
Abstract
Objective
To assess the association between receipt of minimally adequate treatment (MAT) and mortality in a sample of community primary care older adults with depression and anxiety.
Method
The present study was conducted among a sample of 358 older adults ( ≥ 65 years old) with depression or an anxiety disorder recruited in primary care practices between 2011 and 2013. Participants agreed to link their health survey and administrative data for the 3 years preceding and following the baseline interview. Depression and anxiety disorders were based on self-reported symptoms aligned with DSM-5 criteria and physician diagnoses (International Classification of Diseases [ICD], 9th and 10th revisions). MAT was defined according to Canadian guidelines and include receipt of pharmacotherapy and ≥ 4 medical visits within 3 months or a number of psychotherapy sessions (individual, group, or family) over 12 months (depression: ≥8; anxiety disorders: ≥5 to 7). All-cause 3-year mortality was ascertained from the vital statistics death registry in Québec. Propensity score weighted regression analysis was conducted to assess the association between receipt of MAT and mortality adjusting for individual, clinical, and health system study factors.
Results
Receipt of MAT was associated with a reduced risk of mortality (hazard ratio [HR]: 0.27; 95% confidence interval [95% CI], 0.12 to 0.62). Individual and clinical factors associated with increased mortality included older age, male sex, being single, low functional status, and increased physical disorders and cognitive functioning. Lifestyle factors associated with reduced and increased mortality included alcohol consumption and smoking, respectively. Health system factors such as perceived adequate number of visits to speak to the doctor about emotional problems and continuity of care were associated with reduced mortality.
Conclusion
The current study highlights the important role of primary care physicians in detecting and providing MAT for older adults with depression and anxiety, as this may have an effect on longevity.
Introduction
In Canada, the highest increase in the prevalence of mental disorders in the next 20 years will be in older adults with estimates for anxiety and depression reaching 19% in females and 10% in males 1 . Past year prevalence estimates in older adults are 3% and 20% for major and dimensional depression assessed through standardized and self-reported questionnaires 2 , and between 6% and 17% for anxiety disorders3–5. With individuals living longer, a Canadian study, reporting on the distribution of chronic conditions at the time of death, showed a 29% increase in the presence of mood disorders over a 10-year period 6 .
In large international population registry studies, the presence of mental disorders has been associated with excess mortality and premature death due to suicide and chronic medical conditions7–10. Research in Canada analyzing data from the Quebec Integrated Chronic Disease Surveillance System showed that the presence of a mental disorder was associated with an 8 and 5-year reduced life expectancy due to suicide and physical comorbidities in men and women 11 . When looking at differences in life expectancy by disorders, reductions were observed in both men and women for schizophrenia 11 and personality disorders 12 . Reduced life expectancy was also seen in men with mood or anxiety disorders but not in women 11 . A possible explanation put forth by authors was that women are more likely than men to consult for mental health reasons and may therefore be more likely to be detected and treated for their mental health and chronic conditions 11 .
In a general population survey in the United States, the presence of self-reported anxiety or depression was not associated with mortality in those who had consulted a mental health professional, but was associated with increased mortality in those who had not consulted 10 . In older adult Veterans, quality of care defined as an adequate supply of antidepressants and follow-up to monitor drug use was associated with a decreased risk of mortality 13 . The majority of older adults however either receive no or inadequate antidepressant treatment and follow-up mental health care14–16.
In Canada, general population studies have shown that only up to 42% of older adults with a mood or anxiety disorder consulted for their mental health in the past year17,18. When they do, close to 80% of older adults consult their family physician or general practitioner 17 . The current primary care study can contribute to the literature regarding the association between receipt of minimally adequate treatment (MAT) and mortality in older adults with anxiety and depression. The study includes linked health survey and medico-administrative data minimizing information bias regarding the presence of a mental disorder and treatment and allow adjusting for sociodemographic, clinical, and psychosocial variables as potential confounders. This overcomes some of the limitations of previous registry studies in Canada using medico-administrative data only, which would only capture those seeking health services.
Methods
Study Sample
This study is based on a convenience sample of 1811 older adults participating in the Études sur la santé des ainés (ESA) Services study and recruited in primary care practice waiting rooms in one of the largest health regions in the province of Quebec between 2011 and 2013. Study details have been presented elsewhere 19 . Interested participants were contacted by the study coordinator describing study objectives and were interviewed at home by trained health professionals using a computer assisted questionnaire. Cognitive functioning was assessed with a French translation of the Mini-Mental State Examination (MMSE) adapted for at-home interviews in community-living older adults20,21. Individuals scoring less than 22 were not included in this study. Respondents gave written consent to link their data to health administrative data from the Régie de l’Assurance Maladie du Québec (RAMQ), the Maintenance et exploitation des données pour l'étude de la clientèle hospitalière (MED-ECHO) dataset, and the vital statistics death registry in the 3 years preceding and following the baseline interview. These administrative databases provide data on outpatient and emergency department (ED) visits, hospitalizations, physician diagnoses, medications delivered under the Quebec drug plan, and date and cause of death. Permission to link data was obtained from the Commission d’Accès à l’Information du Québec and the compilation was based on data from the © Government of Quebec. Ethics approval for the ESA Services longitudinal study is obtained annually from the ethics committee of the CISSS – Montérégie Centre and CIUSSS Estrie – Centre Hospitalier Universitaire de Sherbrooke.
Of the 1811 participants, 1456 gave access to their administrative data and were covered under Quebec's public drug plan. Of these, 358 had either a physician diagnosis of depression or an anxiety disorder or self-reported symptoms in the last 6 months consistent with those used for DSM-5 criteria (with the exception of functioning impairment) for major depression, social phobia, specific phobia, generalized anxiety disorder, panic disorder, and agoraphobia 22 . The ESA mental health modules of the standardized questionnaire have been described in detail elsewhere 23 . As an example, individuals were identified as having major depression if they reported five of the nine symptoms of depression every day for at least two consecutive weeks, including the presence of depressed mood or loss of interest, and that these symptoms were not due to another disease or a medication 22 . The presence of a physician diagnosis of depression and an anxiety disorder in the health administrative databases was assessed during the 6 months preceding and following the baseline interview. The following codes from the 9th and 10th revisions of the International Classification for Diseases (ICD) were used: 300.0; 300.2; 311.0; 311.9; 300.4; F32; F33; F34.1; F40; and F4124–28. Individuals having other mental disorders weren’t excluded from the analytic sample.
Measures
All-cause 3-year mortality post-interview was ascertained from the vital statistics death registry in the province of Québec 29 .
MAT for depression and anxiety disorders was defined using minimal quality of care indicators based on Canadian clinical guidelines and relevant literature30–37. MAT for depression was based on the presence of a first, second, or third line recommended antidepressant prescription and at least four follow-up visits with a primary care provider (PCP) within 3 months of the diagnosis or prescription delivered or eight sessions of psychotherapy (individual, group, or family) within a year31,35,37,38. MAT for anxiety disorders (except for specific phobia) was based on the presence of a first, second, or third line recommended medication delivered including an antidepressant, anxiolytic, or other recommended medication and at least four follow-up visits with a PCP within 3 months of the diagnosis or prescription delivered or seven sessions of psychotherapy (individual, group, or family) within a year30,34,36. Other guideline-recommended medications include anticonvulsants, atypical antipsychotics (quetiapine, risperidone), buspirone, and atomoxetine 30 . Since pharmacological treatment is not recommended for specific phobia, MAT was defined as the presence of five psychotherapy sessions within a year. The detailed description of MAT for depression and anxiety disorders has previously been described elsewhere 39 .
Although the recommendations for the use of anxiolytic drugs in older adults have evolved in the last decade where some long-acting benzodiazepines may be appropriate for only certain conditions such as severe generalized anxiety disorders, the Beer's criteria state that the use of benzodiazepines in older adults should be avoided40,41. Additional sensitivity analyses were carried out where the presence of a benzodiazepine was not considered in the definition of minimal adequate treatment for anxiety disorders.
The following individual factors measured at baseline were considered as potential confounders in the multivariable models: age; sex (male/female); education (years); marital status (with vs. without partner); total household revenues before taxes (≤25,000$ vs. ˃ 25,000$, to closely reflect low income cut-offs) 42 , functional status (high functioning [first–third quartiles] vs. low functioning [fourth quartile]) was based on 8 dimensions of Instrumental Activities of Daily Living (IADL)43,44; number of physical diseases was based on a list of 17 medical chronic conditions (related to, e.g., cancer, headaches/migraines, arthropathy, musculoskeletal disorders, respiratory disease, cardiovascular disease, gastrointestinal disease, liver disease, urinary tract problems, thyroid problems, diabetes, dermatologic conditions); cognitive functioning was measured with the ESA French translation of the MMSE with possible scores ranging from 22 to 3020,21; childhood trauma (presence vs. absence) 45 ; satisfaction with life was assessed with a French adapted version of the Satisfaction with Life Scale (5–25)46,47; current smoker (yes vs. no), alcohol consumption in the past 6 months (yes vs. no); and number of sessions per week exercised at least 20 min. Patient perceptions about mental health treatment were assessed with the following three questions: (1) perceived physician availability to speak of emotional problems, (2) perceived adequate number of visits with the doctor to speak about emotional problems, and (3) perceived effectiveness of health professionals helping resolve emotional problems. The five answer choices for each question were: certainly, a lot, moderately, a little, not at all, and don’t know. Answers to the three variables were dichotomized and analyzed as follows: Certainly/a lot/moderately versus a little/not at all/don’t know.
Health system factors were also considered and included the number of outpatient and ED visits and hospitalizations in the 3 years preceding the baseline interview, the median distance to private clinics for general medical services, and the median distance to hospital for general medical and psychiatric services. Continuity of care in the 3 years post-interview was the ratio between the number of different physicians consulted over the total number of visits in ambulatory care 48 , which has been previously used in populations of older adults with chronic diseases49,50. A possible score is between 0 and 1, with higher scores representing higher continuity of care 51 . Outpatient and ED visits, hospitalizations and inpatient stay, and the continuity of care index were ascertained using the RAMQ and MED-ECHO administrative database. The median distance to private clinics and hospital was estimated using the Consommation et offre normalisée des services offerts par les Médecins (CONSOM) provincial database 52 .
Analyses
Differences in proportions and means for categorical and continuous variables were ascertained using chi-square and Student’s t-test statistics. Bivariate and multivariable time to event analyses were carried out to assess receipt of MAT and the risk of death controlling for individual and health system factors.
To address the potential treatment selection bias in this observational study, propensity score analysis was carried out where the inverse probability of receipt of MAT was calculated53,54. A propensity score weighted regression model was fitted to assess the effect of receipt of MAT on the risk of death adjusting for study variables. In the analysis of the propensity score, variables that were associated with the outcome of interest, mortality, and factors assessed before treatment assignment were included in the logistic regression predicting receipt of MAT 55 . In the present study, the variables used to assess the probability of receiving MAT were age, sex, marital status, functional disability, number of physical conditions, smoking status, exercise, and number of hospitalizations and ED visits in the past 3 years. Additional analyses also considered the effect of receipt of MAT excluding benzodiazepine use from the definition. Hazard ratios (HRs) are reported with their 95% confidence intervals (95% CIs). All hypotheses were tested at a 95% significance level. Statistical analyses were performed using SAS version V.9.4.
Results
In the present primary care sample of older adults, 77% (n = 274) had an anxiety disorder, 13% (n = 46) depression, and 10% (n = 38) had both. The 3-year risk of mortality reached 6.7% (n = 24). Thirty-nine percent of participants received MAT for their depression or anxiety disorder. The characteristics of the sample are shown in Table 1. In the bivariate analyses, age, marital status, physical functioning, lifestyle behaviors including alcohol consumption and smoking, past hospitalizations and ED visits, and continuity of care were associated with mortality.
Characteristics of Study Sample in Relation to 3-Year Mortality.
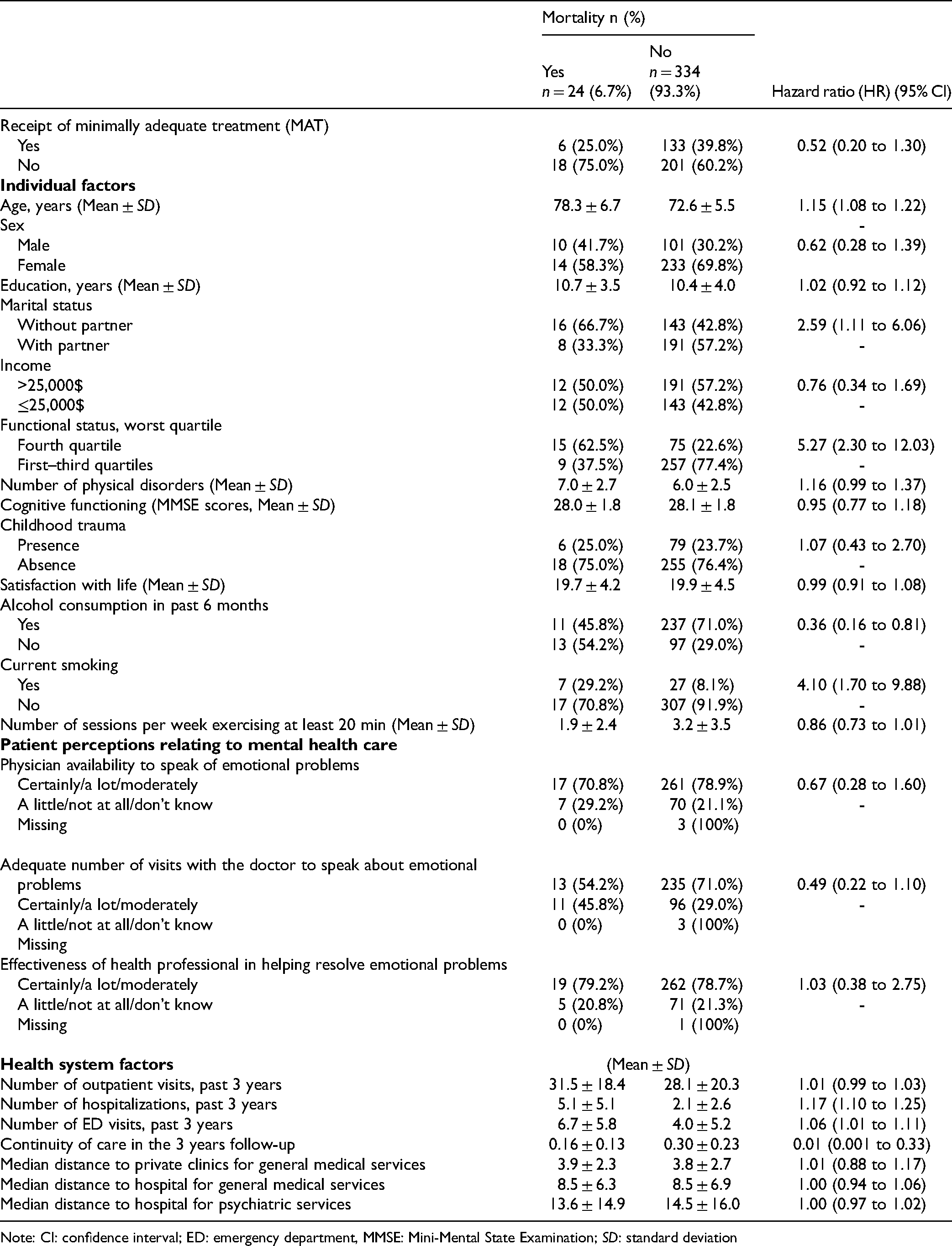
Note: CI: confidence interval; ED: emergency department, MMSE: Mini-Mental State Examination; SD: standard deviation
The weighted and unweighted multivariable analyses are shown in Table 2. Both the unweighted (HR 0.27; 95% CI, 0.08 to 0.93) and weighted (HR 0.27; 95% CI, 0.12 to 0.62) analyses showed a significant association between receipt of MAT and mortality. Additional sensitivity analyses where benzodiazepine use was not considered in the definition of MAT showed similar results.
Multivariable Analyses of Mortality as a Function of Minimally Adequate Treatment (MAT) and Study Variables (n = 351).
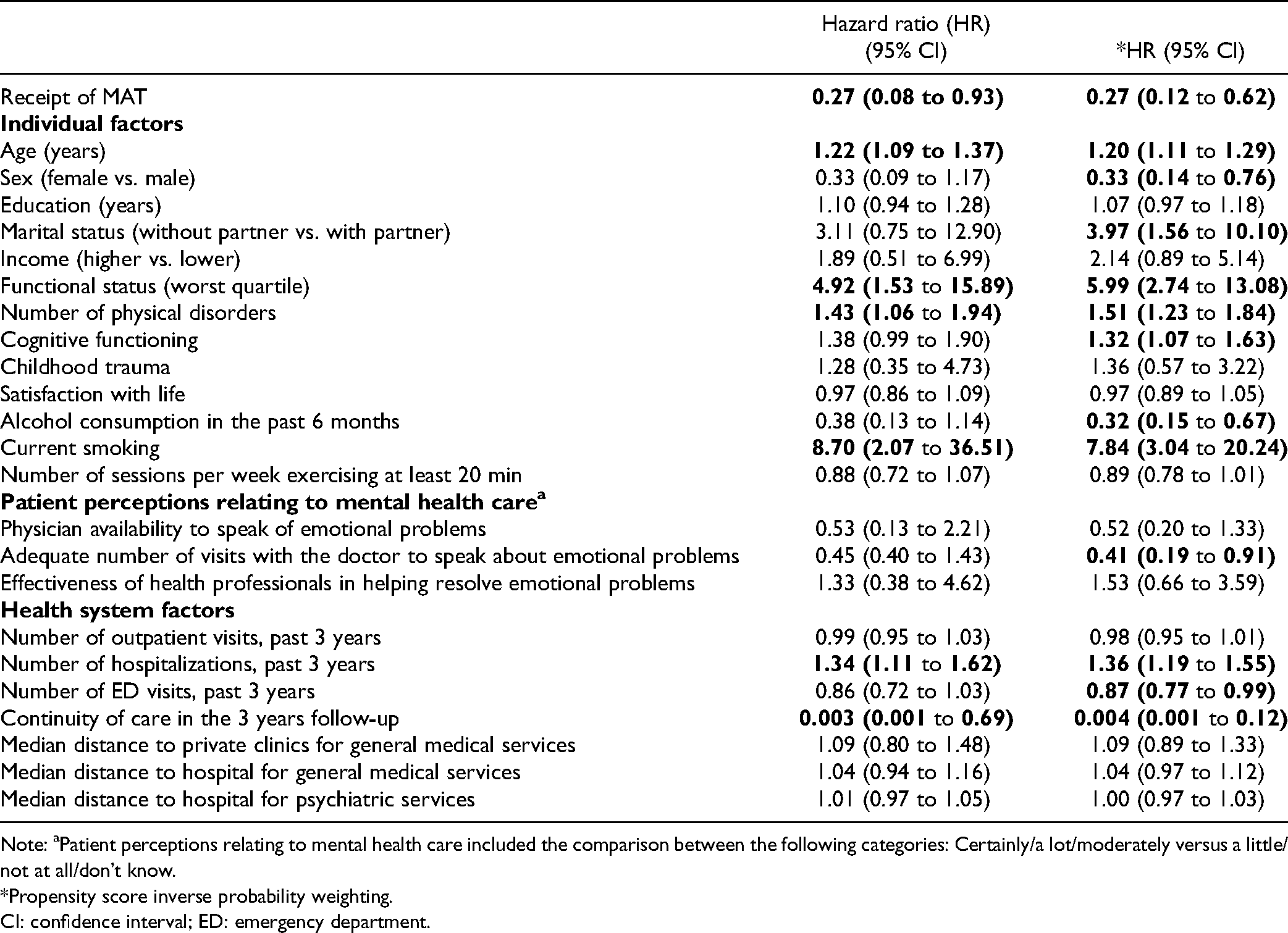
Note: aPatient perceptions relating to mental health care included the comparison between the following categories: Certainly/a lot/moderately versus a little/not at all/don’t know. *Propensity score inverse probability weighting.CI: confidence interval; ED: emergency department.
Individual and health system factors that were significantly associated with increased mortality in the weighted analyses included older age (HR: 1.20; 95% CI, 1.11 to 1.29), being single (HR: 3.97; 95% CI, 1.56 to 10.10), reduced functional status (worst quartile) (HR: 5.99; 95% CI, 2.74 to 13.08), increased number of physical disorders (HR: 1.51; 95% CI, 1.23 to 1.84), higher cognitive functioning (HR: 1.32; 95% CI, 1.07 to 1.63), current smoking (HR: 7.84; 95% CI, 3.04 to 20.24), and past hospitalizations (HR: 1.36; 95% CI, 1.19 to 1.55). Factors that were associated with reduced mortality included female sex (HR: 0.33; 95% CI, 0.14 to 0.76), alcohol consumption (HR: 0.32; 95% CI 0.15 to 0.67), patient perception of having had an adequate number of visits to speak to the doctor about emotional problems (HR: 0.41; 95% CI, 0.19 to 0.91) and increased continuity of care (HR: 0.004; 95% CI, 0.001 to 0.012).
Discussion
In the present primary care sample of older adults with self-reported and physician-diagnosed anxiety or depression, receipt of MAT was associated with reduced mortality. Additional analyses where the presence of a benzodiazepine prescription was excluded from the definition of receipt of MAT showed similar results.
Improved mental health follow-up of older adults with major depression and reduced mortality was similarly reported in the PROSPECT study 56 . The trial followed for 5 years older adults in primary care settings that were randomized to practices receiving either primary care physician education sessions alone or adding education for patient families, and a depression care manager within practice 57 . In a large U.S. Veteran population, adequate mental health care, defined as at least three visits within a 3-month period after diagnosis58,59, was associated with a reduced risk of 1-year mortality. Also in a sample of Veterans, an adequate supply of antidepressants measured on the basis of the medication possession ratio (≥80%) 13 was not associated with mortality. Although these study populations are not directly comparable, the findings mostly support the importance of quality mental health care and continuity of primary care for older adults with depression and anxiety in reducing mortality. Future studies should focus on assessing which component of quality mental health care is associated with a decreased risk of mortality.
A previous study in older adults showed that the presence of major depression, anxiety, suicidal ideation, and psychological distress was associated with low satisfaction with continuity of care, patient–provider interactions, and low satisfaction with adequacy of care. While controlling for a number of individual socioeconomic, clinical, and lifestyle factors, it was interesting to note, that patient perceptions relating to physician availability to speak of emotional problems and perceived effectiveness of consulting health professional in resolving emotional problems was not associated with mortality. Increased continuity of care and patient-perceived adequate number of visits to speak about emotional problems in the present study were associated with a reduced risk of mortality, which has been reported elsewhere60–62.
The present study included a number of strengths and limitations. First, the presence of mental disorders was based on information from self-reports and physician diagnoses, which may have reduced the potential for information bias related to social desirability in health surveys and underreporting of diagnoses in health administrative data as physicians are not obligated to report for payment 63 . Second, the definition of MAT included receipt of individual, group, or family psychotherapy either in the public or private sector adding to the validity of the measure overall. Follow-up visits with psychiatrists weren’t considered in the definition. However, only four participants had a psychiatrist visit in the 12 months following the interview and no participant had more than two visits, therefore minimizing any misclassification bias. Although treatment recommendations for different anxiety disorders differ, the same definition of minimal adequate treatment was applied for all anxiety disorders included in the study with the exception of specific phobia. Third, to reduce the potential selection bias related to receipt of MAT, propensity score analysis was carried out while including the control of a number of individual and health system factors. Although the majority of variables were assessed by self-report and may have been subject to recall and social desirability bias, we do not expect the potential information bias to have been different between deceased and non-deceased individuals. Fourth, in the absence of a randomized controlled trial, confounding by indication can’t be ruled out and the results can’t be considered as proving that MAT for depression or anxiety decreases all-cause mortality and this despite the use of a propensity score analysis. Fifth, given that this was a convenience sample of French speaking older adults consulting in primary care practices, a possible selection bias remains. However, the majority of older adults in the province of Quebec has a family physician 64 and consult their primary care physicians annually. Sixth, recruitment of participants was limited to one specific health administrative region in the province of Quebec, which may have limited generalizability. However, the region was one of the largest in the province with the highest proportion of older adults and covered geographically rural and urban regions. Seventh, using an MMSE cut-off of 22, the study sample included individuals with mild impairment but excluded individuals with substantial deficits in cognitive functioning 65 , therefore limiting the generalizability of conclusions to individuals with more severe clinical profiles. Although not observed in the multivariable analyses, the propensity score analysis unexpectedly showed an increase in mortality with higher cognition. This finding is unexpected as cognitive impairment has previously been associated with increased mortality. It is possible that this is a chance finding given the small sample size or may reflect residual confounding. We note that this sample generally had good cognitive functioning with a mean MMSE score of 28 and in some analyses decline in cognition, rather than baseline cognition, has been more robustly associated with mortality when baseline comorbidities have been adjusted for 66 . Lastly, the sample size of this study with respect to cases of depression and deaths was limited and may have led to increased uncertainty surrounding some estimates.
Although significant associations were observed with the main independent variable of interest and mortality, future larger and longer longitudinal studies are needed to better ascertain the effect of quality health care on mortality for individuals with depression and anxiety. For instance, it was not possible to assess whether the associations observed were mainly explained by pharmacotherapy and follow-up, psychotherapy or both. Given that the combined effect of pharmacotherapy and psychotherapy has been associated with more favorable outcomes and longer remission 67 , it may be of interest to assess their specific and combined effect on mortality. Further, given the important costs and negative health outcomes associated with the use of benzodiazepines in older adults, alternative treatments such as cognitive-behavioral therapy may be more appropriate in treating anxiety disorders and other related problems 68 .
In summary, the present study underlines the importance of primary care physicians in detecting and providing adequate quality mental health care for older adults with depression and anxiety, as this may be associated with longevity.
Footnotes
Acknowledgment
The authors acknowledge D. Berbiche for merging dataset and the preparation of study variables.
Authors’ Contribution
HMV defined the analytic plan and performed all statistical analyses and wrote the first draft of the paper. CLL contributed to the analytic plan. CLL, SG, and PR contributed to the interpretation of results and revised the manuscript. All authors read and approved the final manuscript.
Data Availability
The authors are not legally authorized to share or publicly publish linked survey and health administrative data due to privacy or ethical restrictions related to the use of administrative provincial health data. Participants were not requested to give informed consent for data sharing. Questions should be addressed to the research ethics committee. The province of Québec’s “Commission d’Accès à l’Information” gave approval to merge these datasets.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The longitudinal ESA Services study was supported by an operating grant from the Fonds de Recherche en santé du Québec (FRSQ) (#16000, #22251, PI: Dr. M Préville). The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript. C. Lamoureux-Lamarche was the recipient of a PhD’s bursary from the Fonds de Recherche du Québec – Santé (FRQS) in partnership with the SPOR Quebec SUPPORT Unit. S Grenier was supported by a Junior 2 salary award from the FRQS during the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the FRSQ en Santé Québec, (grant numbers #16000 and #22251).