
Abstract
Objectives:
To examine the trends in cannabis use within 30 days of first admission to inpatient psychiatry in Ontario, Canada, between 2007 and 2017, and the characteristics of persons reporting cannabis use.
Methods:
A retrospective cross-sectional analysis was conducted for first-time admissions to nonforensic inpatient psychiatric beds in Ontario, Canada, between January 1, 2007, and December 31, 2017, using data from the Ontario Mental Health Reporting System (N = 81,809).
Results:
Across all years, 20.1% of patients reported cannabis use within 30 days of first admission. Use increased from 16.7% in 2007 to 25.9% in 2017, and the proportion with cannabis use disorders increased from 3.8% to 6.0%. In 2017, 47.9% of patients aged 18 to 24 and 39.2% aged 25 to 34 used cannabis, representing absolute increases of 8.3% and 10.7%, respectively. Increases in cannabis use were found across almost all diagnostic groups, with the largest increases among patients with personality disorders (15% increase), schizophrenia or other psychotic disorders (14% increase), and substance use disorders (14% increase). A number of demographic and clinical factors were significantly associated with cannabis use, including interactions between schizophrenia and gender (area under the curve = 0.88).
Conclusions:
As medical cannabis policies in Canada have evolved, cannabis use reported prior to first admission to inpatient psychiatry has increased. The findings of this study establish a baseline for evaluating the impact of changes in cannabis-related policies in Ontario on cannabis use prior to admission to inpatient psychiatry.
Introduction
There is a multifaceted relationship between cannabis and mental health conditions. 1,2 Known associations between cannabis use and psychosis are long-standing, even when considering genetic predispositions. 3,4 Associations with other conditions are not as consistent. Some evidence points to a dose–response relationship between cannabis use and the risk of depression. 5 Other studies have found predictive associations between cannabis use and alcohol and substance use disorders, but not mood or anxiety disorders. 6 While a small subset of persons who use cannabis are estimated to have a cannabis use disorder, 7,8 the prevalence of cannabis use disorders is higher among persons diagnosed with other mental health conditions. 9,10 For persons living with a mental health condition, there is little to no evidence of a therapeutic benefit from cannabinoid compounds. 11 Ongoing use of cannabis among persons living with mental illness may exacerbate psychiatric symptoms and interfere with disease management. 12 –15 As such, there is a general consensus that cannabis use as self-medication for mental health conditions is ineffective. 2 Together, these findings underscore the complexities in evaluating the impact of the cannabis-related policies on the onset and clinical management of mental health conditions.
Canada’s medical cannabis policy framework has evolved since 2001 16 and has coincided with a proliferation of illegal online and storefront dispensaries purporting to provide medical access to cannabis. 17 Trends in cannabis use among the general population have varied by age between 2004 and 2014, with the only decrease being among those under 18 years. 18 Among adults, trends in cannabis use among the general population in Canada remained stable between 2004 and 2010 and increased across all age groups between 2011 and 2017. 19 Between 2007 and 2014, the health care costs for cannabis in Canada increased by 28%, 20 where hospital stays for cannabis-use disorders increased by 40%. 21 Similarly, hospitalizations in the United States associated with cannabis use disorders have increased with the emergence of medical and nonmedical cannabis policies. 22,23 Furthermore, variations in medical cannabis policies across the United States are associated with variations in prevalence of severe mental illness. 24 With evolving cannabis policies in Canada, there remains a need to understand broader patterns of cannabis use among persons with mental illness.
This study examines trends in cannabis use prior to first psychiatric hospital admissions in Ontario, Canada, between 2007 and 2017, the year prior to legalization of cannabis for nonmedical use. We also examine the characteristics associated with reports of cannabis use prior to admission.
Methods
Data
Using a retrospective cross-sectional design, we analyzed data from the Ontario Mental Health Reporting System (OMHRS) of the Canadian Institute for Health Information (CIHI). The OMHRS is based on data from the Resident Assessment Instrument for Mental Health (RAI-MH), an assessment mandated for use since October 2005 in all psychiatry beds in Ontario, Canada. CIHI is responsible for data quality checks that include reporting inappropriate data to the submitting hospital and requesting data corrections. Data for this study were obtained through a sharing agreement between CIHI and interRAI Canada at the University of Waterloo. This study received approval from the Office of Research Ethics at the University of Waterloo.
The RAI-MH includes 396 items that are completed at admission and at discharge to designated psychiatric beds. 25 The RAI-MH includes domains assessing mental and physical health status, substance use, cognitive performance, daily functioning, social relationships, education and employment, and health service use. Clinical staff complete the assessment using multiple sources of information, such as interviews with the person, information available in the health record, and information from other key informants (e.g., family members, first responders, and other clinical staff who are familiar with the person). 25 The majority of the items are observational. For instance, when coding hopelessness the assessor would record the number of days in the prior 3 days that the person expressed hopelessness as reported by the person or as observed by, for instance, the clinical team. Training and ongoing support for the completion of the RAI-MH are provided to hospital staff by CIHI and by clinical educators embedded within hospitals.
Service Context and Sample
Inpatient psychiatric services in Ontario include secondary and tertiary services offered in a mix of psychiatric units in community hospitals and designated psychiatric hospitals. Most inpatient psychiatric services are publicly funded under universal health coverage administered by the Province of Ontario. The majority of admissions in Ontario are classified as acute where the goal is crisis assessment and stabilization, with several hospitals also offering specialized services such as psychosocial rehabilitation, concurrent substance use treatment, and geriatric psychiatry. 26,27 In Ontario, inpatient psychiatric care is often the first point of contact to the health system for persons experiencing a first-episode mental illness. 28
We included data for all persons aged 18 years and older at their first admission to a psychiatric hospital for all admissions that occurred between January 1, 2007, and December 31, 2017. First admissions were identified by selecting the first hospital stay for each person in the OMHRS data and then including only patients who had no previous admissions to a psychiatric bed (an item on the RAI-MH). Stays of less than 72 hrs were excluded as not all items from the RAI-MH are completed for these patients. Forensic patients were excluded given that administrative parameters such as apprehension and initial confinement may have limited their access to cannabis in the 30 days prior to being assessed with the RAI-MH. The final sample included 81,847 patients.
Variables
A brief description of all study variables can be found below. For a more comprehensive description of all variables, please refer to the Supplemental Files.
Cannabis and other substance use behavior
The RAI-MH captures patterns of substance use based on the time since the person last used cannabis, opiates, cocaine/crack, stimulants, inhalants, and/or hallucinogens. A binary variable was created for each substance based on use of the substance within 30 days of the date of admission to hospital. Use within the prior 30 days can be considered a proxy indicator of more frequent or persistent use. 29,30 It was not possible to identify patients who had never used cannabis (or other substances) as the item uses the same code for patients who had used cannabis more than 1 year ago and for patients who have never used cannabis. Other substances of interest included use of alcohol in the prior 14 days and daily use of tobacco. On the RAI-MH, potential problems with addiction are assessed using a scale that sums 4 items scored as yes/no: expressions of guilt about substance use, feels the need or been told by others to cut down on substance/alcohol use, bothered by criticism of substance/alcohol use, and need to use substances/alcohol first thing in the morning. Scores ≥2 were considered indicative of problematic substance or alcohol use.
Demographic factors
Demographic variables included year of admission, age at admission (18 to 24, 25 to 34, 35 to 44, 45 to 54, 55 to 64, 65 and older), marital status, highest level of education, living alone prior to admission, residential instability, homelessness, employment status, and any lifetime financial hardship (major loss of income or serious economic hardship due to poverty). Gender was coded as male or female.
Diagnoses
The RAI-MH captures diagnostic categories from the Diagnostic and Statistical Manual of Mental Disorders (DSM) based on the diagnosis assigned by a psychiatrist overseeing the care of the person. Primary, secondary, and tertiary DSM diagnoses from the discharge assessment were included. For admissions between 2007 and 2015, categories were based on the fourth edition of the DSM, 31 while admissions from 2016 to 2017 were coded based on categories from the fifth edition. 32 For ease of interpretation, diagnostic categories from the fifth edition were cross-walked to their analogue in the fourth edition. For instance, the DSM-V category for trauma- and stressor-related disorders was grouped with the DSM-IV category for anxiety disorders. The 7 diagnostic groups used for analysis were neurocognitive disorders, substance-related and addictive disorders (excluding cannabis use), schizophrenia spectrum and other psychotic disorders, mood disorders (bipolar and related disorders, and depression), anxiety disorders, personality disorders, and other disorders. The “other” diagnostic category included categories found in less than 5% of the study population. Cannabis use disorders, which included both cannabis abuse and cannabis dependence, were identified using the DSM-IV (304.3, 305.2) and DSM-V (F12.1 or F12.2) codes that were available from the OMHRS data.
Clinical characteristics
Variables used to assess social life included having supports for discharge; interpersonal conflict with friends, family, and/or staff; history of emotional, sexual, or physical abuse; and police intervention for crime within the prior year.
Symptom severity was evaluated using several items and subscales from the RAI-MH. Risk of harm to self was based on items assessing the presence of self-injurious acts or self-harm ideation within the 30 days prior to admission and history of suicide attempt. Violent behavior in the 30 days prior to admission was identified using 3 items: violent acts, threats, or ideation. Physical pain was based on an item measuring the frequency of pain experienced by the patient in the 3 days prior to assessment (daily, less than daily, no pain). The Positive Symptom Scale (PSS) sums items measuring the frequency of hallucinations, command hallucinations, delusions, and abnormal thoughts into a scale ranging from 0 to 12, with higher scores indicating greater number and frequency of positive symptoms of psychosis. 33 The Social Withdrawal Scale ranges from 0 to 6 based on the presence of the following 6 symptoms over the prior 3 days: lack of motivation, anhedonia, loss of interest, reduced interaction, decreased energy, flat affect. 34 The Cognitive Performance Scale ranges from 0 to 6 based on a decision tree that considers several RAI-MH items, including cognitive skills for daily decision-making and short-term memory. 35 The Depressive Severity Index ranges from 0 to 15 based on a sum of 5 items, including persistent crying/tearfulness and hopelessness. 36 A Mania Scale with a range of 0 to 18 was constructed for this study by summing 6 items: inflated self-worth, hyperarousal, irritability, increased sociability/hypersexuality, pressured speech/racing thoughts, and labile affect. In the data set used for this study, the Cronbach α of the Mania Scale was 0.76.
Statistical Analysis
All analyses were conducted using Statistical Analysis Software (SAS) 9.4. Overall trends in cannabis use within 30 days of admission were reported for the period between 2007 and 2017, as well as by age, gender, and DSM diagnostic categories. Chi-square analyses were used first to identify demographic and clinical factors significantly associated with 30-day cannabis use (results available in the Supplemental Files). Multivariable logistic regression models were fit using candidate variables with year of admission being added to the final model. Model fit was assessed by the area under the curve (AUC). We then tested 2-way interaction terms to examine differences in 30-day cannabis use across diagnostic groups and gender, age, and first admission status.
Results
Descriptive statistics of patients over time are found in Table 1. The proportion of patients aged 18 to 24 increased by 7.4% from 2007 to 2017, while the proportions decreased for those aged 35 to 44 and 45 to 54. The proportion of patients admitted involuntarily decreased over time, from 21.5% in 2007 to 13.9% in 2017. There was a 4.0% increase in the proportion of patients with schizophrenia or other psychotic disorders and a 10.4% increase in anxiety disorders. While the proportion of patients with a noncannabis substance use diagnosis decreased by 4.2%, the proportion with cannabis use disorders increased from 3.8% to 6.0% between 2007 and 2017.
Characteristics of Patients at First Admission to Inpatient Psychiatry in Ontario, Canada, between 2007 and 2017.
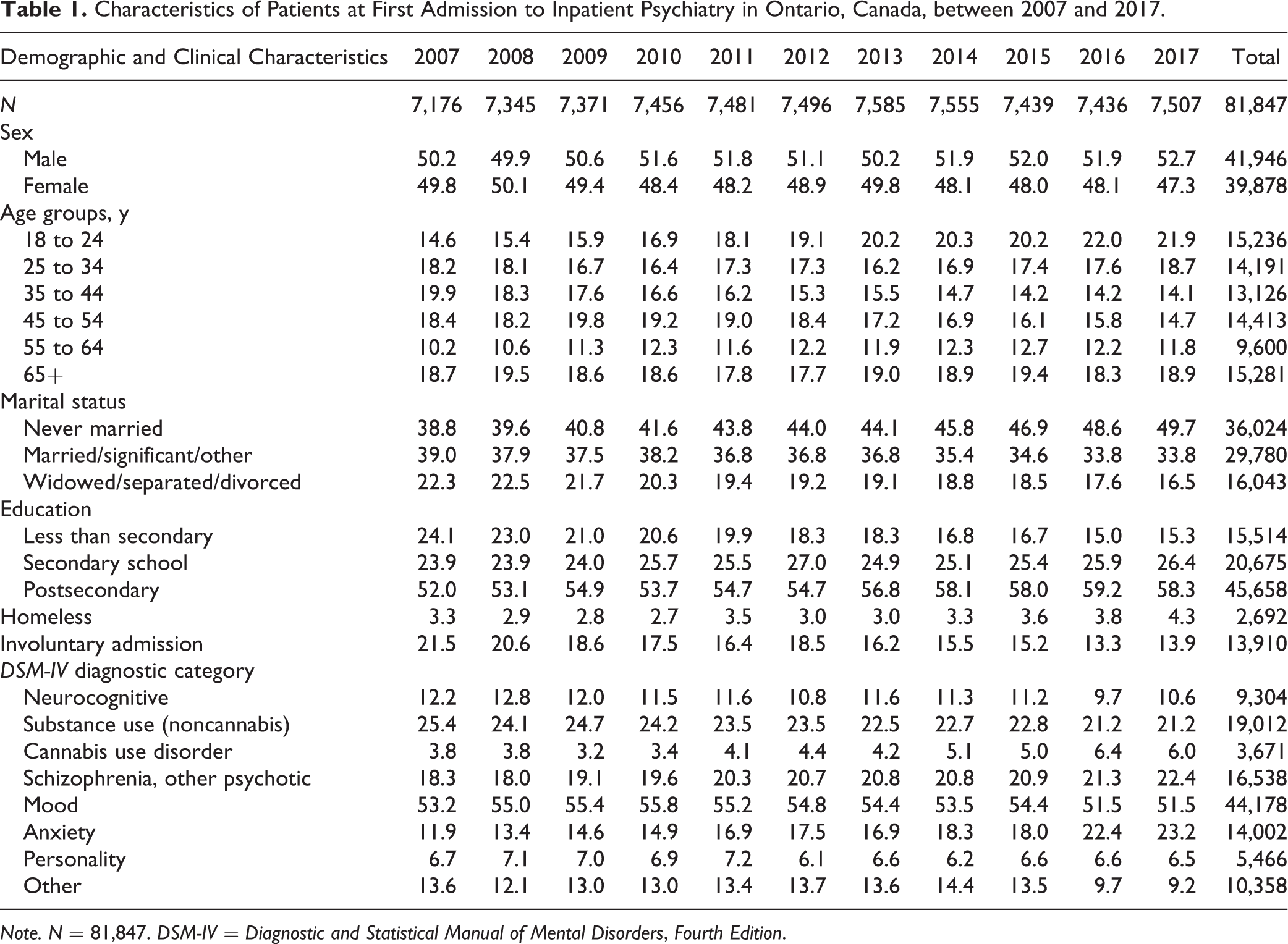
Note. N = 81,847. DSM-IV = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition.
Across all years, the proportion of inpatients reporting cannabis use within 30 days of admission was 20.1% (n = 16,463). Table 2 reports the proportion of patients using cannabis within 30 days of admission by demographic and diagnostic characteristics. The proportion of patients who used cannabis increased from 16.7% to 25.9%. Cannabis use was more common among males and increased by 9.9% between 2007 and 2017 (compared to a 7.9% increase among females). In 2017, 47.9% of patients aged 18 to 24 and 39.2% of patients aged 25 to 34 had used cannabis within 30 days of admission, representing increases of 8.2% and 10.7%, respectively. While relatively few patients aged 55 to 64 used cannabis, the proportion reporting cannabis use more than doubled between 2007 and 2017. Among conditions where cannabis use was more common, the highest relative increase in cannabis use by diagnosis was among patients with anxiety disorders (93.1%), personality disorders (77.8%), and schizophrenia or other psychotic disorders (79.4%).
Proportions of Patients Reporting Cannabis Use Within 30 Days of First Admission to Inpatient Psychiatry in Ontario, Canada, by Gender, Age Categories, and DSM-IV Diagnostic Categories.
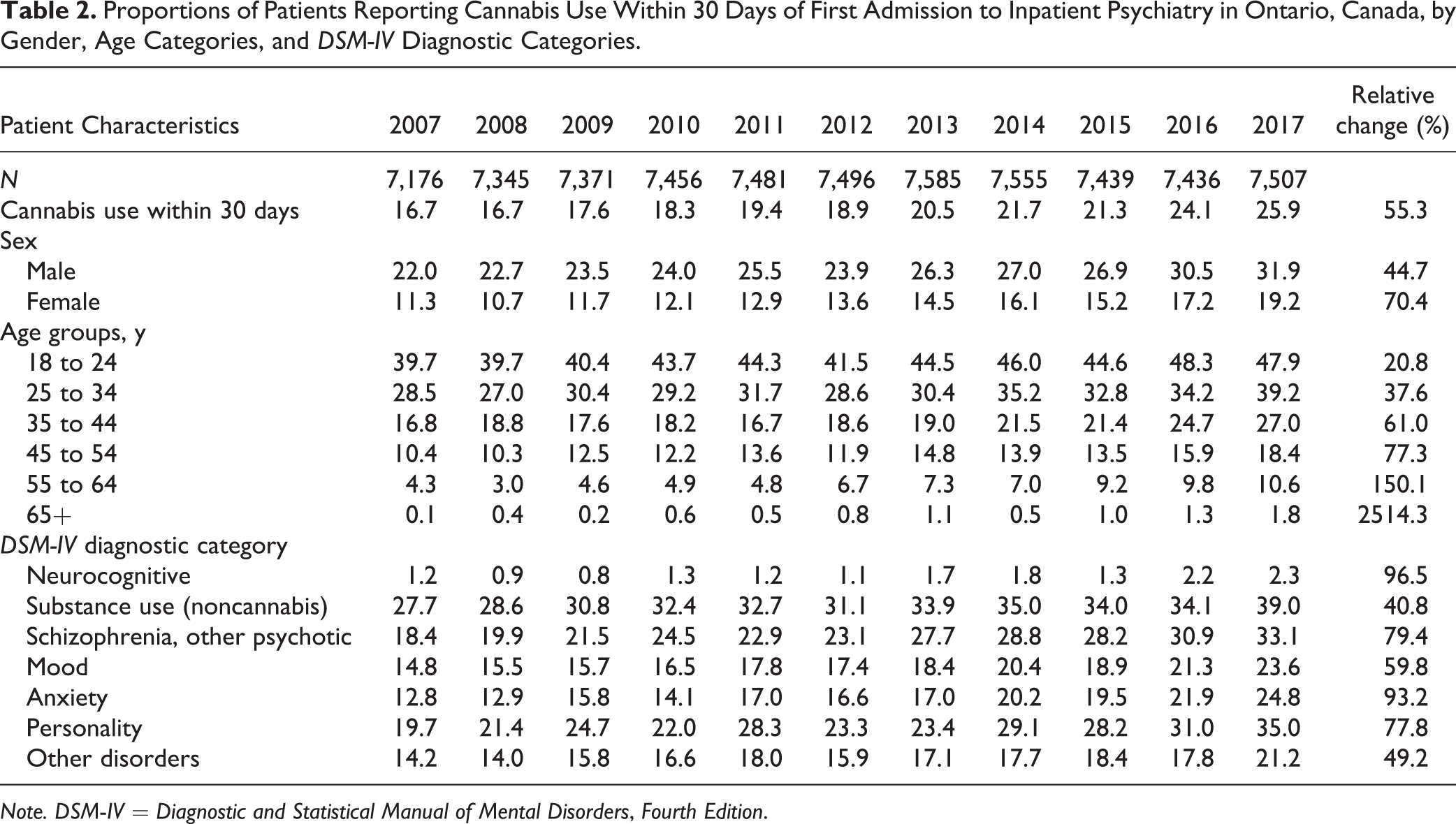
Note. DSM-IV = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition.
Results of the main effects logistic regression model can be found in Table 3 (AUC = 0.88). Holding all other variables constant, the odds of cannabis use prior to admission decreased as patient age and/or cognitive impairment increased, and among those who were married and/or had a higher level of education. Patients who were male and those who experienced any lifetime abuse had greater odds of cannabis use. Patterns of substance use were strongly associated with cannabis use, including daily tobacco use, alcohol use in the prior 14 days, substance use diagnoses, and use of other substances in the 30 days prior to admission. Having schizophrenia or other psychotic disorders or a mood disorder was also associated with greater odds of cannabis use compared to those without these disorders. Those who experienced violence ideation or threatened violence were 36% more likely to have used cannabis compared to those with no violent behavior. For a 1 point increase in the PSS, there was a 3% increase in the odds of cannabis use. A 1 point increase in the Mania Scale was associated with an 8% increase in the odds of cannabis use prior to admission. While the odds of cannabis use did not significantly differ between 2007 and 2008, the odds of cannabis use increased linearly across years of admission with patients in 2017 being more almost twice as likely to have used cannabis prior to admission compared to patients admitted in 2007.
Multivariable Logistic Regression Results Examining Factors Associated with Cannabis Use Within 30 Days of Admission to Inpatient Psychiatry in Ontario, Canada, from 2007 to 2017.
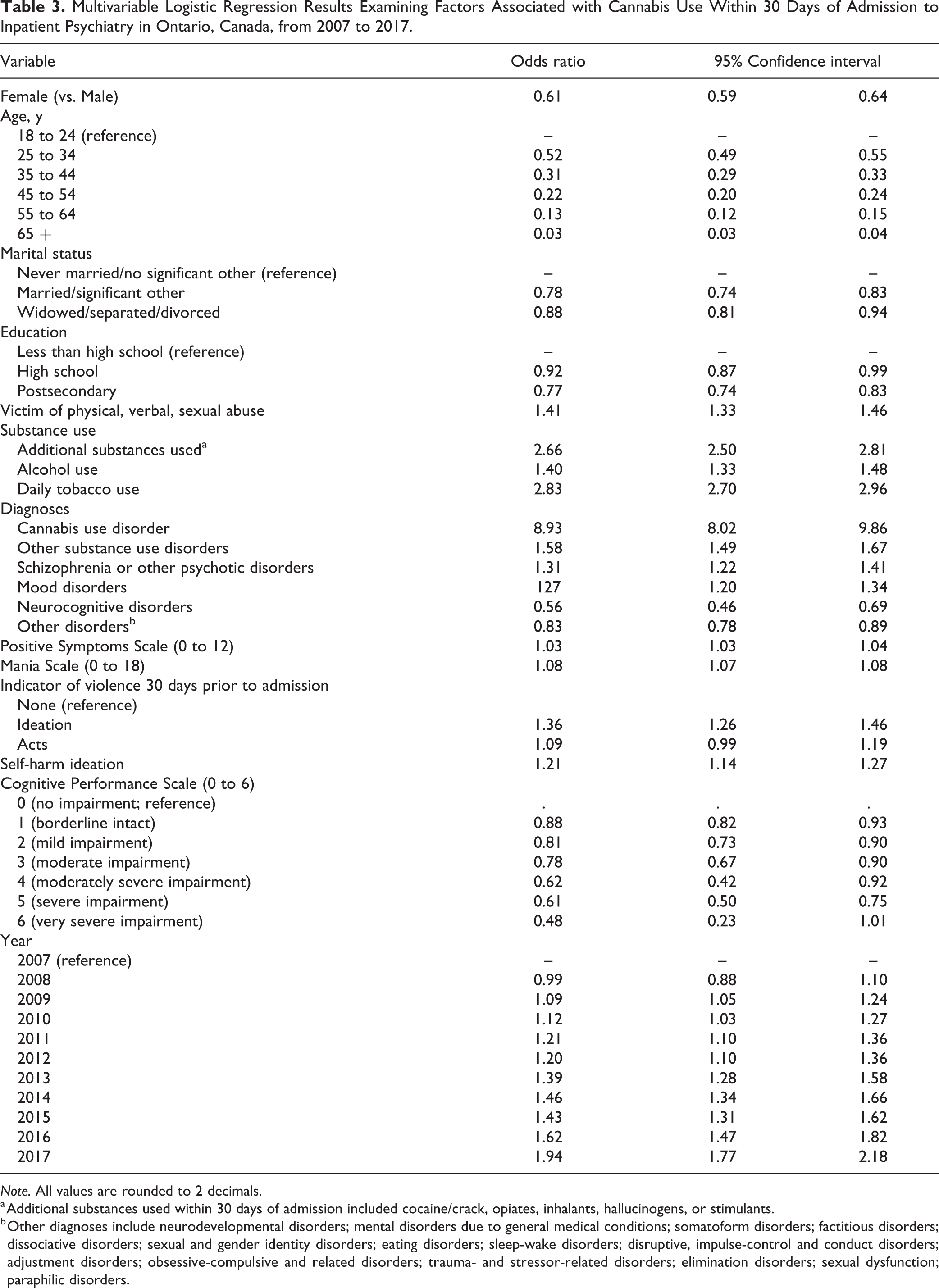
Note. All values are rounded to 2 decimals.
a Additional substances used within 30 days of admission included cocaine/crack, opiates, inhalants, hallucinogens, or stimulants.
b Other diagnoses include neurodevelopmental disorders; mental disorders due to general medical conditions; somatoform disorders; factitious disorders; dissociative disorders; sexual and gender identity disorders; eating disorders; sleep-wake disorders; disruptive, impulse-control and conduct disorders; adjustment disorders; obsessive-compulsive and related disorders; trauma- and stressor-related disorders; elimination disorders; sexual dysfunction; paraphilic disorders.
A significant interaction was found between gender and schizophrenia (Wald χ2 = 16.95, df = 1, P < 0.0001). Figure 1 shows that the proportion of males with schizophrenia and other psychotic disorders who used cannabis was 12.1% higher than males without this diagnosis. There proportion of females with schizophrenia who used cannabis was 1.6% lower compared to the proportion of females without this diagnosis.
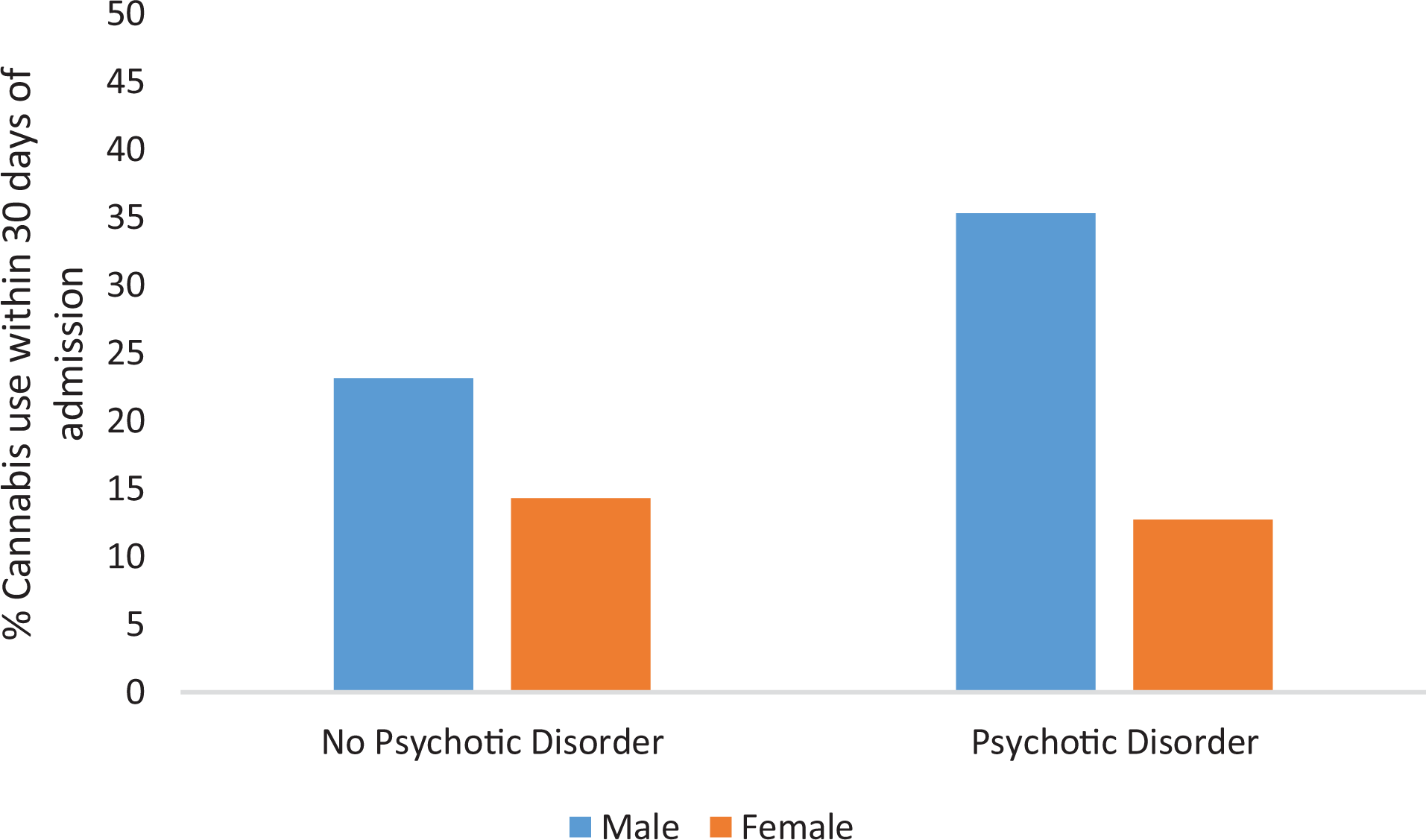
Percentage of patients with and without psychotic disorders, by gender, who used cannabis within 30 days of first hospital visit to inpatient psychiatry.
Discussion
This study identified a significant increase in the proportion of patients who used cannabis within 30 days of their first admission to inpatient psychiatry in Ontario, Canada, between 2009 and 2017, compared to 2007. The increase was evident by gender, age, and most diagnostic groups. These findings confirm that cannabis use is more common among persons admitted to inpatient psychiatry compared to general population estimates. For instance, compared to 20% of psychiatric inpatients reporting cannabis use within 30 days of first admission, about 14% of adults in the general population of Ontario reported using cannabis in the prior year in 2017. 37 These differences persist across age groups; for instance, 48% of patients aged 18 to 24 in this study reported cannabis use prior to admission in 2017 compared to 31% of those of the same age group in the Canadian population. 37 Interestingly, the age-adjusted proportion of the Canadian population who reported cannabis use increased by about 7% among males and 6% among females between 2011 and 2017. 19 Therefore, the increasing proportion of psychiatric patients reporting cannabis use may be one indicator of a broader national trend of increased use of cannabis among adult Canadians.
We found that demographics, health behaviors, clinical symptoms, diagnoses, and life experiences were associated with the use of cannabis prior to admission. The nature and implications of these results may be broad, requiring further research. It will be important to further examine the association of cannabis use and mood disorders, including whether use of cannabis is associated with psychotic features of these disorders. Further research is also needed to examine whether cannabis use is associated with the onset of or attempts to cope with the emotional circumstances related to violent ideation or self-harm ideation. The interaction between gender and psychotic disorders provides new insights into the existing relationship between schizophrenia and cannabis. Although sex differences are known in the clinical presentation and prognosis of schizophrenia, 38,39 the differences in cannabis use found among men and women with schizophrenia are not well understood. These differences may relate to variations in how cannabis is metabolized and experienced by each sex 40 and the potential impact this difference might have on ongoing use of cannabis and the onset or course of schizophrenia. Further research is needed to examine this hypothesis using biological measures of sex that were not available in this study. Finally, the multivariable findings of this study may also be useful in evaluations of cannabis-related policies, particularly as covariates to consider when comparing patterns of cannabis use among different cohorts of psychiatric inpatients over time.
There are a number of questions that arise from the trends observed in this study. First, could these trends relate to changing sentiment around the use of cannabis? Several examples from the United States indicate that reduced social stigma and risk perception has resulted in increased use of cannabis. 41 –43 These changing social perceptions may account for the narrowing gap in use among males and females. 44 Additionally, there may have been changes in the social or clinical norms of reporting or discussing the clinical context of cannabis use between clinicians and patients. We must recognize the possibility then that the proportion of patients using cannabis prior to admission were underestimated. However, given that cannabis use increased across a broad set of individual characteristics, including factors like psychosis that have had longer standing associations with cannabis, it seems more plausible that reporting bias was limited.
Second, are increases in cannabis use prior to first admission to inpatient psychiatry related to increases in the use of cannabis for self-medication of unmet mental health needs among the general population? Self-medication to cope with mental health challenges has become a prominent theory to explain use of cannabis 2 . However, with limited evidence supporting the effectiveness of cannabinoids in treating mental health conditions, 11 use of cannabis to self-medicate may actually lead to a vulnerability to addiction or to the development of other mental health conditions. 2 This cannot be answered by the data presented in this study because reasons for use were not assessed. Instead, we present this as a hypothesis to be addressed in future research. By definition, all patients in this study have a mental health concern. If patients admitted to inpatient psychiatry were using cannabis to self-medicate prior to admission, an opportunity exists for counselling and education about the risks of that practice. With limited access to mental health care in some areas in Ontario, 45 it may be that increases in cannabis use prior to psychiatric admission reflect attempts to cope with mental health conditions.
Third, are increases in the proportions of patients using cannabis prior to first admission to inpatient psychiatry related to changes in cannabis policies? The findings of this study spanned much of the period where access increased to illegal cannabis retail outlets, and medical cannabis policies evolved. 16,17 For instance, before being repealed and replaced by the nonmedical cannabis policies within Canada’s Cannabis Act in 2018, allowances had been introduced into the Access to Cannabis for Medical Purposes Regulations for home growing of cannabis, including for personal use and on behalf of one with a medical authorization for use. 16 In other jurisdictions, liberal medical cannabis policies that provided broader opportunities to access cannabis were associated with higher prevalence of mental illness compared to jurisdictions with more restrictive policies. 24 Therefore, it may have been that the liberalization in cannabis policies in Canada was associated with increases in the proportions of individuals using cannabis prior to first admission to inpatient psychiatry.
Limitations
The secondary analysis of health care data introduces the potential for reporting and selection biases. Our findings cannot generalize to all persons with mental health conditions or all persons using cannabis in Ontario, Canada. Additionally, we were not able to ascertain the reasons for and frequency of a person’s cannabis use, including use for medical purposes. We also could not examine the ratio of tetrahydrocannabinol to cannabidiol within the cannabis that was used. We were not able to account for potential changes to the organization and delivery of inpatient services between 2007 and 2017. Other than a decrease in involuntary admissions, other indicators of case mix, including the use of other substances, did not change. However, since we only had data on patients with stays greater than 72 hrs, we could not account for changes in clinical knowledge or practice patterns that may have led to differences in who was actually admitted to hospital among all persons using cannabis prior to presenting to hospital.
Conclusion
Cannabis use prior to admission has become more common among persons at first admission to inpatient psychiatry in Ontario, Canada. While underscoring the importance of clinically reviewing cannabis use among all patients admitted to inpatient psychiatry, these findings also establish a baseline for evaluating the impact of changes in cannabis-related policies in Ontario on rates of cannabis use among patients a first time admissions to inpatient psychiatry.
Supplemental Material
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720984679 - How High? Trends in Cannabis Use Prior to First Admission to Inpatient Psychiatry in Ontario, Canada, between 2007 and 2017: À quelle hauteur? Les tendances de l’usage du cannabis avant la première hospitalisation en psychiatrie en Ontario, Canada entre 2007 et 2017
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720984679 for How High? Trends in Cannabis Use Prior to First Admission to Inpatient Psychiatry in Ontario, Canada, between 2007 and 2017: À quelle hauteur? Les tendances de l’usage du cannabis avant la première hospitalisation en psychiatrie en Ontario, Canada entre 2007 et 2017 by Taylor McGuckin, Mark A. Ferro, David Hammond, Shannon Stewart, Bridget Maloney-Hall, Nawaf Madi, Amy Porath and Christopher M. Perlman in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, sj-docx-2-cpa-10.1177_0706743720984679 - How High? Trends in Cannabis Use Prior to First Admission to Inpatient Psychiatry in Ontario, Canada, between 2007 and 2017: À quelle hauteur? Les tendances de l’usage du cannabis avant la première hospitalisation en psychiatrie en Ontario, Canada entre 2007 et 2017
Supplemental Material, sj-docx-2-cpa-10.1177_0706743720984679 for How High? Trends in Cannabis Use Prior to First Admission to Inpatient Psychiatry in Ontario, Canada, between 2007 and 2017: À quelle hauteur? Les tendances de l’usage du cannabis avant la première hospitalisation en psychiatrie en Ontario, Canada entre 2007 et 2017 by Taylor McGuckin, Mark A. Ferro, David Hammond, Shannon Stewart, Bridget Maloney-Hall, Nawaf Madi, Amy Porath and Christopher M. Perlman in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
The study sample was drawn from OMHRS data collected and maintained by CIHI. CIHI and the University of Waterloo have a data-sharing contract permitting the use of anonymized data for research purposes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mark Ferro serves on the editorial board of the Canadian Journal of Psychiatry. The remaining authors have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Canadian Institutes of Health Research Catalyst Grant: Population Health Intervention Research on Legalization of Cannabis/ Subvention catalyseur: Recherche interventionnelle en santé des populations liée à la légalisation du cannabis.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.