
Abstract

Keywords
Introduction and Background
There is an ongoing debate in Canadian medical, legal, and ethical circles regarding the provision of medical assistance in dying (MAiD) for patients with mental illness. We will establish as background that if MAiD became available for psychiatric disorders, patients with borderline personality disorder (BPD) will be among those requesting the service. Therefore, we evaluate relevant concerns regarding MAiD provision to this patient population. This article’s purpose is 2-fold: first, to highlight considerations within the debate of whether MAiD can be appropriate for mental illness such as BPD. Second, to guide the assessment of patients with BPD for eligibility should MAiD for mental illness become available in Canada.
MAiD in Canada
In 2015, the Supreme Court of Canada ruled unanimously in the case of Carter v. Canada to overturn our national prohibition on MAiD. 1 The current MAiD eligibility criteria are from Bill C-14 (see Figure 1). 2
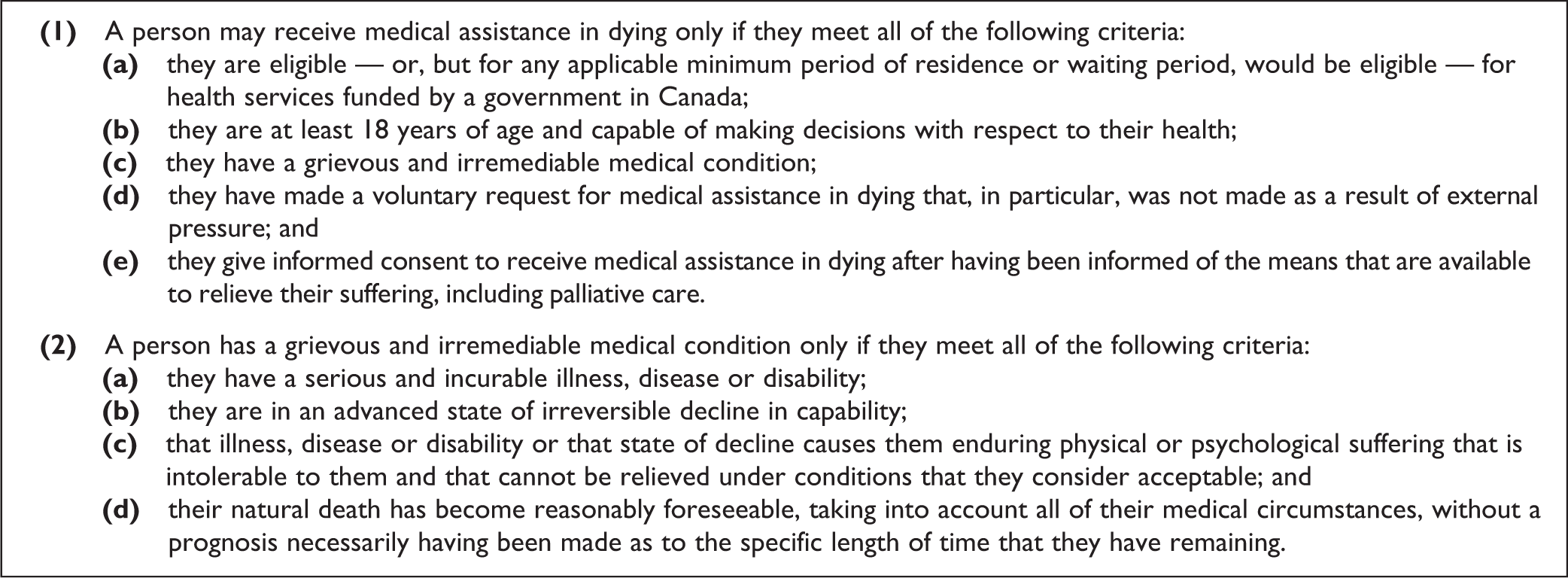
Canadian medical assistance in dying eligibility criteria. 2
Of note, criterion 2d is under review after a Quebec court found the criterion unconstitutional in 2019 (Truchon v. Attorney General of Canada). Data provided by the government of Canada indicate that 13,946 people received MAiD since it became available, with a 26.1% increase in annual cases in 2019 relative to 2018. Therefore, MAiD represented approximately 2.0% of all Canadian deaths in 2019. 3
BPD
BPD is a mental illness associated with emotional instability, interpersonal dysfunction, and significant functional impairment. BPD is prevalent in the population and even more so in health care settings with a 5 year mean prevalence of 1.6% and a lifetime prevalence of 5.9%. 4 In health care settings, patients with BPD make up approximately 20% of psychiatric inpatients and 10% of outpatient visits. 5
BPD among Patients Requesting MAiD
Due to the novelty of MAiD, especially for mental illness, there is limited data available and it largely comes from Western Europe. In review of the literature, we identified 5 relevant studies. All 5 studies included data on the proportion of patients requesting MAiD suffering from an unspecified personality disorder, with results ranging from 41% to 57%. 6,7 The proportion of those that received MAiD ranged from 41% to 54%. 6,8 Only 2 of the studies included data on the proportion of patients requesting MAiD for psychiatric reasons who were diagnosed with BPD specifically, with results ranging from 5.7% to 27%. 8,9 None of the studies published the proportion of those with BPD requesting MAiD that received the service.
These data, although limited, indicate that patients with BPD request MAiD when available and represent a significant proportion of requests made for psychiatric disorders. Given this, the administration of MAiD to this population has been discussed, highlighting concerns including the mutability of suicidal ideation, the effectiveness of psychotherapeutic interventions, the impact of patient–physician communication, and the variable training received by physicians assessing MAiD eligibility. 10 To contribute to this discussion, 3 concerns are examined regarding the provision of MAiD to those with BPD.
Concern 1: Can BPD Cause Suffering?
To meet Canada’s MAiD eligibility criteria from Bill C-14, a patient must be in a state that “…causes them enduring physical or psychological suffering that is intolerable to them and that cannot be relieved under conditions that they consider acceptable.” This criterion requires interpretation, as “suffering” is a term with varying usage among writers and practitioners. On the basis of a literature review, Dees et al. defined suffering as a “profoundly personal experience of an actual or perceived impending threat to the integrity or life of the person, which has a significant duration and a central place in the person’s mind.” 11
In a qualitative study assessing the suffering of psychiatric patients requesting euthanasia, Verhofstadt et al. identified 5 domains of suffering. 12 We believe this framework is generally applicable and useful in understanding the nature of suffering in BPD, particularly the domains of intrapersonal suffering, suffering from interpersonal interaction, and existential suffering. For example, the emotional dysregulation characteristic of BPD may impact emotional reasoning (i.e., mistaking strong emotions for fact) and disrupt social relationships, contributing to interpersonal suffering. Psychiatric suffering was explored again in 2020 by Lengvenyte et al. 13
Supporting the existence of suffering in BPD is the high lifetime rate of suicide and suicide attempts among these patients. A previous review of the literature found the rate of suicide in BPD to be as high as 10%. 14,15 Specifically, a prospective cohort study of patients with BPD demonstrated a 5.9% suicide rate at 24-year follow-up while a longitudinal cohort study with a median follow-up of 18 years suggested a lifetime suicide risk of 6.67% for men with unipolar affective disorders and 0.72% for men without a psychiatric diagnosis. 16,17 The attempted suicide rate among patients with BPD was found to be as high as 85%. 14 Patients with BPD suffer from comorbid conditions, both psychiatric and somatic, that increase the risk of suicide and likely affect the experience and intensity of suffering. 14
While recognizing and understanding suffering in BPD may be helpful to clinicians, suffering as it pertains to MAiD eligibility is subjectively experienced and its tolerability can only be appraised by the physician as a result of extensive dialogue with the patient. 18 The personal nature of this determination leads us to our next concern.
Concern 2: Does BPD Impair a Patient’s Ability to Provide Informed Consent?
The cognitive–affective features of BPD may impact a patient’s ability to provide informed consent for MAiD. Informed consent requirements are under provincial jurisdiction in Canada. Ontario is currently operating under the Substitute Decisions Act of 1992 (SDA) and The Health Care Consent Act of 1996. To be declared incapable of providing informed consent in Ontario, a patient must meet at least 1 of 2 criteria laid out in the SDA. 19
A patient may be deemed incapable if they are unable to understand information that is relevant to making a decision regarding their health. unable to appreciate the reasonably foreseeable consequences of a decision, or lack of decision.
In their independent summary on the state of knowledge surrounding MAiD for mental illness, the Council of Canadian Academies acknowledged that mental illness can affect both the voluntariness of consent and the decision-making capacity that is required. It does not however discuss BPD specifically. 1
In addition to affecting the immediate experience of suffering, the cognitive–affective features of BPD may impact patients’ appreciation of the future course of their suffering. As discussed under Concern #3, the vast majority of patients will obtain remission from BPD; however currently, it is unclear whether it is possible to predict the outcome for individual patients and they may struggle to appreciate these future outcomes. Furthermore, these cognitive–affective features of BPD may impair the decision-making process by patients failing to take time to render a decision or by catastrophizing the worst possible outcome, for example, symptom relief.
Three documented affective–cognitive characteristics of BPD appear as potential impediments to patients’ capacity to appreciate the consequences of their decision. They are (i) impulsivity, 4,20 (ii) attentional biases toward negative stimuli, 21 and (iii) thought distortions regarding the nature of the world, including the need for “protective action” (taking action to avoid future negative emotion). 21 We found no discussion of the effect of these features on a patient’s capacity to provide informed consent, but their potential impact could be as follows.
Impulsivity
Impulsivity includes features such as decreased time to decision making and less attention paid to potential consequences. 22 Patients with BPD consistently choose more immediate awards over rewards delivered at a later time, and thus, impulsivity may impact their decision making around relief of suffering that might come over time. 4 These features may not impact a patient’s ability to eventually understand and appreciate the consequences of their decision but do put patients at risk of making a decision before they have reached an appropriate level of understanding or appreciation.
Attentional Biases
Attentional biases toward negative stimuli may warp a patient’s ability to weigh the consequences of pursuing or not pursuing MAiD. For example, when patients with BPD think of their lives, they may attend disproportionately to events inducing negative rather than positive emotions, thereby compromising their ability to appreciate fully the consequences of MAiD. These negative attentional biases may make the patient discount any hope for the future as evidence has demonstrated that patients with BPD and depression report more hopelessness than depressed patients. 23
Thought Distortions
Although cognitive distortions may occur in individuals without a mental disorder, their occurrence in BPD may impact capacity. A distorted sense of the world in which one perceives their surroundings as bad, painful, and lonely may disrupt a patient’s ability to weigh the consequences of pursuing or not pursuing MAiD, similarly to the negative attentional biases described above. For a more detailed analysis of the effects of cognitive distortions on consent, we recommend the recent paper published by Justine Dembo et al. 18
Beyond accepting that these characteristics may impact a patient’s appreciation of negative consequences, we must consider whether the impact is significant enough to affect the validity of the consent. It has long been understood that the threshold for capacity is related to the seriousness of the decision being made, 24 and the legal and moral basis for this is described in the study of Buchanan. 25 This is a key consideration in our discussion of consent for MAiD, given that MAiD is a decision that carries with it the most significant of consequences.
Given the variable features of BPD in addition to a variable threshold for capacity, it is impossible to say broadly whether patients with BPD are compromised in their ability to provide consent for MAiD. However, it is reasonable to conclude that there are aspects of BPD that could compromise an individual patient’s ability to provide consent, and therefore, these should be considered in the process of any capacity assessment.
Concern 3: Can Suffering from BPD be Considered Irremediable?
Previous work has described variable arguments regarding the nature of irremediability; 26 however, we will discuss irremediability as defined in Bill C-14 specifically which includes a reasonably foreseeable natural death, an incurable illness, and symptoms that are nonrelievable via means that are acceptable to the patient. 2 We will not discuss the foreseeable death criterion, as this is likely being removed imminently. 27 Instead, when determining if a patient with BPD’s suffering fits this definition, the primary difficulty lies with the term “incurable,” which is undefined in most medical literature but has been previously discussed. 1 One proposed option uses a reductionist biological approach to define cure as eradicating an underlying pathophysiology. Unfortunately, the pathophysiologies of mental illness remain poorly characterized and are typically unestablished. The term curable is not frequently used for mental illness, where more often symptom relief or remission is considered.
Within the context of MAiD assessments for patients with BPD, irremediability will likely consist of an inability to sufficiently reduce symptoms and/or suffering. As discussed above, suffering is personal in how it is experienced and evaluated. However, symptom severity can be assessed based on treatment response and has been examined over time.
Symptom relief over time has been documented by a prospective follow-up study of borderline patients over 20 years follow-up. 28 Two outcomes were assessed: remission, no longer meeting BPD criteria for a period of 2 years, and recovery, a global assessment of functioning (GAF) score of 61 or higher. It is worth noting that the GAF score required to be considered in recovery indicates mild residual symptoms or difficulty in social functioning, and the tolerability of this will include the judgment of the patient (see Concern 1). The researchers found that at 16-year follow-up, 99% of patients had achieved a 2-year remission; however, only 59% of patients with BPD had been in recovery for at least 2 years. These data make clear that sustained symptomatic remission from BPD is common; although, sustained recovery is less so (41% of patients had GAF scores below 61 at 16-year follow-up). Patients without sustained recovery could be considered irremediable based on symptom presence and the personal intolerability of social dysfunction; however, these data neither prove nor disprove BPD as irremediable and the meaning of irremediable BPD demands further investigation.
Even if the existence of irremediable BPD were to be established, how this can be accurately determined or predicted remains unclear. Currently unanswered questions include the following: How many therapies must be tried, and for how long, before we are sufficiently certain the disorder is irremediable? Stand-alone evidence-based psychotherapies for BPD have been demonstrated to be effective for borderline symptoms and suicidal features (effect sizes ranging from 0.31 to 0.44). 29 Mehlum et al. recommended adherence to guidelines for state-of-the-art treatment for BPD as a measure of adequate therapeutic interventions prior to considering MAiD. 10 In Canada, there are no accepted guidelines for BPD treatment; although, developing Canadian guidelines could help the profession prepare for MAiD. However, treatment guidelines rarely account for the acceptability of treatment options to individual patients which is paramount given MAiD eligibility only requires treatments acceptable to the patient. This amplifies the importance of considering the impact of personality disorders on treatment refusal. 26 Also worth considering in the determination of irremediability are developmental and maturational factors that may influence what is acceptable or unacceptable to the patient.
Conclusion
The discussion about the role of MAiD for mental illness in Canada will remain a divisive issue politically and ethically. Should MAiD for mental illness become available in Canada, patients with BPD will be among those requesting MAiD. Therefore, to contribute to the discussion, we have reviewed 3 concerns in its application for patients with BPD and drawn the following conclusions. First, we assert suffering in psychiatric illness has been previously described and exists for patients with BPD. Additionally, suffering is a personal and subjective experience that is independently judged by patients in conjunction with the appraising physician. Second, there are cognitive–affective features within BPD that may impact the experience of suffering, the ability of patients to foresee relief from suffering, and their ability to provide informed consent to available treatments and/or MAiD. With the variability in BPD presentations, each case must be considered independently. Finally, current evidence does not rule out the existence of irremediable BPD, however, we have inadequate knowledge to address its existence in a particular patient.
Our review makes clear the need for further research to address the following areas. The existence and nature of irremediable cases of BPD should be explored, while accounting for comorbidity and the potential for self-resolution of suffering over time. If irremediable BPD is established, the threshold at which a patient could be considered irremediable from BPD must be defined. Developing Canadian consensus treatment guidelines for patients with BPD would assist in this determination. Research is required to understand how the cognitive–affective characteristics of BPD may impact consent capacity. Future enquiry should examine the outcomes of MAiD availability on the delivery of services, considering those who receive the intervention, are denied the intervention, and those without a desire for MAiD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Links receives book royalties from the American Psychiatric Association Publishing
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.