
Abstract
Introduction:
Previous research has shown that the socioeconomic status (SES)–health gradient also extends to high-cost patients; however, little work has examined high-cost patients with mental illness and/or addiction. The objective of this study was to examine associations between individual-, household- and area-level SES factors and future high-cost use among these patients.
Methods:
We linked survey data from adult participants (ages 18 and older) of 3 cycles of the Canadian Community Health Survey to administrative health care data from Ontario, Canada. Respondents with mental illness and/or addiction were identified based on prior mental health and addiction health care use and followed for 5 years for which we ascertained health care costs covered under the public health care system. We quantified associations between SES factors and becoming a high-cost patient (i.e., transitioning into the top 5%) using logistic regression models. For ordinal SES factors, such as income, education and marginalization variables, we measured absolute and relative inequalities using the slope and relative index of inequality.
Results:
Among our sample, lower personal income (odds ratio [OR] = 2.11, 95% confidence interval [CI], 1.54 to 2.88, for CAD$0 to CAD$14,999), lower household income (OR = 2.11, 95% CI, 1.49 to 2.99, for lowest income quintile), food insecurity (OR = 1.87, 95% CI, 1.38 to 2.55) and non-homeownership (OR = 1.34, 95% CI, 1.08 to 1.66), at the individual and household levels, respectively, and higher residential instability (OR = 1.72, 95% CI, 1.23 to 2.42, for most marginalized), at the area level, were associated with higher odds of becoming a high-cost patient within a 5-year period. Moreover, the inequality analysis suggested pro-high-SES gradients in high-cost transitions.
Conclusions:
Policies aimed at high-cost patients with mental illness and/or addiction, or those concerned with preventing individuals with these conditions from becoming high-cost patients in the health care system, should also consider non-clinical factors such as income as well as related dimensions including food security and homeownership.
Introduction
Research has shown that a small proportion of patients account for a disproportionately large share of health care costs across all care settings. For example, in 2010, 1% of patients in the United States accounted for 21% of total health care spending. 1 Similarly in Canada, in 2012, 1% of patients in Ontario accounted for 29% of public health care costs. 2 Despite universal health coverage in Canada, research has shown that socioeconomic status (SES) can influence health care utilization. For example, low-income individuals have been found to be more frequent users of primary care. 3 Thus, it is likely that this SES–health relationship (i.e., gradient) also extends to high-cost patients. 4 Most research on high-cost patients has solely employed administrative health care data, 2,5,6 which lack information on certain socio-demographic characteristics, such as marital status and ethnicity, health behaviours, such as smoking and drinking, and SES (income, educational attainment and occupation).
Recent work has made use of administrative health care data linked to the Canadian Community Health Survey (CCHS), a national population-based survey. One study, which examined high-cost patients in Ontario, Canada, found that high-cost status was strongly associated with being older, having multiple chronic conditions and reporting poorer self-reported health status. 7 The authors found that, even after adjusting for relevant covariates, poor (vs. good) self-reported health was associated with a 26-fold increase in the odds of becoming a high-cost patient (in the 99th percentile of the cost distribution vs. the bottom 50th percentile). Moreover, the study found that high-cost patients tended to be of lower SES. These findings were further confirmed by the authors in the development and validation of their High Resource User Population Risk Tool, which showed that household income was the strongest socioeconomic driver associated with high resource use. 8
Other work has examined the socioeconomic determinants of becoming a high-cost patient in the future 4 and found that future high-cost status 5 years following the CCHS interview was most strongly associated with lower personal income, food insecurity, and non-homeownership. Moreover, living in a highly deprived or low ethnic concentrated neighbourhood was also an important predictor. However, this work did not examine the SES–high-cost user relationship among specific high-cost patient subgroups, such as those with mental illness and/or addiction. Previous research suggests that high-cost patients with mental illness and/or addiction have a different patient profile than other high-cost patients, as they are younger and more likely to live in low-income neighbourhoods and incur higher costs than high-cost patients without mental illness and/or addiction. 2,9 According to the Gelberg–Andersen Behavioral Model for Vulnerable Populations, 10 which has been used to conceptualize health care utilization among high-cost patients with mental illness, 11,12 predisposing factors, such as sex, age, and ethnicity, and enabling factors, such as income and area of residence, play an important role in explaining how these individuals interact with the health care system. Given the relationship between SES and health care use, and consequently high-cost status, it is important to understand which patient characteristics could help inform targeted policies and/or interventions aimed at individuals at risk of becoming high-cost patients. Thus, the aim of this study was to understand the associations between individual-, household- and area-level SES characteristics and the likelihood of becoming a high-cost patient among individuals with mental illness and/or addiction.
Methods
Setting and Data Sources
Ontario is Canada’s most populous province (13.4 million in 2012 13 ). The costs of most health care services received by legal residents are covered by a universal, single-payer health care system, which is funded through general taxation. Eligibility for health care coverage in Ontario can be ascertained through the Registered Persons Database, a population-based registry, while encounters with the health care system are recorded in administrative health care databases, which include the following: Discharge Abstract Database (DAD), Ontario Mental Health Reporting System (OMHRS), National Ambulatory Care Reporting System (NACRS), Ontario Health Insurance Plan (OHIP) claims database, Ontario Drug Benefit claims database, National Rehabilitation Reporting System, Continuing Care Reporting System, and Home Care Database. A full description of each database can be found in the Online Appendix (Table S1). For respondents who consent, these administrative data can be linked to the CCHS. The CCHS is a cross-sectional survey conducted by Statistics Canada, which collects information on health determinants, health care utilization, and health outcomes of the Canadian population aged 12 years and over. Persons living on First Nations reserves, institutionalized persons, and full-time members of the Canadian Forces are excluded from the sampling frame. 14 The survey and administrative databases were linked using unique encoded identifiers and analysed at Institute for Clinical Evaluative Sciences (ICES) in Toronto, Ontario. The use of these data for research was authorized under Section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a research ethics board. This study is reported as per REporting of studies Conducted using Observational Routinely(RECORD)-collected health data guidelines. 15
Study Population
The cohort study included all respondents aged 18 years and older from the 2007/2008, 2009/2010 and 2011/2012 CCHS surveys who consented to have their survey data linked to administrative data for research purposes (N = 91,741). Individuals were excluded if they did not have a valid health card at, or in the 2 years prior to, survey response (N = 1,508 excluded) or if they appeared in a previous cycle of the CCHS (N = 387 excluded). We restricted our cohort to respondents who had 1 (or more) mental health and/or addiction-related health care encounter in the 2 years prior to survey response (N = 75,254 excluded; see Figure 1). Encounters for mental health and/or addiction were defined as any psychiatric hospitalization (in the DAD and OMHRS), emergency department visit (in the NACRS) or 2 or more outpatient physician visits separated by no more than 2 years (in the OHIP claims data) with a relevant mental health and/or addiction diagnostic code (see Online Appendix Table S2). 16
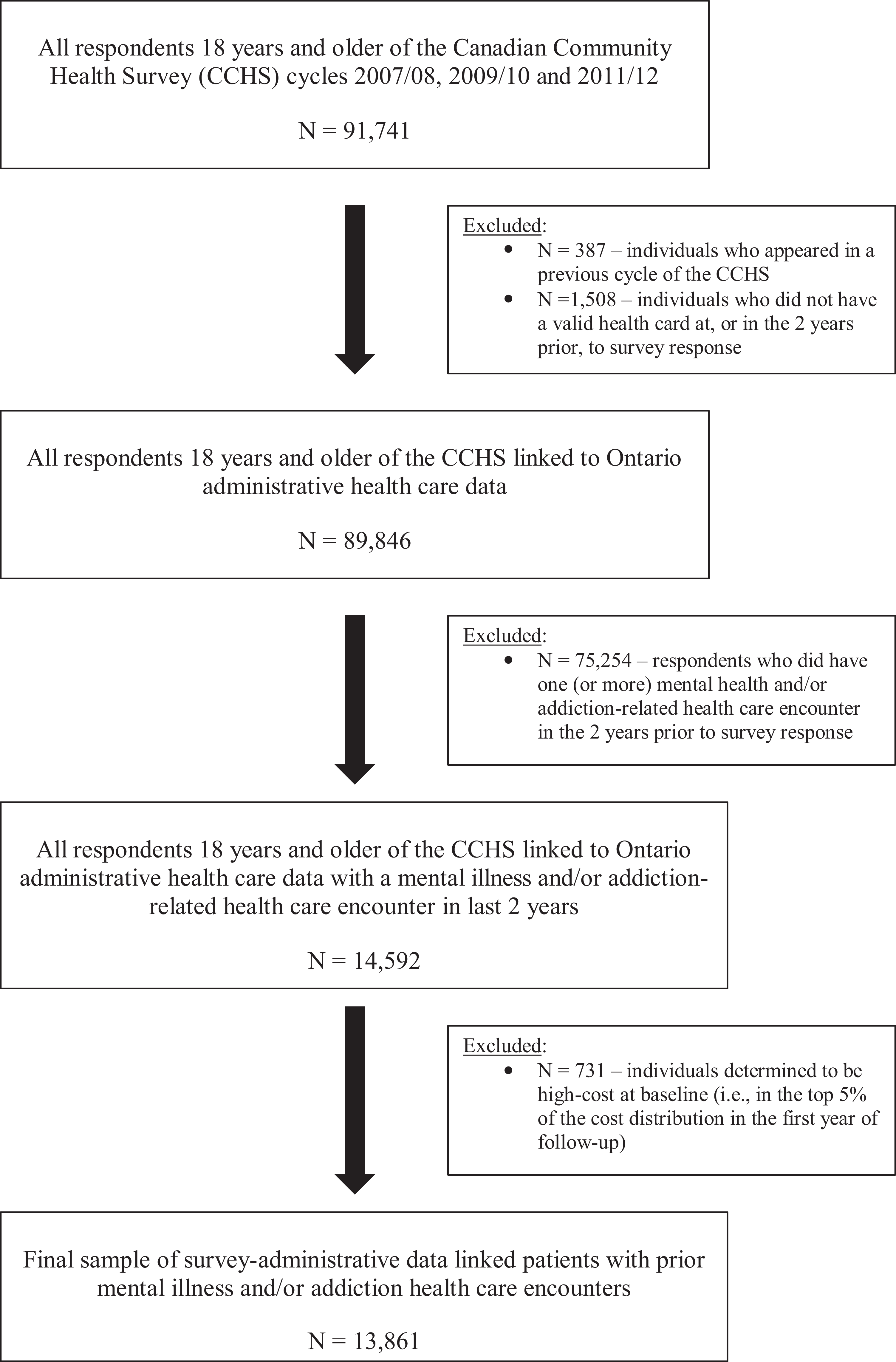
Patient cohort selection process.
Variables
For all respondents, we obtained age and sex from the CCHS. Prior hospitalizations, emergency department visits and physician billings (DAD, NACRS and OHIP datasets, respectively) and the Johns Hopkins ACG® System Version 10 software were used to derive Aggregated Diagnosis Groups (ADG) scores, a weighted summary score of patient comorbidity, which is predictive of 1-year mortality. 17
Individual-, household- and area-level demographic and SES factors were examined, informed by the Gelberg–Andersen behavior model for vulnerable populations 10 and previous related research. 4 From the CCHS, we identified ethnicity, country of birth, marital status, personal income, personal educational attainment, equivalized household income quintile, highest level of household education, household food insecurity, homeownership, and urban/rural residence. From the Registered Persons Database and 2006 Census data, we identified area-level income quintiles. Other area-level determinants included the dependency quintile (which considers adults who are unemployed, unable to work and in unpaid professions), the material deprivation quintile (which considers income, education, single-parent families and housing quality), the residential instability quintile (which considers neighbourhood quality and cohesiveness) and the ethnic concentration quintile (which considers the proportions of recent immigrants and visible minorities), each derived from the 2011 Ontario Marginalization Index. 18 Categorization of all SES factors was consistent with prior evaluations of determinants of high-cost patient transitions from the general population. 4
All individuals were tracked in the administrative data for up to 5 years following survey response, for which we ascertained all health care costs paid for by the Ontario Ministries of Health and Long-Term Care using a person-centred costing methodology described elsewhere. 19 We included all costs attributable to hospital encounters (including inpatient acute, designated inpatient psychiatric and same-day surgery facilities, emergency department visits, dialysis and cancer clinics, inpatient rehabilitation, complex and continuing care facilities), costs of physician visits and related care, costs of outpatient drugs dispensed for eligible persons (i.e., those aged 65 years and older or on social assistance) and costs of home care. Costs were divided for each year of follow-up. Costs that overlapped years (e.g., hospital stays) were divided on a pro rata basis. For each year of follow-up, we ranked individuals according to their costs incurred relative to the study population. The outcome of interest was ever becoming a high-cost patient (ever-high-cost patient), defined as respondents who were in the top 5% of the cost distribution in any year of follow-up, as done elsewhere. 4,8 In secondary analyses, ever-high-cost patients were based on the top 10% of the cost distribution. Individuals determined to be high cost at baseline (i.e., in the top 5% or 10% of costs in the 5 year of follow-up) were excluded from analyses (N = 731 and 1,461, respectively; see Figure 1), given our interest in investigating upstream determinants of becoming a high-cost patient.
Statistical Analysis
We quantified associations between individual-, household- and area-level SES factors and ever-high-cost patient using logistic regressions. We derived unadjusted, age-adjusted, ADG-adjusted, and age–sex–ADG-adjusted (i.e., fully adjusted) associations for each SES factor, separately, for a total of 4 models. Associations were reported as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). Given that within-area variation did not differ much from the between-area variation (61% of the neighbourhoods only had 1 individual, and only about 1% of neighbourhoods had 5 or more individuals), we were not able to undertake multilevel analyses.
For ordinal variables (income, education and marginalization variables), we also calculated the slope index of inequality (SII) and relative index of inequality (RII). 20 These regression-based measures consider the full distribution of SES and summarize the level of absolute or relative inequality, respectively, into 1 number. Here, we regressed the ever-high-cost patient on each respondent’s rank in the cumulative distribution of each SES factor (ranging from 0, for the highest SES position, to 1, for the lowest SES position) using logistic regression. Models were adjusted for age, sex and ADG score. From these models, we derived the SII by contrasting marginal predictions of the cumulative rank variable at values of 0 and 1. The RII was derived by dividing the slope index of inequality by the population mean.
Respondent’s missing information on a given SES factor was excluded from the analysis. To assess possible bias, we compared characteristics of respondent’s missing (vs. not missing) information on each SES factor. Generally, less than 10% of the initial sample was missing data on SES, with the exception of personal income (12.6%). Balanced repeated replication of the survey weights provided by Statistics Canada was used in all analyses to obtain estimates representative of the Ontario population and to account for complex survey design. Weights were adjusted for the pooling of CCHS surveys using the approach described by Thomas and Wannell. 21 SAS Enterprise Guide Version 6.1 (SAS Institute Inc., Cary, NC) was used to create the dataset and Stata/MP Version 15 (StataCorp, College Station, TX) was used for all analyses.
Results
Table 1 provides the characteristics of the patient cohort (N = 13,861), overall and by ever-high-cost patient (top 5%) outcome. A total of 1,424 (7.6% of the weighted sample) became a high-cost patient within 5 years of the CCHS interview. There were no sex differences according to the outcome; however, individuals with mental illness and/or addiction who became high-cost patients were, on average, older than those who did not and more likely to be of White ethnicity. They were also more likely to have a lower personal income and not have completed post-secondary education. These findings held when we examined household-level SES; moreover, individuals who became a high-cost patient within 5 years were more likely to live in a household that was food insecure. Finally, when examining area-level socio-demographic and socioeconomic factors, we found that individuals with mental illness and/or addiction who become high-cost patients were more likely to live in low-income and highly marginalized neighbourhoods in terms of dependency, material deprivation and residential instability.
Distribution of Characteristics according to 5-year High-cost Patient (HCP) Trajectories (Top 5% in Costs) among Adult Ontarians with Prior Mental Health and/or Addiction Health Care Encounters.
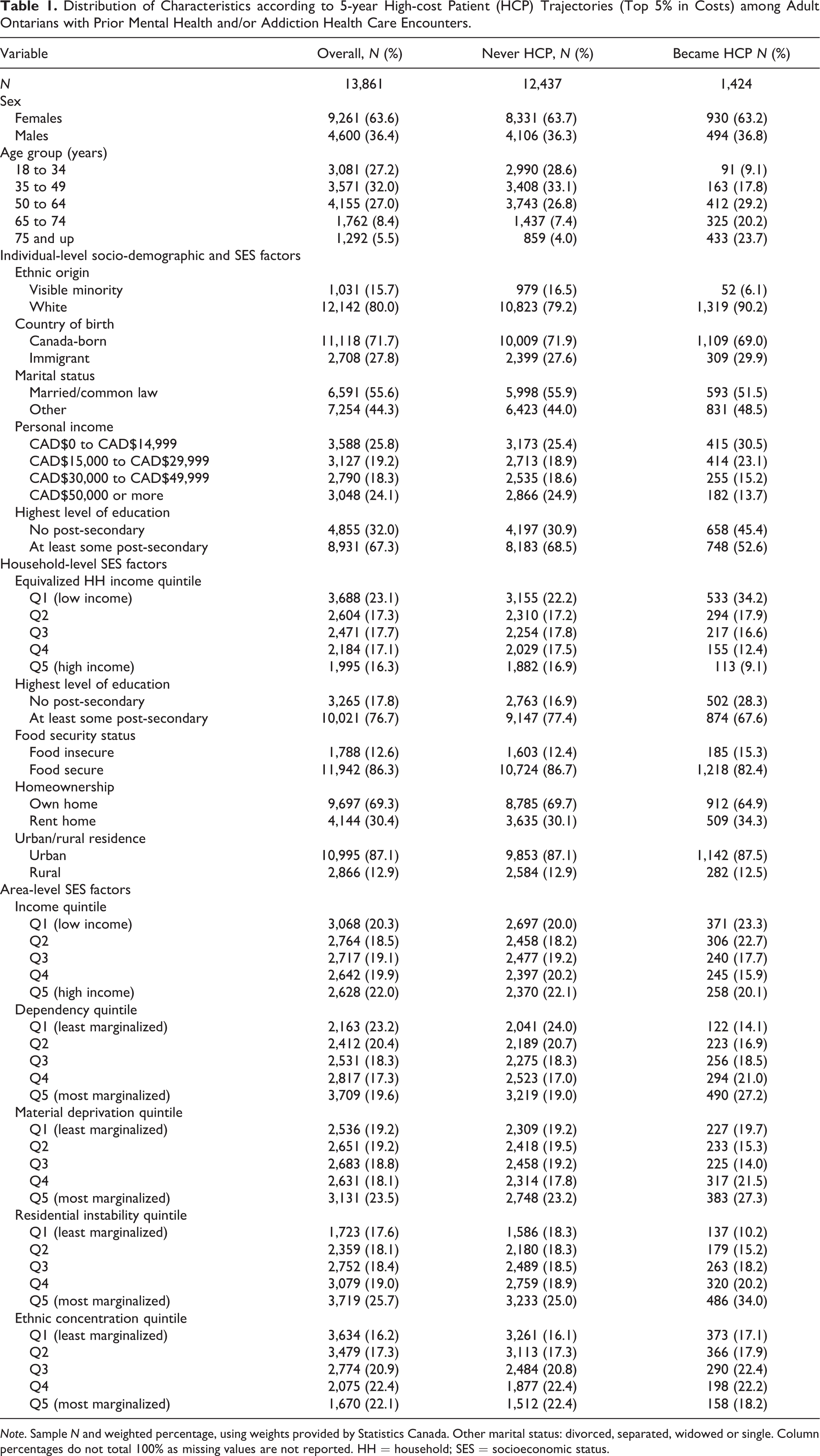
Note. Sample N and weighted percentage, using weights provided by Statistics Canada. Other marital status: divorced, separated, widowed or single. Column percentages do not total 100% as missing values are not reported. HH = household; SES = socioeconomic status.
Table 2 includes the results from the logistic regression examining the association between various socio-demographic and socioeconomic characteristics and the odds of becoming a high-cost patient (in the top 5%) within 5 years. The strongest predictor at the individual level across all 4 models was individual income. In particular, we found a stepwise income gradient, where the less personal income an individual had, the higher were the odds of that individual becoming a high-cost patient within a 5-year period. For example, in the fully adjusted model, compared to the reference category (CAD$50,000 and more), individuals with a personal income between CAD$0 and CAD$14,999 had an OR of 2.11 (95% CI, 1.54 to 2.88). Individuals with no post-secondary education (compared to those with post-secondary education) were also more likely to become a high-cost patient within a 5-year period (OR = 1.34, 95% CI, 1.09 to 1.67). At the household level, income was again the strongest predictor among all household-level variables across all models, where individuals in the lowest household income quintile had an OR of 2.11 (95% CI, 1.49 to 2.99) compared to those in the highest household income quintile for the fully adjusted model. Moreover, individuals living in households that were food insecure (OR = 1.87, 95% CI, 1.38 to 2.55) and that rented (OR = 1.34, 95% CI, 1.08 to 1.66) had higher odds of becoming a high-cost patient compared to those who were food secure and owned a home, respectively. Finally, at the area level, residential instability was the largest predictor. For example, individuals who lived in neighbourhoods with the most residential instability had an OR of 1.72 (95% CI, 1.23 to 2.42) compared to those living in neighbourhoods with the least residential instability when adjusting for relevant covariates. For the other dimensions of deprivation, the gradient was either less clear (e.g., area-level income) or non-existent (e.g. area-level ethnic concentration). Findings were qualitatively the same when we replicated the analysis among individuals in the top 10% of the cost distribution (see Table 3).
Associations (as Odds Ratios) of Becoming High Cost—Defined as Being in the Top 5% of Health Care Spending—according to Various SES Measures.
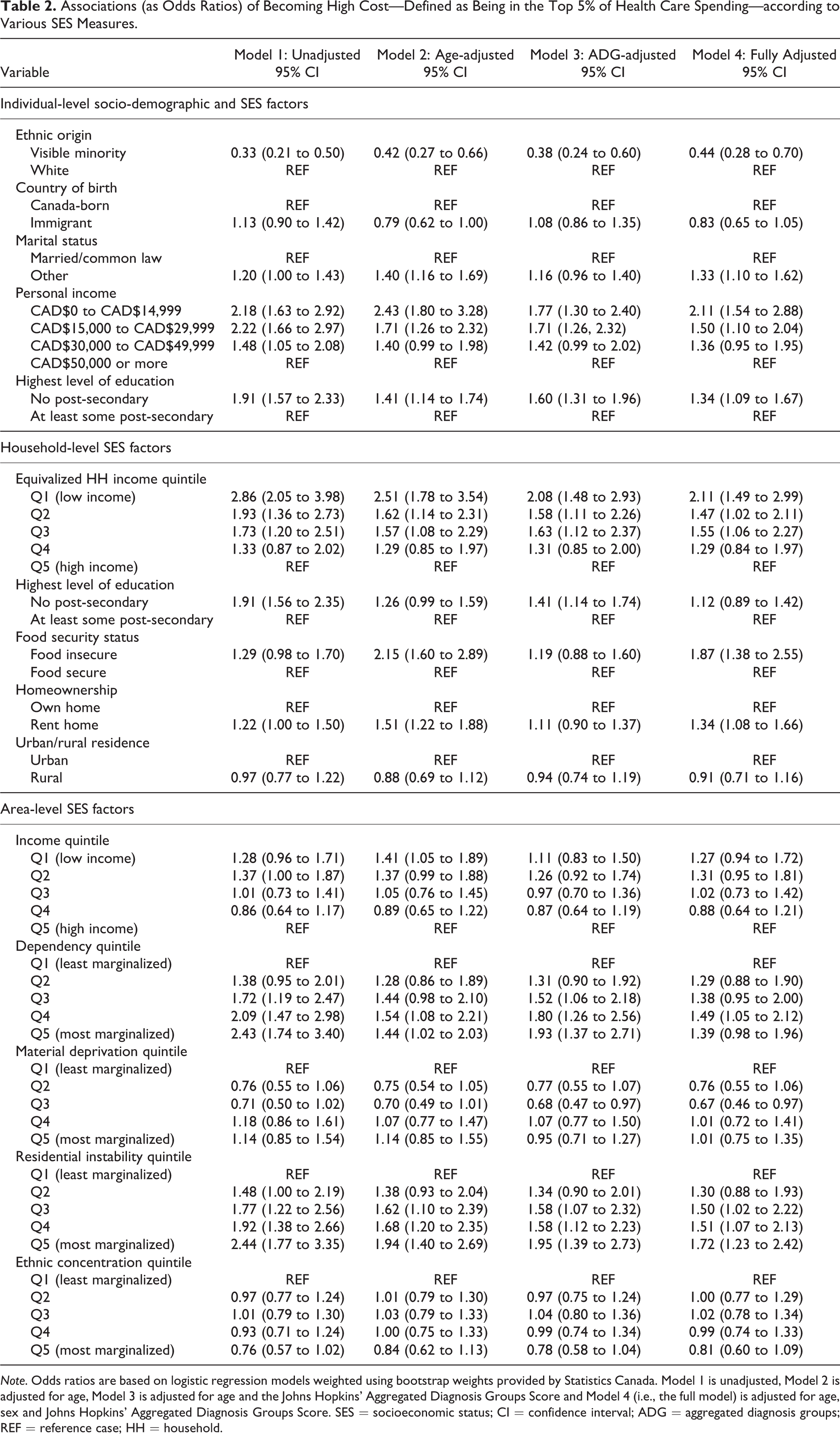
Note. Odds ratios are based on logistic regression models weighted using bootstrap weights provided by Statistics Canada. Model 1 is unadjusted, Model 2 is adjusted for age, Model 3 is adjusted for age and the Johns Hopkins’ Aggregated Diagnosis Groups Score and Model 4 (i.e., the full model) is adjusted for age, sex and Johns Hopkins’ Aggregated Diagnosis Groups Score. SES = socioeconomic status; CI = confidence interval; ADG = aggregated diagnosis groups; REF = reference case; HH = household.
Associations (as Odds Ratios) of Becoming High Cost—Defined as Being in the Top 10% of Health Care Spending—according to Various SES Measures.
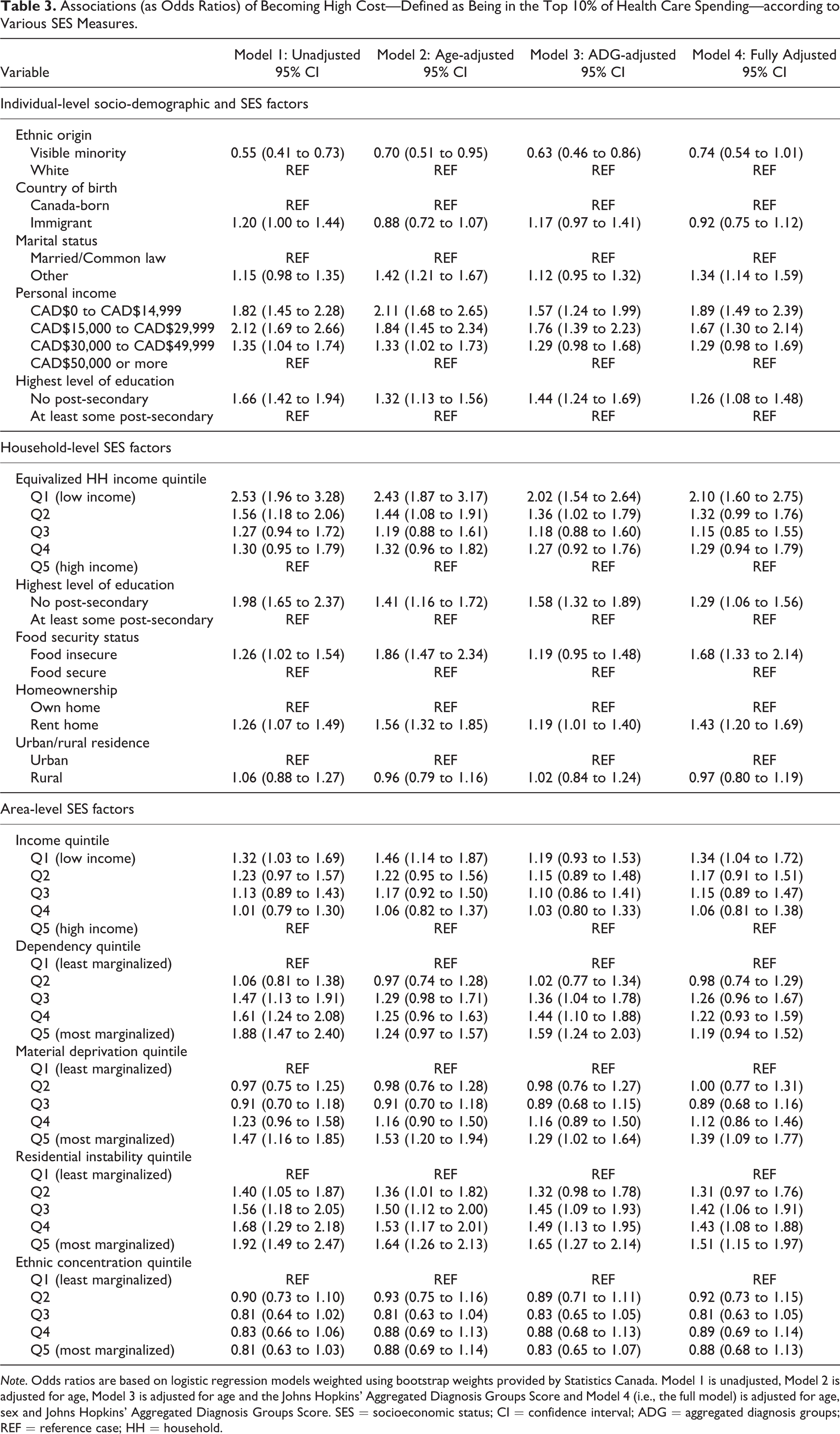
Note. Odds ratios are based on logistic regression models weighted using bootstrap weights provided by Statistics Canada. Model 1 is unadjusted, Model 2 is adjusted for age, Model 3 is adjusted for age and the Johns Hopkins’ Aggregated Diagnosis Groups Score and Model 4 (i.e., the full model) is adjusted for age, sex and Johns Hopkins’ Aggregated Diagnosis Groups Score. SES = socioeconomic status; CI = confidence interval; ADG = aggregated diagnosis groups; REF = reference case; HH = household.
Table 4 provides the results on the absolute and relative summary measures of inequality according to multiple (ordinal) socioeconomic factors. Overall, the results suggest pro-high-SES gradients in high-cost transitions for most SES factors. For example, the SII for personal income (for the top 5%) was −5.75 (95% CI, −8.19 to −3.32), which means that moving from the lowest to the highest personal income level is associated with roughly a 6% reduction in the proportion of patients with mental illness and/or addiction who became a high-cost patient. The corresponding RII of −0.80 (95% CI, −1.14 to −0.46) indicates that this inequality gap is 80% of the mean outcome (here, 7.2% among those with complete information). For household income and area-based material deprivation, inequality gaps were only statistically significant considering top 10% high-cost transitions (95% CIs contained the null value). For area-based ethnic concentration, no inequality gap was evident for either outcome.
Absolute and Relative Inequality in 5-year High-cost Patient (HCP) Trajectories according to Multiple (Ordinal) SES Factors.
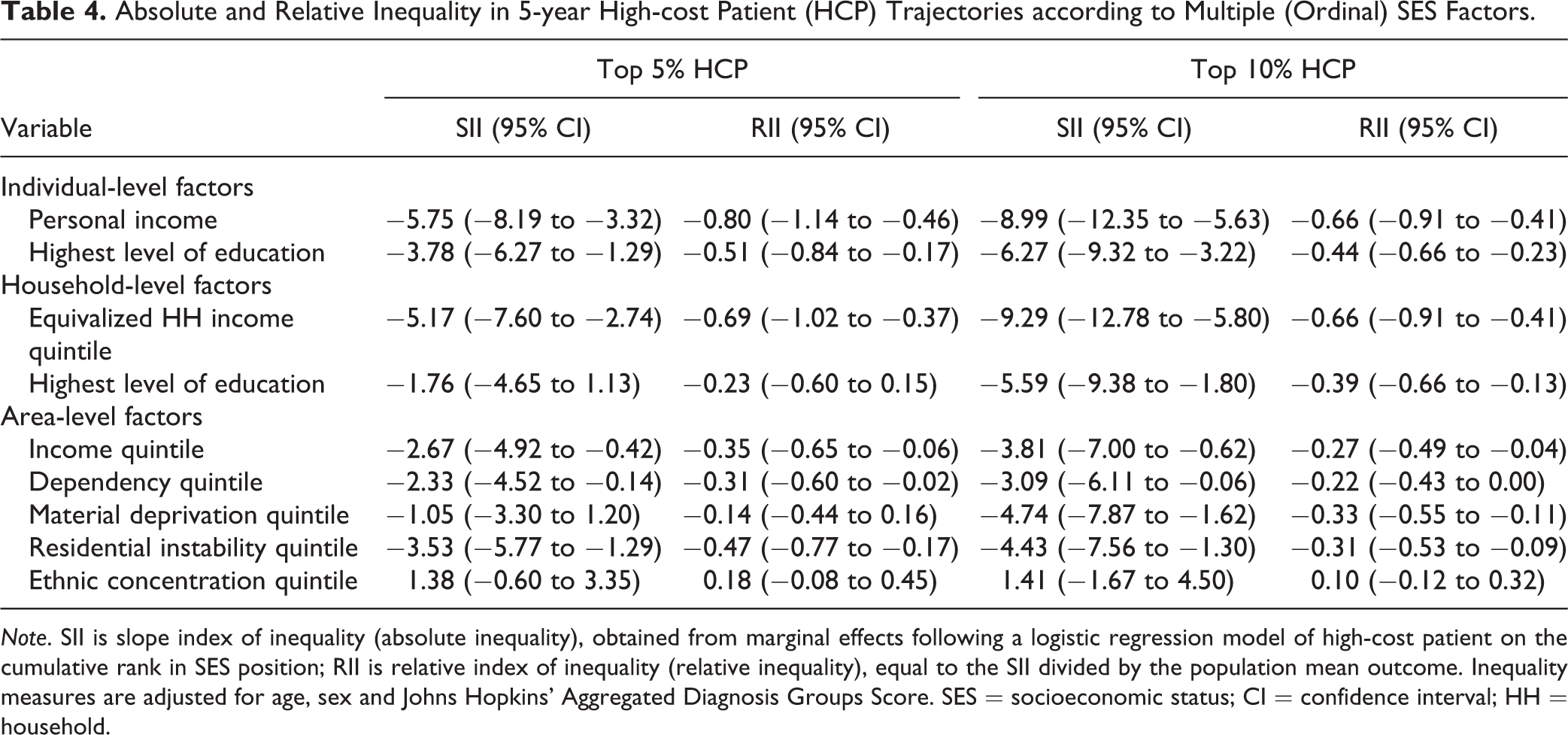
Note. SII is slope index of inequality (absolute inequality), obtained from marginal effects following a logistic regression model of high-cost patient on the cumulative rank in SES position; RII is relative index of inequality (relative inequality), equal to the SII divided by the population mean outcome. Inequality measures are adjusted for age, sex and Johns Hopkins’ Aggregated Diagnosis Groups Score. SES = socioeconomic status; CI = confidence interval; HH = household.
Discussion
Previous research has shown that many factors that affect the SES–health gradient lie outside of the health care system. 4 Understanding high-cost use from a broader perspective, including a comprehensive understanding of the role of SES, is important to inform policies and interventions aimed at mitigating high-cost use of health care services and improving population health. Even after controlling for relevant socio-demographic and clinical characteristics, such as sex, age and comorbidity, informed by our conceptual model, our findings suggest that high-cost patients with mental illness and/or addiction of lower SES (namely, lower individual and household income) were more likely to become high-cost patients within a 5-year period. Moreover, individuals living in households that were food insecure or that rented had higher odds of becoming a high-cost patient. At the neighbourhood/area level, residential instability was an important predictor of future high-cost status. Overall, these results support the idea that SES can operate at different levels (including individual, household, and area levels). 4 These findings were further confirmed by analyses using summary measures of health inequality.
Our findings are in line with previous related work. One study, which linked administrative health care data to survey data, also found that high-cost patients tended to be of lower SES and that household income was the strongest socioeconomic driver of becoming a high-cost patient. 7 Moreover, this last finding is in line with recent research assessing the concordance between individual- and area-level income data, which found that socioeconomic disparities in premature mortality were greater for individual-level income than area-level income. 22 Other work, which examined the socioeconomic determinants of future high-cost status, found that becoming a high-cost patient in the 5 years following the CCHS interview was most strongly associated with lower personal income, food insecurity, and non-homeownership. 4 Prior research has noted that individuals who are food insecure have higher costs of care 23 and higher rates of mental health care service utilization. 24 We too found that lower personal income, lower household income, food insecurity and non-homeownership were important predictors of becoming a high-cost patient 5 years after the survey interview, though the effects (as measured by ORs) were comparatively larger in our study. We also found that individuals who became high-cost patients were more likely to be of White ethnicity, in line with previous research. 4,7 This suggests that ethnic-specific strategies may be required. However, contrary to previous work, which found that living in a highly deprived or low ethnically concentrated neighbourhood were important predictors of becoming a future high-cost patient, we found that residential instability was a relevant area-level factor in predicting future high-cost status among individuals with mental illness and/or addiction (and with larger effects than those found in previous research 4 ). We extended this work by making use of summary measures of inequality and found that inequality favoured the most well off at multiple levels (individual, household, area), with some exceptions (ethnic concentration area).
This work has important policy implications. It provides evidence on the importance of the social determinants of health, such as income and related dimensions, on health care use and costs and, ultimately, high-cost status. Household income was an important predictor of future high-cost status among individuals with mental illness and/or addiction; furthermore, we found a larger OR associated with this variable than previous work. 4 This may suggest that these high-cost patients may require more tailored strategies than the general high-cost population. 9 Food insecurity was also an important predictor of future high-cost status. Thus, health care providers may play a role in screening patients with mental illness and/or addiction for poverty and providing them with assistance. 24 Our work also suggests that area-level factors, namely around residential instability, need to be considered when thinking about models of care for individuals at risk of becoming high-cost patients, which may point to a potential role for municipalities and other bodies outside the health care sector.
This study made use of multiple cycles of a large, nationally representative survey linked to administrative health care data, which enabled us to not only create a population-based sample of high-cost patients with mental illness and/or addiction but also obtain rich data on patients’ SES. This research also addresses an important gap in the literature. Few studies have been able to explore the role of individual SES among high-cost patients due to data limitations. Nonetheless, our analysis has a few limitations. While the CCHS is meant to be representative of Canadian residents, it excludes individuals living in institutions, on Aboriginal reserves and in certain remote areas as well as full-time members of the Canadian Forces. 25 As a result, homeless individuals and First Nations people living on reserve have been excluded. Given the high rates of mental illness and substance use among these populations, 26,27 alongside the barriers they face in accessing health care (such as discrimination), it is likely we would have found larger SES inequalities; future research should seek to examine these populations in more detail as well as differences by ethnicity. Additionally, our sample likely includes individuals with less severe forms of mental illness and/or addiction who are more likely to be able to respond to the CCHS. We defined mental illness and/or addiction based on diagnoses available in the existing administrative health care data; some individuals may have obtained mental health and/or addiction-related care that was not captured in the administrative data. Furthermore, we were only able to capture data on individuals who sought and obtained care; many people who struggle with mental illness and/or substance use do not seek care. Although our analysis includes over 90% of health care costs covered under the public health care system, some costs could not be accounted for, as these data are not currently available for research purposes at ICES, namely costs of addiction-related health care provided through community-based agencies. Finally, although we examined individuals at risk of becoming a high-cost patient by examining trajectories over time, we did not employ longitudinal data models, which address the existence of repeated observations on the same individual; this should be explored in future work.
Conclusion
Extensive research has examined high-cost patients; however, little work has examined the role of SES in becoming a high-cost patient for individuals with mental illness and/or addiction. We found that lower SES, such as lower income, food insecurity, and non-homeownership, as well as residential instability at the area-level, are important predictors of future high-cost status among these individuals. Thus, policies aimed at high-cost patients with mental illness and/or addiction, or those concerned with preventing individuals with these conditions from becoming high-cost patients, should also consider non-clinical factors such as income, as well as related dimensions of these, such as food security and homeownership.
Supplemental Material
Supplemental Material, sj-docx-1-cpa-10.1177_07067437211004882 - Looking beyond Administrative Health Care Data: The Role of Socioeconomic Status in Predicting Future High-cost Patients with Mental Health and Addiction: Voir au-delà des données administratives des soins de santé : le rôle du statut socio-économique pour prédire les patients à coût élevé en santé mentale et dépendance
Supplemental Material, sj-docx-1-cpa-10.1177_07067437211004882 for Looking beyond Administrative Health Care Data: The Role of Socioeconomic Status in Predicting Future High-cost Patients with Mental Health and Addiction: Voir au-delà des données administratives des soins de santé : le rôle du statut socio-économique pour prédire les patients à coût élevé en santé mentale et dépendance by Claire de Oliveira, Luke Mondor, Walter P. Wodchis and Laura C. Rosella in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions, results and statements expressed herein are those of the authors and not necessarily those of CIHI and are independent from funding sources. The data from this study is held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the data publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at ![]() DAS. No endorsement by ICES or the Ontario Ministry of Health is intended or should be inferred. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. Note, in 2018, the institute formerly known as the Institute for Clinical Evaluative Sciences formally adopted the initialism ICES as its official name. This change acknowledges the growth and evolution of the organization’s research since its inception in 1992, while retaining the familiarity of the former acronym within the scientific community and beyond.
DAS. No endorsement by ICES or the Ontario Ministry of Health is intended or should be inferred. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. Note, in 2018, the institute formerly known as the Institute for Clinical Evaluative Sciences formally adopted the initialism ICES as its official name. This change acknowledges the growth and evolution of the organization’s research since its inception in 1992, while retaining the familiarity of the former acronym within the scientific community and beyond.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Ontario Ministry of Health and Long-Term Care (Ontario Ministry of Health) to the Health System Performance Research Network (HSPRN: fund #06034, recipient WPW), and by ICES, which is also funded by an annual grant from the Ontario MOHLTC.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.