
Abstract
Objective
Growing evidence suggests asthma increases perinatal mental illness risk, but few studies have explored the impact of asthma severity and control. Our objective was to explore the association between asthma severity and control and perinatal mental illness risk and the impact of asthma exacerbations during pregnancy on postpartum mental illness risk.
Methods
This was a population-based retrospective cohort study of all women in Ontario, Canada, from 2005 to 2015 with a singleton live birth who used public drug insurance, excluding women with recent history of mental illness. We constructed modified Poisson regression models to assess the risk of perinatal mental illness, defined as a mood or anxiety, psychotic or substance use disorder, self-harm or other mental illness diagnosed from conception to 365 days postnatally. Models controlled for socio-demographic factors and medical history.
Results
There were 62,583 women in the cohort (46.7% between 15 − 24 years), of whom 22.7% had asthma (94.3% mild, 5.7% moderate/severe; 86.5% controlled and 13.5% uncontrolled). After adjustment, there was increased risk of perinatal mental illness with mild asthma (adjusted relative risk [RR]: 1.12; 95% confidence interval [CI], 1.09 to 1.16) and moderate/severe asthma (aRR: 1.16; 95% CI, 1.04 to 1.30) compared to no asthma. Controlled asthma (aRR: 1.11; 95% CI, 1.08 to 1.15) and uncontrolled asthma (aRR: 1.19; 95% CI, 1.11 to 1.27) were also associated with increased perinatal mental illness risk compared to no asthma. Women with worsened asthma during pregnancy had the highest risk of postpartum mental illness compared to no change in asthma status (by severity: aRR: 1.57; 95% CI, 1.36 to 1.80; by control: aRR: 1.37; 95% CI, 1.22 to 1.54).
Conclusion
Asthma is associated with increased risk of perinatal mental illness, particularly in the presence of asthma exacerbations in pregnancy. The results support multidisciplinary collaborative care programmes throughout the perinatal period, especially among women with asthma exacerbations during pregnancy.
Introduction
Asthma is a risk factor for mental illness outside of pregnancy, 1 but few studies have examined the association between asthma and mental illness in the perinatal period. Asthma severity and control, including asthma exacerbations in pregnancy, may influence this association since worse asthma symptoms could lead to increased psychosocial stress or trigger an immunological response. Given that asthma is one of the most common chronic conditions among reproductive-aged individuals, 2 and that perinatal mental illness can have lasting negative effects on mothers and children, 3 an understanding of the impact of asthma on perinatal mental health is essential for informing multidisciplinary preventive and treatment efforts. We examined the association between asthma severity and control and risk of perinatal mental illness and the impact of asthma exacerbations during pregnancy on postpartum mental illness risk.
Methods
This retrospective cohort study used administrative health datasets, linked using unique encoded identifiers and analyzed at formerly the Institute for Clinical Evaluative Sciences (ICES), Ontario, Canada (Supplemental Table 1). We included 15 to 49-year-old women with singleton births (fiscal years 2005−2014), who had Ontario Health Insurance Plan eligibility for ≥2 years pre-conception and received ≥1 prescriptions under the Ontario Drug Benefit Programme from 12 months pre-conception to delivery. Excluded were women with a recent history of mental illness ≤2 years pre-conception. Data use was authorized under section 45 of Ontario’s Personal Health Information Protection Act and does not require ethics review.
Active asthma was defined as ≥2 physician visits or ≥1 hospitalizations due to asthma in the two years pre-conception (Supplemental Table 2). We measured asthma severity and control in the 12 months before conception using a method developed by Firoozi et al. 4 based on patterns of acute health care use and asthma prescriptions, resulting in two asthma severity (mild, moderate/severe) and control categories (controlled, uncontrolled). Asthma exacerbations were defined as worsening in severity or control during pregnancy compared to preconception. The referent comprised women without asthma.
Perinatal mental illness was a mood or anxiety, psychotic or substance use disorder, self-harm or other mental illness recorded in ≥1 family physician or psychiatrist visits, hospitalizations or emergency department visits in pregnancy or up to 365 days postnatally (SupplementalTable 3).
Analyses used modified Poisson regression, adjusting for socio-demographics, asthma comorbidities, other chronic diseases and remote history of mental illness (Supplemental Table 4 and Supplemental Figure 1).
Results
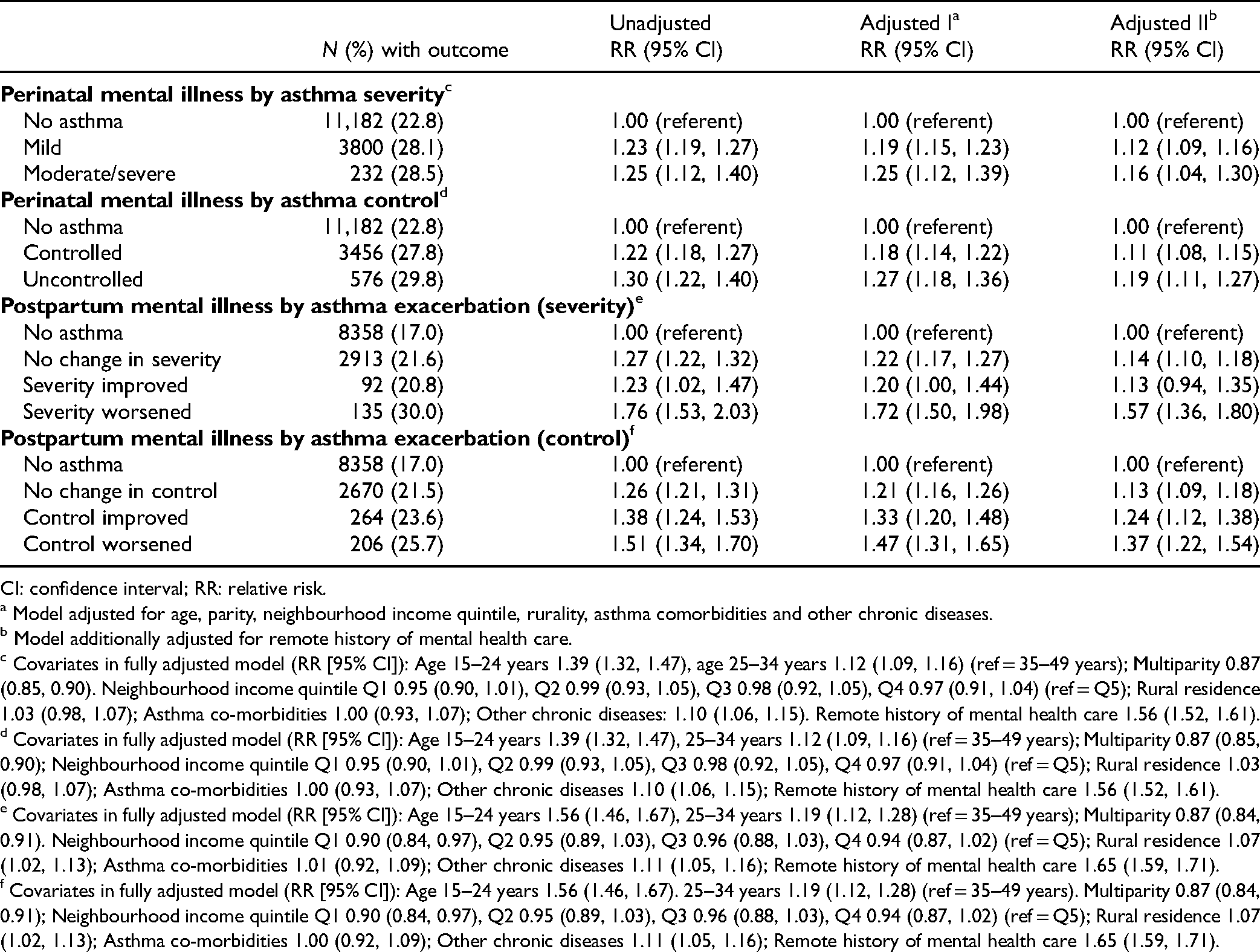
There were 62,583 women in the cohort, of whom 22.7% had asthma (Supplemental Table 5). Women with moderate/severe and mild asthma, compared to those without asthma, had higher rates of perinatal mental illness (28.5% and 28.1% vs 22.8%), corresponding to adjusted relative risks (aRR) of 1.16 (95% confidence interval [CI], 1.04 to 1.30) for moderate/severe and 1.12 (95% CI, 1.09 to 1.16) for mild asthma (Table 1). Women with uncontrolled and controlled asthma, compared to those without asthma, also had higher rates of perinatal mental illness (29.8% and 27.8% vs 22.8%), corresponding to aRRs of 1.19 (95% CI, 1.11 to 1.27) for uncontrolled and 1.11 (95% CI, 1.08 to 1.15) for controlled asthma.
Risk of Perinatal Mental Illness by Asthma Severity and Control.
CI: confidence interval; RR: relative risk.
Model adjusted for age, parity, neighbourhood income quintile, rurality, asthma comorbidities and other chronic diseases.
Model additionally adjusted for remote history of mental health care.
Covariates in fully adjusted model (RR [95% CI]): Age 15–24 years 1.39 (1.32, 1.47), age 25–34 years 1.12 (1.09, 1.16) (ref = 35–49 years); Multiparity 0.87 (0.85, 0.90). Neighbourhood income quintile Q1 0.95 (0.90, 1.01), Q2 0.99 (0.93, 1.05), Q3 0.98 (0.92, 1.05), Q4 0.97 (0.91, 1.04) (ref = Q5); Rural residence 1.03 (0.98, 1.07); Asthma co-morbidities 1.00 (0.93, 1.07); Other chronic diseases: 1.10 (1.06, 1.15). Remote history of mental health care 1.56 (1.52, 1.61).
Covariates in fully adjusted model (RR [95% CI]): Age 15–24 years 1.39 (1.32, 1.47), 25–34 years 1.12 (1.09, 1.16) (ref = 35–49 years); Multiparity 0.87 (0.85, 0.90); Neighbourhood income quintile Q1 0.95 (0.90, 1.01), Q2 0.99 (0.93, 1.05), Q3 0.98 (0.92, 1.05), Q4 0.97 (0.91, 1.04) (ref = Q5); Rural residence 1.03 (0.98, 1.07); Asthma co-morbidities 1.00 (0.93, 1.07); Other chronic diseases 1.10 (1.06, 1.15); Remote history of mental health care 1.56 (1.52, 1.61).
Covariates in fully adjusted model (RR [95% CI]): Age 15–24 years 1.56 (1.46, 1.67), 25–34 years 1.19 (1.12, 1.28) (ref = 35–49 years); Multiparity 0.87 (0.84, 0.91). Neighbourhood income quintile Q1 0.90 (0.84, 0.97), Q2 0.95 (0.89, 1.03), Q3 0.96 (0.88, 1.03), Q4 0.94 (0.87, 1.02) (ref = Q5); Rural residence 1.07 (1.02, 1.13); Asthma co-morbidities 1.01 (0.92, 1.09); Other chronic diseases 1.11 (1.05, 1.16); Remote history of mental health care 1.65 (1.59, 1.71).
Covariates in fully adjusted model (RR [95% CI]): Age 15–24 years 1.56 (1.46, 1.67). 25–34 years 1.19 (1.12, 1.28) (ref = 35–49 years). Multiparity 0.87 (0.84, 0.91); Neighbourhood income quintile Q1 0.90 (0.84, 0.97), Q2 0.95 (0.89, 1.03), Q3 0.96 (0.88, 1.03), Q4 0.94 (0.87, 1.02) (ref = Q5); Rural residence 1.07 (1.02, 1.13); Asthma co-morbidities 1.00 (0.92, 1.09); Other chronic diseases 1.11 (1.05, 1.16); Remote history of mental health care 1.65 (1.59, 1.71).
Compared to women without asthma, postpartum mental illness risk was greatest in women with worsened asthma severity in pregnancy (aRR: 1.57; 95% CI, 1.36 to 1.80), followed by no change (aRR: 1.14; 95% CI, 1.10 to 1.18). Compared to women without asthma, postpartum mental illness risk was greatest in women with worsened control (aRR: 1.37; 95% CI, 1.22 to 1.54), followed by improved control (aRR: 1.24; 95% CI, 1.12 to 1.38; Table 1 and Supplemental Table 6).
Results were similar when prenatal and postpartum mental illness were examined separately (Supplemental Table 7) and when we required ≥2 physician visits to define perinatal mental illness (Supplemental Table 8).
Discussion
In this population-based study, asthma was associated with a small increase in perinatal mental illness risk, with slightly greater risk with moderate/severe and uncontrolled asthma compared to mild and controlled asthma, respectively. We observed stronger associations in the presence of asthma exacerbations in pregnancy. A UK study examined asthma severity by asthma medication use in a cohort of >280,000 pregnancies, and similar to our results, reported higher risk of prenatal depression among women with severe asthma versus those with unmedicated asthma, as well as an association between asthma exacerbations before pregnancy and increased risk of prenatal depression. 5
Reproductive-aged women who receive Ontario Drug Benefits are those with disabilities on social assistance, or with high prescription costs (7.4% of the obstetric population), which may reduce study generalizability. Measurement of asthma severity and control was limited by lack of information about symptoms, which may vary by season. Perinatal mental illness may have been under-ascertained due to lack of universal screening guidelines in Ontario, and other barriers to seeking care. Individual-level socio-economic characteristics and social support were unavailable.
Our results reflect the possible utility of multidisciplinary collaborative care programmes to optimize perinatal mental health outcomes among women with severe or uncontrolled asthma, including perinatal mental illness screening and early intervention, particularly for those with asthma exacerbations during pregnancy.
Data Access
The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (e.g., healthcare organizations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at www.ices.on.ca/DAS (email: das@ices.on.ca). The full dataset creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programmes may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437211039790 - Supplemental material for Asthma Severity and Control and Their Association With Perinatal Mental Illness
Supplemental material, sj-docx-1-cpa-10.1177_07067437211039790 for Asthma Severity and Control and Their Association With Perinatal Mental Illness by Amira M. Aker, Anne L. Stephenson, Andrew S. Wilton, Simone N. Vigod, Cindy-Lee Dennis, Astrid Guttmann and Hilary K. Brown in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Government of Ontario is intended or should be inferred. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed herein are those of the author and not necessarily those of CIHI. We thank IQVIA Solutions Canada Inc. for use of their drug information file.
Declaration of Conflicting Interests
SV receives royalties for authorship of materials related to depression and pregnancy from UpToDate Inc. All other authors have no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. This study also received funding from: Canadian Institutes of Health Research [Grant #376290 to HKB]. Parts of this material are based on data and information compiled and provided by: [OHIP, CIHI, OMHRS, NACRS, MOMBABY and ODB]. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. The funding agency had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; or decision to submit the manuscript for publication. This research was undertaken, in part, thanks to funding from the Canada Research Chairs Program to HKB.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.