
Abstract
Objective:
Telehealth is being increasingly incorporated into the delivery of mental health care and has received widespread attention during the COVID-19 pandemic for its ability to facilitate care during physical distancing restrictions. Videoconferencing is a common telehealth modality for delivering psychotherapy and has demonstrated similar outcomes to those of face-to-face therapy. Cognitive behavioural therapy (CBT) is the most common psychotherapy evaluated across various telehealth modalities; however, studies on CBT delivered via videoconference, particularly in a group therapy format, are lacking. Further, little research exists on videoconference group CBT for anxiety disorders. Accordingly, the present study compared the outcomes of group CBT for anxiety and related disorders delivered via videoconference versus face-to-face.
Method:
Using a non-randomized design, data on attendance, dropout, clinical outcomes, and functional impairment were collected from 413 adult outpatients of a tertiary care anxiety disorders clinic who attended a CBT group for panic disorder/agoraphobia, social anxiety disorder, generalized anxiety disorder (GAD), or obsessive-compulsive disorder delivered either face-to-face (pre-COVID-19 pandemic) or via videoconference (since the onset of COVID-19 pandemic). Outcomes were assessed using well-validated self-report measures. Data were collected pre-treatment, across 12 weekly sessions, and post-treatment. Intent-to-treat analyses were applied to symptom outcome measures.
Results:
Face-to-face CBT conferred only a slight benefit over videoconference CBT for symptom outcomes across all groups, but when assessed individually, only the GAD group showed greater symptom improvement in the face-to-face format. Effect sizes for significant differences between the delivery formats were small. Participants in videoconference groups tended to have slightly higher attendance rates in some instances, whereas functional improvement and treatment dropout were comparable across the delivery formats.
Conclusions:
Results provide preliminary evidence that videoconference group CBT for anxiety and related disorders may be a promising and effective alternative to face-to-face CBT. Additional research is needed to establish equivalence between these delivery formats.
Introduction
As technology has become widely accessible to health-care consumers, with 99.3% of Canadian households subscribing to either mobile or Internet services, 1 telehealth is being increasingly incorporated into the delivery of health care. 2,3 The principal advantage of telehealth is its ability to reduce access-to-care barriers such as limited health services in remote communities, 3,4 travel costs, 5,6 patients’ functional limitations, 7,8 and stigma associated with certain types of care. 9,10 Since the outbreak of the COVID-19 pandemic, telehealth has additionally received widespread attention for its ability to facilitate an alternative avenue to care while reducing the risk of disease transmission. 11 –13 Indeed, recent reports highlight the explosive expansion of telehealth services during COVID-19, 14 –17 which has transformed health-care delivery across numerous systems. 17
Telehealth has been particularly actively adopted in the mental health field, 18 –21 where it is termed telemental health. A common modality in telemental health is videoconferencing, which facilitates real-time communication between users at different locations using both audio and video input. Telemental health has demonstrated feasibility and acceptability when used for diagnostic assessment and treatment services across diverse clinical presentations, populations, and age groups. 18,19,22 Furthermore, outcomes of various videoconference interventions (e.g., psychotropic medication, psychotherapy, combination treatment) have generally demonstrated symptom improvement comparable to face-to-face interventions for common clinical presentations (e.g., depression, anxiety, posttraumatic stress disorder [PTSD]). 23 –31 Similarly, treatment adherence, 25 attendance, 30 dropout, 30 and satisfaction 24 –26,30 have been shown to be comparable between videoconference and face-to-face interventions.
Evaluations of videoconference psychotherapy in particular have largely focused on cognitive behavioural therapy (CBT), 32 an evidence-based treatment for a wide range of disorders. 33 Consistent with the broader literature on videoconference interventions, studies of videoconference CBT support its feasibility, 34 and preliminary findings suggest similar clinical outcomes to those of face-to-face CBT for concerns such as anxiety and depressive disorders, 26,28,29 PTSD, 31,35 and bulimia nervosa. 36 Similarities in clinical outcomes have further been reported in systematic reviews. 37 –39
Although promising effects have thus far been reported, when compared to the volume of research on other telemental health modalities, considerably less literature has focused on videoconference CBT. 37,40,41 Furthermore, most work in this area has investigated individual rather than group CBT. 32 While evaluations of videoconference group CBT are scant, a recent systematic review demonstrated that generally, group-based psychotherapies are feasible and efficacious in a videoconference format. 42 The few studies that have more specifically evaluated videoconference group CBT have primarily focused on PTSD, with results demonstrating outcomes similar to face-to-face CBT groups. 30,43 –45
Surprisingly, there is little research on videoconference CBT groups for anxiety disorders, the most prevalent psychiatric disorders 46 with a high burden of illness. 47 CBT is the psychological treatment of choice for anxiety disorders, 48,49 and, in a face-to-face context, CBT groups for anxiety disorders are as efficacious as individual CBT. 50 To our knowledge, no studies have evaluated anxiety outcomes in videoconference group CBT for anxiety disorders, highlighting the need for further research to establish the effectiveness of this treatment modality for these common disorders.
Group therapy offered via videoconference has the potential to be resource efficient (e.g., more patients can be seen concurrently without the need for more physical space) while conferring additional benefits of telehealth. These potential benefits must be considered alongside any unique resource requirements for videoconferencing, such as technological equipment and the number of clinicians required to facilitate a videoconference group. The development of accessible mental health interventions is highly relevant during the COVID-19 pandemic, which has seen a marked rise in reported mental distress in both general 51 –53 and psychiatric 54 populations alongside access-to-care barriers associated with physical distancing. It is also important within the broader mental health care milieu, where numerous barriers to accessing mental health care have been identified. 55
The purpose of the current study was to conduct a preliminary analysis of outcomes from group CBT for anxiety and related disorders delivered via videoconference versus face-to-face. These treatments were compared within a tertiary care specialist anxiety disorders clinic, which, like many health services during COVID-19, rapidly pivoted from in-clinic face-to-face care to remote care via videoconference. Using a non-randomized design, data on clinical outcomes, attendance, dropout, and functional impairment were collected from groups delivered via videoconference in spring/summer 2020 and compared to respective data from face-to-face groups collected prior to the pandemic. Our goal was to contribute our findings to the telehealth literature during a time when various stakeholders are seeking novel ways to reduce barriers to mental health care. Based on the reviewed literature, we hypothesized that we would observe similar outcomes between group CBT delivered via these two modalities with respect to symptom change, treatment attendance, dropout, and functioning.
Methods
Participants
Participants were outpatients of a tertiary care anxiety disorders clinic in a public hospital in Hamilton, Ontario, who consented to the inclusion of their demographic and clinical information in a research database. Inclusion criteria for research participation paralleled the eligibility criteria for treatment, including age 18 or older, a current Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) anxiety or related disorder diagnosis for which group treatment was available, and English language proficiency. Exclusion criteria included other more pressing clinical issues (e.g., another disorder causing more distress/impairment, active suicidality, significant substance use). We elected to include individuals (n = 6) who completed two different courses of CBT (i.e., completed a group for one disorder followed by a group, later, for a different disorder) within the study period, resulting in a sample of 419 observations from 413 unique individuals.
Participants’ mean age was 34.94 years (SD = 12.27). The majority identified as female (68.4%), white (87.4%), in a relationship (62.9%), and had completed college or university (56.8%). All participants had a primary diagnosis of a DSM-5 anxiety or related disorder (panic disorder and/or agoraphobia [PDA], social anxiety disorder [SAD], generalized anxiety disorder [GAD], or obsessive-compulsive disorder [OCD]), as determined by a semi-structured psychodiagnostic interview 56 (73.0%) or psychiatric consultation (27.0%). Forty-nine percent of participants had at least two diagnoses, most commonly another anxiety or mood disorder. For additional sample characteristics, see Table 1.
Baseline Sample Characteristics.
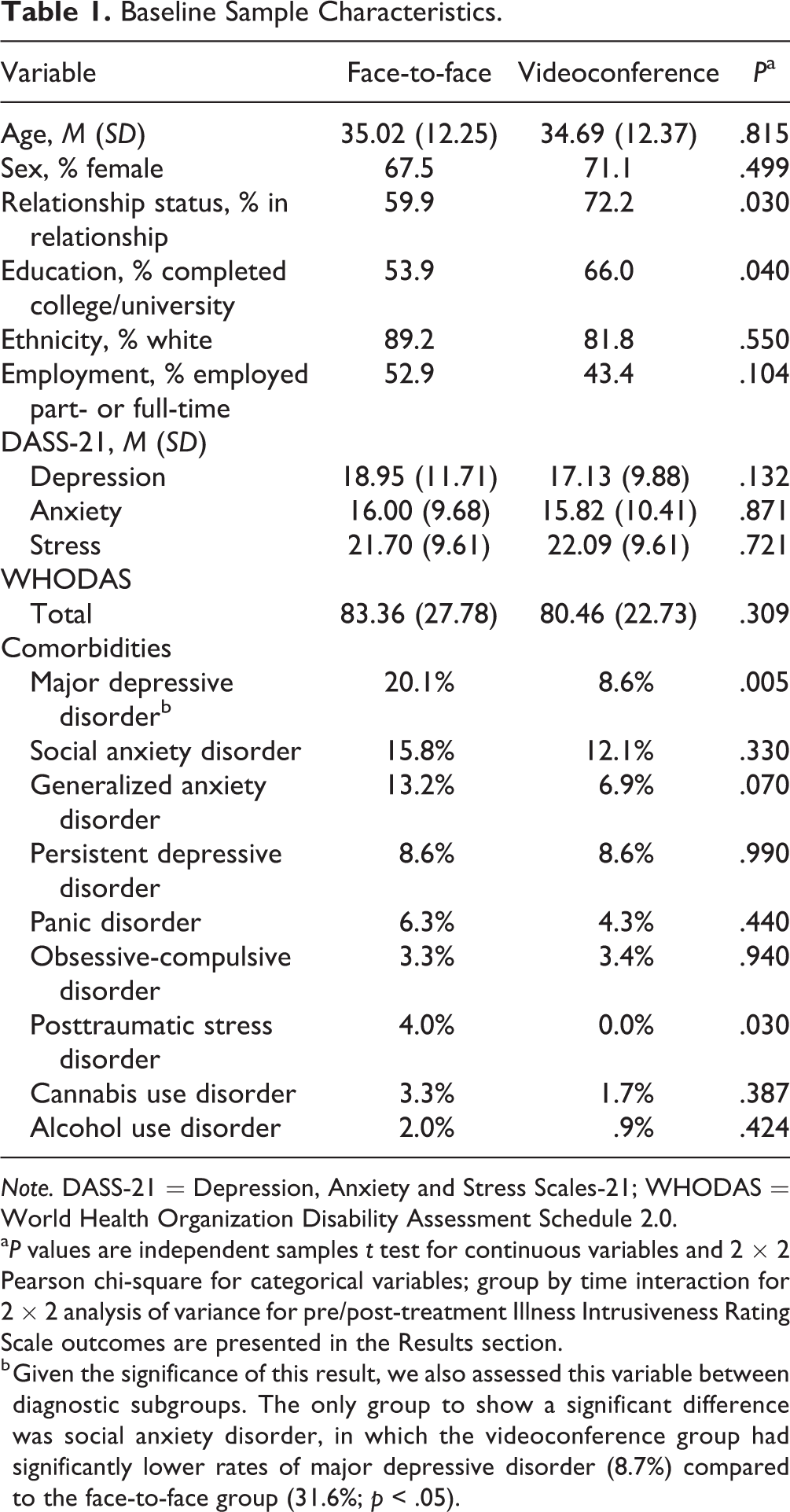
Note. DASS-21 = Depression, Anxiety and Stress Scales-21; WHODAS = World Health Organization Disability Assessment Schedule 2.0.
a P values are independent samples t test for continuous variables and 2 × 2 Pearson chi-square for categorical variables; group by time interaction for 2 × 2 analysis of variance for pre/post-treatment Illness Intrusiveness Rating Scale outcomes are presented in the Results section.
b Given the significance of this result, we also assessed this variable between diagnostic subgroups. The only group to show a significant difference was social anxiety disorder, in which the videoconference group had significantly lower rates of major depressive disorder (8.7%) compared to the face-to-face group (31.6%; p < .05).
Treatment
Both face-to-face and videoconference CBT were facilitated using 12-session disorder-specific manualized CBT group protocols for SAD, PDA, GAD, and OCD. The treatment manuals were developed at our clinic based on existing widely used CBT protocols. 57 –66 The same manuals were used for both treatment modalities, but additional supplementary materials were developed for the videoconference groups detailing in-session exposures suitable for videoconferencing. To prepare for the delivery of the videoconference groups, we consulted other teams with experience in videoconference treatment, reviewed the literature on virtual treatments, and held numerous meetings to plan risk management, engagement, and in-session exposures. For both delivery formats, 2-hour weekly group sessions were facilitated by two therapists, including at least one experienced clinician (e.g., psychologist, social worker) and another clinician or a clinical learner. The same therapists facilitated treatment through both modalities. The mean number of participants per group was 9.79 (SD = 2.31).
Face-to-face groups were facilitated in conference rooms at the clinic, with participants seated around a large table. A whiteboard was used to deliver some of the treatment content. Videoconference groups were facilitated through a secure cloud-based platform, Zoom Video Communications Inc., 67 which participants accessed through their electronic medical record. Participants used a range of electronic devices to attend sessions, most commonly a laptop (55.4%) and a smart phone (15.4%), although only 56% of participants reported on this variable. Participants attended the videoconference sessions from their home or other private environment. They received extensive operational instructions for the videoconference platform and guidelines to ensure appropriate decorum and participation using this platform. Group norms were established to approximate face-to-face treatment (e.g., video on with face showing; “gallery view” to simultaneously see the therapists and other participants). Videoconference sessions were provided in real time. A screen share function was used to display a virtual whiteboard on which some of the treatment material was presented; content from the treatment manuals was additionally screen-shared.
Measures
Psychodiagnosis
Current diagnoses were determined with either a psychiatric interview or the Diagnostic Assessment Research Tool (DART), 56 a semi-structured diagnostic interview for assessing DSM-5 mental disorders. Preliminary findings demonstrate excellent construct validity of DART modules as well as good convergent and discriminant validity. 68
Baseline distress and functioning
Distress at pre-treatment was assessed with the Depression, Anxiety and Stress Scales-21 (DASS-21), 69 a psychometrically sound 70 self-report measure comprised of three 7-item scales assessing symptoms of depression, anxious arousal, and stress (tension/negative affect). Global functioning was assessed pre-treatment with the World Health Organization Disability Assessment Schedule-2.0, 71 a 36-item measure of self-reported disability secondary to psychiatric and medical illness.
Attendance and dropout
Group therapists recorded weekly treatment attendance on an attendance record. Dropout was conceptualized as attending <8 sessions and not attending the final three sessions.
Symptom change
Symptom change was assessed with disorder-specific, self-report measures, including the following: in the SAD groups, the Social Phobia Inventory (SPIN), 72 a 17-item measure of social anxiety symptoms; in the PDA groups, the Panic Disorder Severity Scale–Self-Report (PDSS-SR), 73,74 a 7-item measure of the frequency of panic attacks and associated distress, avoidance, and functional impairment; in the GAD groups, the Penn State Worry Questionnaire (PSWQ), 75 a 16-item measure of trait-like worry severity, and the Penn State Worry Questionnaire–Past Week (PSWQ-PW), 76 a 15-item measure adapted for weekly assessment of worry; and in the OCD groups, the Obsessive Compulsive Inventory–Revised (OCI-R), 77 an 18-item measure of the severity of OCD symptoms. These widely used measures have demonstrated sound psychometric properties in clinical samples (SPIN, 72,78 PDSS-SR, 74,79 PSWQ, 80,81 and OCI-R 82 ). The SPIN, PDSS-SR, and OCI-R were administered pre- and post-treatment and weekly for 12 sessions. The PSWQ was administered pre- and post-treatment, and the PSWQ-PW was administered weekly.
Change in functioning
Functional changes from pre- to post-treatment were assessed with the Illness Intrusiveness Rating Scale (IIRS), 83 a 13-item self-report measure of functional impairment secondary to illness assessed across Instrumental, Intimacy, and Relationships and Personal Development subscales. The IIRS has demonstrated sound psychometric properties in psychiatric populations. 84
Procedures
All procedures were approved by the Hamilton Integrated Research Ethics Board. Psychometric assessment was completed upon entry to the program. Participants were referred to group CBT if their principal concern matched the disorder treated in one of the available groups. Those who attended group CBT between May 2018 and December 2019 received the treatment face-to-face, and those who attended between May 2020 and September 2020 received the treatment via videoconference.
Self-report measures were administered electronically via a browser-based data collection software (Research Electronic Data Capture). 85 Participants received emailed links with a specified period to complete the measures. Group therapists completed the attendance record on a weekly basis.
Statistical Analysis
Hierarchical linear modelling (HLM) 86 was used to assess the effect of group (face-to-face vs. videoconference) on the trajectory of change in symptom severity over time. Primary outcomes were assessed with time (coded weekly) at Level 1 and group at Level 2. Single-level HLMs were also performed on each of the face-to-face and videoconference groups, individually, to assess the difference in effect size between treatment formats. An intent-to-treat approach was taken for symptom outcome measures to maximize sample size and external validity of results. Data were collected weekly from pre-treatment, through 12 weeks of treatment, to post-treatment (14 data points). Finally, a series of independent samples t tests and Pearson chi-squares were performed to assess attendance variables and pre-/post-change in IIRS scores. Given the sample-intensive nature of HLM analyses, we prioritized maximizing the total number of observations rather than ensuring equal group size between face-to-face and videoconference samples.
Z-scores were calculated for comparisons across groups. Given differences in methodology between validation studies for each of the respective questionnaires, z-scores were used for the full-sample analysis, whereas raw scores were used for individual group analyses. Where possible, sample means for non-anxious controls were used. All sample means were gathered from each questionnaire’s respective validation study. These were 48.80 (SD = 13.80) for the PSWQ, 75 18.82 (SD = 11.10) for the OCI-R, 77 and 6.10 (SD = 6.00) for the PDSS-SR. 87 No control sample was available, to our knowledge, for the PSWQ-PW. We elected to use a mid-treatment reference score of 45.43 (SD = 16.48). 76 The SPIN score for non-anxious controls is 12.10 (SD = 9.30). 72 Given this score is low relative to sample means for SAD, this value results in overly inflated z-scores relative to the other samples in the present study. Furthermore, some researchers also support a higher cut-off value of 30 on the SPIN. 88,89 Therefore, the sample mean of 22.70 (SD = 10.00) for the “mildly impaired” subsample was used. 72
Results
There were no baseline differences, as assessed by independent samples t tests, between the face-to-face and videoconference groups on any outcome variable (see Table 1).
Attendance and Dropout
Significantly more sessions were attended by participants in the videoconference versus face-to-face GAD groups, t(146) = −2.02, p = .045, d = .17. The difference in attendance between the two delivery formats approached significance for the full sample, t(371) = −1.94, p = .053, d = .10. Figure 1 shows the mean session attendance for all groups. Treatment dropout did not differ significantly between groups, with observed dropout rates of 24.5% for face-to-face and 15.3% for videoconference, χ2 (1, N = 371) = 3.18, P = 0.08, φ = .09.
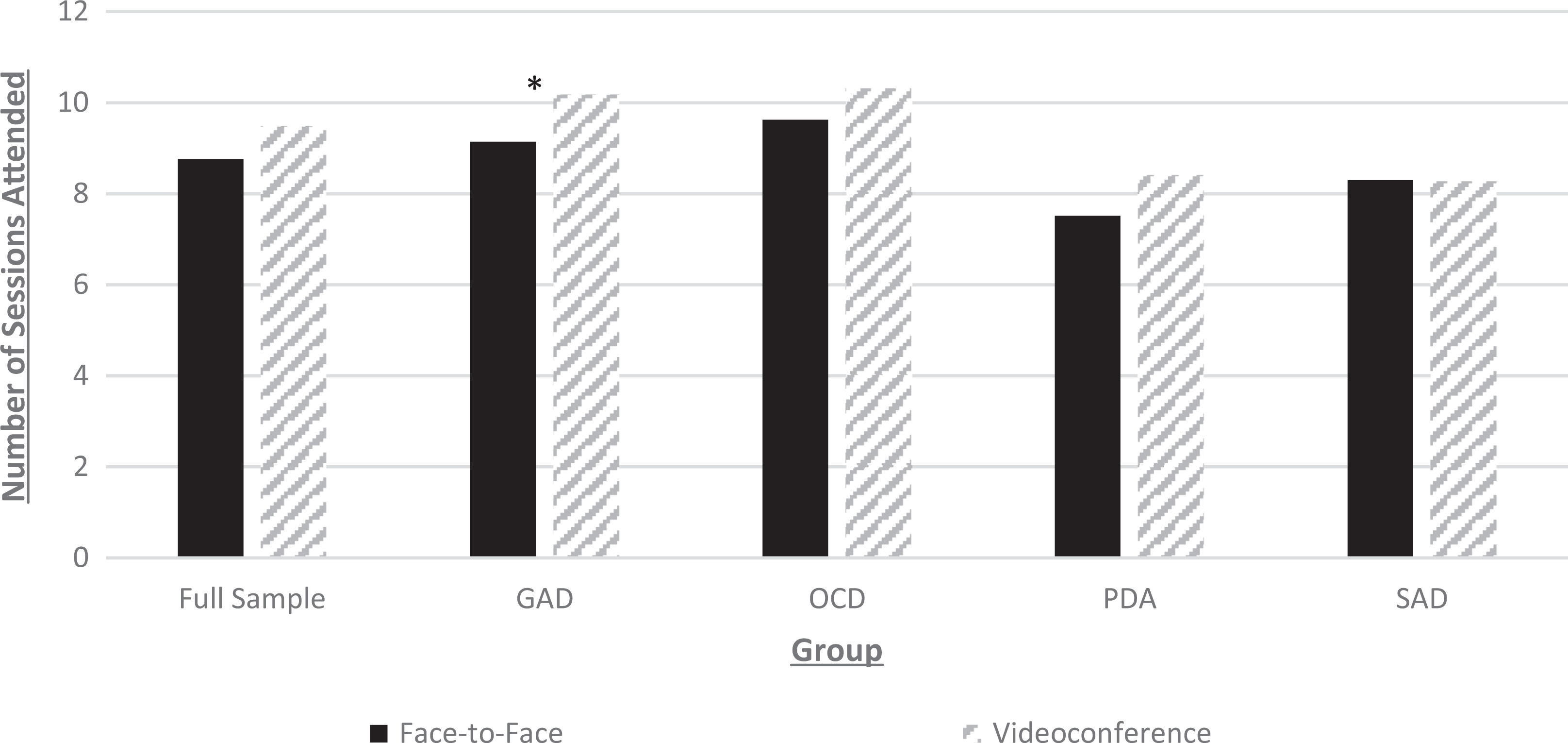
Session attendance between face-to-face and videoconference group delivery (total 12 sessions). GAD = generalized anxiety disorder; OCD = obsessive-compulsive disorder; PDA = panic disorder and/or agoraphobia; SAD = social anxiety disorder. *P < 0.05.
Symptom Change over Time
There was a significant effect of group in the full-sample analysis, b = .05, SE = .01, t = 4.74, P < 0.001, d = .23, and in the GAD subsample, b = .69, SE = .01, t = 2.70, P = 0.008, d = .20. These results indicate a small but significant positive effect of face-to-face treatment on reduction in symptom severity over time, relative to videoconference treatment (see Table 2 and Figure 2). This effect was not significant for SAD (P = 0.11), PDA (P = 0.17), and OCD (P = 0.69) groups.
Hierarchical Linear Modelling Assessing the Change in Primary Outcome Variables over Time from Pre- to Post-treatment.
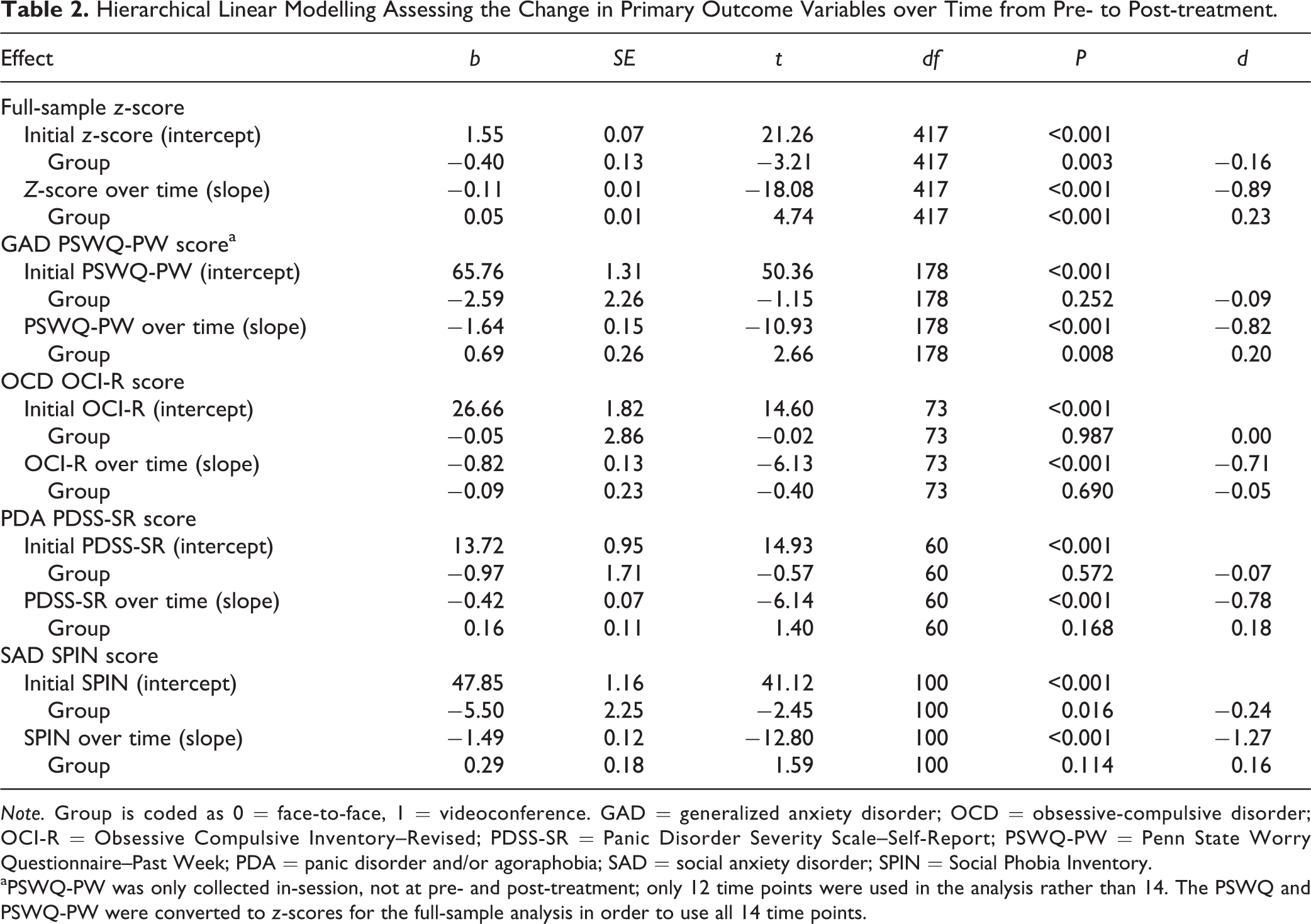
Note. Group is coded as 0 = face-to-face, 1 = videoconference. GAD = generalized anxiety disorder; OCD = obsessive-compulsive disorder; OCI-R = Obsessive Compulsive Inventory–Revised; PDSS-SR = Panic Disorder Severity Scale–Self-Report; PSWQ-PW = Penn State Worry Questionnaire–Past Week; PDA = panic disorder and/or agoraphobia; SAD = social anxiety disorder; SPIN = Social Phobia Inventory.
aPSWQ-PW was only collected in-session, not at pre- and post-treatment; only 12 time points were used in the analysis rather than 14. The PSWQ and PSWQ-PW were converted to z-scores for the full-sample analysis in order to use all 14 time points.
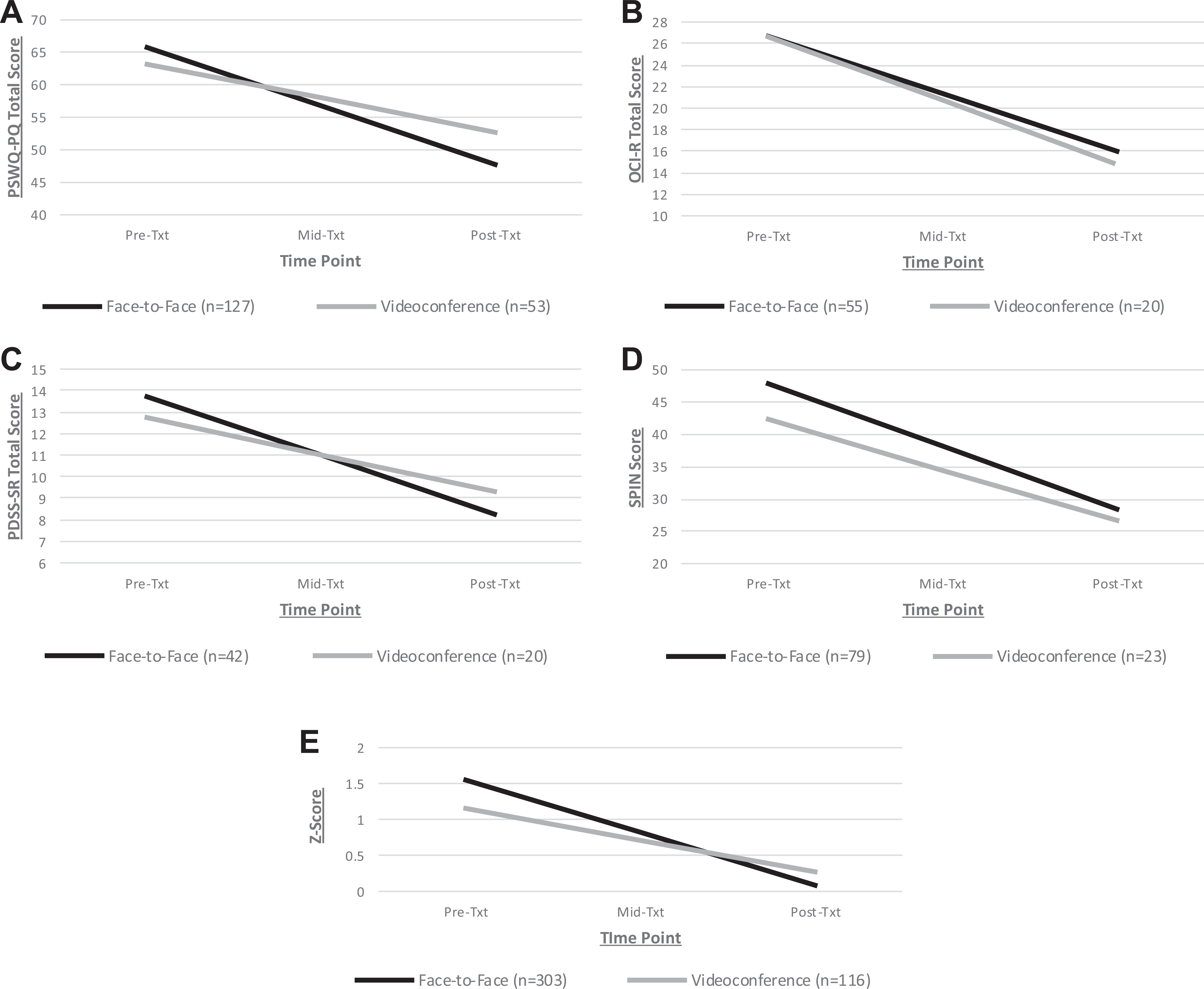
Results of 2-level hierarchical linear modelling models with group (0 = face-to-face, 1 = videoconference) predicting trajectory of change in symptom severity over the course of treatment. (A) GAD PSWQ-PW scores over time. (B) OCD OCI-R scores over time. (C) PDA PDSS-SR scores over time. (D) SAD SPIN scores over time. (E) All groups z-scores over time. GAD = generalized anxiety disorder; OCD = obsessive-compulsive disorder; OCI-R = Obsessive Compulsive Inventory–Revised; PDA = panic disorder and/or agoraphobia; PDSS-SR = Panic Disorder Severity Scale–Self-Report; PSWQ-PW = Penn State Worry Questionnaire–Past Week; SAD = social anxiety disorder; SPIN = Social Phobia Inventory.
Of note, there was an effect of group on the intercept for the full sample. To assess whether baseline z-score had any effect, we performed a model including group, baseline z-score, and the group × z-score interaction at Level 2. Both group, b = .03, SE = .01, t = 3.48, P < 0.001, d = .19, and baseline z-score, b= −.04, SE = .01, t = -6.97, P < 0.001, d = −.37, were independently significant predictors of change in symptom severity over time, but the interaction was not, b = .01, SE = .01, t = .53, P = 0.60, d = .03. These results indicate that participants who received face-to-face treatment achieved greater symptom severity reductions regardless of baseline severity.
Effect sizes (Cohen’s d) for treatment were mostly comparable between face-to-face and videoconference delivery, with videoconferencing tending to have slightly lower effects than face-to-face. This was true for the full sample (videoconference = −.90, face-to-face = −1.04), GAD (videoconference = −.61, face-to-face = −.97), PDA (videoconference = −.67, face-to-face = −.95), and SAD (videoconference = −1.43, face-to-face = −1.44) but not OCD (videoconference = −1.11, face-to-face = −.82).
Given heterogeneous comorbidities throughout the sample, and the higher incidence of depression in the face-to-face vs. videoconference groups, we performed supplementary analyses observing the effect of group at Level 2 while controlling for comorbidities and DASS-21 depression scores at baseline at Level 1. Although DASS-21 depression was an independently significant predictor of the primary symptom outcome measure in each group and in the full sample (with greater depression scores indicating worse symptom severity, Ps < 0.001), this was not the case for overall comorbidities (Ps = 0.057 to 0.83). Most importantly, neither depression nor comorbidities significantly impacted the effects of group at Level 2. This finding was supported by nearly identical significance and deviance statistics between the models with and without comorbidity variables.
Change in Functioning
All IIRS scores (see Table 3) showed significant main effects of time (Ps < 0.001), indicating improved functional impairment over the course of treatment. Neither the main effects of group nor the group by time interactions were significant (Ps > 0.05) for the IIRS total or subscale scores.
2 × 2 Group × Time ANOVA for IIRS Total and Subscale Scores.
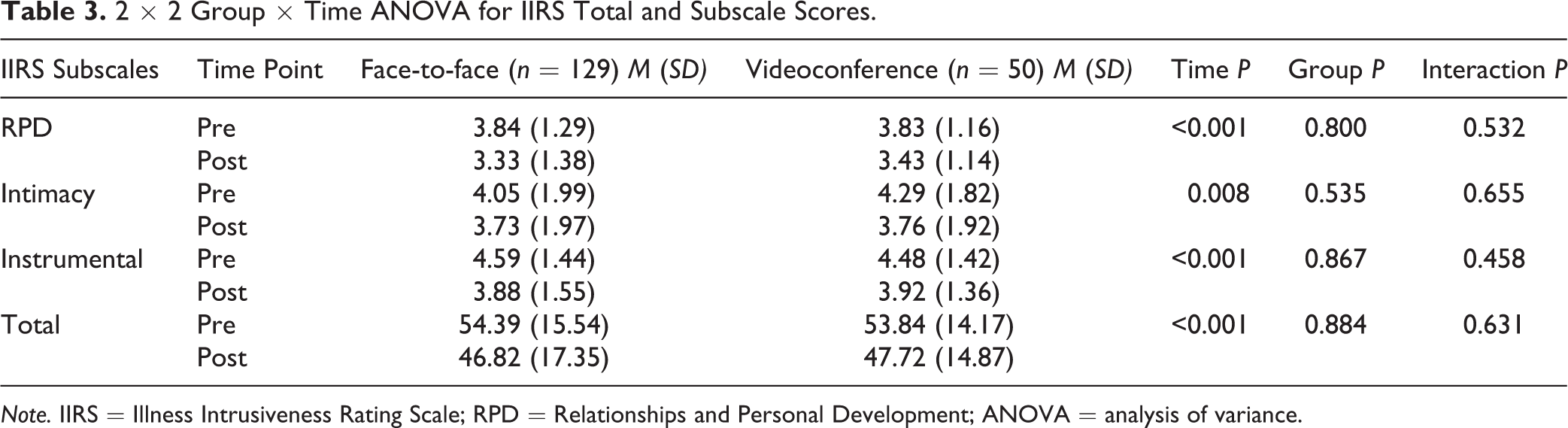
Note. IIRS = Illness Intrusiveness Rating Scale; RPD = Relationships and Personal Development; ANOVA = analysis of variance.
Discussion
This study compared outcomes in face-to-face and videoconference group CBT for anxiety and related disorders. When evaluating symptom outcomes across all groups, there were only slight differences between the treatment formats, conferring a small benefit for face-to-face delivery, although this was not the case for all groups. When assessed individually, only the GAD group showed greater symptom improvement in the face-to-face format. Furthermore, effect sizes for significant differences between formats were small (d = .20 to .23). It is possible, however, that subsample analyses were not adequately powered to detect differences between groups via HLM. Participants in videoconference groups tended to have slightly higher attendance rates in some instances, whereas the two treatment modalities evidenced comparable improvement in illness intrusiveness. Given the relatively small sample size of the videoconference groups, these results are preliminary; however, they point towards potentially promising similarities in outcomes between virtual and in-person treatment delivery.
Despite the distress and uncertainty associated with COVID-19, 51 –54,90 our findings demonstrate that group CBT for anxiety can be successfully delivered via videoconference even during a pandemic. Indeed, participants who received videoconference group therapy did so during a time when we might anticipate poorer anxiety treatment outcomes, irrespective of the mode of delivery. Further, the small effect sizes we observed between delivery formats on symptom measures are similar to those reported elsewhere, 26,91 and the medium-to-large effect sizes we observed in symptom changes over time are generally consistent with those reported in meta-analyses of CBT. 92 –94
The finding of greater GAD symptom improvement in face-to-face versus videoconference delivery warrants attention. GAD is characterized by intolerance of uncertainty, causing excessive worry about new situations. 95 –97 With telehealth care being unfamiliar to many individuals, videoconferencing might have provoked greater treatment-related anxiety among the GAD sample, hampering their outcomes. Additionally, symptom improvement might have been more difficult to achieve in this population via videoconference treatment during a global catastrophic event compared to that observed in the face-to-face treatment predating the pandemic. This is tempered with the observation that at least at baseline, both groups did not significantly differ in reported depression, anxiety, or stress.
Importantly, the results of this investigation support positive outcomes in CBT delivered via videoconference despite this treatment being rapidly adapted to a virtual context to continue service delivery during a pandemic. Although the shift necessitated quick action, important steps were nonetheless taken by our team to optimize treatment engagement, including research and preparation to apply this model of care; adaptation, where relevant, of treatment components; and extensive support to patients to increase the usability of the technology.
As this investigation has pioneered some of the first data comparing face-to-face versus videoconference group-based CBT for anxiety disorders, it has brought forth important limitations and considerations for future research. First, while this investigation is timely and contributes to the literature supporting videoconference group psychotherapy during a globally challenging period, our results may have been affected by important confounds that were not possible to control in the current study design. First, the face-to-face and videoconference groups were facilitated during different time periods. It is necessary to compare service delivery formats in an ongoing fashion to determine comparability as environmental and societal stressors change. This would additionally clarify whether the benefits to attendance we observed in videoconference relative to face-to-face treatment are better explained by the delivery format, other factors such as greater engagement in treatment offered during global distress, or other pandemic conditions that might have uniquely impacted the sample attending videoconference groups.
Second, with only those equipped with an electronic device participating in videoconferencing, self-selection bias may have influenced our results. Higher retention may have occurred due to a motivated and technologically adept cohort opting to enter treatment in this format. Moreover, the face-to-face versus videoconference groups significantly differed in education status, with more participants in the latter having a post-graduate degree. Whether this difference underlies self-selection, such that a cohort with higher socioeconomic status entered videoconference treatment, remains to be further investigated.
It is also notable that we implemented a treatment model with participants attending videoconference sessions from their homes, but various other models are possible (e.g., videoconference sessions attended from a local clinic, videoconference sessions augmented with prerecorded psychoeducational videos). The extent to which our findings are consistent with, or diverge from, those implementing other variations of videoconferencing is an important avenue for future research.
Although previous work has demonstrated similar treatment satisfaction between telepsychotherapy and in-person psychotherapy, 24 –26,29 this investigation is additionally limited in having not measured patient satisfaction with treatment. Future qualitative research may be valuable to elucidate patients’ experiences with videoconference group psychotherapy, particularly in a pandemic context. We also did not measure group process mechanisms (e.g., group cohesion), which warrant closer examination. A nascent literature suggests small reductions in cohesion in videoconference versus face-to-face groups but no significant impact on outcome. 42 Finally, in addition to benefits conferred by videoconferencing, there are limitations to consider (e.g., online or environmental distractions during sessions, requirement of an electronic device, type of device used to attend sessions).
The results of this preliminary investigation suggest that videoconference group CBT for anxiety disorders may be a reasonable alternative to face-to-face treatment, which is particularly valuable in the context of the COVID-19 pandemic but also holds broader potential to widen the accessibility of mental health services. Future research is critical to strengthen the emerging literature on group CBT for anxiety disorders via videoconference, with efforts to determine whether equivalence in modalities can be claimed (i.e., through randomized controlled trials).
Footnotes
Authors’ Note
For access to the data, please contact the corresponding author.
Acknowledgements
We wish to acknowledge the clinicians at the Anxiety Treatment and Research Clinic at St. Joseph’s Healthcare Hamilton who facilitated the CBT groups, as well Ashleigh Elcock for her assistance with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.