
Abstract

Introduction/Background
In 1997, the Canadian Psychiatric Association (CPA) and the College of Family Physicians of Canada (CFPC) published a position paper 1 highlighting the importance of improving collaboration between family physicians and psychiatrists and proposing ways in which this could be advanced. In 2011, an updated position paper reviewed the growing evidence, defined principles to guide collaboration and the external changes required to support it, broadened the scope of collaboration to include all mental health and primary care providers and services, and made recommendations for future priorities. 2
Since that time, collaborative mental health care (CMHC) has played a greater role in the planning and organization of Canadian health-care systems. 3 There is a growing recognition of its potential to improve access to care (especially for marginalized and underserved populations), to integrate physical and mental health care, and to facilitate transitions in care.2,4–22 Evolving models of care are increasingly informed by evaluation data and the experiences of individuals with lived experience and families23–26 and use quality improvement methods and implementation science to guide their implementation and outcome measures.24,26,27 This has allowed programs to better respond to the needs of specific populations and support physicians and other health-care providers while building system capacity.3,10,11,28–36 Collaborative models are also being applied to integrate care within other settings such as universities and colleges, workplaces, shelters and long-term care facilities, tailoring services to meet the unique needs of these groups.2,3,10,37,38
This has led to the emergence of a Canadian Collaborative Care Model, 10 which has built upon the CFPC’s seminal vision of the practice of family medicine in Canada, “The Patient’s Medical Home,” 39 which embraces a multidisciplinary, team-based approach to patient and family-centred primary care across the lifespan. It has also been influenced by the Collaborative Care Model developed in the United States by Katon and colleagues for which there is robust evidence as to its benefits for improving processes of care and individual and population outcomes.12,13,29,40
With limited Canadian data, however, questions remain as to which populations and problems are best served by collaborative models and the extent to which CMHC can assist with prevention, early detection, relapse prevention and reducing stigma, while also addressing complex and co-morbid medical conditions. And in a time of virtual care, how can we best use technologies for tele-mental health care, training, support, enhancing self-management and solidifying partnerships.
Our goals in updating this position paper, therefore, are to provide guidance to providers, administrators, educators, researchers and funders to accelerate the introduction of more standardized, evidence-supported approaches to care, and to enhance our understanding of the role of collaboration in addressing wider issues facing any health-care system.
Definitions
Values and Goals
Collaborative care needs to be rooted in core values.32,37,42 These include:
It is person and family centred, with the person themselves always being a partner in their own care. Equity in access, service delivery and outcomes. Services are inclusive and nonstigmatizing. It promotes health and wellbeing. It addresses social and economic determinants of health, including systemic racism. Improve access to services. Enhance the experience of those receiving care. Offer sustainable and cost-effective services. Achieve better outcomes. Enhance the experience of providing care.
In general, program/project goals and activities will reflect these values2,3,10,11,32,43 and will aim to:
The Impact and Benefits of Collaborative Care
The preponderance of research evidence for CMHC is based on studies of the model developed by Katon and colleagues over the past 25 years.13,29 This emphasizes: (a) team-based care, (b) measurement-based care and treatment-to-target, (c) evidence-informed treatment algorithms, and (d) population-oriented care using patient registries and proactive outreach.
Studies spanning different age groups and countries, including Canada, and which have primarily addressed depression13,18,31,44,45 and anxiety46–48 have consistently demonstrated the benefits of CMHC in improving patients’ symptoms and global and physical functioning.12,13,21,29,31,49 The evidence suggests that it increases patients’ use of preventative advice, helps with treatment adherence, and results in better health outcomes and higher rates of satisfaction for both patients and providers.3–5,7–9,13,15,18,19,22,23,31,50–55 Care is more continuous and better coordinated by health-care professionals who are able to treat a wider range of problems, while the coordination of physical and mental health-care services decreases stigma and fosters greater cultural congruence and superior outcomes for individuals with chronic conditions.3,7,18,21,56,57
Collaborative care also improves access while reducing wait times, emergency room visits and hospitalizations. It is seen as cost-effective, avoiding duplication of services and reducing the likelihood of medical errors, and supports population health.7,10,48,51–53,58,59
From a systems perspective, CMHC increases the capacity of family practices—with more people being seen and the skills of primary care providers being augmented—and of the mental health system, of which primary care is now understood to be an integral part.3,10,11,50,52,58
Principles to Guide Collaborative Care
Collaborative care is most likely to be successfully implemented and sustained when based upon principles, rather than simply adopting or transposing a model that has worked elsewhere, without regard for the local context.2,4,10,11,29,38,41,52,53,60,61 Clinicians and planners can then introduce ideas and models based upon these foundational principles and adapt evidence-informed approaches to their local needs, resources and expectations. These guiding principles are organized into those that apply to (a) partnerships between services or systems and (b) between health-care professionals.
Collaboration Between Services or Systems
Collaboration is a process that changes and evolves in response to patient, physician and system variables. It is not a single event or endpoint, and its primary goal is to improve health outcomes.
Physical proximity facilitates closer collaboration.
Models should be individually tailored to each physician or practice—“one size fits one.”
Communication—in person or using technology—is the cornerstone of collaboration and is most effective when both formal and informal means are consistently employed. Language used should be clear, mutually understood, culturally sensitive and recovery oriented.
Transitioning to collaboration requires (a) strong leadership and management, (b) champions to translate innovative ideas into action, (c) engagement from everyone involved at all levels of organization and (d) respect for each other’s expertise and work experiences.
New models need to be sustainable, able to survive the departure of the initial founders, and with the potential to be transferred to other settings.
Collaborative care exists within a wider community and fiscal landscape, so approaches must be adapted according to resource availability, local culture, geography and the severity of the individual’s problem.
Collaborative projects should be planned together from the outset, with clear goals and a mechanism for regular evaluation of progress.
Collaboration Between Providers
Goals for collaboration and individual patient care should be developed together and based upon the patient’s wishes, with the tasks and roles being allocated according to respective skills, interests and resources of each provider and not solely by discipline.
The person and their family should always be at the centre of care, with services adjusting as their needs change over time.
There should be a regular and unimpeded flow of information.
Collaborative care should focus on prevention, wellness promotion and adaptive functioning, as well as treatment and relapse prevention.
Components of Effective Projects
Evidence from multiple sources points towards the following as core elements of effective CMHC.3,10–13,31,38,41,60–63 Care should be:
Activities of Successful Collaborative Care
Programs with limited resources may need to focus on one or two discrete areas of practice such as rapid access to psychiatric consultation, education sessions for primary care physicians, or telephone consultation and support. Additional resources can facilitate more comprehensive collaboration and support. These activities (see below) should enhance and complement (rather than duplicate) existing services and treatments.3,4,10–13,18,31,37,38,42,50,52,56,62–65
Direct Clinical Care Within a Collaborative Partnership
Clinical consultation for children, youth, and adults.
Short-term care and stabilization through: Medication management. Brief psychotherapy—mainly cognitive behavioural therapy, interpersonal psychotherapy or solution-focused therapy. Case management.
Family and couple assessments or treatment.
System navigation and linkages.
Patient education and self-management support.
Telephone or virtual backup or support.
Case discussions and reviews.
Coordinating Care
Development of individualized care plans.
Identification and coordination of resources.
Assistance with navigation to other services.
Ongoing communication.
Building System Capacity
Offering skill-building educational sessions for the primary care team.
Providing information on resources or links to websites.
Providing screening, monitoring, and other clinical tools that can be incorporated within the electronic health record and clinical workflows.
Using technology to reach specific populations and health-care professionals.
Developing evidence-informed programs.
Improving the Care of Populations
Advocating for policy changes, partnerships and program adaptations to achieve equitable health outcomes for disadvantaged populations.
Monitoring the wellbeing of populations through: Early detection/intervention. Relapse prevention.
Providing culturally relevant health education for patients and caregivers.
Roles of the Mental Health Team Members
In a “shared-care” model, the family doctor, psychiatrist, and other mental health professionals (usually a psychologist, social worker, or nurse) will determine between them who is best positioned to provide specific aspects of care and allocate responsibility accordingly.10–13,66,67 In most instances, the family physician will continue to deliver care after a consultation or brief treatment, with support from the mental health team, but the presence of a psychiatrist or other mental health professional enables them to expand their role, knowing that support is readily available.
While the primary role of the psychiatrist is usually to provide consultation and short-term care or stabilization,66,68 they also need to focus on indirect care (e.g., case discussions) and capacity building (e.g., through case-based education) among the primary care team, and assistance with referrals. The psychologist, social worker, or nurse have many potential roles including assessment, care planning and ongoing therapy, monitoring and support, system navigation, and information for the team. This will vary according to their scope of practice and practice needs.
Primary health-care providers such as nurses, dietitians, occupational therapists, physiotherapists, pharmacists and social workers are well positioned to recognize mental health problems, provide support or advice, consult with other members of the team, and deepen a patient’s understanding of the interconnected nature of their physical and mental health care problems.
Specific roles for each team member are outlined in Table 1.
Potential Roles of the Mental Health Team Members

Medico-Legal Responsibility
While the “most responsible physician” in collaborative projects is most often the family physician, responsibility, and potential liability are shared.2,11 Information can be exchanged within a patient’s “circle of care” and all health-care professionals are expected to follow the standards expected of their discipline and the protection of privacy of personal health information guidelines for documentation and communication.
Organization and Practice Changes Required to Support Collaborative Care
Changes to the way care are organized within a practice are often important for successful and sustainable collaboration.11,64 These include: Adequate preparation/training for working in primary care. Person-to-person handovers of care (“warm handoffs”). The use of treatment protocols, guidelines or care pathways. Shared record keeping and charting. Case registries to promote a population focus. Protected time for collaborative activities. Incentives (academic, professional, financial, etc.) to promote the collaborative practice. Measurement, evaluation, and needs assessment using both quantitative and qualitative information.
Collaboration is also more likely to succeed if other external supports are in place, such as advocacy, guidelines, and support from provincial or national organizations, and training in academic settings.The development of a provincial or territorial policy framework that incorporates CMHC, and ongoing funding for innovative projects and knowledge translation, are also key.
2
Changes That any Mental Health Service can Make to Enhance Collaboration
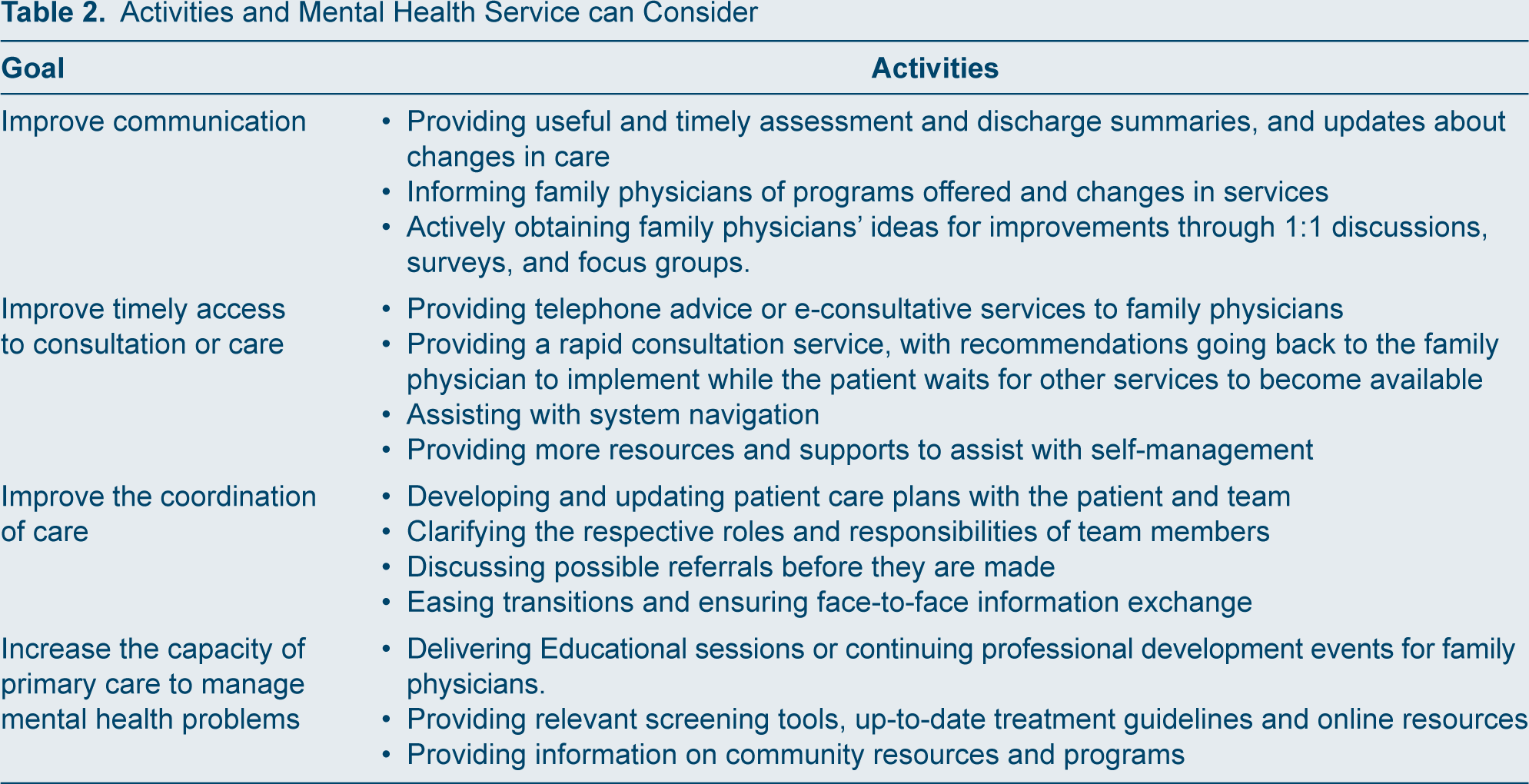
Better collaboration with primary health care should be a goal for all mental health-care services.10,11 While the primary focus of this position paper is on the integration of mental health providers within primary care, every mental health service can introduce changes to improve communication and coordination of care, increase access or enhance the capacity of primary care to deliver effective mental health care. Options to consider are outlined in Table 2.
Activities and Mental Health Service can Consider
Use of Newer Technologies
Telehealth and Virtual Care
This is an increasingly common option for the delivery of care48,69–72 and has become the primary mode of care provided during the COVID-19 pandemic. Telehealth can improve access for underserviced populations and individuals living in remote or distant areas, which may not have direct access to mental health services, or where a “distance” consultation is more convenient for the patient. It can even be employed within the same community, reducing the need for psychiatrists or mental health workers to travel, or for continuity of care when out of their office. And it permits the asynchronous participation of wider participants, improving care coordination and planning.
Telehealth can support distance learning through webinars or less formal teaching sessions (often case-based) with a group of family physicians. Another option is the “train the trainer” model such as that employed by Project ECHO, 71 in which local providers in a more distant community are trained and supported from another location with regular access to case discussions, education, and support. ECHO is also to provide indirect case management support.
Virtual appointments and online education are going to be integral to all future collaborative care. This can extend the reach of CMHC and help make other activities such as monitoring after an episode of care much easier. Experiences during the COVID pandemic suggest many patients are satisfied with virtual care and no-show rates may be lower. This can also be an equity issue as not everyone has access to the internet or even a phone, or a private setting from which to speak in comfort.
Use of Apps and Online Resources
There are an increasing number of apps, websites, and other online resources that can be provided to patients to assist with self-management.73,74 It helps if providers are familiar with the more commonly used apps, including those that have a cost, and can direct patients to those that are appropriate for their care.
Other Technologies
Other ways to provide support include the phone, email and direct messaging including questions and answers on a list serve. Secure platforms are essential. Where supported, access to centralized portals enables multiple health-care professionals to communicate and review consultations, investigations and laboratory results.
Integration of Physical Health Care into Mental Health Settings
In many parts of Canada, individuals living with a mental health and addiction problem, particularly those with severe and persistent mental illnesses, face difficulties in accessing regular, comprehensive, and continuing care. One solution has been the integration within a mental health program of family doctors and/or other health-care professionals (e.g., nurse practitioners) who will visit on a regular basis to assess both acute and chronic health problems, initiate treatment where possible, provide health teaching and education, and link individuals with other required health services. 49
“Team” Competencies and Training for Health-care Professionals
Working collaboratively requires specific skills on the part of mental health professionals.10,11,67,72,75–77 Some are personal qualities and attitudes such as flexibility, respect, a willingness to learn and recognizing that one does not always need to be the “expert.” They also need to appreciate the role primary care plays in any health-care system, the demands it faces, and how these are managed on a daily basis. One way to understand this is to spend a day shadowing a more experienced colleague.
All health-care professionals should possess effective communication skills and cultural sensitivity as well as be aware of and able to mitigate implicit bias and reduce the stigma associated with accessing mental health services or having a mental health problem.
The preparation of future primary care and mental health professionals to work in collaborative partnerships is central to the long-term sustainability of collaborative care, so that this style of practice becomes an integral and expected part of practice for all future practitioners.78–80While collaborative care placements will no longer be mandatory for Canadian psychiatry residents under the new Competency by Design (CBD) curriculum, all residents should continue to have a robust experience in CMHC to appreciate the role family medicine plays and the benefits of better collaboration, and to develop competencies as a consultant and collaborator. Faculty development is also important.
The training of family medicine residents in behavioural science must also continue to be emphasized, to prepare them for their future practice, including working in teams and settings that integrate mental health professionals.
Program Evaluation and Quality Improvement
Evaluation should be built in from the outset of any initiative, with clarity about its purpose and how the results will be used, and by whom.24,81,82 Involvement of patient partners throughout all stages of program planning and evaluation is crucial and many resources exist to support this.23,25 Evaluation should consider: (a) to what extent the overall goals for the collaboration between 2 systems or sectors are being met (outcomes), (b) to what extent the planned changes to care delivery have been implemented (processes) and (c) whether the necessary supports are in place for program effectiveness and sustainability.
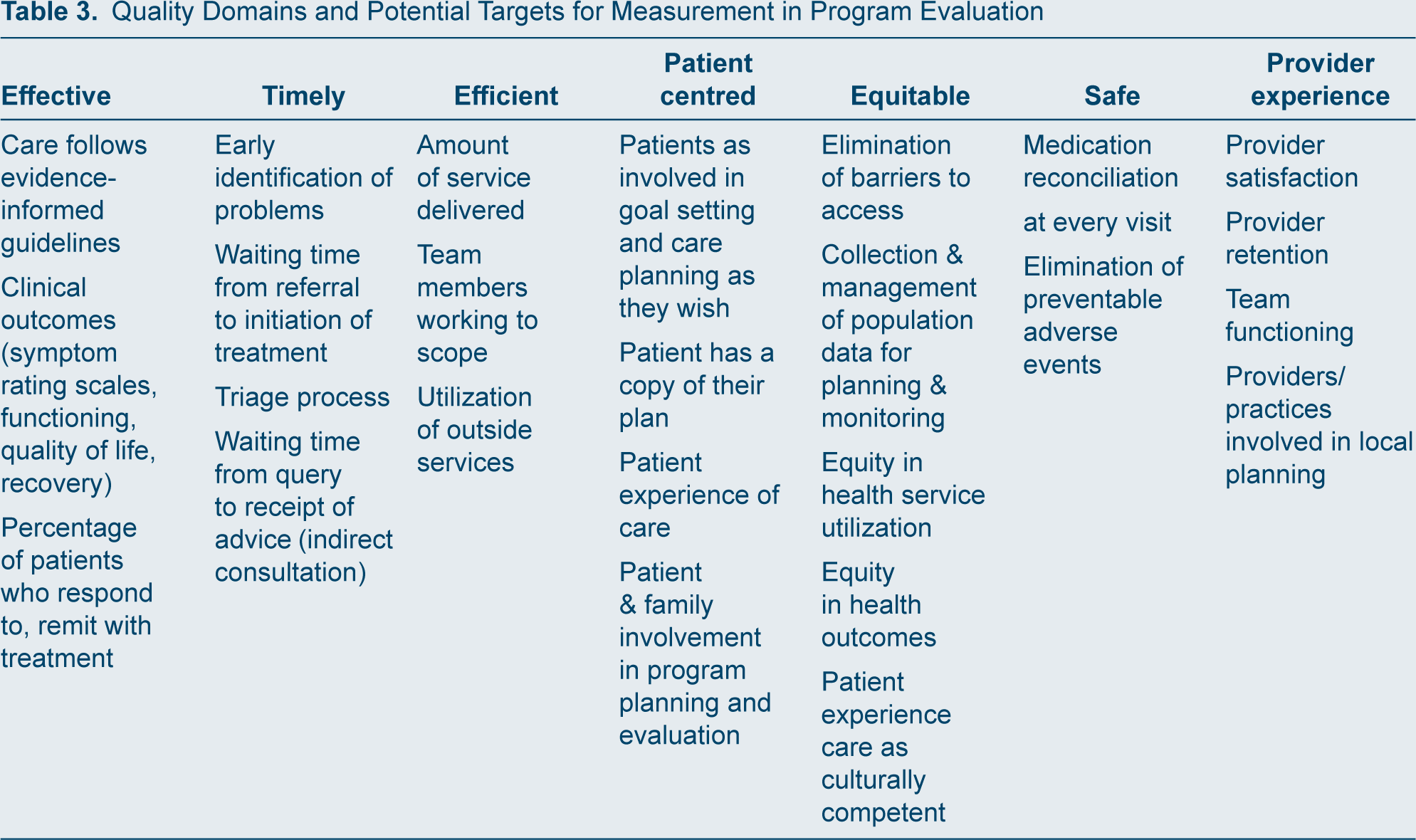
Evaluation materials should be easy to complete, use validated measurement tools wherever possible and balance quantitative and qualitative data. The areas being measured should fit within the domains of quality care (see Table 3), with each domain including a variety of process and outcome measures. Evaluation should be predominantly formative, allowing for iterative refinement and using small tests of change.
Quality Domains and Potential Targets for Measurement in Program Evaluation
Challenges
Despite the progress that has been made, challenges can arise.10,11,37,43,47,64,66,81,83,84 Insufficient resources may limit what a program can accomplish, so expectations, services, and priorities need to be adapted accordingly. Space may be at a premium, necessitating flexibility and often sharing, with mental health professionals having to adjust to working under different conditions from those to which they are accustomed.
Time constraints are frequently a factor and require compromise by everyone. Mental health professionals need to respect the multiple demands on family physicians, while the family physician needs to be willing to find time for case discussions, reviews, and other activities. These challenges are further exacerbated by both the shortage of family doctors and psychiatrists in many parts of Canada. It is also a style of practice that may not suit everyone, so assessing aptitude for this work and adequate preparation before starting are important.
A Vision for the Future
Looking ahead, we envisage well-integrated mental health and primary care network in each community in Canada with four components that complement and reinforce one another.
The first sees family physicians and other primary care professionals playing a growing role in delivering mental health care, even without the addition of new resources, by increasing the skills and capacity of the primary care sector to deliver “primary mental health care,” supported by the local mental health system.
The second is the building of stronger partnerships between all mental health and addictions services and their primary care colleagues, to both improve access to care and support and assist primary care to deliver effective mental health care.
The third element is the integration of mental health-care providers within primary care settings to improve access to high-quality mental health and addiction assessment and treatment and enhance the patient experience. Family physicians will then be better positioned to engage in earlier detection, relapse prevention and wellness promotion.
And finally, this redesigned system needs to be supported by (a) a funding strategy that supports successful ongoing projects and innovations, (b) provincial or territorial plans that outline clearly the role of primary care and CMHC within redesigned mental health and addiction systems, and (c) a training strategy to prepare all providers for new roles, especially psychiatry, and family medicine residents.
Potential to Address Other Challenges in the System
While not a “magic bullet,” mental health providers working in primary care can assist both the practice and the local system to address mental health problems that face every health care system. These can include:
Preventing avoidable emergency department visits through earlier intervention and relapse prevention. Improving transitions, especially from hospital to community and from youth to adult services. Supporting aging populations living with complex and chronic conditions. Reducing fragmentation and duplication of services and costs. Reducing errors and increasing patient safety. Meeting the needs of specific populations (rural and isolated communities, those who are living with opioid or other addictions, people from diverse cultural backgrounds). Improving preventive care, especially for children, including pro-active follow-up after the 18-month Well Baby visit.
Recommendations
Taking all the above into consideration, we are making the following recommendations:
Funding
The pool of health-care professionals from all disciplines who are funded to work in collaborative projects needs to be increased.
Physician funding models and billing tariffs need to change to support collaborative practice.
Funders should take into account the potential cost savings associated with successful CMHC (earlier recognition, less service duplication, reduction in preventable emergency department visits, less reliance upon other sectors such as child protection and justice systems) with their decision-making and planning.
Evaluation
Measurement and evaluation should be routinely included in collaborative projects—based upon a project’s goals—to demonstrate a program’s impact and its accountability for resource utilization.
Developing the Model
Models of CMHC need to be evidence-informed, team-based, stepped, shared, coordinated, person and family-centered, recovery-oriented and trauma-informed, and focused on populations as well as individuals.
Collaborative care must be culturally sensitive, relevant, and responsive to the needs of specific communities, including those who are marginalized, racialized, indigenous and underserviced, and counter racism and oppression.
The “reach” of CMHC can be increased through task shifting; the use of technology to promote access and coordination of care; and partnerships with community agencies.
Greater attention must be paid to transition between sectors and services, and direct communication about care plans.
Circles of care should include family members, care partners or informal supports as identified by the patient.
Collaborative care must address the mental and physical health consequences associated with adverse childhood events and recognize the role CMHC could play in mitigating the long-term consequences.
Front-line providers including family doctors and psychiatrists need to be involved in the planning and implementation of new models.
Social determinants need to be incorporated within collaborative projects, including appropriate housing, food security, and support for a meaningful activity or a return to the workplace.
Training
Psychiatry residents need to continue to receive training in CMHC within the new Competency by Design curriculum.
Family medicine residents will be expected to assess and manage patients with common behavioural, mental health, and substance use conditions and encouraged to engage in CMHC whenever possible and appropriate.
Expanding the Model
All mental health services should develop strategies for working more collaboratively with their local community by (a) improving communication and coordination of care with family doctors and primary care colleagues, (b) improving access, and (c) building the capacity of primary care.
Integration of family medicine within mental health teams and services to better meet the physical health of individuals living with severe and persistent mental health problems who don’t have access to a primary care provider.
System Integration
Local, regional, and provincial/territorial networks aimed at sharing information about what is working and how it can be spread should be established in these jurisdictions.
Research
The evidence base for CMHC should be broadened to include economic analyses; determinations of which populations and problems are best treated in which settings, key care processes to achieve good individual and population outcomes, and ways in which CMHC can address wider health system issues.