
Abstract
Background
Compared to treatment as usual (TAU), early psychosis intervention programs (EPI) have been shown to reduce mortality, hospitalizations and days of assisted living while improving employment status.
Aims
The study aim was to conduct a cost-benefit analysis (CBA) and a cost-effectiveness analysis (CEA) to compare EPI and TAU in Canada.
Methods
A decision-analytic model was used to estimate the 5-year costs and benefits of treating patients with a first episode of psychosis with EPI or TAU. EPI benefits were derived from randomized controlled trials (RCTs) and Canadian administrative data. The cost of EPI was based on a published survey of 52 EPI centers in Canada while hospitalizations, employment and days of assisted living were valued using Canadian unit costs. The outcomes of the CBA and CEA were expressed in terms of net benefit (NB) and incremental cost per life year gained (LYG), respectively. Scenario analyses were conducted to examine the impact of key assumptions. Costs are reported in 2019 Canadian dollars.
Results
Base case results indicated that EPI had a NB of $85,441 (95% CI: $41,140; $126,386) compared to TAU while the incremental cost per LYG was $26,366 (95% CI: EPI dominates TAU (less costs, more life years); $102,269). In all sensitivity analyses the NB of EPI remained positive and the incremental cost per LYG was less than $50,000.
Conclusions
In addition to EPI demonstrated clinical benefits, our results suggest that large-scale implementation of EPI in Canada would be desirable from an economic point of view .
Introduction
Psychotic illnesses result in impairment in reality testing, social and vocational functioning in people affected from them. The first episode of psychosis occurs generally between the ages of 15 and 30 years 1 and the incidence of first episode of non-affective psychosis has been reported in Ontario as 33.3 per 100,000 per year. 2 Early psychosis intervention programs (EPI) programs consist of multidisciplinary teams providing rapid psychiatric assessment and follow-up for youth aged typically 16 to 35 (criteria can vary by program) and include an array of psychosocial interventions (e.g., case management, family interventions).3–6 Several randomized controlled trials (RCTs) have shown that EPI was associated with better outcomes than treatment as usual (TAU) (e.g., in terms of hospitalizations, remission, involvement in work or school, symptom severity, quality of life). 7 Canadian administrative data from the catchment area of the Prevention and Early Intervention Program for Psychoses (PEPP) in London, Ontario, have also shown that mortality rates were four times lower in EPI users compared to a matched control group. 8 While EPI programs are now considered best practice in Europe, North America and Australia, differences in the availability of EPI programs between countries and different regions within countries remain.9–12
EPI programs have also been found to be cost saving or cost-effective compared to TAU as shown by a recent systematic review of 19 economic evaluations of EPI versus TAU. 9 However, only one study was conducted in Canada based on a matched cohort analysis 13 and this study did not consider the cost of the EPI program itself. As such the value of EPI programs in Canada is unknown, which represents an important gap in knowledge as EPI programs are not universally available across Canada.11,14 It is therefore critical to document their economic value to support the broader implementation of EPI programs in Canada. Therefore, the objective of this study was to conduct an economic evaluation of EPI compared to TAU in Canada.
Methods
Methods Overview
A decision analytic model was created to estimate the 5-year costs and benefits of EPI compared to TAU in individuals with first time psychosis in terms of hospitalizations, employment, number of assisted living days and mortality. Costs and benefits beyond one year were discounted annually at a rate of 1.5%. 15 A cost-benefit analysis (CBA) and a cost-effectiveness analysis (CEA) were conducted to compare EPI and TAU from a societal perspective. Scenario analyses were conducted to test the robustness of the results when changing key assumptions. Costs were reported in 2019 dollars.
Model Structure
The structure of the model is shown in Figure 1 and is similar to two previous EPI decision-analytic models.16,17 The model assumes that each month, a proportion of individuals will die. Alive individuals can be hospitalized or employed while the remainder will not. Additionally, an overall mean number of assisted living days are applied to all patients who are alive.
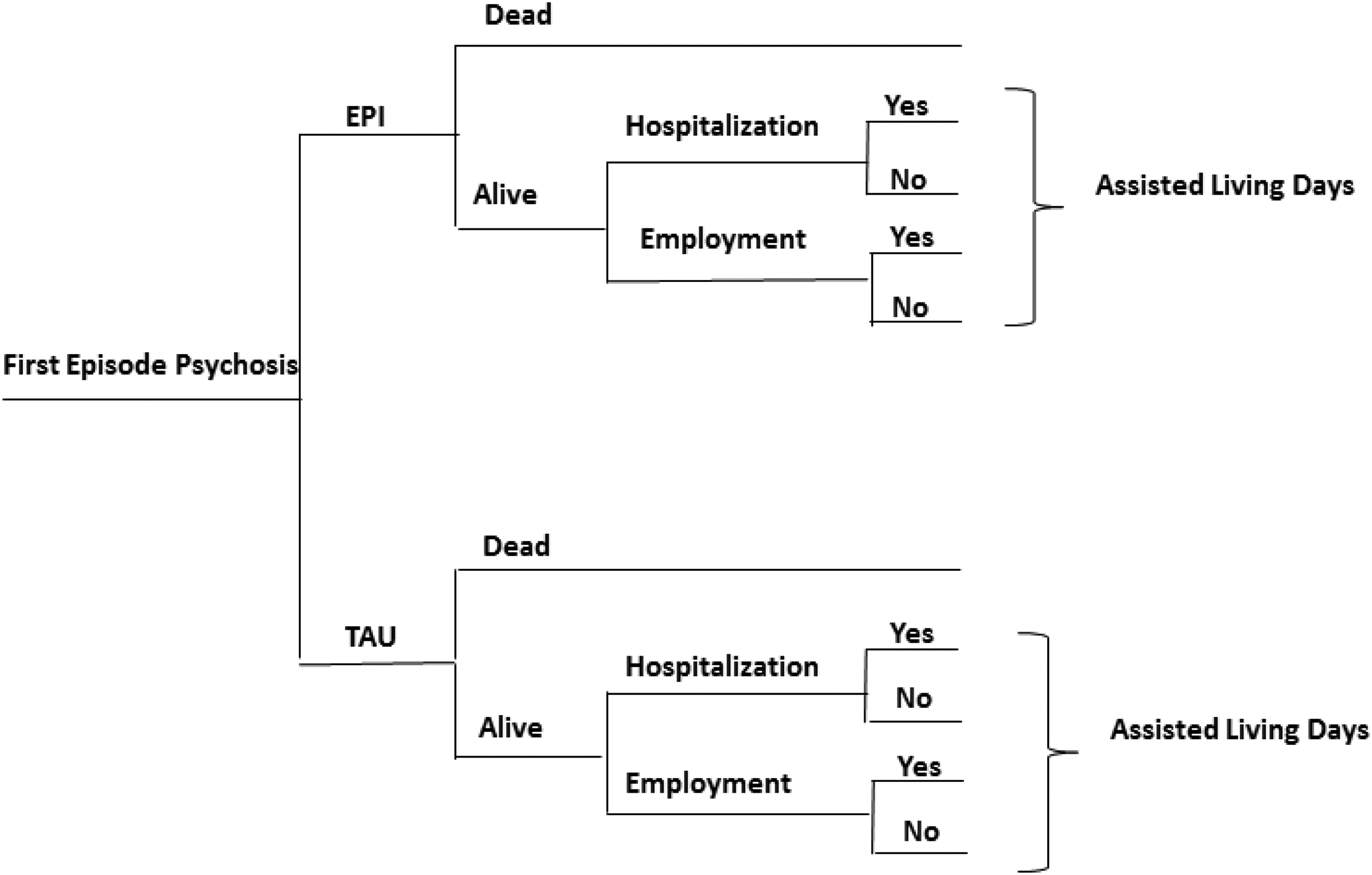
Model structure.
Clinical Inputs
In the absence of RCT data, mortality data were based on linked administrative databases from Ontario comparing over 5 years a cohort of individuals with first-episode psychosis using EPI services and a propensity matched control group of non-EPI users (i.e., TAU). 8 Based on an absolute risk reduction of 2.5% (95% CI: 1.3%, 3.7%) in favor of EPI, all cause mortality was modeled as 3.9% in TAU and 1.4% for EPI in the first two years following admission. 8 Since there were no differences in all cause mortality between EPI (1.5%) and TAU (1.7%) in the period between 2 and 5 years after admission, 8 TAU mortality rate was assumed for EPI for years 2–5.
Estimates of the mean number of hospitalizations and employment rates between EPI and TAU were based on a recent meta-analysis of RCTs comparing EPI versus TAU in early phase psychosis. 7 Based on a pooled analysis 7 of 7 RCTs (LEO, 18 STEP, 19 OTP, 20 COAST, 21 RAISE-ETP, 22 JECP, 23 PIANO 24 ), the mean (standard deviation [SD]) number of hospitalizations was 0.41 (0.30) for EPI and 0.59 (1.11) for TAU. To accommodate the monthly time periods of our model, these estimates were divided by the sample size weighted mean duration of the 7 RCT's (i.e., 17 months) included in the calculation of the number of hospitalizations. Based on Canadian data 14 and the duration of the RCTs included in the meta-analysis, the model assumes that EPI was provided for two years. After 24 months of EPI treatment, the model conservatively assumes the same hospitalization rates between EPI and TAU (i.e., impact of EPI on hospitalization does not continue after treatment cessation).
The proportion of individuals who were employed or in school after being treated with EPI or TAU were derived from the same meta-analysis. 7 The results which were based on 6 RCTs (LEO, 18 STEP, 19 RAISE-ETP, 22 JCEP, 23 OPUS, 25 PIANO 24 ) indicated that the proportion of patients that were either employed or in school following TAU treatment was 45.3% while the relative risk of being in school or employed with EPI compared to TAU was 1.13 (95% CI: 1.03, 1.24, p = 0.01). 7 Therefore the proportion of patients assumed to be working or in school following EPI treatment was calculated at 51.2% (45.3% × 1.13). To evaluate the impact of EPI on employment and associated productivity gains we used data from a Canadian study 26 which indicated that 72% of subjects in the EPI program who were either employed or in school, were in fact employed. In the absence of data, we also assumed 72% of TAU patients who were either employed or in school, were in fact employed. Therefore, the model assumes that 36.9% (i.e., 51.2% x 72%) and 32.6% (i.e., 45.3% x 72%) of EPI and TAU patients were employed following treatment, respectively. We further applied EPI Canadian data to estimate that amongst EPI and TAU patients that were employed, the proportion working full-time was 64% while the proportion working part-time was 36%. 26 Since it is unlikely that the effect of EPI on employment would be immediate, a 6-month delay from entering the program until EPI led to higher employment was assumed based on clinical opinion. Beyond the duration of the EPI intervention (i.e., 24 months in the base case analysis), we conservatively assumed that the effect of EPI would not last after EPI is stopped. Therefore, after 24 months, the proportion of individuals employed or in school in the TAU arm was applied to both the EPI and TAU arms.
To model the number of days in assisted living, data from the OPUS RCT was used as it is the only RCT reporting data on the mean number of days in assisted living associated with EPI and TAU. 27 In OPUS, 27 assisted living referred to facilities that were staffed around the clock for individuals with mental health problems. In the five-year follow-up of OPUS, EPI patients were found to have a lower mean number of assisted living days compared to TAU patients for a period of 3–5 years post treatment initiation, but not during the first two years post-treatment initiation. During years three to five, the mean (SD) number of assisted living days was reported to be 57 (213) and 102 (282) when EPI was compared to TAU, for a difference of 45.1 days (95% CI: 0.31, 89.9, p = 0.05). 27 This is equivalent to a monthly mean number of assisted living days of 1.58 for EPI and 2.83 for TAU. These differential rates were applied during months 25 through 60 in the 5-year base case analysis. During the first 24 months the mean number of supported housing days for TAU was applied to both treatment arms.
Cost Inputs
All costs are reported in 2019 dollars. The per-patient cost of providing EPI in Canada was based on a 2012 survey of 52 EPI programs in Ontario 11 in which participants were asked to provide the annual EPI budget (i.e., “What is your EPI program budget per annum?”) (Mean of $462,411) and the annual number of patients using EPI services (i.e., please indicate the “Currently registered clients") (mean of 62). Using this information, the per-patient annual cost of treating with EPI was calculated at $7,458 (i.e., $462,411/62). This study also reported the results by small or large catchment areas (e.g., $6,902 and $7,985, respectively) which were used in scenario analyses. Since the information reported in the survey included overheads but not psychiatrist fees, psychiatrist fees were added to the EPI cost per patient derived from the survey. Based on expert opinion, it was assumed EPI patients would have a psychiatric visit every 2 weeks for the first 3 months of EPI treatment, every 4 weeks during months 4 through 12 and every 6 weeks during the second year of EPI services. Assuming an initial psychiatric consultation fee of $300.70 (Ontario Schedule of Benefits, billing code A190) 28 and following psychiatrist consultations fees of $173.70 (billing code K198; 2 units) 28 the per-patient total physician fees applied to the first and second year of EPI treatment were $2,733 and $1,390 respectively. To the best of our knowledge no Canadian studies have compared the cost of treating first episode psychosis with TAU. Therefore we relied on two economic evaluations based on the Lambeth Early Onset (LEO) (TAU = 60% of EPI cost 16 ) and OPUS (TAU = 40% of EPI costs 29 ) RCTs to estimate the cost of TAU at 50% (e.g. average of the two studies) of the costs of EPI including psychiatrist fees. The EPI and TAU per-patient annual costs of treatment were converted to 1-month cost to accommodate the model's one-month time periods. Differential costs for the EPI and TAU arm were applied in the first 24 months of the model. After 24 months the cost of TAU was applied to EPI arm as our base case analysis assumes that the duration of EPI programs was 24 months. 14
Based on data from the Canadian Institute for Health Information (CIHI) the model considers an average cost of $13,266 for a hospitalization for schizophrenia/schizoaffective disorder (Case Mix Group 707, length of stay of 19.3 days). 30 CIHI hospitalization costs do not include physician costs. Therefore, based on expert opinion, the costs of psychiatrist visits during the EPI hospital stay were added assuming three psychiatrist visits per week. The model assumes a cost per day in assisted living of $87 based on the median cost per day in assisted living among five provinces reported in a recent Canadian study and adjusted to 2019 dollars using the Canadian Consumer Price Index for shelter. 31 Because of the variation in the cost of assisted living in this study, 31 the daily cost of assisted living was varied in scenario analysis. To estimate productivity costs associated with employment, a monthly wage was applied to individuals who were employed during each month. Since young people with early psychosis may be more likely to be employed in lower paying jobs, 17 the Ontario minimum wage of $14 per hour 32 was assumed to be conservative in our estimates. Furthermore, it was assumed that full-time employees would work 40 h per week, while part-time employees would work 20 h per week.
Economic Evaluation
A CBA and a CEA were performed to determine the economic value of EPI compared to TAU. Under the cost-benefit framework, the net benefit (NB) associated with treating patients with EPI instead of TAU was calculated as the difference between the incremental monetized benefits (i.e., hospitalization, employment, assisted living days and mortality) and the incremental treatment costs of EPI versus TAU. To model monetized life years lost, a value of $100,000 per year of life was applied to each year of the expected remaining life of our population based on the value of statistical lives recommended by the Treasury Board of Canada for valuing premature mortality (i.e., $6.1 million in 2014 or $7.9 million in 2019 dollars). 33 A standardized mortality ratio for schizophrenia compared to the general population of 2.5 34 was applied to Canadian life table data to estimate life years lost and lifetime monetized life years lost assuming an average age of 25 years 8 for our population. In the CEA, costs (treatment costs and costs related to hospitalization, productivity and assisted living days) and effectiveness (i.e., life-years) were compared between EPI and TAU to determine the incremental cost per life year gained (LYG) associated with EPI.
Several scenario analyses were conducted to evaluate the impact of key model assumptions on the results including: 1) using different values for the relative price of TAU compared to EPI (i.e., base case 50%, scenario analyses using 40% and 60%) and for EPI annual treatment cost (base case = $7,458) to reflect low ($6,902) and high ($7,985) catchment areas; 2) varying the number of psychiatrist visits during the EPI program by + /-20% and the daily cost of assisted living (base case: $87, scenario analysis using $60 or $100); and 3) assuming that the effect of EPI on employment would be immediate (base case: 6-month delay).
To deal with the uncertainty associated with the model parameters, probabilistic analyses was undertaken for the base case and scenario analyses. In probabilistic analysis, 15 each parameter is assigned a probability distribution and the model is simulated a large number of times (e.g., N = 1,000 simulations). A 95% CI can then be evaluated for each model outcome. For the CBA, the proportion of simulations for which the NB was positive was calculated while cost-effectiveness acceptability curves (CEAC) 35 were used in the CEA to determine the probability of EPI being cost-effective at different levels of willingness to pay per LYG (e.g., $100,000/LYG). Table 1 provides a summary of the base case values and the associated distributions considered for the simulations. 35 To measure the impact of the assumptions made for the parameters’ distributions, we conducted additional probabilistic analyses by changing the value of the standard errors (SEs) (i.e., assuming the SEs are half or twice the SEs used in the reference case).
Summary of Values, Parameters and Sources of Clinical and Cost Variables Used in the Analyses.
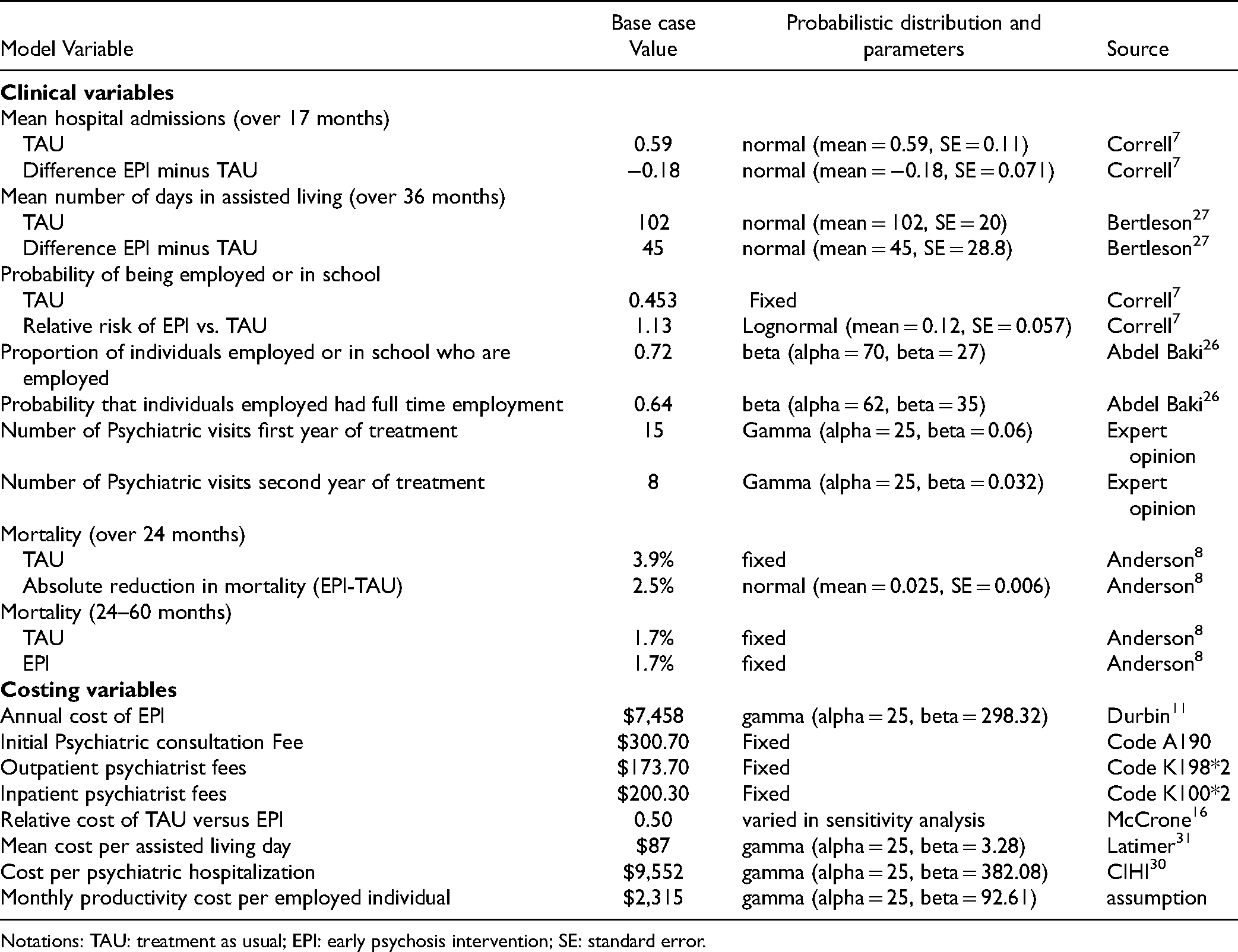
Notations: TAU: treatment as usual; EPI: early psychosis intervention; SE: standard error.
Results
In the base case, the CBA results indicated that the additional costs associated with treating patients with EPI compared to TAU ($10,909; 95% CI: $7,779, $14,999) were lower than the associated monetized benefits ($96,351, 95% CI: $51,211; $137,500), yielding a NB of $85,441 (95% CI: $41,140; $126,386). The NB was positive in 100% of the simulations. In the CEA, the incremental cost per LYG of EPI compared to TAU was $26,366 (95% CI: dominates TAU, [i.e., less costly, more life years]; $102,269) and the probability of EPI to be cost-effective at a willingness to pay of $100,000/LYG was 0.96 (Figure 2). Table 2 presents the details.
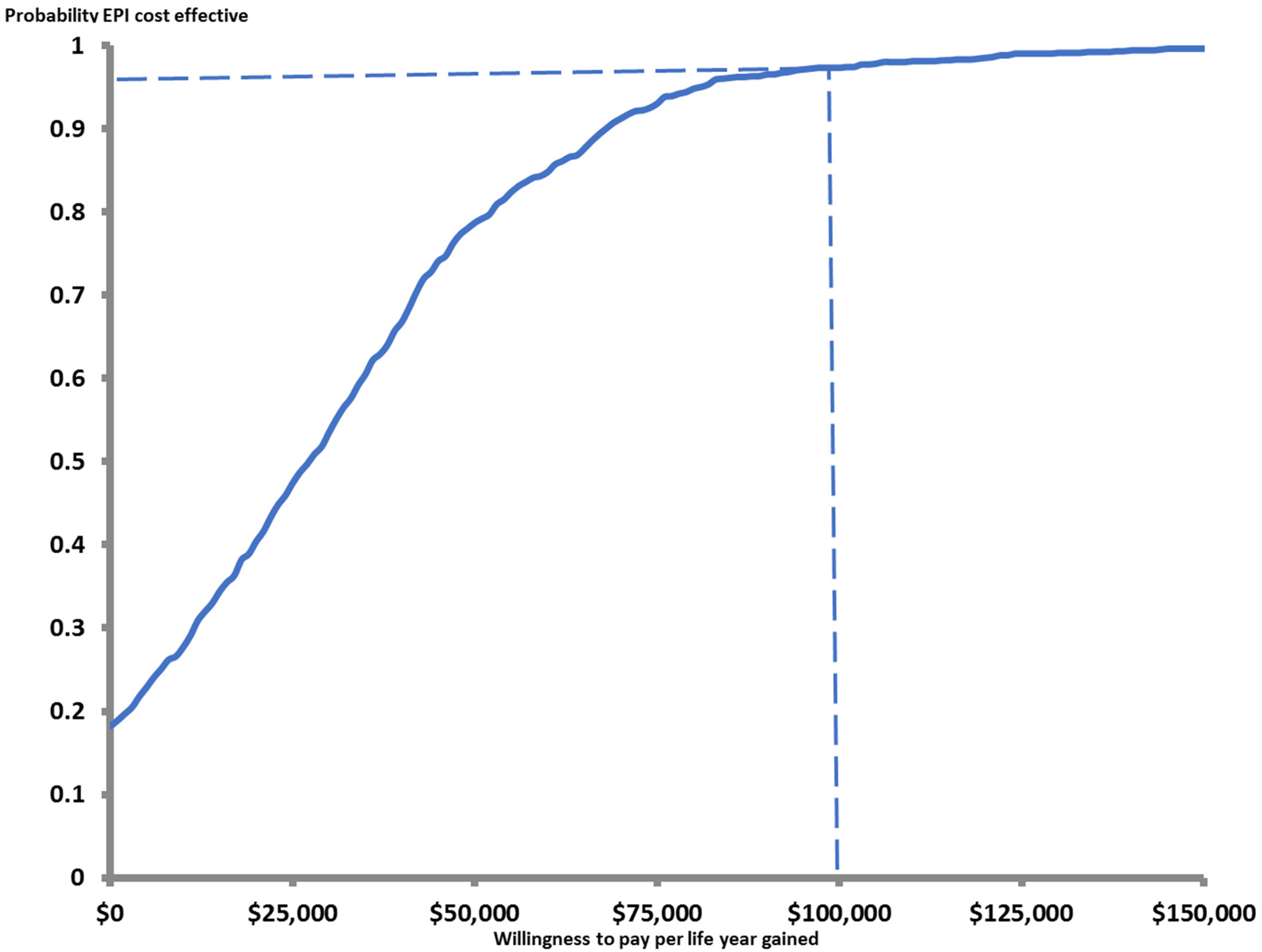
Cost-effectiveness acceptability curve.
Cost Benefit and Cost-Effectiveness Analyses (EPI Compared to TAU): Base Case Probabilistic Results.
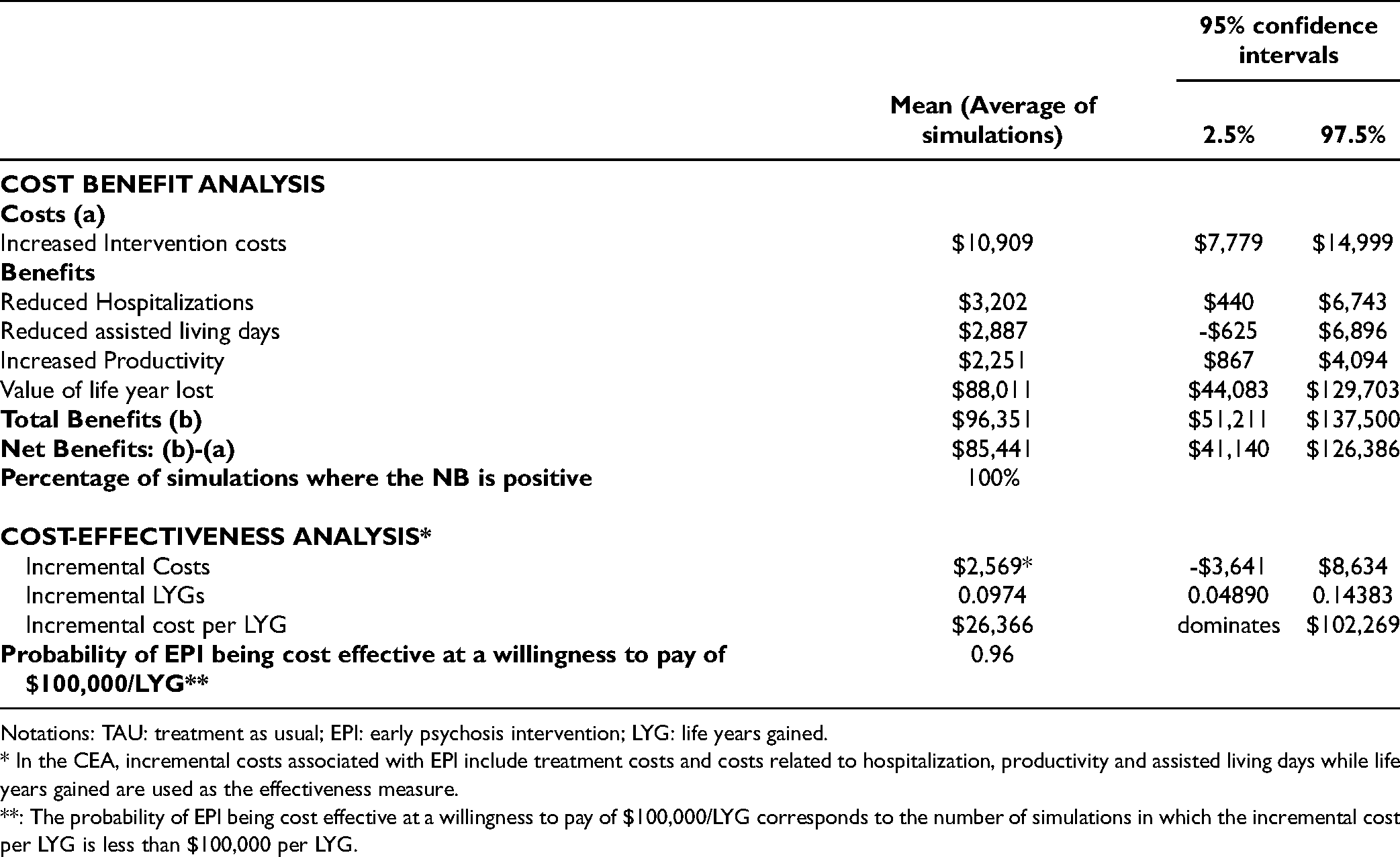
Notations: TAU: treatment as usual; EPI: early psychosis intervention; LYG: life years gained.
* In the CEA, incremental costs associated with EPI include treatment costs and costs related to hospitalization, productivity and assisted living days while life years gained are used as the effectiveness measure.
**: The probability of EPI being cost effective at a willingness to pay of $100,000/LYG corresponds to the number of simulations in which the incremental cost per LYG is less than $100,000 per LYG.
Using wider distributions for the probabilistic analysis had the most impact on the results (Table 3) but still the NB was positive in 97% of the simulations in the CBA and the probability of EPI to be cost-effective at a willingness to pay of $100,000/LYG was 0.84 with incremental cost-effectiveness ratios of less than $50,000/LYG.
Scenario Analyses (Probabilistic): Early Psychosis Intervention (EPI) vs. Treatment as Usual (TAU).
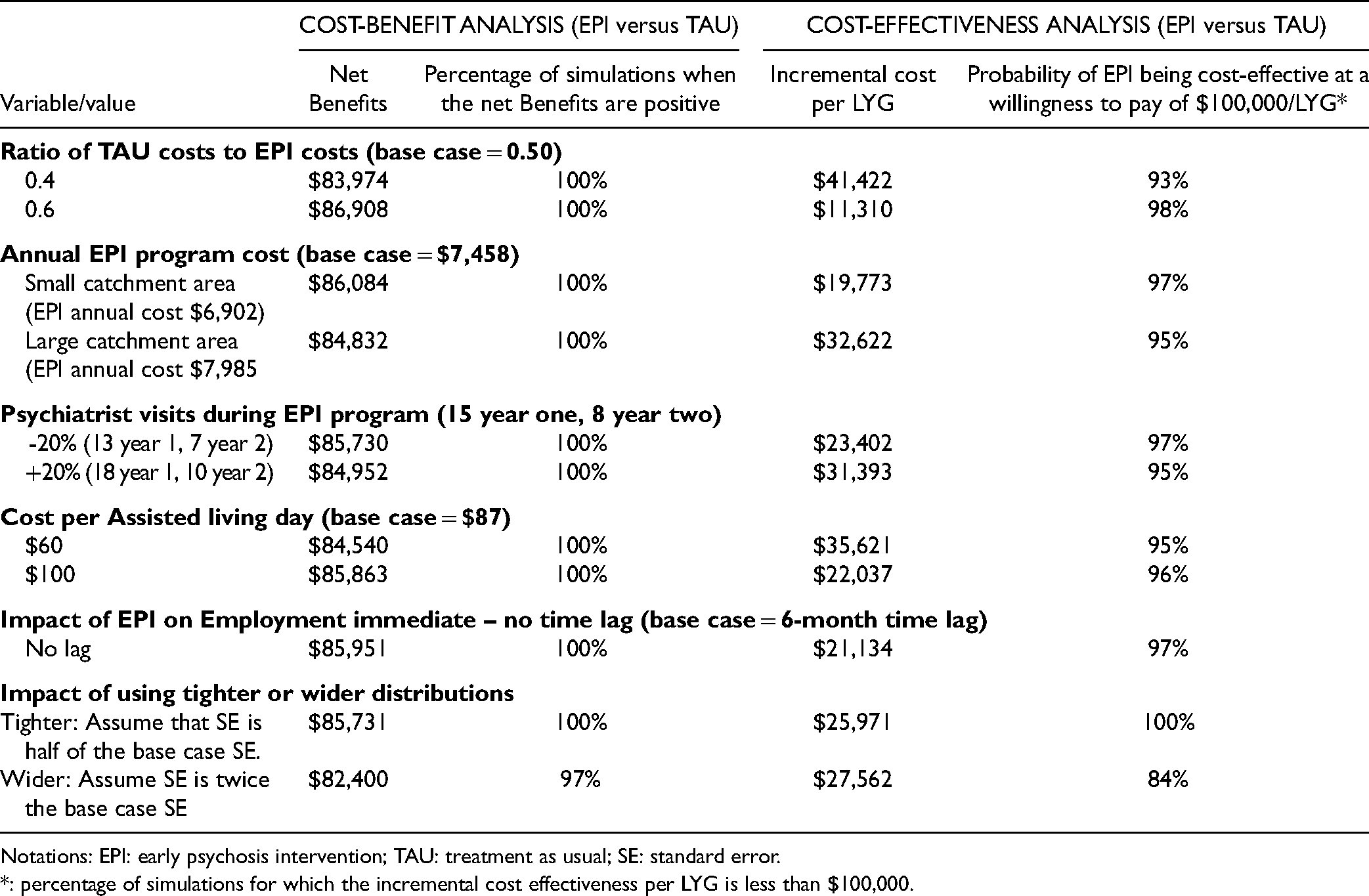
Notations: EPI: early psychosis intervention; TAU: treatment as usual; SE: standard error.
*: percentage of simulations for which the incremental cost effectiveness per LYG is less than $100,000.
Discussion
Despite the recommendations of several provincial guidelines5,36 EPI is not yet universally offered in Canada. 14 This study is a first step in understanding the economic value associated with the provision of EPI in Canada and makes an important contribution to the economic literature on EPI. Our base case results suggest that EPI provides good value for money compared to TAU as shown by the CBA (NB of $85,441) and the CEA (Incremental cost per LYG of $26,366). In all scenario analyses comparing EPI versus TAU, the NB remained positive and the incremental cost per LYG was less than $50,000/LYG. The evidence provided here does suggest that EPI should be offered to all young Canadians experiencing first episode psychosis.
Our base case results were aligned with a recent systematic review of 19 economic evaluations of EPI services across the world, which showed that EPI was a cost-effective treatment strategy. Compared to these economic evaluations, 9 our study has several strengths. First the clinical data used to model the impact of EPI on hospitalizations and employment was based on a recent meta-analysis of several RCTs comparing EPI and TAU in different countries and settings. 7 Data on the impact of EPI on assisted living days was based on one of the largest RCTs to date. 27 While the mortality data were derived from Canadian non-randomized evidence, the risk of confounding in this study was reduced due to the use of propensity scoring matching to create comparable cohorts of EPI and non-EPI users. 8 Another strength of the analysis is that it is fully probabilistic and therefore, the uncertainty around the model parameters is considered. We also used several conservative assumptions in our estimates. For example, we assumed that the treatment duration and benefits of EPI lasted 2 years based on the duration of RCTs included in the meta-analysis while there may be value in extending EPI beyond 2 years as shown in a recent Canadian 37 study and as now suggested in some provincial guidelines.5,6 In terms of limitations, although Canadian unit costs were used in the analysis, none of the RCTs included in the meta-analysis used for this evaluation 7 were conducted in Canada although they represented many different jurisdictions across the world. However, the generalizability of the trial results to current Canadian practice is unknown. In addition, RCTs may have had higher standards of fidelity than real world practices of EPI although the recent OPUS-real-world 38 data confirmed the effectiveness of EPI in real-world settings. We also did not model the costs and monetized benefits of providing EPI beyond 2 years. While we were able to derive a per-patient cost of EPI treatment based on a survey of 52 EPI services in Ontario, 11 the costs of EPI may be different in other Canadian provinces. The cost of TAU was not available in Canada and we had to rely on international data from LEO 16 and OPUS. 29 Furthermore, what is considered as TAU is variable and may differ between jurisdictions. However, the results of our scenario analysis varying the cost of EPI or TAU did not change the study conclusions. Due to the lack of Canadian data, community medication costs associated with EPI and TAU were not included. However, although not directly comparable, the recent Canadian economic evaluation of a 3-year RCT extension following two years of EPI did not find a statistically significant difference in medication costs between EPI and TAU over the three years of participation. 39 Another major limitation of our economic evaluation is that due to the lack of data, we did not model the impact of EPI and TAU on health-related quality of life (HRQoL) using an outcome such as quality adjusted life years (QALYs). This is not unique to our study as two recent published economic evaluations of EPI39,40 have used relapse avoided or months in total symptom remission in their cost-effectiveness calculations. Due to the scope of our CBA and CEA, we did not evaluate issues related to the universal implementation of EPI services in Canada. Those issues are important as the recent Ontario data 2 from the catchment area of the London-based EPI program indicated that approximately 50% of first-episode psychosis patients did not contact the EPI program for screening or admission. 41 Differences in EPI access were also seen across socio-economic strata, which raised important issues regarding equity in access. 41 In addition, while EPI programs can be offered in specialized settings by a dedicated team (e.g., academic hospitals), recent RCT data from the US/Canada (RAISE 22 ) and Italy (PIANO 24 ) have shown that integrating the provision of EPI services in community mental health teams (CMHT) by training CMHT staff to deliver EPI model-based care is also effective22,24 and cost-effective. 42 This may help provide access to EPI services especially in smaller communities where the small number of incident cases does not allow the regrouping of first episode psychosis patients and EPI staff in a separate specialised service. Finally, to ensure quality of care, maximise access, attainment of expected superior EPI outcomes, and similar cost between EPI programs, fidelity to the model is of utmost importance. Therefore, continuous training and monitoring involving community of practice and/or learning healthcare systems are also key when implementing EPI programs. 12
This economic evaluation also identified a few important areas for future research priorities. First and foremost, more information on the cost of providing EPI and TAU is needed in Canada and elsewhere. Second, efforts should be made to determine the economic value of providing EPI beyond 2 years although the recent Canadian economic evaluation of a 3-year RCT extension following two years of EPI did not find a statistically significant difference in hospitalizations between EPI and TAU. 39 Finally, there is a need to generate HRQoL data associated with EPI or TAU treatments which could be used to conduct cost-utility analyses, and to leverage administrative databases to document the epidemiology, costs, and outcomes associated with EPI compared to TAU.
Given the demonstrated clinical benefits of EPI, large scale implementation of EPI has been recommended in different Canadian provinces. Our results suggest that the large-scale implementation of EPI in Canada would also be desirable from an economic point of view. However, future research is required to provide more certainty about the costs of providing EPI and TAU to better support decision-making about large scale implementation of EPI in Canada.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the McConnell Family Foundation and the Canadian Institute of Health Research, (grant number 156947).