
Abstract
Objective:
The purpose of this study was to increase the understanding of the Canadian forensic psychiatry system by providing a population-based overview of the Ontario forensic mental health system.
Methods:
Data were collected on 1,240 accused adults who were subject to the jurisdiction of the Ontario Review Board (ORB) between 2014 and 2015. Archival data were retrieved from annual ORB hearing hospital reports for accused supervised by all nine adult forensic psychiatry facilities across Ontario.
Results:
The sample included not criminally responsible (NCR; 91.6%) and unfit to stand trial (UST; 8.4%) accused. The majority of the sample was male (85.7%), single (70.1%), unemployed (63.6%), with a high school education (48.8%). Most were on a detention order (78.5%) and almost half were living in the community at the time of the report (48.8%). The majority had prior contact with psychiatric services (83.1%) and/or the criminal justice system (70.6%) before entering the forensic system. A history of elopement (31.5%) and inpatient aggression was high (60.6%). Most had a psychotic spectrum disorder (81.6%) and over half had a substance use disorder (57.2%) in the reporting year. A range of index offences was observed (69.9% violent, 20.3% general, 9.8% sexual), and the majority of the sample (61.0%) had an index offence that resulted in no injury or a minor injury to the victim.
Conclusion:
The Canadian forensic psychiatry system is comprised of a unique subset of justice-involved individuals. This study provides a detailed examination of accused who are subject to the jurisdiction of the ORB and provides key insight into risk factors associated with offending behaviour in this population. The results of this study will provide a framework for future studies examining the association between mental disorder and violence and the treatment trajectories for those in the forensic psychiatry system.
Introduction
In Canada, legislative changes and landmark court cases occurring after the deinstitutionalization movement contributed to the growth of the forensic psychiatry population 1 –6 and has led to a more heterogenous profile of individuals (referred to as accused under the Criminal Code) within the system. 7 –9 Accordingly, examining the characteristics of this unique and varied group is critical as they are known to face complex challenges and require specialized and costly services. Currently, there is a lack of population-level data regarding forensic psychiatry patients in Canada. Extant research often suffers the limitations of small sample sizes drawn from one or a few forensic psychiatry institutions. Notably, the National Trajectory Project (NTP) that collected longitudinal data across three provinces between 2000 and 2008 provided important insights into the profile of individuals found not criminally responsible (NCR) in Canada. 10 However, the NTP examined only a cross section of the Ontario population and since that study, no other evaluation has been undertaken to further understand the profile of individuals who are within the forensic mental health system. Building on the work of the NTP, this study aimed to examine the characteristics of individuals under the purview of the Ontario Review Board (ORB). The ORB oversees one of the largest numbers of forensic facilities and forensic patients in Canada. This study serves to provide an in-depth and updated description of the forensic mental health population, long after key landmark court cases, such as Winko. 11
Canadian Legislation
In Canada, an accused is found unfit to stand trial (UST) if they are unable, on account of mental disorder, to understand the nature or object of proceedings, the possible consequences of the proceedings, or communicate with counsel. 12 An NCR verdict is rendered if the Court determines that the individual was suffering from a mental disorder at the time of the offence or omission, that rendered them incapable of appreciating the nature and quality of the act or omission, or knowing that it was wrong. 12 UST and NCR accused fall under the auspices of a provincial Criminal Code Review Board. Review boards are independent quasi-judicial administrative tribunals mandated under the Canadian Criminal Code. 12,13 Review board hearings are held not less than annually for each individual under their jurisdiction to render and review dispositions. 12 The dispositions a review board can order include; (1) detention order: the accused can be detained at a facility; (2) conditional discharge order: the accused is to live in the community while subject to certain conditions; and (3) absolute discharge order: the accused is no longer subject to the oversight of the review board. 12
Objectives
The objective of this article is to provide a detailed and representative description of the Ontario forensic psychiatry patient population, including sociodemographics, historical characteristics (i.e., family history, personal history, psychiatric history), criminogenic characteristics, and behaviour (i.e., escape, aggression, self-harm). The value of descriptive study designs is well-recognized, and this in-depth overview of the forensic mental health system serves to add critical information to the forensic psychiatry literature and discipline, including key insights about the population and factors that impact risk, trajectory, and recovery. 14 –17
Method
Design and Sample
This study used a retrospective chart review design to examine UST and NCR accused in Ontario. The sample included 1,240 accused who were under the jurisdiction of the ORB between 2014 and 2015. This year was randomly selected by the ORB and annual hospital reports were provide by the ORB for the study. The first author (GC) received all available electronic annual ORB hearing hospital reports from the ORB for accused supervised by all nine adult forensic psychiatry facilities. Hospital reports for accused awaiting their initial ORB hearing, waiting to return to court, recently discharged from the ORB, or not entered into the electronic system were not received.
Ethics
Ethical approval was obtained from the Hamilton Integrated Research Ethics Board (HiREB # 7235-C). The waiver of informed consent and data governance were performed in accordance with the Tri-Council Policy Statement–2 (TCPS-2), Personal Health Information Protection Act (PHIPA), and HiREB. Patient identifiers were autotomized and removed, in line with ethical standards.
Measures and Data Sources
ORB hospital reports
The annual ORB hospital report is a document prepared by the accused persons’ clinical team. Each year, the past review period summaries are retained in the document, and the present review period is added, creating a robust documentation of the accused’s progress while under the ORB. The ORB hospital reports utilized for this study were prepared for annual hearings held in the 2014 or 2015 year.
Data collection
Data were extracted from the ORB hospital reports using a coding form. The variables of interest were those known to be associated with offending behaviour in the literature. 18 –20
Personal history
The presence or absence of items mentioned in the report regarding home configuration before the age of 16 were coded.
Diagnoses
Primary, secondary, and tertiary diagnoses that were specified in the reporting year were coded. Primary diagnoses were defined as the accused’s psychiatric condition that was the basis of their UST or NCR finding, was mainly responsible for their admission, was considered the most serious, was the focus of their treatment, and/or explicitly specified in the hospital report. Additional diagnoses were coded as secondary and tertiary diagnoses, corresponding to how they were listed in the hospital report and/or with respect to their seriousness, and relevance to admissions and treatment.
Index offence characteristics
The coding of index offences was based on the Cormier-Lang system, a commonly used framework for categorizing criminal charges. 20 –22 The offence for which the NCR or UST verdict was rendered was coded as the index offence. When NCR or UST verdicts were reached for multiple offences for one individual, the most serious offence was coded as the index offence. Violent offences were chosen over general offences (i.e., non-violent offences), and sexual offences were chosen over general and violent offences. When there were no obvious differences between the severity of the offences, the details of the earliest index offence were recorded. Additional victim characteristics were coded for violent and sexual index offences. The index offences were coded into general, violent, and sexual categories, and subsequently coded and aggregated according to the Uniform Crime Reporting Survey (2) 23 to correspond with the classification used by the NTP. 10
Criminal history
Offences that were committed prior to the index offence were divided into categories of “general,” “violent,” and “sexual” offences and were coded as a previous “charge” and/or “conviction.” Charges and convictions received as a juvenile were included. Data were collected on the number of charges and convictions that took place after the index offence and while the individual was under the jurisdiction of the ORB and were coded separately as re-offences and categorized as “general,” “violent,” and “sexual” offences.
Procedure
All research staff were trained by the senior investigators (GC, MM, HM) and a research assistant (KM) who developed the coding materials and coding manual. New coders were trained by completing training cases alongside the research assistant before coding independently.
Coded variables included information on sociodemographic characteristics, personal history, psychiatric history, criminal history, and index offence characteristics. Categories that were specifically coded using only information in the reporting year (2014–2015) included: forensic status, diagnoses, aggression, self-harm, and dispositions. When information on the aforementioned categories were discussed in the report (e.g., family history) but the presence of a specific variable was not mentioned (e.g., family history of mental illness) the item was coded as non-existent for the accused (e.g., “No” family history of mental illness). Categories that were completely missing from the report (e.g., no mention of family history in the report) were coded as “unknown” (e.g., family history of mental illness “unknown”).
Analytic Strategy
The current project analysed information by calculating frequency statistics and descriptives. The normality of the distribution was assessed by histograms and the Shapiro–Wilk test. Mean (M) and standard deviation (SD) were used when data complied with a normal distribution, otherwise median (MED) and quartiles 25 and 75 are reported. Missing data were identified as unknown for categorical variables and included in the analysis, while missing data for continuous variables were excluded from the analysis. Excellent interrater reliability was achieved for the 10% of cases in the sample that were coded by two coders. The average κ coefficient for categorical variables was 0.83. The average intraclass correlation coefficient for continuous variables was 0.92. All data were analysed using the Statistical Package for the Social Sciences (version 26).
Results
Sociodemographic Characteristics
The sample consisted of 1,063 males (85.7%), 173 females (14.0%), and 4 accused who identified as transgender (0.3%). The median age at the time of the annual report was 41 (32.0–51.8). Information about race/ethnicity was included in half of the reports (51.1%). The majority of the sample was described as being single at the time of the report, with no biological children, unemployed, and had a high school education (see Table 1).
Sociodemographic Characteristics of Study Population.
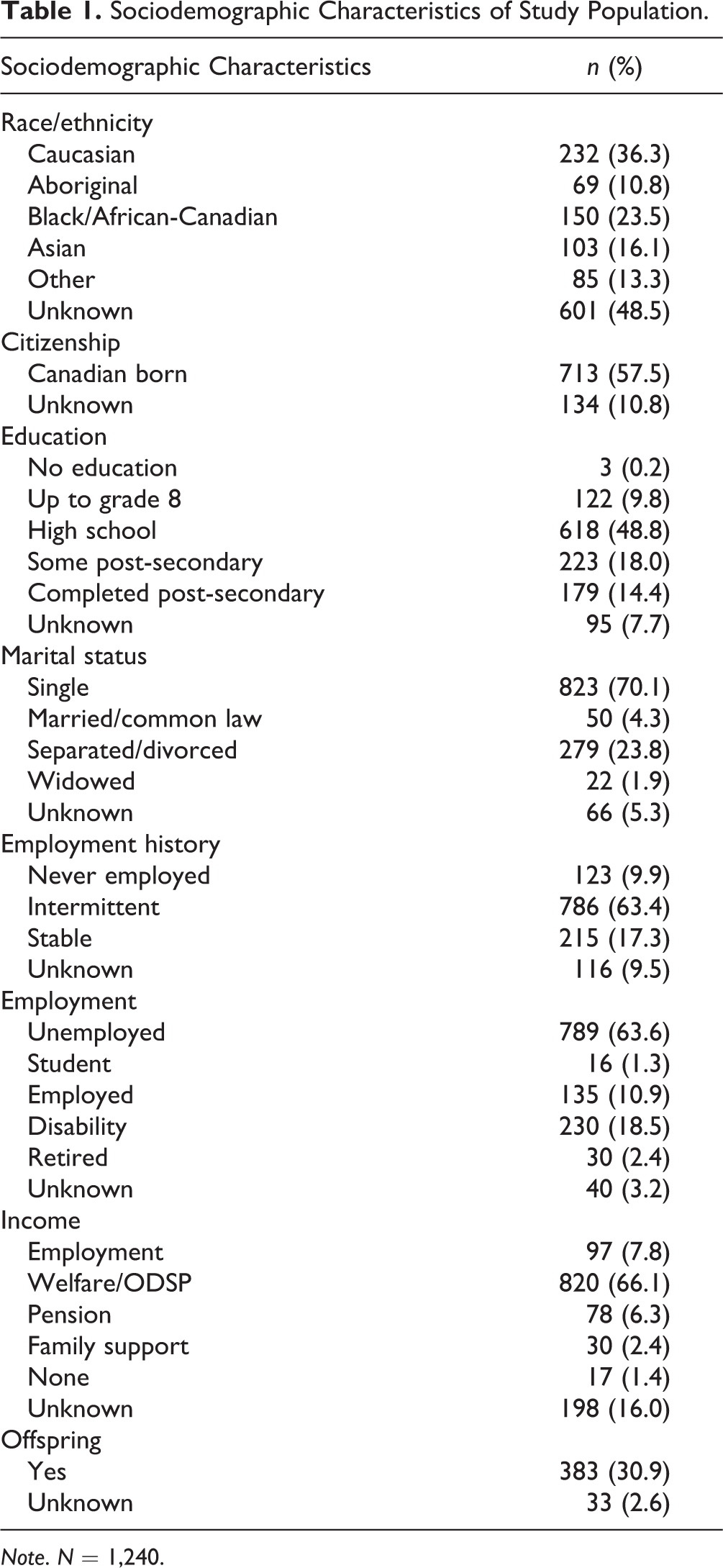
Note. N = 1,240.
Forensic Status
The majority of the sample had received an NCR (91.6%) verdict, including 13.2% that had a previous UST finding. 8.4% of the sample were UST, which included 5.2% that were permanently UST. a There was an almost equal distribution of inpatients (51.2%) and outpatients (48.8%). Detention orders for outpatients (27.3%) were slightly more common than conditional discharge orders (21.5%). Length of stay in the forensic system was calculated as the time between a UST or NCR verdict to the ORB hospital report preparation date for the review period. The median length of stay for the sample was 60 months (27.0–113.8).
The disposition recommendation made by the clinical team in the hospital report to the ORB included 859 detention orders (69.3%). Conditional discharge dispositions were recommended in 248 cases (20.0%), and absolute discharges in 122 cases (9.8%). There were 11 instances in which no recommendation was included or a recommendation was made that did not conform to the aforementioned dispositions.
Personal History
Half of the sample (51.9%) experienced a change in their home configuration before the age of 16, with a median of 2 (1.0 to 3.0) changes. Irrespective of whether individuals experienced a change in their home configuration, majority of the sample (77.4%) lived with both biological parents at some point in childhood (see Table 2). Childhood abuse of any form (i.e., physical, verbal, and/or sexual abuse) was commonly reported (see Table 2).
Incidence of Types of Home Configuration in Childhood and Personal History Characteristics.
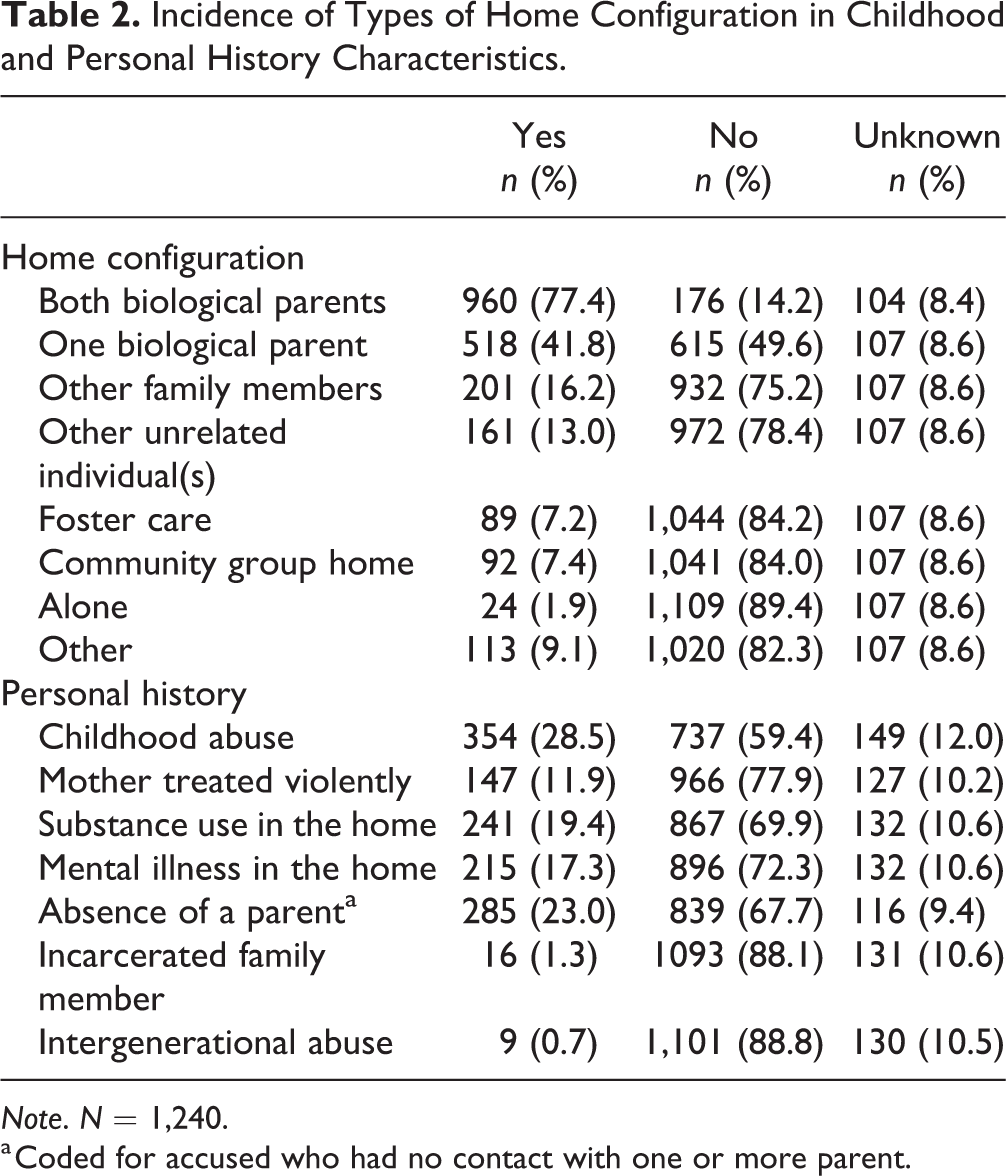
Note. N = 1,240.
a Coded for accused who had no contact with one or more parent.
It was found that 40.4% of the sample had a family history of mental illness, 27.1% had a family history of substance abuse, and 7.3% had a family member with a criminal history. Family history was unknown for the aforementioned items in 18.6%, 16.5%, and 21.4% of cases, respectively.
Psychiatric History
In total, 83.1% of the sample had a psychiatric admission prior to their UST or NCR verdict, with information unknown for 17 cases. The median age at first admission was 23 (19.0 to 31.0), as was the median age at first diagnosis (18.0 to 30.0). Data were unknown for 4.1% and 11.6% of the cases, respectively. A history of psychiatric relapse was found in 80.7% of cases, with a median of 4 (2.0 to 9.0) admissions. b Information was unknown for 1.6% and 4.3% respectively.
A history of non-adherence with treatment was reported in 74.1% of cases; 64.7% of cases had a history of being unresponsive to pharmacological treatment and 42.9% had been previously found incapable to consent to treatment by a provincially appointed Mental Health Act Review Board (Ontario Consent and Capacity Board). Data were unknown in 6.5%, 15.8%, and 9.5% of cases, respectively.
In total, 69.4% had a history of substance abuse, including a high prevalence of both alcohol and drug use (41.9%). Having a history of drug abuse exclusively (16.8%) was more common than a history of alcohol abuse only (9.1%). In 1.6% of cases, a history of substance abuse was mentioned but the type of substance was not specified. Prior substance abuse was unknown for 2.5% of cases.
It was found that 31.5% of cases had a history of escape or attempted escape. History of escape was unknown for 8 cases; 60.0% of the sample had a history of inpatient aggression that occurred prior to the reporting year. Having only a history of outpatient violence was uncommon (2.1%); 49.7% of the sample had a history of inpatient physical aggression against others, followed by verbal aggression (33.5%), physical aggression against objects (30.0%), and sexual aggression (28.2%); 14.7% of the sample had a history of inpatient self-harm. c Previous inpatient aggression and self-harm data were unknown for 37 cases.
Diagnoses
Psychotic spectrum disorders accounted for 81.6% of primary diagnoses, with schizophrenia being the most common diagnosis. The total percentage of substance use disorders in the sample was 57.2%, and the total percentage of personality disorders was 27.8%. Three quarters of the sample had a comorbid psychiatric diagnosis (74.6%). A third of the sample had more than two psychiatric diagnoses (34.2%; see Table 3).
Prevalence of Primary, Secondary, and Tertiary Diagnoses in the Most Recent Reporting Year.
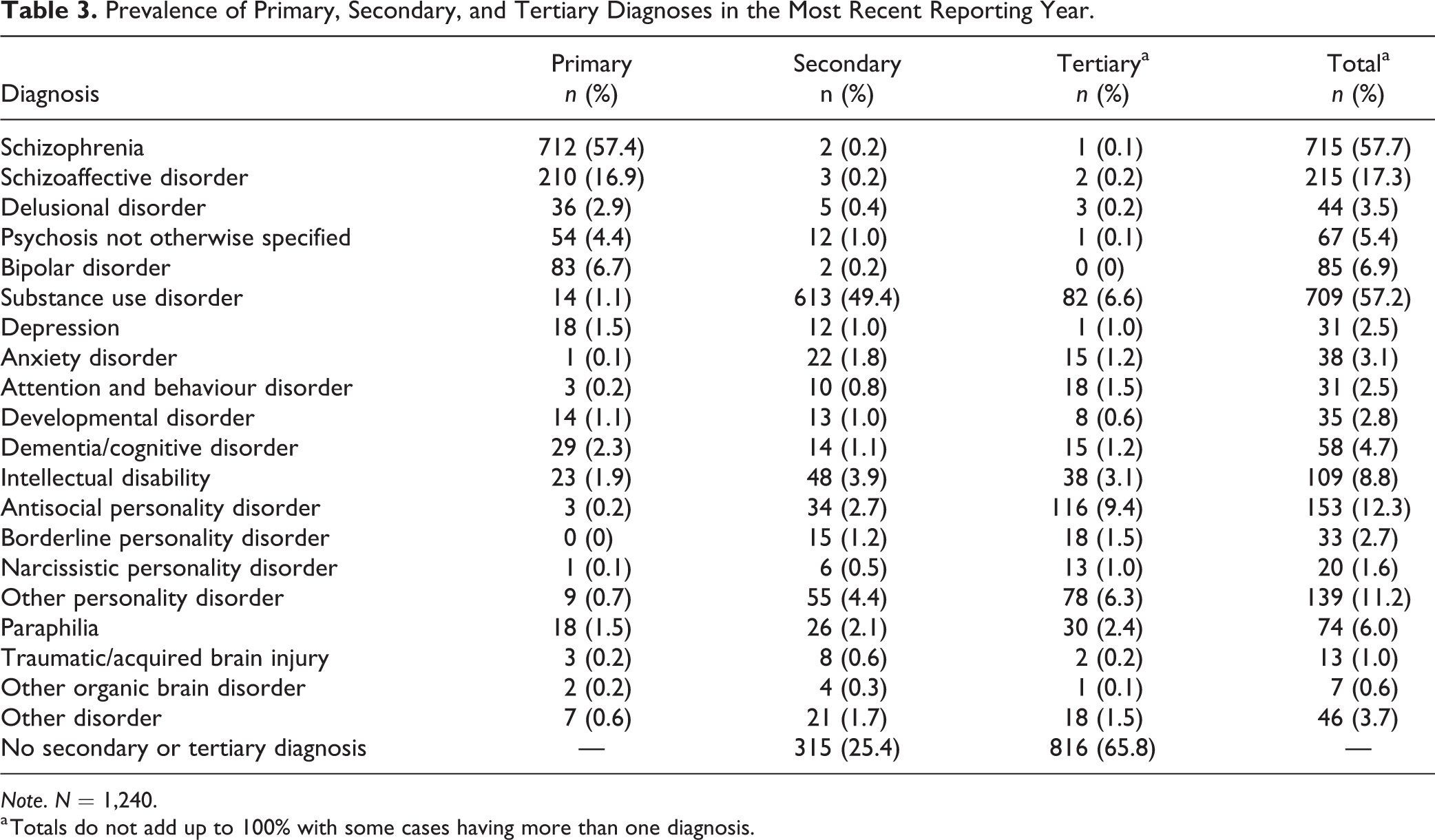
Note. N = 1,240.
a Totals do not add up to 100% with some cases having more than one diagnosis.
Criminogenic Characteristics
Criminal history
Previous NCR findings accounted for 4.0% of the sample. Information about previous general (i.e., non-violent offences), violent, and sexual charges were unknown for 4.0%, 4.0%, and 4.5% of cases, respectively. Previous general, violent, and sexual convictions were unknown for 5.1%, 5.0%, and 4.7% of cases, respectively; 70.6% of the sample had a previous criminal charge and 57.2% had a previous conviction. A history of general charges (61.9%, Med = 5.0, 2.0 to 12.0) and convictions (56.2%, Med = 6.0, 2.0 to 15.5) were more common than violent charges (59.6%, Med = 3.0, 1.0 to 6.0) and convictions (43.3%, Med = 2.0, 1.0 to 5.0). Prior sexual offence charges (10.2%, Med = 1.0, 1.0 to 2.0) and convictions (6.4%, Med = 1.0, 1.0 to 2.0) were less frequent.
It was found that 13.4% of the sample were charged for an offence committed while under the jurisdiction of the ORB; 7.5% of the sample were convicted for re-offenses, while 5.9% of the sample had charges that did not result in convictions, either due to being acquitted, stayed, dismissed, withdrawn or resulting in an UST or NCR verdict.
Index offence characteristics
All reports included the index offence(s). The median age at the time the index offence was 32 (25.0 to 43.0); 33.5% of offences involved a weapon and 11.8% of accused were intoxicated at the time of the index offence, with information unknown in 3.1% and 3.5% of cases, respectively.
The majority of cases (64.7%) had multiple offences for which an NCR or UST verdict was rendered. Violent index offences were most common (69.9%), followed by general offences (20.3%), and sexual offences (9.8%). A total of 62 different Criminal Code offences were found within these categories. Assaults accounted for almost half of the index offences in the sample, followed by threats and other interpersonal offences (see Table 4).
Classification of Index Offences (N = 1,240), and Victims and Injuries Sustained for Violent and Sexual Index Offences (n = 988).
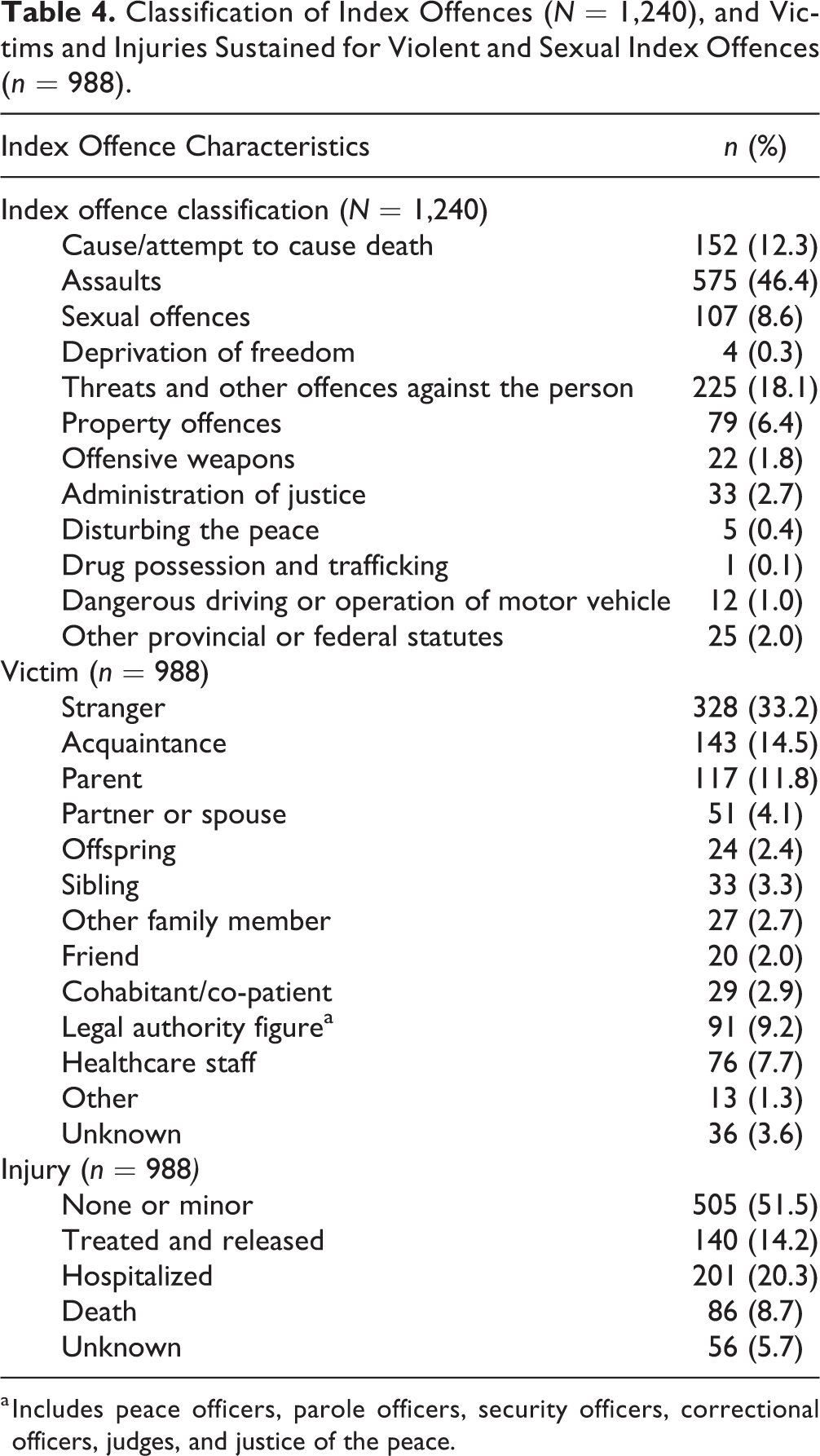
a Includes peace officers, parole officers, security officers, correctional officers, judges, and justice of the peace.
The majority (61.0%) of the index offences in the sample resulted in no injury or minor injuries to the victims. 16.2% of index offences resulted in injuries that required the victim to be hospitalized, 11.3% resulted in the victim being treated and released, and 6.9% resulted in death. See Table 4 for further detail on injuries sustained by victims of violent and sexual offences.
Victim gender was available for 90.7% of violent and sexual offences. Female victims (48.4%) were more common than male (42.3%) victims. The relationship with the victim was included in 96.4% of violent and sexual cases; 44.9% of victims of violent and sexual offences were known to the accused, including family members, acquaintances, friends, cohabitants and co-patients. Strangers accounted for a third of the victim relationships, followed by legal authority figures and healthcare staff.
Inpatient aggression and self-harm
Information about aggressive behaviour and self-harm for the most recent reporting year was present in 97.6% of cases; 65.9% were reported to not engage in any aggressive behaviour or self-harm. Verbal aggression (27.3%) was most the most common form of inpatient aggression, followed by physical aggression against others (14.1%), aggression against objects (11.0%), and sexual aggression (10.1%); 2.3% engaged in self-harming behaviours.
Discussion
This paper included 1,240 UST and NCR accused from all adult forensic psychiatry facilities in Ontario to provide detailed and comprehensive descriptives of this unique psychiatric and justice-involved population. The descriptive nature of this study provides a framework for future research and base rates for comparisons to be made on important features of this population by researchers, clinicians, and policy makers. Given the federal Criminal Code operates across Canada, this study of one province may give some indication of the Canadian forensic psychiatry system.
Psychotic spectrum disorders remain the most common diagnoses and substance use disorders are increasingly overrepresented. 6 –8,24,25 Substance use represents a critical risk factor, and it is imperative that interventions targeting substance use are increasingly incorporated into practice. 7,24,26 Many accused in the current sample had previous contact with psychiatric services and the criminal justice system. Psychiatric services should continue to integrate risk assessments into regular practice. 1 Indeed, additional training or support could be provided to non-forensic services so that amenable risk factors and protective factors are targeted to help individuals desist from offending. 27 Additionally, inpatient aggression remains a critical concern on psychiatric units. 28,29 Risk assessments focusing on the immediate and short-term prediction of violence may further assist in the identification and prevention of inpatient aggression. 30
In comparison to the NTP, higher rates of index offences of assault, sexual offences and offences that caused or attempted to cause death were found in the current sample 8 . Deprivation of freedom offences, property offences, weapons, and administration of justice offences were lower compared to the NTP. 8 In line with the evidence provided by the NTP, Ontario’s forensic psychiatry population appears to have a higher prevalence of serious offences compared to other provinces 8 and lower incidents of the NCR defence being used for relatively minor offences. This is likely a result of the robust court diversion program in Ontario which aims to divert most minor offences early in the process.
While it was determined that NCR and UST accused were more likely to enter into the forensic psychiatric system due to the commission of a violent offense, it was found that offences resulting in death were uncommon, as the majority of offences resulted in no or minor injuries. It was also found that those known to the accused were more commonly the victims of the index offences than strangers. 8,27 Family members were found to be especially vulnerable to being victimized. The overrepresentation of family members as victims is an ongoing concern that warrants further investigation. 31,32
Strengths
This study was by far the largest in population and scope to provide a comprehensive and detailed analysis of Ontario forensic psychiatry patients. Previous studies have been limited in sample size or have only consisted of accused from one facility. Moreover, UST accused were included in the current sample, a group which the extant literature on Canadian forensic psychiatry populations has often failed to account for. In addition, the use of all available ORB hospital reports for the 2014 to 2015 year provides a more recent account of the profile of this population since the time of data collection encompassed by the NTP, for instance, and since landmark court cases such as Winko. 10,11
Limitations
Given international legislative differences, the generalizability of some of the findings may be limited to Canada. This study is also limited by reliance on archival records, and the use of only one data source, albeit a composite one. The study also faced the limitation of missing data as the population-based and retrospective design did not allow direct access to individuals.
Future Directions
Given the increasing heterogeneity and diversification of the forensic psychiatry population, it is critical that research continues to examine existing and emergent criminogenic and clinical profiles of this population. This empirical evidence would support professionals involved in forensic psychiatry and legal tribunals remaining as informed as possible when making important decisions for this unique group that often requires costly services. If rehabilitation and recovery is to occur, an understanding of the clinical profile of forensic psychiatry patients is critical.
Future research should aim to provide population-level empirical data regarding the characteristics of forensic psychiatry patients and incorporate this evidence into best practices. Moreover, given the findings of this study, such research should include treatment efficacy, recovery trajectories, and inpatient behaviours. Population-level research should also encompass the correlates and precursors related to certain offending behaviour, and those specific to certain populations of accused and victims. The findings from this data will elucidate the factors that contribute to length of stay and successful trajectories within the forensic psychiatry system allowing for enhanced forensic psychiatry care. Accordingly, as this study is part of a larger research project, we will continue to examine a multitude of research questions to expand on key areas within forensic psychiatry.
Footnotes
Authors’ Note
The data for the current study are available in the public domain through the Ontario Review Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by unrestricted funding provided by Janssen Pharmaceuticals, Inc. (Chaimowitz, G. Retrospective Data Abstraction Project, Janssen ORB Study 2015).