socioeconomic inequalities using the material and social deprivation index. 41 Analyses were conducted using SAS Enterprise Guide (version 8.3.2). Survey sampling weights were applied so that the analyses would be representative of the Québec population. The EQC 2019 used 500 bootstrap weights to account for the complex sampling design. 29 All sample size numbers represent value collected and authorized by ISQ according to weighted sample design; therefore, only the observation of weighted proportion is recommended.
Other Sources of Supply Used by Study Population (n = 1799). a
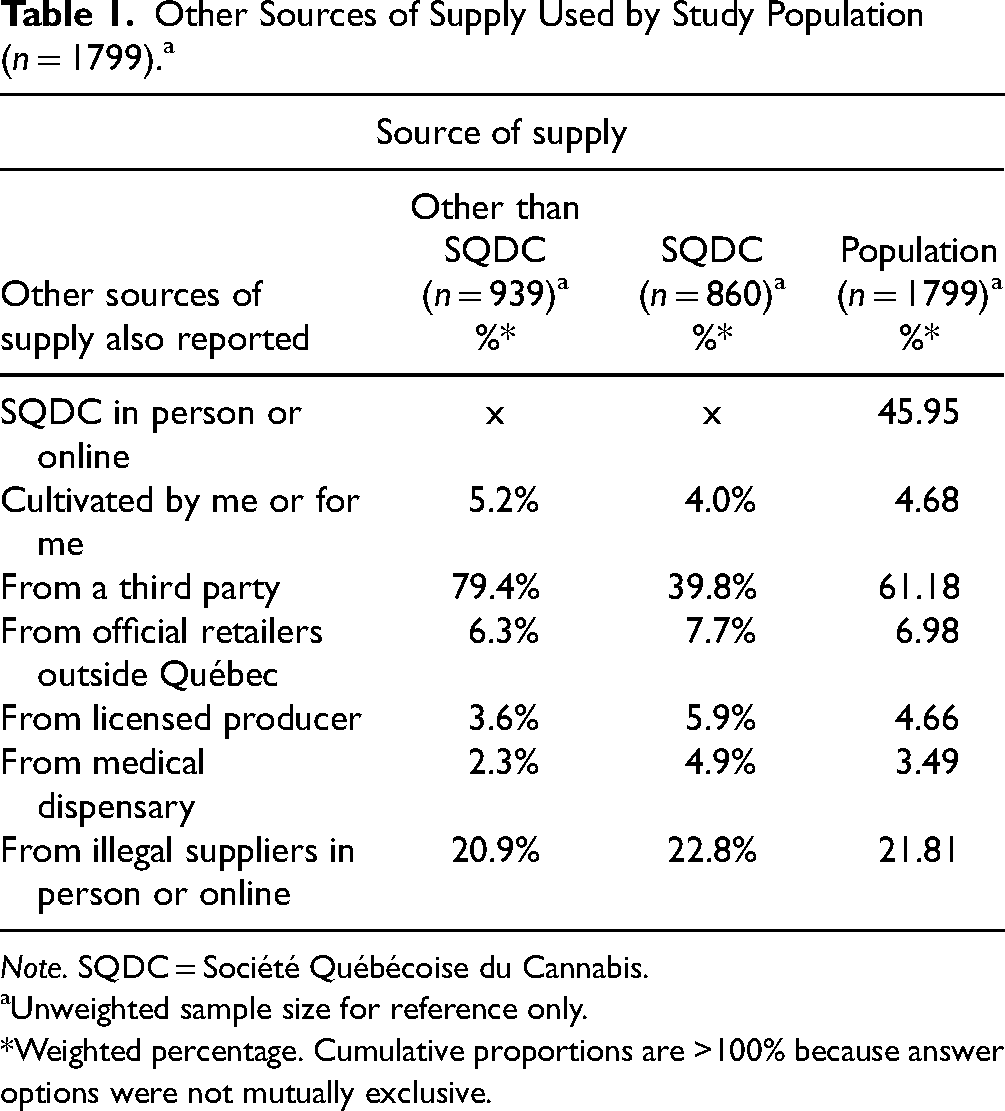
Note. SQDC = Société Québécoise du Cannabis.
Unweighted sample size for reference only.
*Weighted percentage. Cumulative proportions are >100% because answer options were not mutually exclusive.
Specific Prevalence of Cannabis-Related Harms Vulnerability Indicators (n = 1799). a
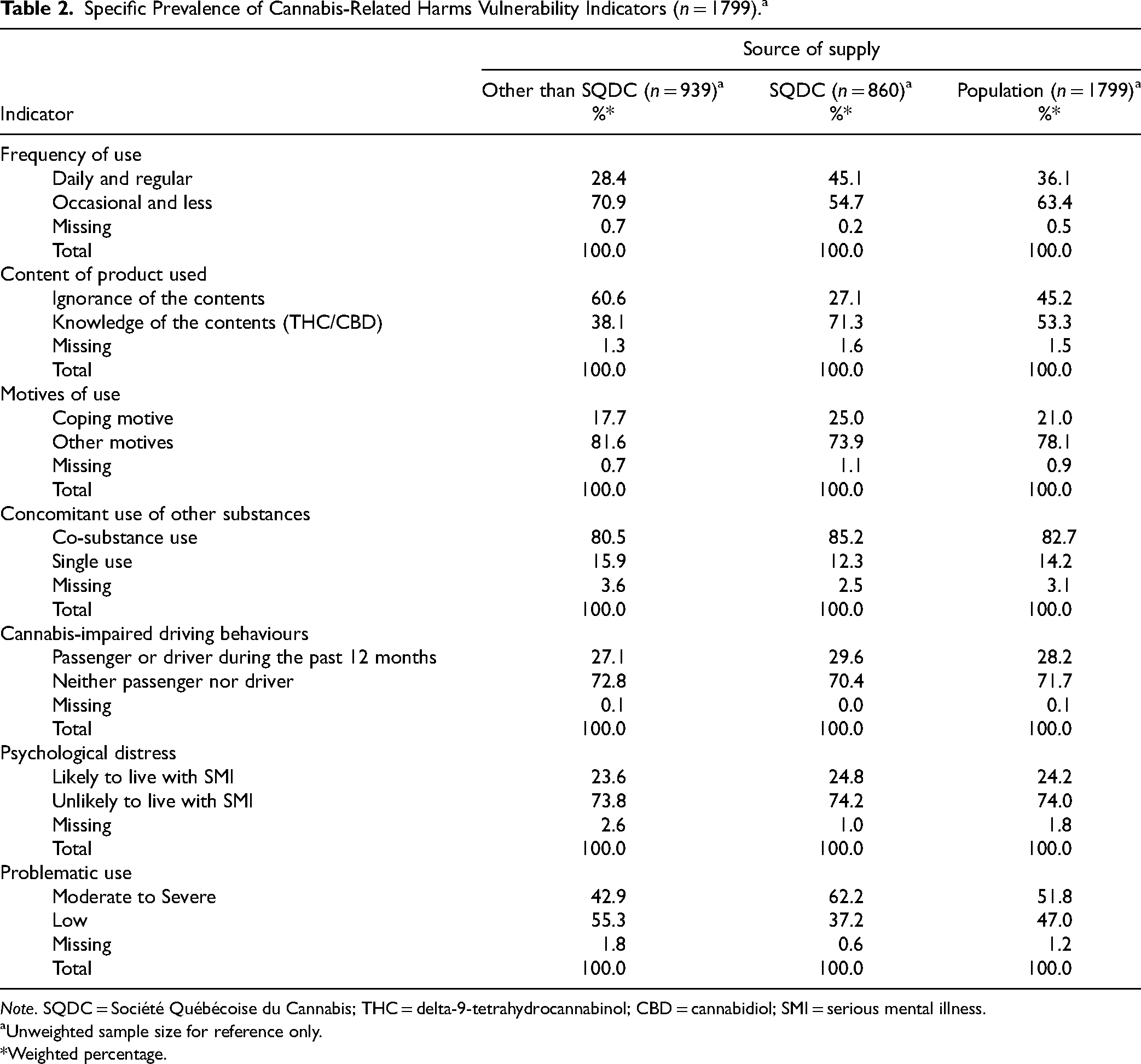
Note. SQDC = Société Québécoise du Cannabis; THC = delta-9-tetrahydrocannabinol; CBD = cannabidiol; SMI = serious mental illness.
Unweighted sample size for reference only.
*Weighted percentage.
Results
Sample Characteristics
The prevalence of cannabis use in the 3 months preceding the survey approximated 13% and cannabis use in 12 months preceding the survey approximated 16%, according to EQC 2019. 28 Among individuals aged 18 and above who used cannabis in the past year, 52.2% had acquired cannabis from SQDC and 47.8% had acquired cannabis only from other sources. The mean age was 37.2 (SD 11.8) years for the total sample, 35.3 (SD 16.0) years for the group acquiring from SQDC, and 38.7 (SD 17.3) years for the group acquiring from other sources. Complete population sociodemographic characteristics are presented in Table 1. Additionally, other sources of cannabis supply also used by participants are described in Table 2.
Sociodemographic Characteristics (n = 1864). a
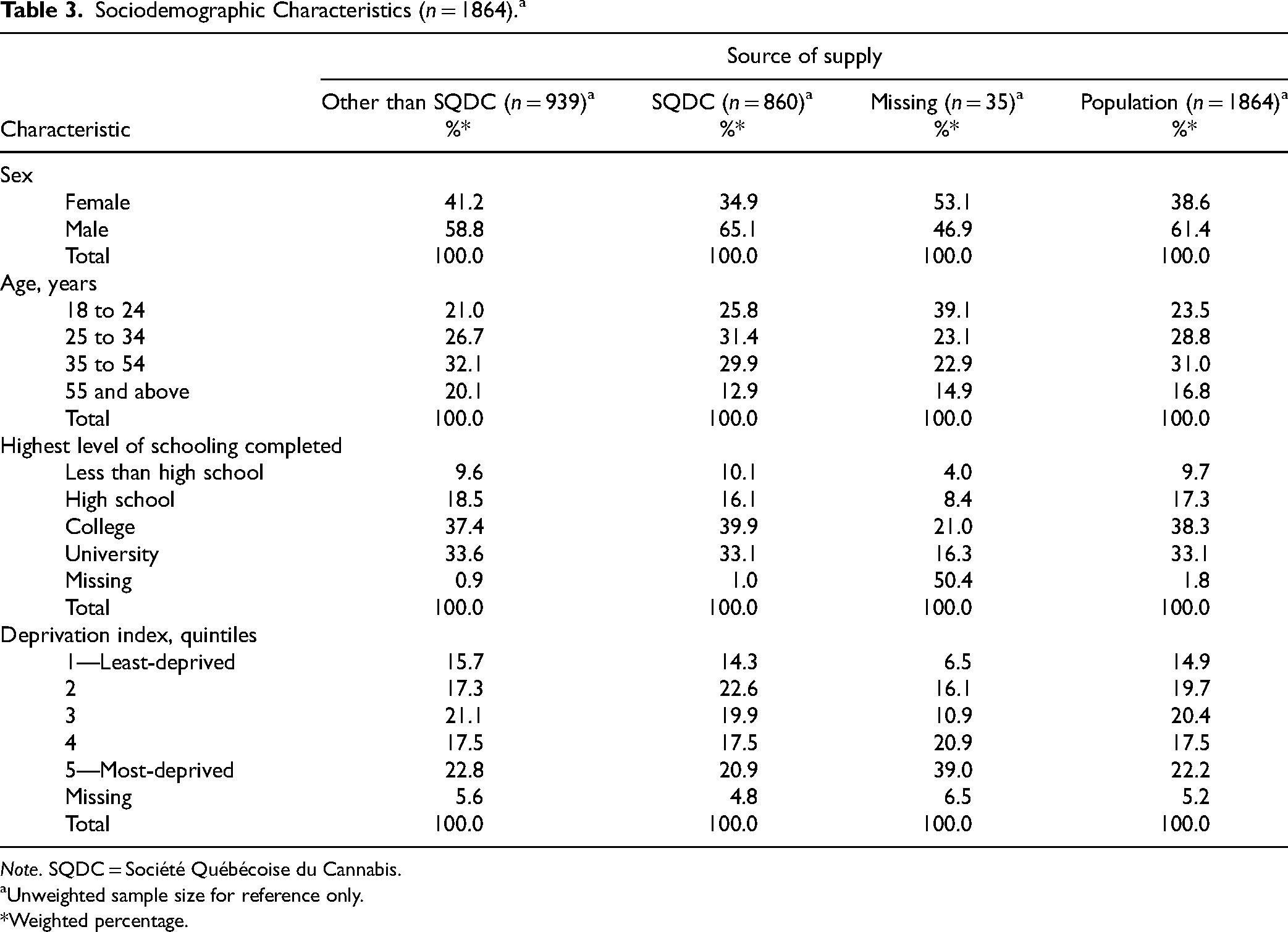
Note. SQDC = Société Québécoise du Cannabis.
Unweighted sample size for reference only.
*Weighted percentage.
A complete description of cannabis-related harms indicators is found in Table 3. The majority (63.4%) of respondents were using cannabis moderately (occasional use or less than once per month) and a substantial proportion (36.1%) were using it heavily (many times per week or daily). About half (53.3%) were able to declare the content of products and the other half (45.2%) were unable to do so. Twenty-one percent of respondents used cannabis to cope with negative emotions, and the vast majority (82.7%) used cannabis in combination with other psychoactive substances. Over a quarter of respondents (28.2%) presented cannabis-impaired driving behaviours, and a quarter of respondents (24.4%) reported experiencing severe psychological distress. Finally, half of the respondents (51.8%) presented a moderate to severe risk of problematic use (see Table 2).
Models Examining Associations with Vulnerability Indicators
Figure 1 illustrates the weighted, adjusted associations between the source of cannabis supply and cannabis-related harm vulnerability indicators. The vulnerability profiles of respondents acquiring cannabis from other sources were similar to the profiles of respondents acquiring it from SQDC in terms of frequency of use (adjusted odds ratio [aOR] = 0.46; 95% CI = 0.12–1.68), motives of use to cope with negative emotions (aOR = 0.62; 95% CI = 0.16–2.46), concomitant use of other substances (aOR = 0.80; 95% CI = 0.14–4.75), cannabis-impaired driving behaviours (aOR = 0.99; 95% CI = 0.27–3.62), psychological distress (aOR = 0.99; 95% CI = 0.26–3.79), and problematic cannabis use (aOR = 0.46; 95% CI = 0.13–1.65). Individuals acquiring from other sources were significantly more likely to be unaware of cannabis content when compared to SQDC sourcing (aOR = 4.12; 95% CI = 1.10–15.41) (see Figure 1).
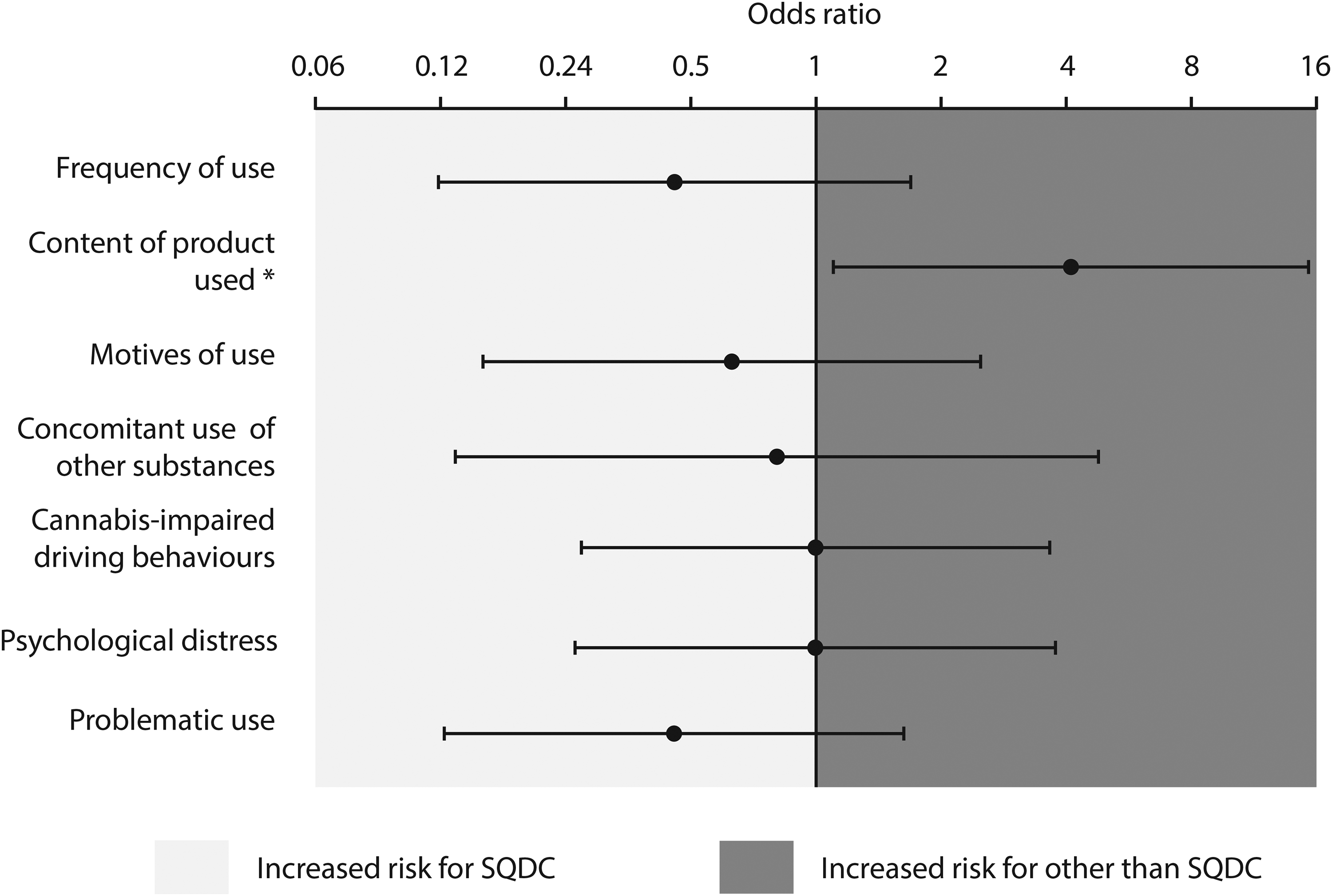
Adjusted odds ratio expressing the vulnerability for cannabis-related harms according to the source of supply.
Sensitivity Analysis
A sensitivity analysis was performed with the ASSIST score treated as a continuous variable using linear regression. The group with individuals purchasing from SQDC had a mean score of 7.3 (SD 5.4) for problematic use whereas the comparison group of individuals who did not use the legal modality of SQDC had a mean score of 4.9 (SD 4.7). The association with ASSIST score remained non-significant in the linear model (mean estimate = −2.15; 95%CI = −44.51 to 40.21, p = 0.92). In a second sensitivity analysis, we compared the vulnerability profiles of participants according to the proportion of cannabis products acquired from the SQDC. Specifically, participants who acquired their cannabis products exclusively (100%) from the SQDC were compared with those who partially acquired their products from the legal source (1%–99%). No significant associations emerged between any vulnerability indicators of consumers when comparing partial to exclusive supply: frequency of use (aOR = 3.31; 95% CI = 0.41–26.46), cannabis content (aOR = 0.78; 95% CI = 0.08–7.47), use to cope with negative emotions (aOR = 1.51; 95% CI = 0.23–9.85), concomitant use of other substances (aOR = 3.09; 95% CI = 0.01–923.05), drug-impaired driving behaviours (aOR = 2.97; 95% CI = 0.37–23.85), psychological distress (aOR = 1.34; 95%CI = 0.13–14.22), and problematic use (aOR = 4.00; 95% CI = 0.27–58.60).
Discussion
The present cross-sectional, population-based survey study explored the vulnerability profiles of consumers sourcing their cannabis from the SQDC and those getting it elsewhere. Our results showed that individuals who obtained their cannabis from sources other than SQDC were significantly more likely to be unaware of the cannabinoid contents of products purchased, while their vulnerability profiles were overall similar to consumers who acquired their non-medical cannabis from the provincial retailer.
Data from the EQC 2019 provide information regarding cannabis-related behaviours during the first year of legalization in Canada. Québec's non-medical cannabis retail started operating in October 2018, and data collection for the EQC (2019) was conducted between February 2019 and June 2019. The EQC was administered during the first year of operations, which was marked by a shortage of supply, delays, and long wait times for delivery for both in-person and online purchases, leaving many individuals to turn to other sources to fill the gap. The short time between the opening of branches and administration of the survey left little time for consumers to change their purchasing habits and transition towards the SQDC, as some people could have been using other sources out of necessity, that is, because no other sources were available at that time. Almost half (45.1%) of those acquiring cannabis from the SQDC were using daily or almost daily, in contrast to a recent Canadian study suggesting that individuals who use daily or almost daily were less likely to acquire dried cannabis from a legal source. 42 The same study also suggested an association between legal cannabis retailing and the perceived and objective proximity to in-person store locations. These findings highlight the specific contextual factors of our study, including the timing of the survey and access to retailers. Similar studies should be replicated in the current context, where a growing number of stores and more efficient delivery modalities have allowed increased access to products in Québec and elsewhere.
The lack of knowledge about cannabis content among people not purchasing cannabis from the SQDC is not trivial from a public health perspective. The concentration of delta-9-tetrahydrocannabinol (THC) in cannabis products has increased over the past 30 years. 43 High THC concentrations have been associated with escalating addictive potential 30 and an increased risk of negative outcomes, including psychosis. 44 The recently published Lower Risk Cannabis Use Guidelines propose choosing products with low THC concentration or with balanced ratios of THC/CBD. 18 However, consumers often do not have the accurate information required to make an informed decision. 45 Unregulated cannabis products tend to have inaccurate or no label indicating THC level. 32 The importance of product purity and contaminant control cannot be overlooked as the health impact of toxic content in unregulated products has yet to be assessed.18,46 Our results imply that the purchase of cannabis from regulated supply sources, like the SQDC, is associated with increased knowledge of the cannabinoid content. While it remains to be determined whether this knowledge translates into a reduction in the negative consequences of cannabis use, our findings suggest that regulated sourcing may facilitate consumers’ adherence to public health recommendations.
The absence of significant association between the vulnerability of consumers (except for knowledge of content) and the source of supply suggests that those at risk were equally reached by new legal modalities. A key aspect of cannabis legalization in Québec focused on providing preventive information focused on risk factors (e.g., mental health status, frequency of use), while supporting legal cannabis sourcing. It is plausible that individuals at-risk of cannabis-related harm were as equally reached by these public health messages. At-risk populations, which include individuals who use cannabis frequently, are also likely to experience encounters with the criminal justice system due to unregulated sourcing and use. The opportunity to avoid such encounters may have been a sufficient incentive for at-risk individuals to use SQDC. Legal cannabis modalities offer not only access to quality-controlled products but also an ideal setting in which to provide harm reduction education and intervention. 18 Our results suggest that these benefits can be made accessible to at-risk individuals and those diverse strategies are needed to ensure that consumers shift to safer regulated cannabis sourcing.
Limitations
Our study has several limitations. Firstly, Québec is distinct from other jurisdictions in that the public monopoly administration of cannabis sales restrains the emergence of an open market or private stores.47,48 Our results may not be generalizable to other models of cannabis retail, including commercial, for-profit outlets. Secondly, the study consists of a secondary analysis of data from a population-based survey (EQC) constructed for another purpose, that is, to gather data concerning consumption habits and behaviours in Québec. 28 Despite the use of validated measures commonly used in research (i.e., ASSIST, Kessler, etc.), variables for this study were self-reported and might be subject to recall bias, with no other objective measures collected, such as urinary THC levels. Finally, while the population weights (i.e., “bootstraps”) used in data collection and design methodology 29 strengthened the generalization of results, the cross-sectional design does not allow for ascertainment of temporality or causality of relations between sources of supply and vulnerability profile of individuals who use cannabis.
Conclusion
Our study results made it possible to examine the vulnerability profiles of individuals who use cannabis according to specific post-legalization sources of supply in a representative sample. Our results captured the profiles of individuals who acquired cannabis from a regulated retailer in Québec, as well as provided a baseline from which to observe the ongoing trends in the province during this period of transition in cannabis-related legislation. No associations were detected between the source of cannabis of supply and potential vulnerability indicators of cannabis-related harms. Purchase from the SQDC was associated with increased awareness of the content of cannabis products. These results might suggest that regulated supply is reaching populations at high risk of experiencing cannabis-related harms. It remains to be determined if these trends are maintained over time and how they translate into the overall prevalence and severity of cannabis-related harms.
Footnotes
Acknowledgments
We thank the Canadian Centre on Substance Use and Addiction who funded this study. We are grateful to all participants, collaborators, project manager (Paméla Lachance-Touchette), and medical writers (Helen Kang and Léa Gagnon) for their contributions. We also thank the Institut de la statistique du Québec and the Centre d’intégration et d’analyse des données médicales du Centre hospitalier universitaire de l’Université de Montréal (CITADEL) for their help.
Data Access
The ISQ provided data used for this study. The ISQ is not responsible for the interpretation or compilation of the results. Data are free to access for researchers, faculty, and students at participating postsecondary educational institutions.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DJA holds a scholar award from the Fonds de recherche du Québec en Santé; he will receive investigational products (starting in 2022) from Tetra Bio Pharma and currently receive investigational products from Cardiol Therapeutics for clinical trials funded by the Québec Ministry of Health and Social Services, which supports Dr. Jutras-Aswad research program on cannabis. Dr. Jutras-Aswad also reports consultancy and expert testimony for the provincial and federal governments on cannabis-related themes. SL has received an untied educational grant from Indivior, unrelated to this work. ER, FC, NK, SD, and CD report no potential conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Centre on Substance Use and Addiction (grant number #4.3a- 410-08-3454).