
Abstract
Objective
New coronavirus (COVID-19) pandemic socioeconomically affected the world. In this study, we measured the perceived stress in response to the COVID-19 pandemic among Iranians to determine the groups at both extremes of the spectrum followed by identifying the stressors and coping mechanisms.
Methods
This study was a mixed-methods study. We distributed a web-based 10-item perceived stress scale (PSS-10), to measure perceived stress score (PSS), through social networks from March 12 to 23, 2020. Then, we interviewed 42 students, 31 homemakers, 27 healthcare providers, and 21 male participants to identify the sources of stress and coping mechanisms.
Results
Finally, 13,454 participants completed the questionnaires. The median and interquartile range (IQR) of the participants’ PSS was 21 (15-25). Students, homemakers, and healthcare workers (HCWs) showed a higher median (IQR) of PSS compared to other groups (23 [18 to 27], 22 [16 to 26], and 19 [14 to 24], respectively). Male participants showed a lower median (IQR) PSS (17 [12 to 23]). Content analysis of 121 participants’ answers showed that the most common stressors were school-related issues mentioned by students, family-related issues mentioned by homemakers, and COVID-19-related issues mentioned by healthcare providers. Male participants’ coping mechanisms were mostly related to the perception of their abilities to cope with the current crisis.
Conclusion
Our participants clinically showed a moderate level of PSS. The main stressors among students, homemakers, and HCWs were related to their principal role in this period, and male participants’ coping mechanisms were inspired by the self-image retrieved from the social perspectives.
Introduction
The new coronavirus disease (COVID-19), first reported by China in December 2019, was swiftly spread around the world to make a pandemic that is economically and socially afflicting. 1,2 The early arrival of the pandemic with all the unknown was substantially tolling on the Iranian population and healthcare system.
In an outbreak of highly contagious diseases, quarantine, uncertainty, overload with an intermixture of fictitious and valid information, risk of death, and resulting economic crisis are contributing factors increasing stress. 3 –8 Stress was associated with higher consumption of alcohol and an increase in smoking, immune dysfunction, cardiovascular diseases, and other medical morbidities. 9 –14 Common resulting psychiatric disorders are post-traumatic stress disorder, depression, anxiety, and suicide. 11,15 –18 During a pandemic, healthcare workers (HCWs) are among the highest risk. They are highly stressed by overtime work, shortage of personal protective equipment (PPE) and training, long-term self-isolation, stigma, high exposure to patients’ death, and risk of infection or death to self and family. 10,19,20 While studies of the mental health impact of the pandemic are emerging, the majority of such data is from China and European countries.
Stress is the first detectable reaction to any change, which activates a cascade of physical and mental reactions. Early screening of stress as the tip of the iceberg of psychosocial consequences helps us to predict the extent of possible psychological and behavioral sequels like suicide. Furthermore, determining correlates of a higher level of stress among a population provides the opportunity for planning to modulate the modifiable factors. 21,22
This is an exploratory study to measure the perceived stress in a large number of Iranian population, using social media, during the COVID-19 pandemic. Furthermore, this study identified self-reported causes of the stress and coping mechanisms among groups with significantly different levels of stress.
Method and Material
Cross-sectional Study
This cross-sectional qualitative study was approved by the review board of Iran University of Medical Sciences. Web-based self-administered Farsi-language survey assessing stress over the past month was distributed via social networks including Instagram, Facebook, LinkedIn, Twitter, WhatsApp, and Telegram from March 12 to 23, 2020. We used a virtual sequential chain-referral sampling method. We recruited 250 initial subjects who were asked to answer and distribute the questionnaire. All were Iranian between 20 and 65 years of age from 31 various provinces (Figure 1S). Fifty percent of them were female. After 3 days, we seeded 100 new subjects who were mostly male, from the provinces and occupations with less participation rate. Finally, 13,454 participants completed the questionnaire.
This anonymous survey had 19 items falling into two sections: sociodemographic data and Cohen’s 10-item perceived stress scale (PSS-10). Demographic questions covered age; gender; occupation; health status; location; practicing self-isolation; confirmed or suspected COVID-19 infection among the participants’ family, friends, or colleagues; and COVID-19-related death among family, friends, or colleagues. The validity and reliability of the Farsi version of PSS-10 were previously shown. 23 Informed consent was signed at the beginning of the survey. The responses were automatically stored in a secure cloud-based database.
Statistical Analysis
A descriptive analysis was performed using the median and interquartile range (IQR) for the quantitative variables and frequencies and 95% confidence intervals (95% CI) for the categorical variables. A χ2 test was used to compare categorical variables. Mann–Whitney U and Kruskal–Wallis tests were used to analyze the differences between quantitative variables across categorical factors. A multivariate binomial logistic regression model was used to identify the independent predictors of high levels of stress as defined by total perceived stress score (PSS) of ≥ 20. The statistical analyses were performed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp.; Armonk, NY, USA). The alpha error was assumed as 5%.
Qualitative Study
A qualitative content analysis study was conducted to arrive at self-reported reasons for higher levels of stress among students, female homemakers, and healthcare professionals in addition to those for lower levels of stress among male participants. We recruited those four groups via an announcement on social networks. We selected participants with a convenience sampling method. We briefly explained our initial quantitative findings and rationale to the participants. After they gave informed consent, the facilitators interviewed participants one on one via end-to-end encrypted private text message or voice chat (Table 1S).
Thirty-six female and 6 male college students older than 18 were interviewed by the 2 interviewers. They were from 14 different programs. The facilitators asked them “What are the sources of stress among students during COVID-19 pandemic?”
Furthermore, 31 female homemakers ages ranging from 32 to 65 years, from 9 different provinces of Iran, were interviewed by the 3 interviewers. The facilitators asked them “What are the sources of stress among homemakers during the COVID-19 pandemic?”
Twenty-three female and 4 male HCWs between ages 25 and 40 were interviewed by an interviewer. Eight nurses and 19 physicians from 7 different specialties, from 11 different provinces of Iran, answered the question. The facilitator asked them “What are the stressors for a HCW during the COVID-19 pandemic?
Twenty-one male participants, between 22 and 66 years of age, were also interviewed by 3 interviewers. They were neither college students nor HWCs, from 6 different provinces of Iran, and they had different occupations, including employees, self-employed, and unemployed. The facilitators asked them “What are the reasons that male participants showed a lower level of stress compared to the total population and female participants during the COVID-19 pandemic?”
Data Analysis
The data analysis was performed manually in a Word document. One researcher coded the answers of each group. Then 2 other researchers separately cross-checked the first. The researchers used an inductive approach, an “open coding” method. The analysis was performed in three steps including reducing, clustering, and abstracting. In reducing, the units of analysis were identified by colour codes. Then, the codes with similar content were clustered together. Finally, clusters were abstracted into the themes and subthemes. The manifest content was only analyzed. The frequencies of reduced expressions were counted. Finally, the extracted results were sent back to the participants to receive their feedback.
Results
Cross-sectional Study
Of the 27,378 survey link views, 13,454 forms were submitted (response rate, 49.1%). One questionnaire was excluded due to incomplete data. Those younger than 18 years old (137 respondents) were also excluded. A final number of 13,316 responses were included in the analysis. The age of the respondents ranged between 18 and 86 with a median (IQR) of 32 (27 to 37). The majorities of the patients were female (77·7%) and were living in Iran (97·4%; Table 2S).
In total, 2,204 respondents (16·6%) identified themselves as HCWs with 38·3% nurses and 28·1% physicians (Figure 2S). General practitioners (22·7%) constituted the majority of the physician survey respondents (Figure 3S). Most of the HCWs were practicing in an outpatient setting (13·7%; Figure 4S). Among the non-HCW respondents, the majority self-identified themselves as homemakers (36·2%) followed by students (11·1%) and office workers (9·5%; Figure 5S).
The experience of the patients concerning COVID-19 infection was summarized in Table 3S. Majority of the survey respondents were healthy individuals (83·1%). Most respondents (75·1%) were practicing social isolation.
The PSS for the respondents ranged from 0 to 40 with the median (IQR) of 21 (15 to 25). More than half of the survey respondents (55·9%) demonstrated a high level of stress as defined by the total PSS of ≥ 20. A weak but statistically significant negative correlation was observed between the respondents’ age and their total PSS (Spearman’s ρ correlation coefficient, − 0·20, P < 0·001). The median of total PSS was higher for females compared to male respondents (female: 21; IQR: 16 to 26; male: 17; IQR: 12 to 23; P < 0·001) as well as that for non-HCWs (21; IQR: 16 to 26) compared to HCWs (19; IQR: 14 to 24; P < 0·001). However, no significant difference was observed between the total PSS among different groups of HCWs (P = 0·698). The total PSS between different job categories among non- HCWs showed a significant difference with higher PSS in students (23; IQR: 18 to 27) and homemakers (22; IQR: 16 to 26) versus lower scores in retirees (14; IQR: 10 to 18). The total PSS between the individuals living in Iran and those living in other countries did not show a statistically significant difference (P = 0·83). Similar patterns of differences were observed for both distress and coping components of PSS-10 (Table 4S).
A statistically significant difference was observed between the levels of stress in individuals with different health status (P < 0·001) with a higher median of total PSS reported for hospitalized individuals (Table 4S, Figure 6S). The total PSS were higher in those who were practicing self-isolation (P < 0·001; Table 4S).
A multivariate binomial logistic regression was designed with high (total PSS ≥ 20) and low (total PSS < 20) levels of perceived stress as the dependent variable and model input variables including those variables that were found as statistically significant in the bivariate analysis. The independent factors in predicting total PSS were summarized in Table 5S. The strongest independent factors in predicting a higher PSS were found as being a patient hospitalized for other medical conditions (odds ratio [OR], 6·0; 95% CI, 1·5 to 24·9; P = 0·013) and being female (OR, 2·3; 95% CI, 2.1 to 2·5; P < 0·001).
Qualitative Study
Students
Total numbers of 102 codes were extracted from 42 answers that categorized into 4 main themes consisted of 25 subthemes. Data saturation was noted from the 35th answer. (Table 1).
The Sources of Stress among Students.
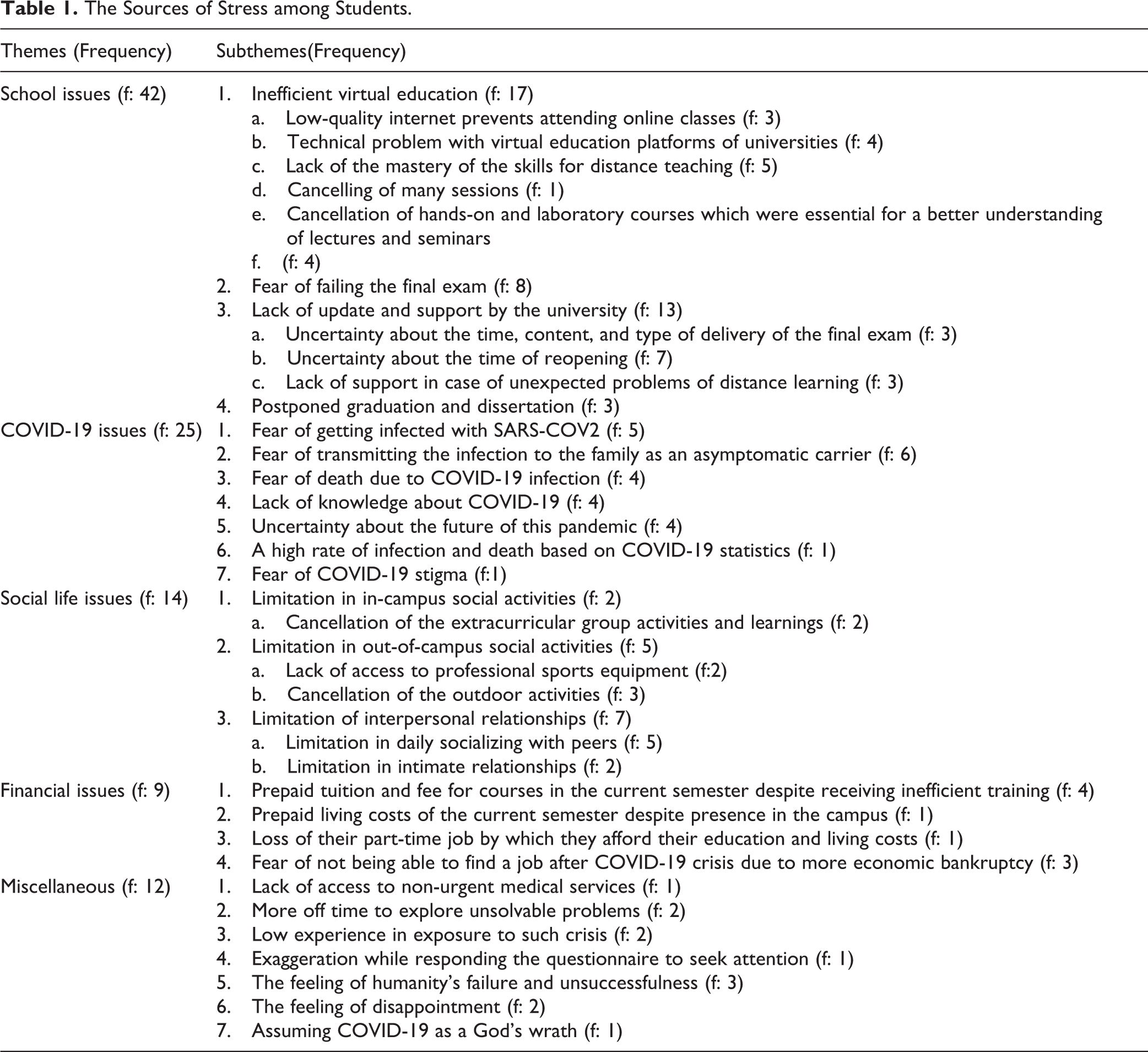
School-related issues, the most frequently mentioned category, was the strongest theme with 42 retrievals among codes. The following quotations were some examples of original data. The virtual education platform of our university is a mess of things. I could not participate in the online classes because of problems with audio, or video, or connection every time. I did not learn anything while I am expected to take the final exam.
Homemakers
Evaluation of 31 answers resulted in 66 codes. Data were saturated at the 21st answer. We categorized the codes into 4 main categories made up of 12 subcategories (Table 2).
The Sources of the Stress among Female Homemakers.
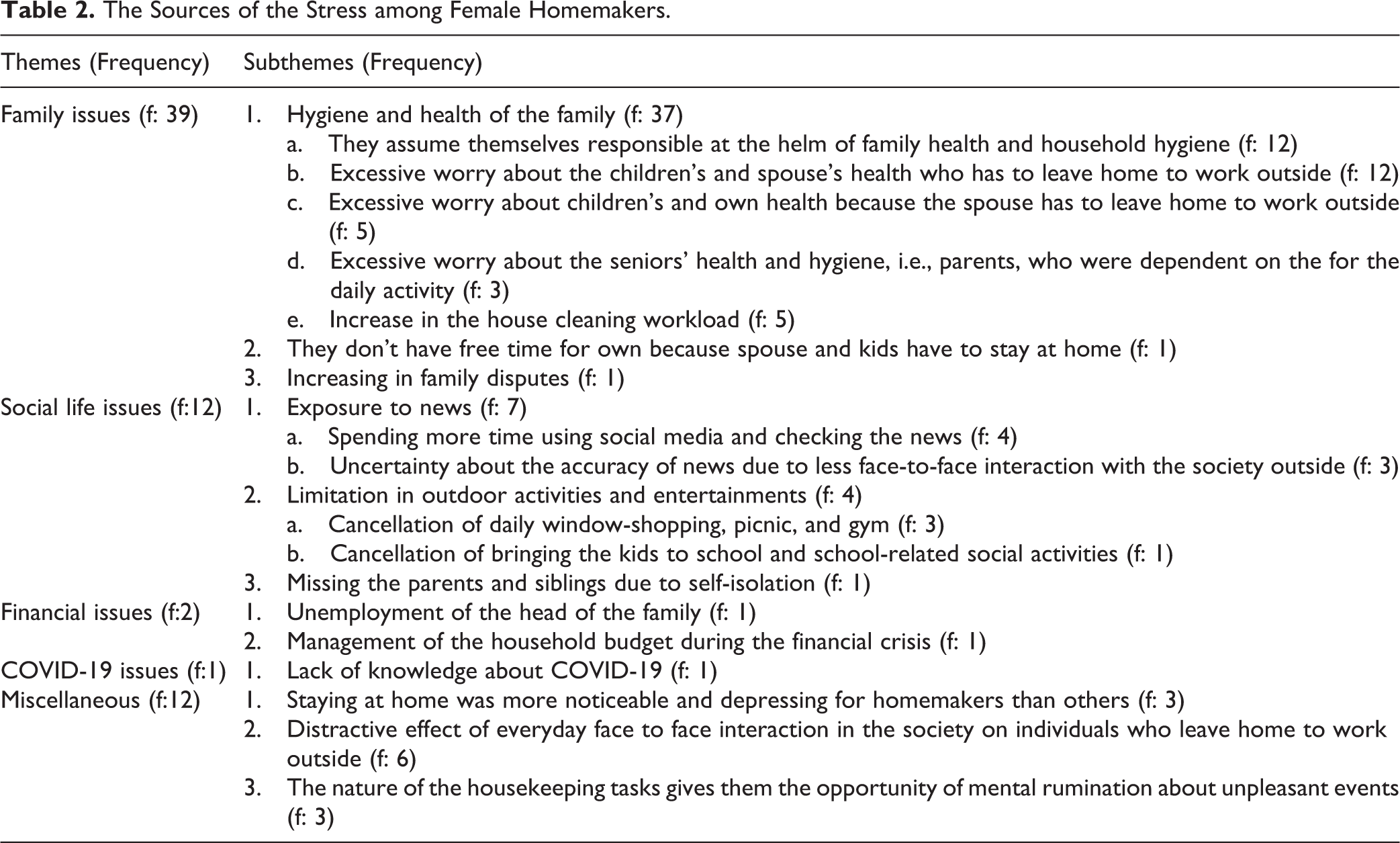
Taking care of the hygiene of the household and health of the family was the most frequent reason mentioned as the cause of homemakers’ high level of stress. The following quotations were some examples of the original data. I am stressed because my husband has lost his job. The family income has dramatically decreased and we have some family disputes.
HCWs
Assessing 27 answers brought about 78 codes. We found that data were saturated at the 25th answer. We sorted the codes into 4 main categories subdivided into 14 subcategories. We brought some examples of the original data below (Table 3). I am afraid that I get the disease or take the disease home. If I catch the disease, who will take care of my baby boy?
The Sources of the Stress Mentioned by Healthcare Providers.
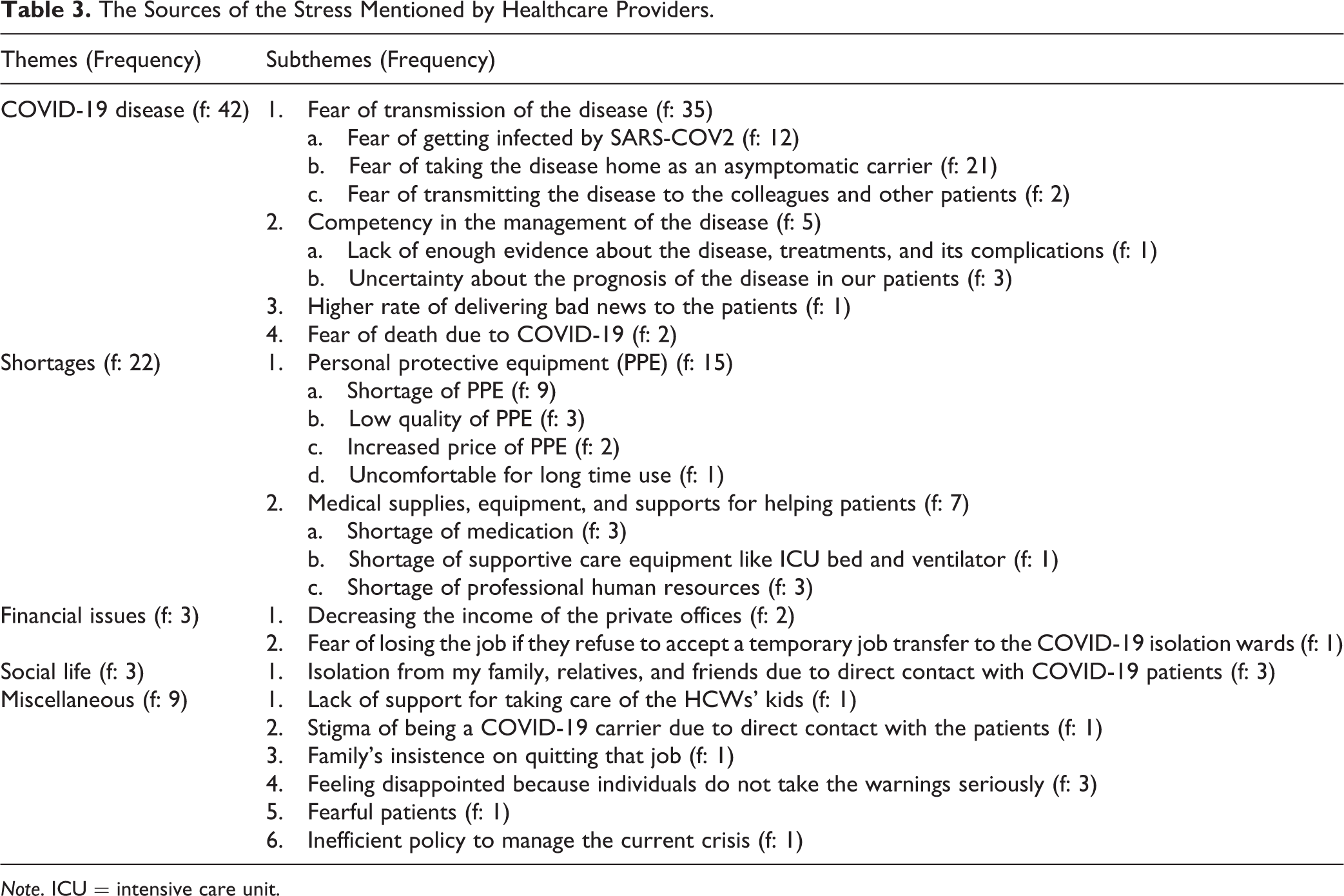
Note. ICU = intensive care unit.
Male Participants
Of 21 answers, 53 codes were highlighted. Data were saturated at the 18th answer. The codes were classified into 4 main categories composed of 16 subcategories (Table 4).
The Mechanisms of Coping with the Stress Mentioned by Male Participants.
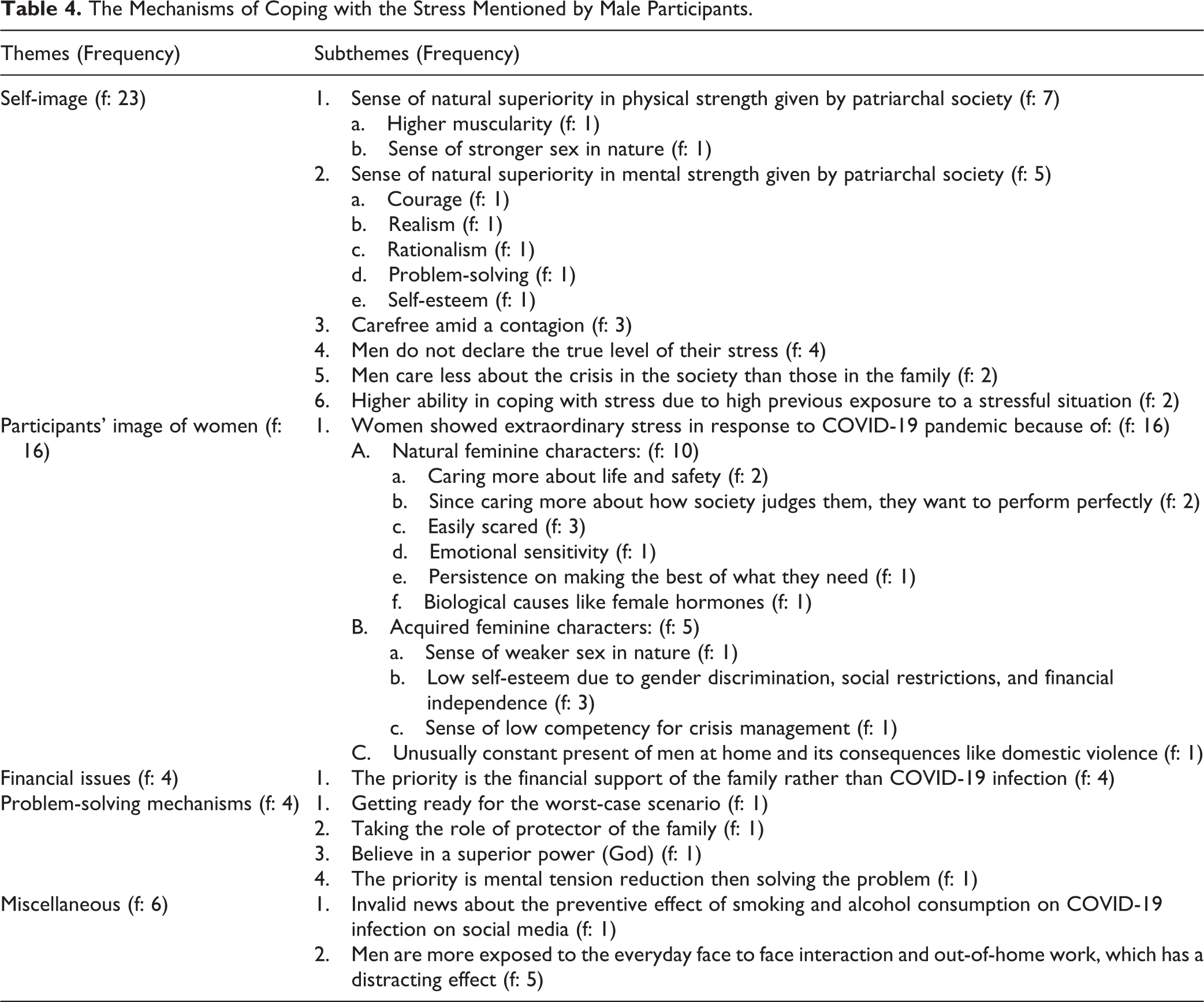
Among Men’s self-image category, the sense of natural superiority in physical and mental strength was the most frequent subcategory. We brought some examples of the original data below. I think that men think that they are powerful due to physical strength or mental excellence in handling difficult situations. Therefore, they have higher self-esteem, which helps them to cope better with stressful situations.
Discussion
To our knowledge, this is the first large study examining the correlates of stress among a large sample of Iranian citizens who have access to the internet and use social medias, the second country hit hard by the pandemic, and still a hot spot. This study showed that Iranian social media users perceived a moderate level of stress, which, compared to the findings of previous study, is lower. 24 It might be due to lower sample size and less diversity among participants in that study. Those scores were higher than the established community norm of 12. 25 Literature review showed no previous evidence for the level of PSS among Iranian general population before COVID-19 pandemic. However, it revealed that the average of our participants’ PSS was higher than the amount of that perceived by Iranian women with infertility referred for the assisted reproductive technology treatment. 26 In this study, the level of stress among COVID-19 patients, HCWs, and healthy controls during the COVID-19 pandemic was a little higher compared to that among Asian patients, HCWs, and healthy controls during SARS outbreak. 27 –29 We think cumulative stress due to rapidly mounting economic crisis and sociopolitical stressors in the country might be the reason for this difference. Since religion has formed a large part of the Iranians’ orientation system, and it is a highly accessible resource in their sociocultural context, it is speculated that Iranians may soothe their stress using religious and spiritual coping methods in the case of insufficient resources and services. 30 However, we showed that our participants had higher levels of stress compared to Asian communities during SARS. It might be rooted in the result of Payir’s study that showed Iranian adults endorsed the importance of science at high levels regardless of their level of religiosity. 31 Therefore, the government’s negligence in establishing and implementing the pandemic-related rules and regulations based on the best current evidence might further increase the stress among Iranians.
We also found no difference in the level of stress between participants in Iran and outside, showing a consistent global pattern of pandemic-related stress. We also found a correlation between social distancing and perceived stress. This could indicate that some level of stress is adaptive and resulting in better compliance with safety measures. The stress is higher among women, homemaker, HCW, and student participants, which was in concordance with the findings in China and Europe during COVID-19 pandemic. 32,33 Literature revealed that women usually show higher levels of impact in response to stress and trauma. 34 Homemaker and student participants are dealing with significant transition and uncertainty. Homemakers, those include feeling responsible for the safety of family, challenge with exposure to contradicting news and instructions on social media about how to take such measures, changes in the family dynamics as the children and spouses are now spending more time at home, interpersonal stress for the same reason, and financial difficulties. Students also have to deal with a quick transition to online school and uncertainty about when the schools open. This is worse given internet infrastructure in Iran is not ideally set for all online work.
Moreover, we found that the amount of stress inversely correlated to the participants’ age, which was in line with the previous findings. 8,24 We also observed that retirees had a significantly lower level of stress. This finding may be due to financial security, less use of unofficial social media, autonomy to choose to stay home regardless of governors’ order, and less change in the normal routine of their life.
Based on the findings in this large number of HCWs, they across different disciplines seem to be stressed almost equally, regardless of their level of contact with COVID-19 patients. The effect of frontline exposure with the patients on the amount of stress perceived by HCWs during an infectious disease outbreak is a controversy among previous literature. 28,35
Besides, our findings showed that non-HCW did not consider the current crisis less stressful than HCWs did, which was in concordance with the findings of previous studies during COVID-19 and SARS outbreaks. 8,29,32 However, the sources of stress may be different between these groups. For example, students mostly identified school-related issues as the source of stress versus homemakers mentioned family-related issues. Whereas, HCWs ranked COVID-19-related issues including fear of death, fear of transmission, and enough competency in the management of the disease as the strongest stressor. In contrary to what published literature has claimed that Iranian HCWs have access to PPE, HCWs ranked shortage, low quality, and increase in price of PPE as the second source of stress. 36 The stressors identified by Iranian HCW in this study were mostly similar to the stressors mentioned by HCWs in the United States. 37 Furthermore, our participants mentioned some additional sources of stress including worry for shortage in medications and therapeutic equipment that they perceived it as their incompetence, job loss, financial insecurity, feeling disappointed and not being understood, and feeling of being stigmatized as a COVID-19 carrier. COVID-19-related stigma and discrimination have been previously reported among HCWs and COVID-19 survivors. 20,38,39 COVID-19-related stigma has some drivers and facilitators that identification of them helps to decrease the nesting of the stigma epidemic via developing an antistigma psychoeducational guide. 20,40 The most frequent source of stress among the most stressful groups has directly related to their job and their principal role in this period. A higher level of stress among women, homemakers, students, and HCWs certainly does not mean that they do not use coping mechanisms. The investigation of their coping mechanisms was not our objective because this study aimed to identify the sources of stress among overwhelmed groups. Besides, we had to shorten the interview and make the questions easy to understand to have more accurate answers and overcome the virtual interview bias.
Furthermore, we identified the groups that perceived lower levels of stress along with their coping mechanisms. Male participants’ coping mechanisms were mostly inspired by gender-oriented self-image rooted in perspectives induced by a patriarchal society. However, it is evident that they are dealing with some stressors during COVID-19 pandemics, as well, which we had to cut the investigations down in benefit of a short and more understandable interview in a virtual setting.
One of the limitations of this study is the generalizability of the findings. Access to the internet and social media, using self-reporting tools, willingness to participate in a survey, virtual interviews, and nonprobability sampling are affecting the representativeness of the study. Using web-based tools, nonprobability sampling and virtual interviews were inevitable in the middle of pandemics for sake of public safety; 72.8% of Iranian families had access to the Internet; 70.5% of them used social media based on the national census in 2017, held by the statistical centre of Iran; however, that access has been increasing by every year as far as broadband Internet penetration rate reached 94% in the first few months of 2020, Communication Regulatory Authority of the Islamic Republic of Iran declared. 41,42 Therefore, we assumed that, of 100 citizens, 94 individuals had access to the Internet at the time of our study. Moreover, we had to use self-reporting tools for data gathering in this study due to safety rules and regulations such as social distancing and self-isolation. The effect of social desirability bias on our data was one of the self-reporting bias, which was prospected during the design phase of the data collection method. To reduce social desirability bias, we chose a predesigned and validated self-reporting instrument; we also guaranteed anonymity and confidentiality at the time of data collection. 43 Our self-reported data can be assumed somehow accurate because we kept the questions short and clear; we avoided difficult concepts; we kept the time frame or recall period short; we guaranteed a strong sense of anonymity and no fear of reprisal. Furthermore, as an incentive to increase the willingness to participate in the study, our team guaranteed to reveal the result of the participants’ PSS, give a brief interpretation of their PSS, and provide the healthcare seekers with virtual primary support. Finally, the results must be conservatively interpreted and generalized.
Women participated in the study 2 times more than men, which may be due to nonprobability sampling, higher levels of stress in women leading to more health-seeking behaviour and a higher rate of social media use. Also, a limited number of hospitalized participants completed the survey due to different reasons including healthcare providers and patients’ families refused to send them the questionnaire, patients’ refusal to complete the survey due to physical or emotional inability, and prohibition of unnecessary contact with isolated COVID-19 wards.
In conclusion, although the findings cannot be easily generalized to the clinical population, it might provide some insight into the sources of stress to be explored among patients who are seen in psychiatric and primary care clinics. The sources of stress in highly vulnerable groups, specifically those mentioned by students, are mostly modifiable. It is expected that authorities and governors provide infrastructures to cope with changes. We suggest that field workers use modified WHO-Psychological First Aid guide to reduce the stress in the public. 44 Since the high level of stress has mental health consequences such as suicide as the worst-case scenario, we suggest the close monitoring of the population by surveys. 44 The development, implementation, and evaluation of mental health interventions, guided by a framework, such as training of the healthcare providers to efficiently screen the psychiatric consequences and providing some publicly available self-learning audiovisual tools to educate the general population about the prevention, alarm signs, and the therapeutic choices of these psychiatric consequences is recomended. 45 Moreover, using a precise and comprehensive COVID-19 mental healthcare toolkit can brought up evidence for research approaches, evaluate the impact of the pandemics on various populations, and shorten the time to action. 46
Supplemental Material
Supplemental Material, sj-pdf-1-cpa-10.1177_07067437211004881 - Perceived Stress among Iranians during COVID-19 Pandemic; Stressors and Coping Mechanisms: A Mixed-methods Approach: Stress perçu chez les Iraniens durant la pandémie de la COVID-19; stresseurs et mécanismes d’adaptation: Une approche de méthodes mixtes
Supplemental Material, sj-pdf-1-cpa-10.1177_07067437211004881 for Perceived Stress among Iranians during COVID-19 Pandemic; Stressors and Coping Mechanisms: A Mixed-methods Approach: Stress perçu chez les Iraniens durant la pandémie de la COVID-19; stresseurs et mécanismes d’adaptation: Une approche de méthodes mixtes by Masoomeh Faghankhani, Faezeh Sodagari, Marjan Shokrani, Hamid Reza Baradaran, Alimohammad Adabi, Masoud Zabihi, Aliyeh Mahdavi Adeli, Mahdi Fathimakvand, Elahe Golalipour, Sina Aghdasi, Arash Javanbakht and Amir Hossein Jalali Nadoushan in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
Masoomeh Faghankhani, Faezeh Sodagari, Arash Javanbakht, and Amir Hossein Jalali Nadoushan equally contributed to this study. The raw data for adults was uploaded as an Excel file.
Acknowledgments
We thank the Dr. Liaosadat Mirsafaei, MD; Hassan Vahidnezhad, PhD; and Amirhossein saeidian, MSc for helping us with circulation of the questionnaire in social media.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.