
Abstract
Background
Youth and young adults have been significantly impacted by the opioid overdose and health crisis in North America. There is evidence of increasing morbidity and mortality due to opioids among those aged 15–29. Our review of key international reports indicates there are few youth-focused interventions and treatments for opioid use. Our scoping review sought to identify, characterize, and qualitatively evaluate the youth-specific clinical and pre-clinical interventions for opioid use among youth.
Method
We searched MedLine and PsycInfo for articles that were published between 2013 and 2021. Previous reports published in 2015 and 2016 did not identify opioid-specific interventions for youth and we thus focused on the time period following the periods covered by these prior reports. We input three groups of relevant keywords in the aforementioned search engines. Specifically, articles were included if they targeted a youth population (ages 15–25), studied an intervention, and measured impacts on opioid use.
Results
We identified 21 studies that examined the impacts of heterogeneous interventions on youth opioid consumption. The studies were classified inductively as psycho-social-educational, pharmacological, or combined pharmacological-psycho-social-educational. Most studies focused on treatment of opioid use disorder among youth, with few studies focused on early or experimental stages of opioid use. A larger proportion of studies focused heavily on male participants (i.e., male gender and/or sex). Very few studies involved and/or included youth in treatment/program development, with one study premised on previous research about sexual minority youth.
Conclusions
Research on treatments and interventions for youth using or at-risk of opioids appears to be sparse. More youth involvement in research and program development is vital. The intersectional and multi-factorial nature of youth opioid use and the youth opioid crisis necessitates the development and evaluation of novel treatments that address youth-specific contexts and needs (i.e., those that address socio-economic, neurobiological, psychological, and environmental factors that promote opioid use among youth).
Introduction
The opioid overdose and health crises are complex and multi-factorial global challenges that impact several different populations. 1 Morbidity and mortality due to opioid use has been documented in North America and in particular in the US; however, Canadian researchers, policy makers, and healthcare professionals also navigate the challenges of reducing the harms of opioid use, specifically among adolescent and emerging adult populations (ages 15–25 years). In 2017, there were 3,987 opioid-related deaths and 20% occurred among the age group 20 to 29 years. 2 Over a recent 5-year period, younger adults had the fastest-growing rates of opioid poisonings. 3 The COVID-19 pandemic exacerbated these trends and a recent provincial study showed the greatest increase in opioid-related deaths among the under 35 age group. 4
Deaths occur not only among long-time substance users but among young people who have used them for the first time. 5 Media coverage has focused on the circulation of potent narcotics like fentanyl and the roles of pharmaceutical manufacturers in perpetuating opioid-related morbidity and mortality.6–8 Despite a popular emphasis on these factors, the (youth) opioid crisis can be understood as an interactive combination of non-actions 9 between opioid producers, medical care systems, government, and other crucial regulatory agencies and a biopsychosocial phenomenon that is inadequately addressed through an emphasis on drug supplies and pharmaceutical manufacturers’ practices. 10
The aforementioned non-actions have been compounded by an absence of Canadian epidemiological data about non-medical opioid use (NMOU) among youth. Provincial surveys (e.g., the Ontario Student Drug Use and Health Survey and the Canadian Tobacco, Alcohol, and Drugs Survey) have served as key indicators for understanding NMOU among youth.11,12 The OSDUHS survey showed that ∼11% of grades 7 to 12 students reported using prescription opioids non-medically and 20% reported it was easy or very easy to acquire access to prescription opioids. 11 These surveys suggest that NMOU rates have remained relatively stable since 2013, but the fact some youth are consuming prescription opioids non-medically is problematic for several reasons. Youth using heroin today are more likely to have initiated use via prescription opioids due to lower costs and greater accessibility 13 and some qualitative studies have shown that youth view prescription opioids as less dangerous or more socially acceptable than other illicit drugs, although perceptions vary with different opioids.14,15
Youth perceptions of opioids are contextualized by neurobiological vulnerabilities, familial, peer, and socio-structural risk factors, and contexts. Youth are more susceptible to impulsivity,16,17 sensation seeking and disregarding negative consequences, and to potential cognitive impairment due to substance use that can continue into emerging adulthood. 18 These vulnerabilities are contextualized by interactions with family members and peers, wherein diversion is thought to be ubiquitous. 19 Indeed, 40% of Canadian students who consumed a prescription opioid were given them by a parent. 19 A recent study showed that youth who live with a family member who have a prescription for opioids are at risk for overdose. 20 Peer, romantic, and/or sexual partners’ opioid use are also risk factors for youth and youth perceptions of opioid use behaviours among their peer groups are predictive of actual opioid use.21,22 Homelessness, trauma, and socio-economic status (SES) are also key contextual risk factors, particularly for opioid use. 13 Canadian youth with low SES are 2.4 times more likely to report using prescription pain relievers (e.g., opioids) than a youth of higher SES. 23
Recent reports published in 2016 24 and 2015 25 noted there were few opioid-specific interventions for young people and most interventions have focused on alcohol, cannabis, and other illicit substances. The only programs that resulted in reduced use of prescription opioids for young people were the PROSPER framework and a personality-targeted intervention.18,26,27 A narrative review of pharmacological treatments for adolescents with opioid use disorder (OUD), discussed the efficacy and risks of various treatments. 28 Across all three reviews, studies were predominantly from prior to 2013.
Due to continuing opioid-related harms to young people in Canada, it is crucial to know what is helpful for preventing and treating opioid use and to determine whether additional solutions have been identified since the publication of the reports. The objectives for this scoping review were to identify novel and promising interventions for youth who are currently using or at-risk for opioid use and to characterize and evaluate the evidence in favour of these treatments. Our review expands on the previous reports and review, as we utilized a systematic search strategy and focused broadly on psychological and pharmacological interventions. To date, there have been no systematic reviews of this kind in the domain.
Methods
Search Strategy
Our objective was to understand the characteristics of youth-focused novel treatments, the multiple ways they are studied, and their impacts on opioid use. We thus adopted a scoping methodology. 29 We searched MedLine and PsycInfo for English studies that were published between 2013 and 2021 to capture interventions that were not included in the international reports.24,25 We input three groups of keywords that captured population, opioid use, and interventions.
The results were imported into EndNote. Titles and abstracts were screened by a research assistant (RA) and a PhD student independently. Full texts were subsequently screened by an RA and a PhD student. If there were discrepancies about whether studies should be included, both reviewers discussed the articles and consulted with the executive team to determine whether the articles should be included. The reference lists were screened to identify additional studies.
Inclusion/Exclusion Criteria
The inclusion criteria were: (1) The study focused on a youth population (15–25 years of age as per the Surgeon General's report 24 ) or youth sub-sample; (2) The study had to include an intervention; (3) The study had to measure impacts on opioid use or high-risk substance use (e.g., methamphetamine, cocaine, or polysubstance use). We excluded studies that focused on adults, that measured outcomes only for other substances (e.g., cannabis), and/or that referenced opioid use but not an intervention. Non-peer-reviewed studies were not included.
Data Charting & Analysis
Data were extracted from the studies regarding the classification of drug use within samples, sample age range and/or mean, the study's focus (e.g., treatment of OUD), the study design (e.g., RCT), the methodologies used to gather data, opioid-specific outcomes, the sample size, the gender and/or sex of the participants, and the geographical location. Each variable was recorded in an excel spreadsheet by an RA and a PhD student.
Results
Combined searches of MedLine and PsycInfo resulted in 1,188 articles. Duplicates were removed (n = 75). The title and abstract scans resulted in the exclusion of 1,044 references. Sixty-nine full texts were screened for inclusion. Fifty-one articles were excluded after the full-text review and 18 were retained for qualitative synthesis. Three articles from citation searching were included, for a total of 21 studies (Figure 1).
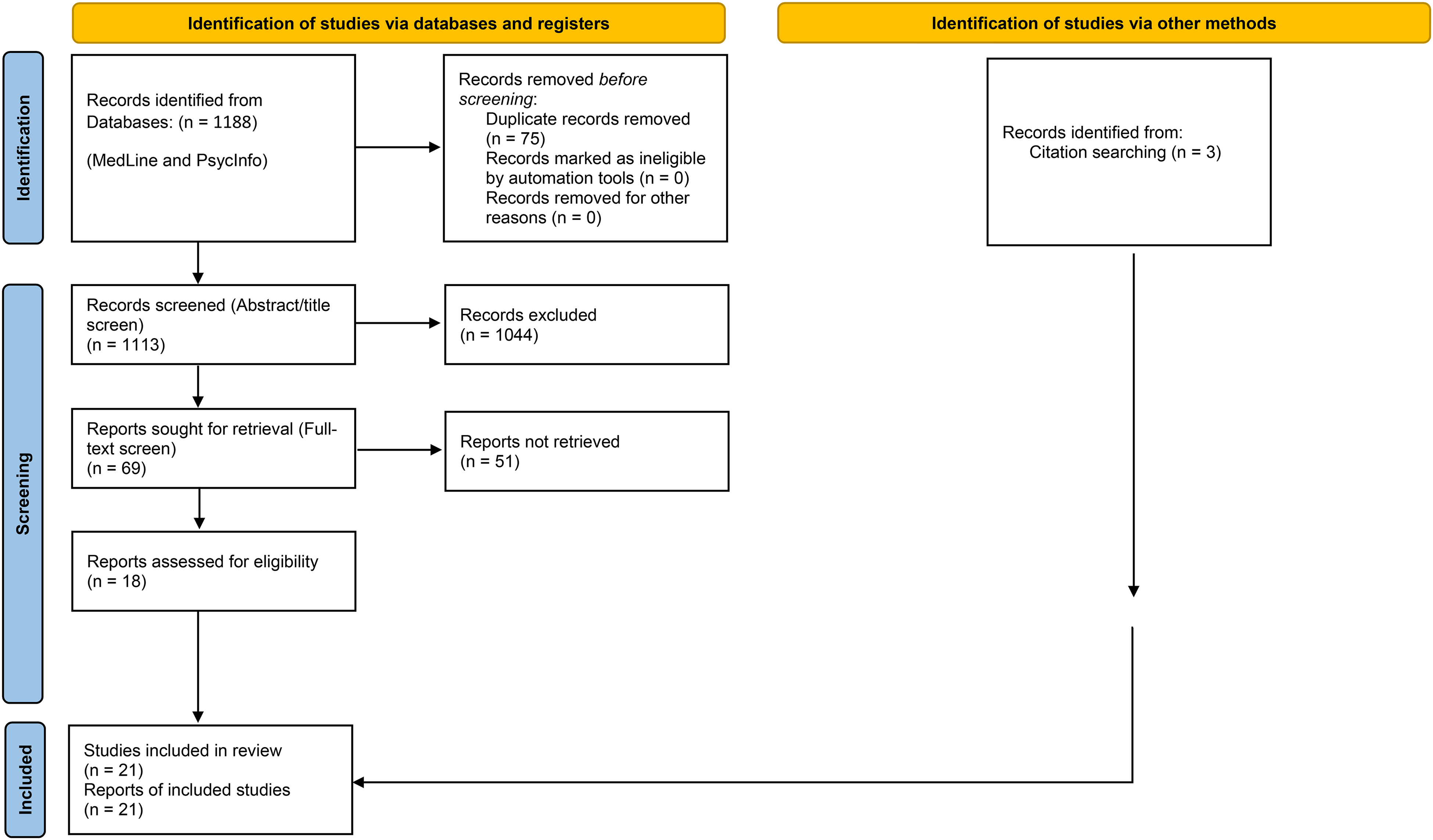
PRISMA flow chart for scoping review.
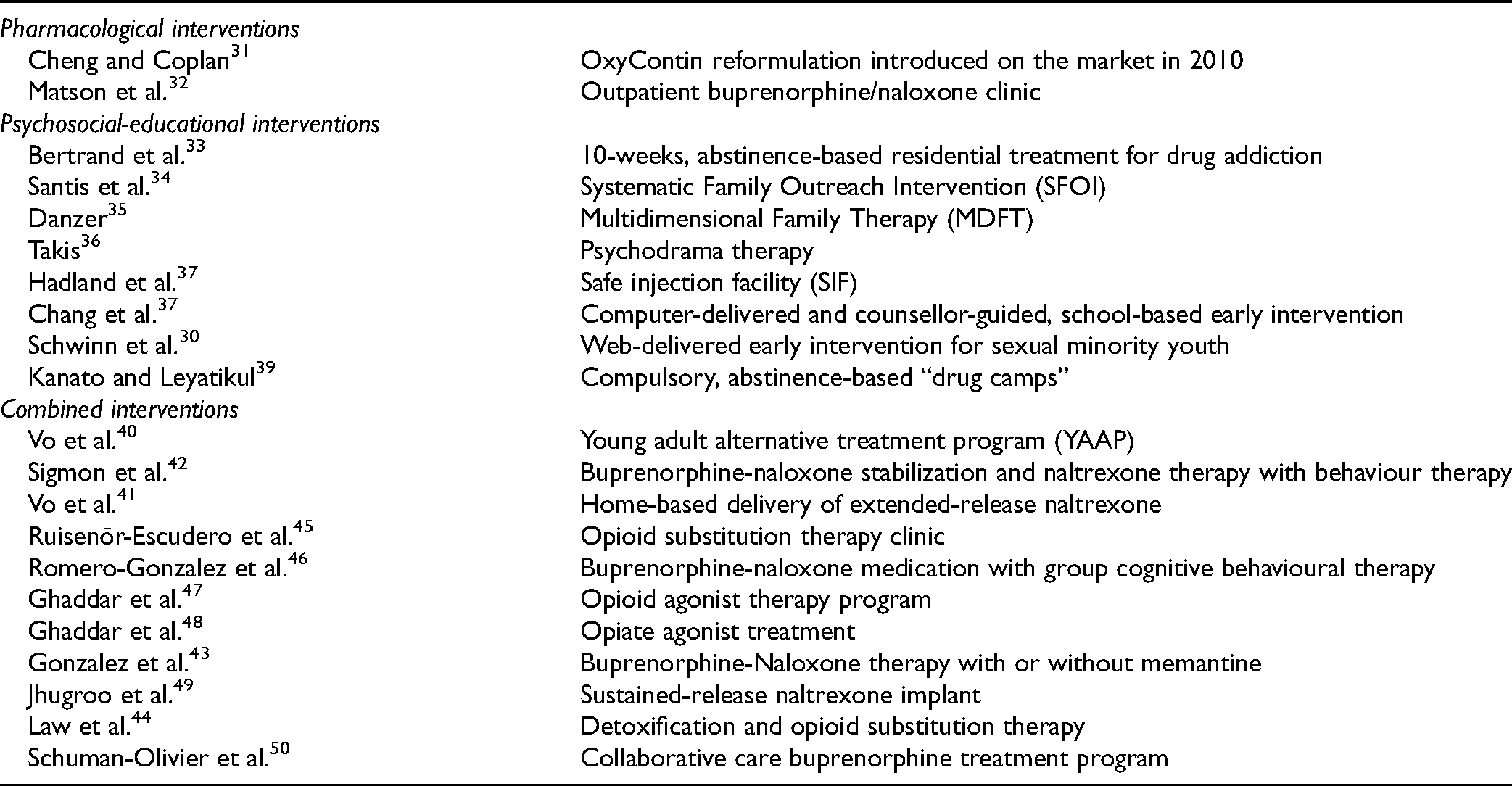
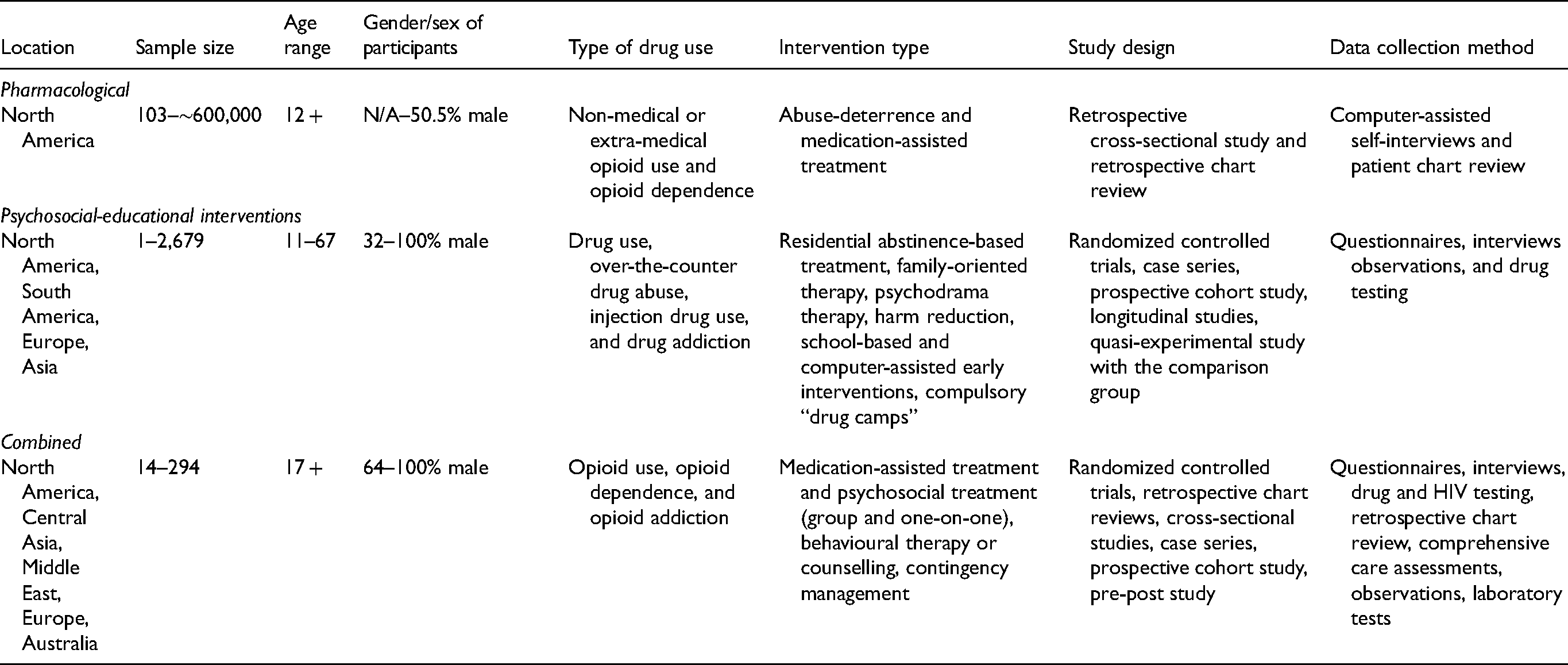
The 21 studies were categorized inductively based on the types of studies. Two were classified as pharmacological, 8 were classified as psycho-social-educational, and 11 were classified as combinations of pharmacological-psycho-social-educational studies (Table 1).
Interventions for Young Opioid Users Identified in the Literature.
Sample Characteristics
Ten studies recruited youth from the US, 2 from Canada, 2 from Lebanon, and 7 studies were from other countries (see Table 2). All study samples had either a mean age between 15 and 25 years (n = 17) or highlighted youth-specific findings, despite a slightly higher average age among the total sample (n = 4). A total of 17 of the 21 studies focused disproportionately on male participants (e.g., a sample that incorporated over 50% male participants) or exclusively on the treatment of male participants. One study purposively recruited a sample of “sexual minority youth” 30 (i.e., queer, gender fluid, and/or “other” genders) alongside women and men. Eight studies reported gender as binary (i.e., male or female). Two studies did not report sample sex or gender, 6 reported on “male” and “female” participants or “men” without referring to whether the status was regarded as sex or gender, and three studies reported “sex.”
Characteristics of Included Studies.
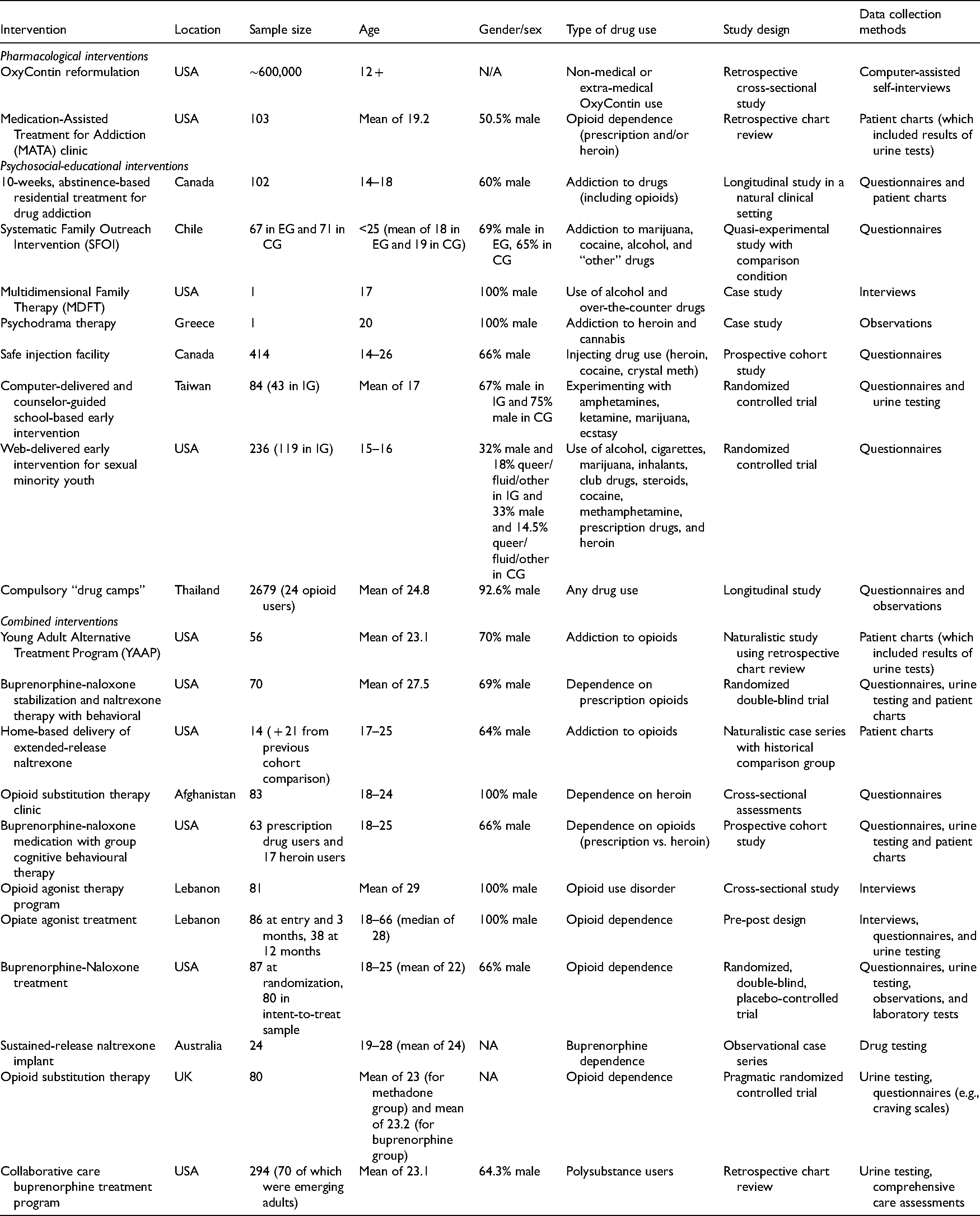
The classification of opioid and other drug use among the samples was heterogeneous. In the pharmacological studies, opioid use was defined as non-medical or extra-medical OxyContin use and opioid dependence. In the psycho-social-educational interventions, youth were classified as “addicted to opioids” and “other drugs,” youth using drugs (e.g., cocaine, methamphetamine, prescription drugs, and heroin), injecting drugs (e.g., heroin, cocaine, and crystal meth), and experimenting with amphetamines. Youth were primarily engaged in prescription opioid (PO) use and/or experienced OUD, or were “experimenting.” In the combined interventions, youth were “addicted to opioids,” “dependent on prescription opioids,” “dependent on heroin,” buprenorphine dependent, seeking buprenorphine treatment, or had OUD.
Characteristics of Study Designs
Pharmacological Interventions
One pharmacological study was a retrospective, cross-sectional study in the US and assessed the incidence of non-medical opioid use before and after the introduction of abuse-deterrent OxyContin in 2010 with an oversampling of youth 12 to 17 years. 31 The additional pharmacological study was a retrospective chart review of adolescents who sought treatment at a Medication-Assisted Treatment for Addiction clinic (MATA). The clinic provided outpatient buprenorphine/naloxone to youth (ages 14–25 years) and helped “manage” other medical and mental health conditions. All participants were prescription opioid-dependent or combined heroin/prescription-opioid dependent. 32
Psycho-Social-Educational Interventions
Youth in the psycho-social-educational studies were younger than youth in the pharmacological/combined interventions and there was a heterogeneity of study designs and methods to impact opioid use and other substance use.
One study was longitudinal and assessed a residential treatment program. 33 A total of 65% of the sample used both alcohol and other drugs, including heroin, opiate, analgesics, “narcotics,” methamphetamine/speed, and cocaine. Another study examined a Systematic Family Outreach Intervention (SFOI) 34 and incorporated a quasi-experimental design and a comparator group (i.e., traditional outreach work). Participants were recruited from “communes” with low-income populations, high rates of substance use and drug trafficking. Approximately 75% of the sample were polysubstance users including alcohol, marijuana, cocaine, and “other” drugs.
Two psycho-therapeutic case studies involved Multidimensional Family Therapy (MDFT) 35 and psychodrama therapy. 36 MDFT involved counselling sessions with the participant and his family members. They were living in a low-income household and the participant had a history of alcohol use and an overdose on over-the-counter substances. There was weekly drug testing. The psychodrama case study involved a participant using heroin and cannabis and included weekly group sessions and one-on-one counselling. His family dynamic was described as “hostile” and “dysfunctional.”
The At-Risk Youth Study (ARYS) was a prospective cohort design and assessed youth use of a Safe Injection Facility (SIF). 37 Participants were street-involved and injected heroin and crystal meth. The population was described as at-risk for morbidity and mortality.
Additional psycho-social-educational studies were computer/web-delivered interventions. The computer-delivered and counsellor-guided intervention 38 was an RCT and completed in schools with youth experimenting with amphetamines, marijuana, ketamine, and ecstasy; 50% reported substance use (SU) among their peers. The web-delivered intervention was also an RCT and targeted sexual-minority youth using alcohol, cigarettes, marijuana, and other drugs (cocaine, methamphetamines, prescription drugs, and heroin). The self-report questionnaires implemented at pre-, post-, and 3-month follow-up recorded information on peer SU. 30
A longitudinal study from Thailand examined compulsory “drug camps” with youth using drugs. 39 The camps were standardized, 9-day rehabilitation programs involving recreational and boot camp activities, drug resistance education, “drug abuse rehabilitation procedures” and occupational training. Drug use and demographic questionnaires were completed by participants. Participant observation procedures were also used. Less than 1% of camp attendees reported using opioids prior to camp and most attendees were amphetamine, alcohol, and polydrug users (31%).
Combined Pharmacological-Psycho-Social-Educational Interventions
The combined studies analyzed variations of Opioid Agonist Therapy (OAT) alongside several psycho-social-educational modalities. Seven of the 11 studies assessed combinations of buprenorphine treatments and other pharmacological and psychosocial adjuncts. There was a heterogeneity of study designs and all studies involved outpatient treatment(s), with one study providing the option to remain in inpatient treatment, before transitioning to outpatient treatment. The combined studies assessed primarily males/men, ranging from 64% to 100% male representation.
A naturalistic and retrospective chart review of 56 patients explored the Young Adult Alternative Treatment Program (YAAP) that provided youth with the option of taking buprenorphine or extended-release naltrexone. 40 Participants had access to counselling, mental health therapy, and psychiatric treatment. Participants had an OUD and were polysubstance users; 89% had a psychiatric diagnosis and 82% injected heroin.
An additional naturalistic study compared home-based delivery of extended-release naltrexone (XR-NTX) by a nurse practitioner with those who had received clinic-based delivery of the same medication in the previous year. 41 The community-based program involved residential detoxification and a 7-day buprenorphine taper for adolescents and young adults with opioid addiction to prescription opioids and heroin; 64% of the participants injected heroin. Youth were invited to continue inpatient treatment before transitioning to outpatient treatment. The youth had the option of receiving counselling at home.
An outpatient double-blinded RCT assessed the effects of a combination of buprenorphine hydrochloride and naloxone hydrochloride dihydrate via 1-, 2-, or 4-week tapers. Participants were dependent on prescription opioids, 41% had used the intravenous route at least once and 89% were polysubstance users. Participants were provided with individual behavioural therapy. 42 The sample had high rates of employment, education, and low rates of medical and psychiatric problems.
An additional 13-week double-blinded RCT compared treatment of opioid-dependent young adults with buprenorphine-naloxone or placebo with 15 or 30 mg of memantine. All participants were offered weekly group cognitive-behavioural therapy. 43
An additional RCT compared the efficacy of lofexidine/methadone and buprenorphine/naloxone during opiate withdrawal following opiate stabilization on methadone and buprenorphine/naloxone among opioid-dependent users. 44 The study included medical/general health questionnaires, physical examinations, and blood tests. The participants were stabilized daily, followed by detoxification. Participants were then treated with either lofexidine/methadone or buprenorphine/naloxone. Vouchers for local grocery stores were provided and this was contingent on opioid negative urine, attendance, and completion of questionnaires.
Two additional studies incorporated prospective cohort designs and assessed variations of OAT. One study included injecting male heroin users and combined methadone with psychosocial therapy, education, recreational, and medical services. 45 Another study assessed buprenorphine-naloxone doses over an 8-week period, after opioid-dependent youth were abstinent from either heroin or prescription opioids. 46 Youth could attend weekly group cognitive behavioural sessions. The participants had employment problems and were likely to be depressed.
An additional cross-sectional study of young men with OUD attending an OAT program 47 integrated psychiatric and psychological care, as well as provided access to a nurse and social worker. A longitudinal study by the same researchers and a different cohort examined the effects of OAT and psychosocial support on opioid-dependent males at the first outpatient community-based treatment centre in Lebanon. 48
An observational case series of 24 opiate-dependent participants evaluated the effects of a double naltrexone implant treatment. Patients travelled from Mauritius to Australia to undergo surgery and follow-ups were done in Mauritius. Patients were provided with 20 min of brief counselling. 49
A retrospective chart review examined opioid-dependent emerging adults’ experiences of a collaborative care buprenorphine treatment program. 50 The program consisted of brief detoxification and buprenorphine induction. The participants were required to attend weekly one-on-one or group psychosocial treatment sessions. A total of 81.4% of the participants reported lifetime use of heroin.
Outcomes of the Studies
Pharmacological Studies
The study examining the incidence of non-medical OxyContin use before and after the abuse-deterrent formulation was released in 2010, showed that there was a 50% reduction in new incidences of OxyContin use between 2010 and 2012 for youth aged 12 to 21 years. However, the same trend of reduced incidence was not observed for youth's NMOU of other prescription opioids (see Table 3 for study outcomes). 31
Outcomes of Included Studies.
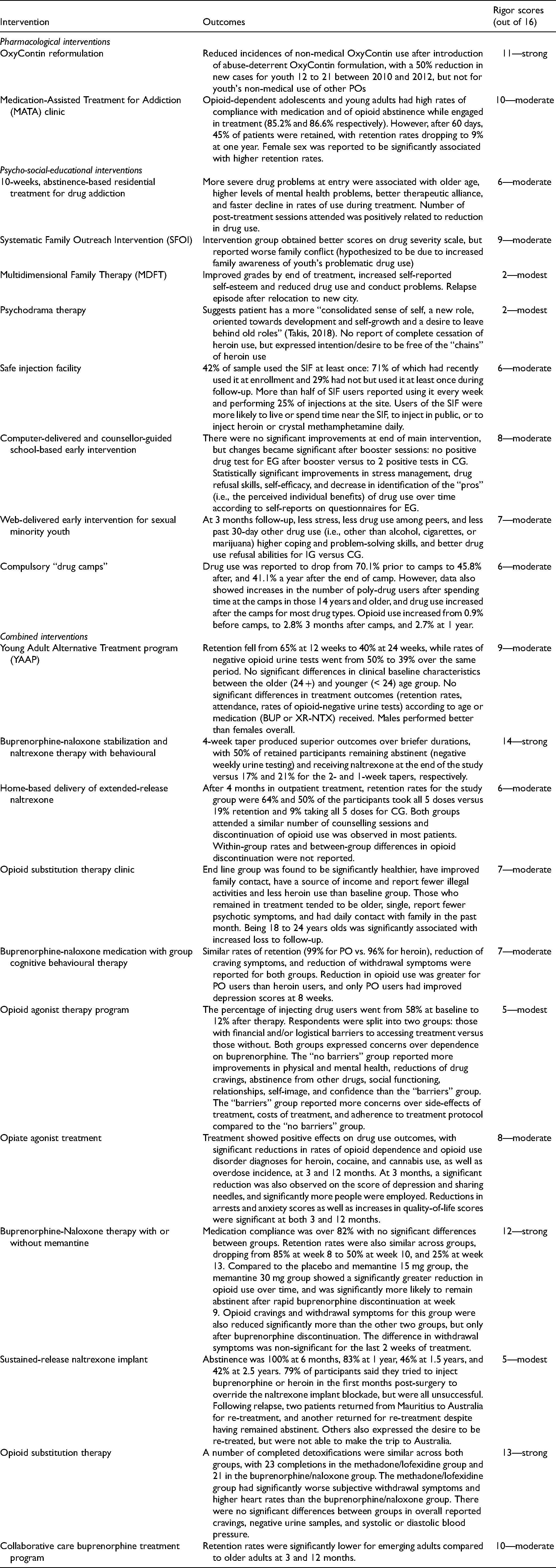
The MATA study indicated that missing urine drug screening rates were low and buprenorphine-naloxone compliance rates and opioid abstinence rates were high while youth were engaged with the clinic. Retention was a major barrier to the success of treatment; 75% returned for a second visit, after one visit, at 2 months, 45% of patients were retained and at 1 year, 9% of patients were active in the program. The authors noted that the female sex was associated with higher retention. 32
Psycho-Social-Educational Interventions
Results of the 10-week residential treatment 33 demonstrated that youth with the most severe drug problems at entry were usually older and experienced the fastest decline in SU during treatment. Higher levels of mental health problems and better therapeutic alliance were associated with higher severity of SU problems at entry. The number of post-treatment sessions attended was positively associated with reductions in SU. Past 30-day heroin, opiate, narcotic, and analgesic drug use were reported and showed a reduction between entry and the 3-month follow-up, with an observed increase at the 6-month follow-up.
The SFOI study 34 demonstrated the intervention group obtained better scores on the addiction severity scale compared to control (traditional outreach work) but reported worse family conflict.
The MDFT case study reported improved grades, increased self-esteem, reduced drug use, and conduct problems, and a relapse episode when he relocated to a new city. 35 The psychodrama case study reported a more “consolidated sense of self, a new role oriented towards development, self-growth and a desire to leave behind old roles” (p. 341). 36 The report also mentioned the participant's desire to be free of the “chains” of heroin use.
A total of 42% of the participants in the SIF 37 study used the facility at least once, and 71% of participants used it around the time of enrollment in the study. More than half of SIF users used it every week and performed 25% of their injections at the site. SIF use was associated with daily heroin injection, daily cocaine injection, and having visited a crack house or shooting gallery.
The computer-delivered intervention 38 resulted in zero positive urine tests (i.e., for use of amphetamines, ecstasy, ketamine, and cannabis) only after the booster sessions, compared to 2 positive urine tests in the control group. Inferential statistics to determine statistical significance were not provided due to a large number of cell counts at zero. The experimental group showed statistically significant improvements in comparison to the control group in stress management, drug refusal skills, self-efficacy, and a decrease in the identification of the ‘pros’ of SU after the boosters.
The web-delivered intervention for sexual minority youth 30 resulted in less stress, less SU among peers, less past 30-day other SU (i.e., use of heroin, methamphetamines, inhalant, club drug, steroid, prescription drugs, and cocaine), higher coping and problem-solving skills, and better drug refusal abilities than the control groups.
The results of the compulsory drug camps 39 were changes in current use from 70.1% before the camps, to 45.8% after the camps, and 41.1% 1 year after the camps. The decrease was accounted for via significant reductions in amphetamine-type stimulant use only. The authors noted that drug use increased for most drug types, including opioids, after the camps (i.e., for opioids from 0.9% before, to 2.8% 3 months after and 2.7% after 1 year). They noted that data from a community study (not cited) showed that many camp attendees became polysubstance users after the camps.
Combined Pharmacological-Psycho-Social-Educational Interventions
The YAAP study 40 reported reduced retention rates over time from 65% at 12 weeks to 45% at 24 weeks. No significant differences in baseline characteristics were observed between older (over 24 years) and younger (under 24 years) youth or in treatment outcomes (i.e., retention rates, attendance, rates of opioid-negative urine tests) according to age or medication (BUP or XR-NTX) received. More males than females completed the program.
The 4-week taper of buprenorphine-naloxone produced superior outcomes when compared to briefer tapers in the combined buprenorphine-naloxone, naltrexone, and behavioural therapy study. 42 Indeed, 50% of retained participants in the 4-week taper remained abstinent from opioids after 12 weeks in comparison to 17% and 21% for the 2- and 1-week tapers, respectively. A total of 50% of 4-week taper participants were also receiving naltrexone at the end of the study, compared to 17% for the 2-week taper and 25% for the 1-week taper group. The difference in naltrexone ingestion between the 4-week group and the 2-week group was significant.
After 4 months in outpatient treatment, the home-delivery of ER naltrexone resulted in 64% retention, in comparison to 19% in the control. A total of 50% of the participants in the experimental group took all 5 doses, in comparison to 9% in the control. 41 Both groups attended a similar number of counselling sessions. Seven of the 9 patients in the experimental group were abstinent from opioids at 4 months. Controls were not assessed for opioid abstinence precluding direct comparisons.
At end-line, male youth enrolled in the OST study were shown to be significantly healthier, have improved family contact and a source of income, report fewer illegal activities and have less heroin use compared to baseline participants. 45 They were also more likely to be single, older, report fewer psychotic symptoms, older age at first heroin use, and in the past month, have greater daily contact with family.
The study of buprenorphine-naloxone medication with group cognitive behavioural therapy for heroin users in comparison to PO users, showed similar rates of retention for both groups. 46 A statistically significant difference was observed in weekly urine toxicologies; 99% of PO users were negative in comparison to 96% of heroin users over 8 weeks. Reductions in craving and withdrawal symptoms were similar in both groups. Reduction in opioid use was greater for PO users than heroin users and only PO users had improved depression scores at 8 weeks.
The study that assessed young men attending OAT defined participants as those with financial barriers and those with no financial barriers to access. 47 Men with no barriers reported more social, physical, and mental benefits of participation including reduced cravings, improved social standing, relationships, and mental health. Both groups worried about dependence on OAT and participants with barriers expressed concerns about treatment benefits. The therapy reduced injecting behaviour from 58% to 12% after the therapy in both groups.
The longitudinal study of the Lebanese OAT clinic showed reduced rates of opioid dependence, overdose incidences at 3 and 12 months, and OUD diagnoses for heroin, cocaine, and cannabis users. At 3 months, a significant reduction was observed in depression scores, needle sharing, and more participants were employed. The reductions in arrests, anxiety scores, and increases in quality-of-life were significant at 3- and 12-month follow-ups. 48
In the double-blinded RCT comparing buprenorphine-naloxone with either placebo, memantine 15 or 30 mg, 82% of participants were compliant with medication. Retention rates were similar in both groups; 85% were retained at week 8, 50% at week 10, and 25% at week 13. The 30 mg group showed a greater reduction in opioid use over time and were more likely to remain abstinent after rapid buprenorphine discontinuation. The 15 mg group did significantly worse than the other 2 groups with regards to reductions in opioid use at weeks 5 and 8. 43
Analysis of the naltrexone implant 49 showed that abstinence from opioid use was 100% at 6 months, 83% at 1 year, 46% at 1.5 years, and 42% at 2.5 years. A total of 79% of participants tried to inject buprenorphine or heroin post-surgery, but all were unsuccessful. Two patients returned to Australia for re-treatment, and another returned for re-treatment despite having remained abstinent. Other participants expressed desires to be re-treated but could not make the trip to Australia.
The collaborative care buprenorphine treatment program demonstrated that emerging adults had lower retention rates than adults at 3 and 12 months. 50
The RCT comparing buprenorphine/naloxone and methadone/lofexidine 44 reported that 44 out of 80 youth successfully completed detoxification. There were no significant differences between the groups who completed detoxification and no significant differences reported in overall reported craving, the proportion of negative opioid urine samples, or systolic or diastolic blood pressure. The methadone/lofexidine participants had significantly worse levels of subjective withdrawal symptoms and higher heart rates than the buprenorphine/naloxone group.
Synthesis of the Results of the Literature Search.
Discussion
Of the total number of studies, we found very few targeted adolescents and young adults (Table 4). The studies that targeted youth were heterogeneous pharmacological, psycho-social-educational, and combined interventions that varied with regards to the samples, the types of interventions and the outcomes reported and achieved.
A notable finding was that almost all of the youth-focused interventions were not tailored a priori to specific youth populations. The intervention for sexual minority youth 30 was the only study that was both tailored a priori through content and practice scenarios to the needs of a potentially marginalized youth population and involved a substantial proportion of (50%) women, queer, and gender-fluid participants. The majority of other studies enrolled over 60% of male participants. This is problematic as the evidence demonstrates young women are uniquely vulnerable to NMOU. They are more likely than men to be prescribed an opioid and to consume opioids for pain relief. Trans and other gender diverse youth are vulnerable to opioid use and were not included in the studies. Future studies could purposively recruit women, gender diverse youth, and integrate youth-tailored materials in interventions to improve treatment relevance and efficacy.
The studies we found focused on the treatment of youth who are already experiencing dependence. This could be due to the limitations of our search terms or indicate a lack of preventive programs for youth in the experimental stages of OU. The computer-delivered intervention in schools was an exception because it focused on youth “experimenting” with substances. 38 Given the frequency of polysubstance use and the improvements observed in stress management, refusal skills, and self-efficacy, the results were nonetheless encouraging. Healthcare professionals should develop and evaluate preventative programs aimed at youth experiencing problems as they explore opioid use.
The majority of studies focused on treatment retention outcomes. Three studies noted older youth had higher retention and faster declines in rates of opioid use during (combined) treatments.33,45,50 The YAAP study found no differences between older and younger participants in retention or reductions in opioid use. 40 Reduced retention over time in several studies may indicate that retention is a barrier to experimental treatment success. The MATA study noted that female sex was associated with higher retention, but this was not reflected on by Matson et al. 32 There is a need to develop an in-depth understanding of factors that promote retention and of how to engage youth throughout the duration of the programs.
The guiding principle of several studies was abstinence from opioids or reductions in use. This may be a deterrent to youth enrollment, as abstinence all the time is often unrealistic. The use of abstinence-based “camps” in Thailand 39 is an example of the abysmal failures of compulsory and abstinence-based approaches for young people. Within a paradigm of harm reduction, the goals of the interventions could include continued safer use to prevent iatrogenic effects of treatments.
The youth opioid overdose and health crises are multi-factorial and we found that consideration of socio-structural factors were not explicitly integrated into the study methodologies, yet were illustrated in more detail in the results. The psychodrama 36 case study referred to the participant’s “hostile” family dynamic, family members were counselled in the MDFT 35 and involved in the SFOI. 34 The involvement of family requires careful consideration as youth reported worsened family conflict after the SFOI and improved family relations after the MDFT. With regards to peers and partners, the intervention for sexual minority youth 30 was the only study that reported reduced peer substance use. Future studies could focus on integrating peers and romantic partners in treatments.
SES was also addressed in the results of some of the studies but was not discussed explicitly a priori. The MDFT, 35 SIF, 37 and SFOI 34 studies recruited youth with low SES and/or who were street-entrenched. Financial factors were mentioned in the results of the 2 studies. Young men in OAT with no financial barriers experienced more benefits than men with financial barriers, suggesting this factor can negatively influence the ability to benefit from OAT. 47 Prescription opioid users in the Sigmon et al. 42 study had high rates of education and employment, which suggests OU and related harms transcends SES and confirms opioid users can come from a variety of backgrounds. One study 44 surmised that contingency management promoted high treatment attendance rates and healthcare professionals could integrate novel approaches like contingency management in treatments of OUD for youth and consider their economic circumstances in the design of interventions.
It was promising to find studies that provided choices for youth within treatments.40,41,45–47 Several studies offered options to participate in counselling, but most studies did not report on whether/how often these options were taken up. It was impossible to discern how they may have differentially impacted the outcomes and going forward researchers should, in collaboration with youth, characterize the impacts of the various combined treatments on study outcomes.
Limitations
We did not develop a search around individual-level risk factors, which could be a strategy to identify additional interventions. Hopelessness is linked with OU among high school and college students, 51 and adult substance users 52 including those in OAT for OUD. Interventions targeting hopelessness have been shown to reduce SU. 32 Similarly, youth living with parents who are prescribed opioids are at risk of exposure to opioids and potential future overdose. 20 Our research was not able to identify interventions for these at-risk youth.
Conclusion
Canadian youth continue to be a vulnerable group in the opioid overdose and health crisis. The evidence base for opioid use treatments among youth is lacking in North America and elsewhere in the world. The studies we found were not tailored to youth-specific socio-ecologies. The heterogeneity of youth experiences with opioids in North America may indicate that traditional approaches to treatment are not attuned to youth-specific intersecting vulnerabilities and contexts.
Within the context of current experimental interventions, we need a greater emphasis on understanding the factors that promote retention among young people, concerted efforts to include young women and gender diverse youth in treatments, programs that assess continued safer use within a paradigm of harm reduction, programs that focus on prevention of opioid use and address youth socio-economic positionalities, and treatment evaluation that seeks to “success” in these programs.
We argue researchers and healthcare professionals can cultivate youth-adult partnerships wherein they can systematically solicit youth feedback about interventions and treatments to improve treatment relevance and efficacy. There clearly needs to be a greater emphasis on understanding and identifying the factors that promote youth participation in opioid use programs and on authentic engagement with youth values and needs. 8
Footnotes
Acknowledgments
We gratefully acknowledge several individuals who contributed to the development of this manuscript including, Dr Ranmalie Jayasinha who offered their generous guidance on the scoping review process. We thank Rodney Stehr who contributed to the initial screening process and procedures. We thank Caroline Mniszak and Nikki Tummon who assisted with the database searches. We also thank the CRISM team members for their ongoing support and feedback on the review process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research (grant no. OCC-154893).
Appendix
Search Terms:
young adult.mp. or Young Adult/
(youth* or adolescen* or teen*).ti,ab.
Drug Users.mp. or Drug Users/
(opiate* or opioid* or heroin*).ti,ab.
Analgesics, Opioid.mp. or exp Analgesics, Opioid/
exp Morphine Derivatives/
exp Prescription Drug Misuse/
exp Opioid-Related Disorders/
exp Street Drugs/
exp Drug Misuse/
(abus* or addict*).ti,ab.
drug inject*.ti,ab.
polydrug*.ti,ab.
Risk Factors/
Health Promotion/
health services/ or adolescent health services/ or community health services/ or emergency medical services/ or health services for transgender persons/ or health services, indigenous/ or mental health services/ or nursing care/ or nursing services/ or patient care/ or pharmaceutical services/ or preventive health services/ or rehabilitation/ or rural health services/ or social work/ or student health services/ or suburban health services/ or urban health services/ or women's health services/
"Early Intervention (Education)"/
preventive health services/ or "early intervention (education)"/ or early medical intervention/ or health education/ or needle-exchange programs/ or primary prevention/ or school health services/ or secondary prevention/ or tertiary prevention/
preventative health services.mp.
Harm Reduction/
Opiate Substitution Treatment/
Methadone/
Narcotic Antagonists/
exp Morphinans/
Substance Abuse Treatment Centers/
exp Psychotherapy/
(psychother* or psychosocial).ti,ab.
counseling.ti,ab.
opioid crisis.ti,ab.
opioid epidemic*.ti,ab.
adolescence.mp. or Adolescent/ or Adolescent.mp.
(codeine* or fentanyl or actiq or duragesic or fentora or hydrocodone or hysingla er or zohydro er or acetaminophen or lorcet or lortab or norco or vicodin or hydromorphone or dilaudid or exalgo or meperidine or demerol or methadone or dolophine or methadose or morphine or astramorph or avinza or kadian or ms contin or ora-morph sr or oxycodone or oxycotin or oxecta or roxicidone or percocet or endocet or roxicet or targiniq er).ti,ab.
4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 32
15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30
((drug* or substance* or opioid*) adj2 (abuser* or addict* or user*)).ti,ab.
((recreational or casual) adj2 (drug* or substance* or opioid*) adj2 (abuser* or addict* or user*)).ti,ab.
1 or 2 or 31
3 or 35 or 36
37 and 38
39 and 33 and 34
limit 40 to (english language and humans and yr="2013 - 2021")