
Abstract
Objective:
Assessing global functioning in psychiatric emergency settings is important for clinicians to estimate severity of mental disorders, devise a treatment plan, and assess the evolution of their patients’ progression over time. The World Health Organization Disability Assessment Schedule-2.0 (WHODAS-2) measures psychological, social, and professional functioning and is recommended as a standardized instrument of choice for use in psychiatric settings. Yet, studies investigating disability profiles of mental disorders using the WHODAS-2 are scarce, and psychometric properties have not been evaluated in a psychiatric emergency context. We describe and compare WHODAS-2 (12-item version) scores across mental disorders (anxiety, mood, psychotic, personality, and substance abuse) in adults admitted to psychiatric emergency.
Methods:
Data from the Signature Bank were used. Participants admitted to psychiatric emergency completed the WHODAS-2 at admission (n = 1,125). Mental disorders were evaluated by psychiatrists, and WHODAS-2 scores were compared across groups. Psychometric properties were evaluated using confirmatory factor analysis (CFA).
Results:
Higher mean WHODAS-2 scores were reported by those with anxiety, mood, and personality disorders (P < 0.001) compared to other psychopathologies. The measure showed good internal consistency (global score α = 0.88; domain subscores α = 0.59 to 0.85) and acceptable goodness of fit indices in CFA confirming the original structure of WHODAS-2.
Conclusions:
Findings from this large-scale study could assist clinicians in interpreting WHODAS-2 scores in psychiatric populations and provide a more detailed portrait of disability profiles associated with different clinical diagnoses.
Introduction
Mental illness is associated with compromised health outcomes worldwide. The Global Burden of Disease Study 1 demonstrates that mental disorders account for 7.4% of disability-adjusted life years, with anxiety and depression ranking among the top two psychiatric causes of disability. Disability stemming from mental illness significantly contributes to the global burden of disease by hindering individuals’ daily activities and productivity, and significant healthcare resources are allocated to improving nonfatal sequelae of illness. 2,3
Disability measures inform on the overall health of populations. From a clinical standpoint, disability assessment predicts service needs and functional outcomes; information that diagnosis alone cannot provide. 4,5 A valid measure of disability based on a cross-culturally generalizable conceptual framework is important for developing comparable and efficient clinical practice and for optimal health management and planning. 4,6 To that effect, the World Health Organization (WHO) developed the International Classification of Functioning, Disability and Health (ICF) in the early 1990s, a framework for defining and classifying functioning and disability. 7 The ICF’s definition of disability is based on the biopsychosocial model and focuses on the relationship between health problems and affected contextual factors. 5 Based on the ICF’s model of disability, the World Health Organization Disability Assessment Schedule 2.0 (WHODAS-2) was created in 1998 to assess global functioning, such as an individual’s ability to perform in different domains of life. The WHODAS-2 was devised for use in healthy and clinical populations, including individuals with physical and psychological disorders.
Prior to the WHODAS-2, global functioning was commonly evaluated in psychiatric settings during a clinical interview using the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV 8 ) Global Assessment of Functioning (GAF) Scale. Functioning was estimated on a numerical scale ranging from 0 to 100. The GAF required a high degree of clinical judgement, substantially limiting its interrater reliability (r = 0.39 to 0.59). 9
In contrast, advantages of the WHODAS-2 include a clear conceptual framework based on the ICF’s biopsychosocial model of disability, the use of Likert scales that improve interrater reliability and a brief format. While the GAF only provides a general functioning score, the WHODAS-2 also includes subscales corresponding to different domains of functioning. Strong psychometric properties have been confirmed for the short 12-item 10,11 and long 36-item 12 WHODAS-2 versions. Across studies including mental and physical health problems, the WHODAS-2 shows good reliability, ability to discriminate among groups, good change sensitivity, adequate structure fit, and good convergent validity with other scales measuring disability, general health and quality of life. 10 –22 While the WHODAS-2 is neither diagnostic nor mental health specific, its qualities led the DSM-5 expert committee to recommend it as the standardized instrument of choice for evaluating global functioning in psychiatric settings. 23
Global functioning is altered in individuals suffering from psychopathology, and its evaluation helps mental health practitioners to assess disorder severity and elaborate rehabilitation strategies. 24 Lower functioning was reported in individuals with anxiety disorders, 25,26 mood disorders, 27,28 psychotic disorders, 13,14,29 personality disorders, 30 and substance abuse. 31 Consistent with findings from the Global Burden of Disease Study, those suffering from anxiety, depression, and schizophrenia seem to be most severely affected 1,14 ; however, further studies are needed to confirm these findings. In psychiatric emergency settings, priority is given to the assessment of global functioning and risk in the initial triage procedure. An individual’s level of functioning at hospital admission can help clinicians devise a personalized treatment plan and estimate progression over time.
For the WHODAS-2 to be useful to mental health practitioners, it needs to reflect the functional outcome of mental disorders and to maintain adequate psychometric properties across different clinical settings. To our knowledge, the psychometric properties of the WHODAS-2 have not been evaluated in a psychiatric emergency context where rapid and efficient disability assessment is required. Further, there is limited research regarding disability profiles of mental disorders using WHODAS-2 scores. Most studies assessing disability in psychiatric populations with the WHODAS-2 have focused on specific psychopathologies, 25,27,32,33 and studies comparing scores across psychiatric disorders are limited by few diagnoses. 19,25 A recent study based on the 2012 Canadian Community Health Survey-Mental Health Component compared mean WHODAS-2 scores (12-item version) across several psychiatric diagnoses, 14 providing some of the most comprehensive findings to date on the disability profiles of mental disorders. However, personality disorders were not included in the study, and diagnostic data were collected retrospectively, assessing the relationship between present global functioning and past diagnoses rather than current disorders. Further studies comparing WHODAS-2 scores across psychiatric diagnoses are warranted to better understand disability profiles of different psychopathologies, to eventually provide a benchmark for clinicians to interpret WHODAS-2 scores in psychiatric populations, and to better assess whether WHODAS-2 scores adequately reflect the impact of mental disorders on functioning.
We address these knowledge gaps by describing and comparing WHODAS-2 (12-item version) scores across psychiatric diagnoses including anxiety disorders, mood disorders, psychotic disorders, personality disorders, and substance abuse in 1,125 patients admitted to psychiatric emergency. A second objective was to evaluate the psychometric properties of the WHODAS-2 in this same population by (a) measuring internal consistency and (b) establishing construct validity using confirmatory factor analysis (CFA).
Methods
Population
We used data from the Signature Bank of the Institut Universitaire en Santé Mentale de Montréal (IUSMM), a large biological, psychosocial and clinical databank of individuals continuously recruited since 2012 at the psychiatric emergency of the IUSMM.
Participants were men and women in the Montreal metropolitan region, presenting to psychiatric emergency. Individuals were approached for recruitment by nurses from the research team within 48 hours of admission, written informed consent was obtained, and the data collection was conducted. Self-report data were collected using an iPad application.
In total, 1,125 participants of the Signature Bank completed the WHODAS-2. Most patients were francophone (97.9%). All participants gave informed consent, and ethical approval was obtained from the research ethics committee of the Integrated Center for Health and Social Services of the East end of Montreal.
Psychiatric Diagnoses
Psychiatric diagnoses were established following clinical interviews conducted by the attending psychiatrist using the 10th revision of the International Classification of Diseases (ICD-10). Participant groups were created based on their primary diagnosis: anxiety disorders (corresponding to diagnoses F40 to F48 of the ICD-10; n = 106), mood disorders (F30 to F39; n = 362), psychotic disorders (F20 to F29; n = 434), personality disorders (F60 to F69; n = 119), substance abuse (F10 to F19; n = 86), and “other disorders” (n = 18). The “other disorders” category included various psychiatric diagnoses of the F section of the ICD-10, such as eating disorders, dementia, and self-harming behavior.
Instruments
WHODAS-2
The 12 item self-administrated version of the WHODAS-2 was used. This measure evaluates global functioning across six domains: mobility, occupational activities, cognition, participation, hygiene, and social life. Individuals rate the difficulties they experienced in the past 30 days for a number of activities using a Likert scale ranging from 0 to 4 (“none,” “mild,” “moderate,” “severe,” or “extreme”). Each domain is measured by two items, yielding six domain scores (range 0 to 8) and 1 general global functioning score (range 0 to 48). Higher scores indicate greater disability.
Adequate psychometric properties of the 12-item version of the WHODAS-2 have been reported. Good internal consistency has been demonstrated by significantly higher scores (P < 0.002) in participants with mental and physical disorders compared to the general population in an Australian sample of 8,841 individuals, 10 and by Cronbach alphas of 0.94 for the total score and of 0.74 to 0.90 for the six domains, in a sample of adults with Huntington’s disease.11 These studies also validate the WHODAS-2 two-level factorial structure comprising a general global functioning factor and six secondary factors corresponding to the six domains of functioning.
Statistical Analyses
Analyses were performed in R version 3.3.0. 34 Psych package 35 was used for reliability analyses and Lavaan package 36 for confirmatory factor analyses (CFA).
WHODAS-2 scores by psychiatric profile
Mean WHODAS-2 scores were compared across psychiatric groups (anxiety disorders, mood disorders, psychotic disorders, personality disorders, substance abuse, and other disorders) using analyses of variance. Post hoc comparisons were performed using Tukey correction for multiple comparisons.
Psychometric properties
Distribution of WHODAS-2 scores was examined. To evaluate internal consistency, Cronbach alpha coefficients 37 were calculated for each of the six WHODAS-2 domains and for the total score. Internal consistency was first tested for all participants and then by sex and primary psychiatric diagnosis. Construct validity was established using a two-level CFA, with first-level factors corresponding to the six WHODAS-2 domain subscales and a second level general factor. Multigroup analyses were conducted by sex to test for measurement invariance across sex.
Results
Descriptive Data
Sample characteristics and sex differences in prevalence of disorders are presented in Table 1. Mean age of participants was 40.4 years (SD = 14.1). The majority of participants were single (79.2%), did not have any postsecondary education (72.5%), and were unemployed at recruitment (68.5%). The psychotic and personality disorder groups had the highest rates of unemployment (80.3% and 70.3%), were the least likely to be married or in a relationship (11.3% and 14.3%), or to have achieved postsecondary education (21.8% and 20.2%) together with the substance abuse group (16.9%).
Sociodemographic Characteristics of the Sample.
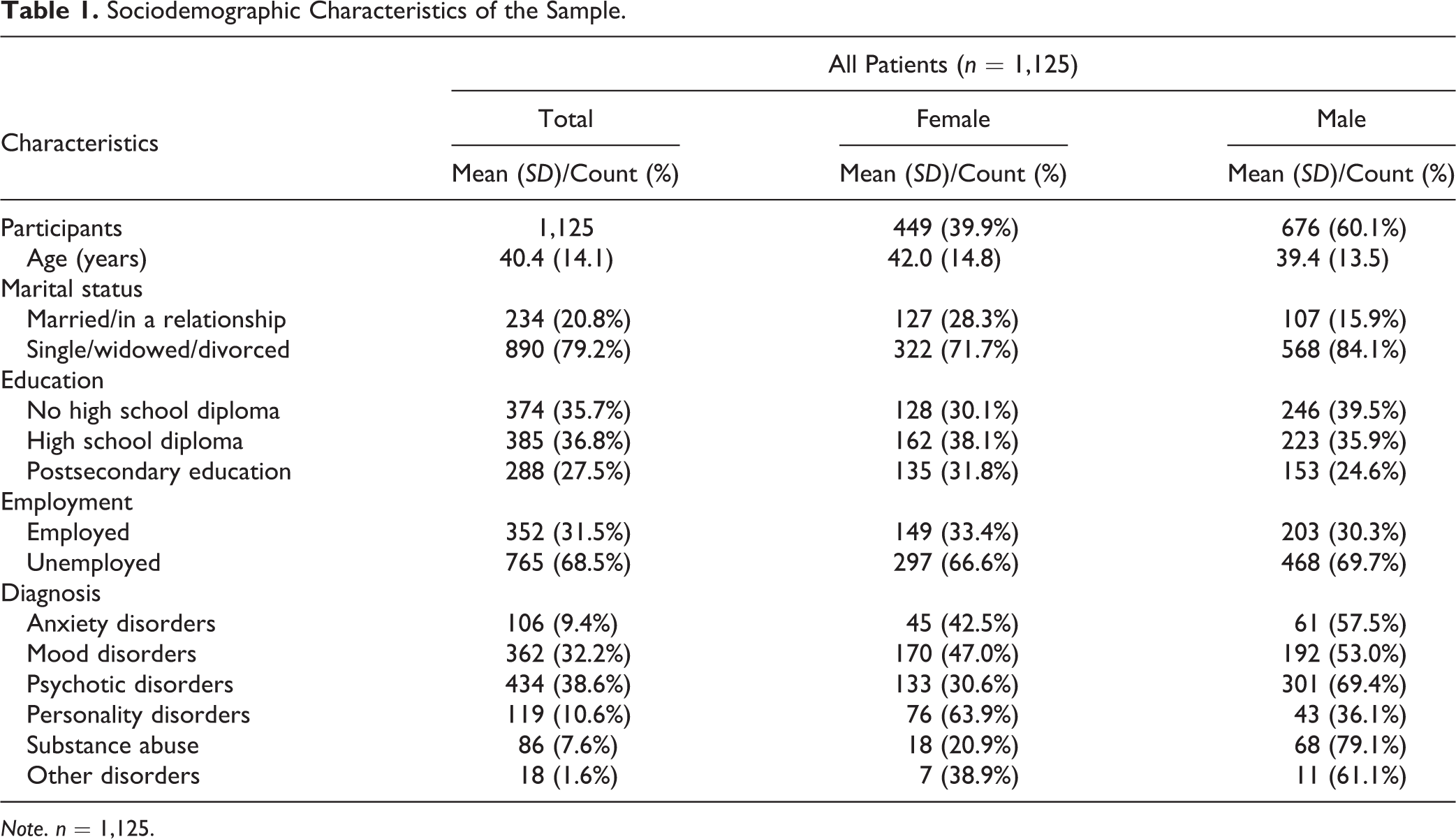
Note. n = 1,125.
WHODAS-2 by Psychiatric Profile
The mood disorders, anxiety disorders, and personality disorders groups had significantly higher mean WHODAS-2 scores than the substance abuse, psychotic disorders, and other disorders groups (P < 0.001). While there was no significant difference between mean scores of the mood, anxiety, and personality disorders groups, participants with personality disorders obtained the highest mean score. See Table 2 for WHODAS-2 scores by diagnosis.
Distribution of WHODAS-2 Scores and Diagnosis.
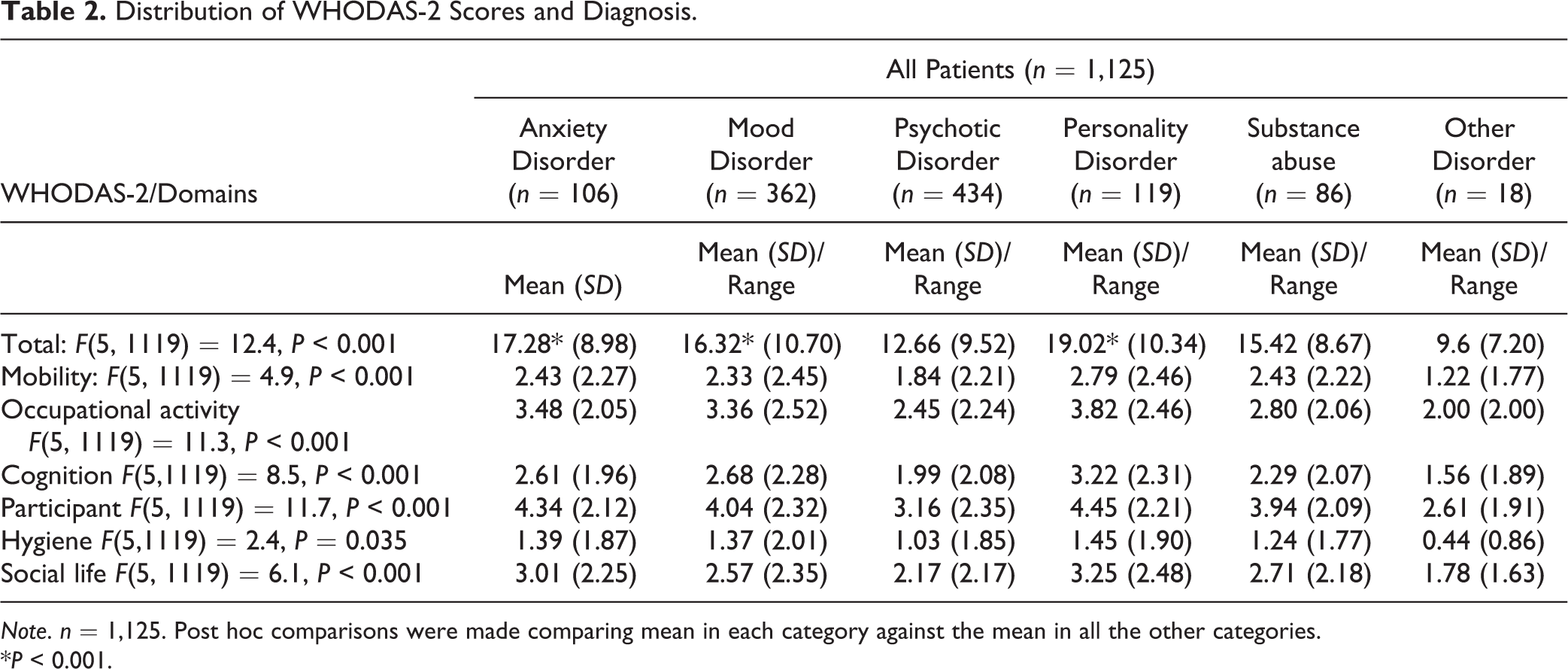
Note. n = 1,125. Post hoc comparisons were made comparing mean in each category against the mean in all the other categories.
*P < 0.001.
Psychometric Properties of WHODAS-2
The global WHODAS-2 mean was 15.11 (SD = 10.11). Ceiling effects were minimal, ranging from 0.2% to 6.3% for the different domains. The floor effect was most pronounced for hygiene scores reaching 61.4%, suggesting little disability in this domain. Cronbach alpha coefficients ranged from 0.59 to 0.85 across domain subscores and was 0.88 for the global WHODAS-2 score. See Table 3 for distribution of WHODAS-2 scores and reliability coefficients.
Distribution of WHODAS-2 Scores and Reliability Coefficients.
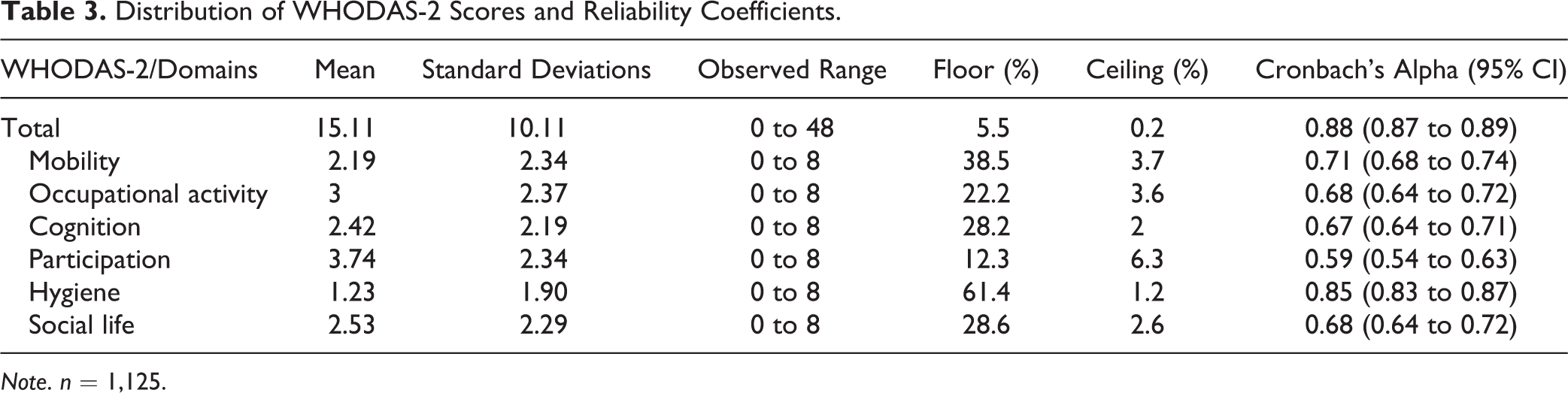
Note. n = 1,125.
Factor structure
CFA results presented acceptable goodness of fit indices (CFI was above 0.95 [0.956] and the upper part of the 90% confidence interval of the RMSEA was lower than 0.08), confirming that the two-level CFA fit the data well. When testing for metric invariance (equal loadings across sex), the scaled χ2 difference was not significant (χ2 = 16.926, df = 11, P = 0.11). However, when testing for scalar invariance (equal loadings and intercepts), the scaled χ2 difference was statistically significant (χ2 = 27.43, df = 5, P < 0.0001). Intercepts of the men were between 0.003 and 0.482 lower than intercepts of the women, suggesting that women reported higher disability scores for most items compared to men. CFA results are presented in Figure 1.
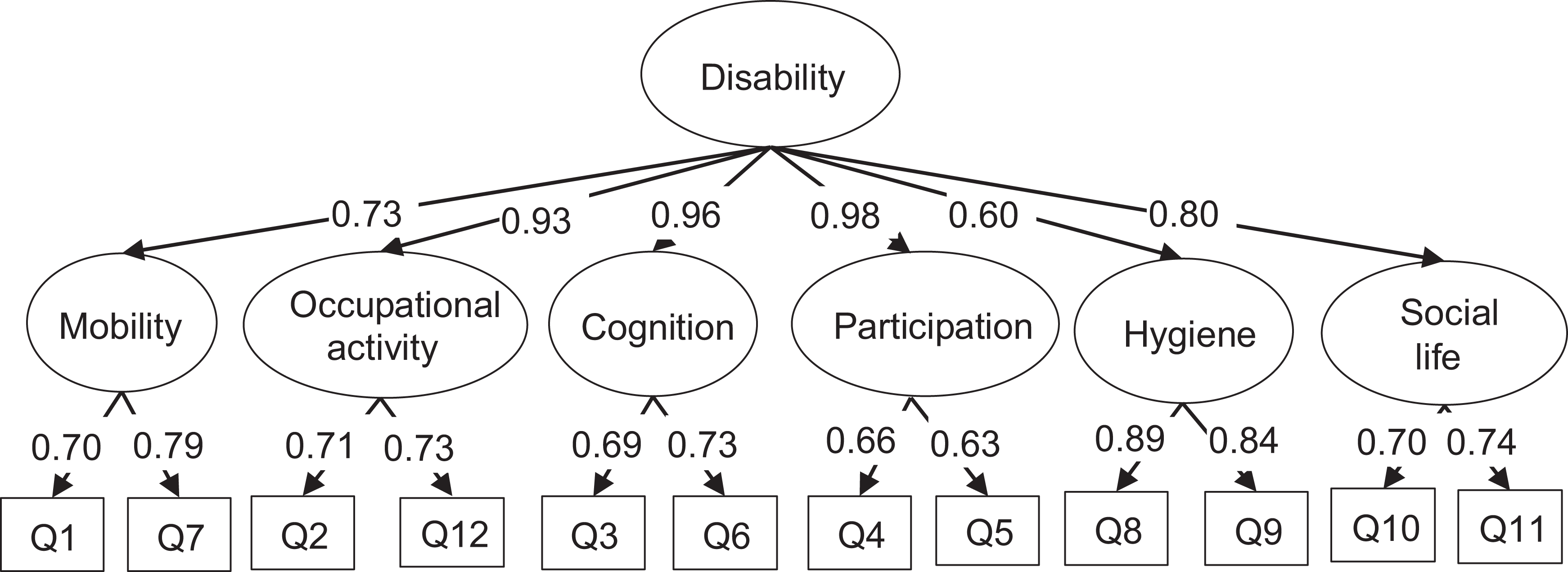
Factor structure of the WHODAS-2 and confirmatory factor analysis.
Discussion
In this large-scale study of adults admitted to psychiatric emergency, we described and compared WHODAS-2 scores (12-item version) across psychiatric diagnoses and assessed psychometric properties. To our knowledge, this constitutes the first large-scale investigation to evaluate the WHODAS-2 in a psychiatric emergency setting. It is important to verify that the WHODAS-2 remains valid in psychiatric emergency contexts where efficient disability assessment must be performed for those presenting with severe psychopathology and heightened emotional states.
WHODAS-2 Scores by Psychiatric Profile
Individuals with anxiety, mood, and personality disorders reported significantly higher mean WHODAS-2 scores (P < 0.001) indicating worse functional disability compared to those with other psychopathologies.
Increasing evidence indicates that anxiety and mood disorders are associated with more severe functional impairment than other mental disorders. 26,38 In one study, anxiety and mood disorders ranked seventh of the top 10 disorders with the greatest impact on work loss days as assessed by WHODAS-2. 39 Recent studies using the WHODAS-2 suggest that depression is associated with more severe disability than other disorders including bipolar disorders, generalized anxiety disorders, and schizophrenia. 14,19 While Sjonnesen et al. reported less impairment for depressed participants diagnosed in the past 12 months than for other psychiatric groups, depressed individuals diagnosed in the past month had a higher WHODAS-2 mean score than any other group. 14 This is consistent with work indicating that functional impairments follow depressive symptomatology and subside as symptoms improve. 40
In our study, participants with personality disorders obtained the highest WHODAS-2 score although scores did not significantly differ from participants with anxiety and mood disorders. This is consistent with studies indicating more severe impairment in individuals with personality disorders. Adults suffering from comorbid axis I and II disorders tend to exhibit more impaired functioning than those with a single axis I disorder, 41 –43 and personality disorders have been associated with poorer quality of life and worse functional impairments than axis I disorders in individuals with no comorbid psychopathologies. 44 Schizotypal and borderline personality disorders have been associated with more severe impairments than major depressive disorder 30 although we were unable to examine functioning associated with specific personality disorders in our study.
Individuals recruited in a psychiatric emergency setting are likely to demonstrate more severe functional impairment than those recruited in non-emergency contexts given the heightened symptomatology experienced during a crisis. Our results support this hypothesis. Compared to previously reported WHODAS-2 scores for depressive disorder (mean score = 27.14/100 17 ) and bipolar disorder (mean score = 19.23/100 for subsyndromic patients and mean score = 12.69/100 for asymptomatic patients in a euthymic phase 27 ), our mood disorders score (mean score = 34/100; Table 2 mood disorders score rescaled on 100) falls at the higher end of the spectrum. Similarly, our study’s mood disorders group scored significantly higher than Sjonnesen et al.’s depression group (diagnosed in the past month; P < 0.0001) suggesting more severe disability within a psychiatric emergency context. 14 Furthermore, the anxiety disorders, mood disorders, and substance abuse groups all reported significantly more functional impairment than participants in the Sjonnesen et al.’s depression (past 12 months), general anxiety disorders, and bipolar disorders groups (P < 0.0001). 14 While these findings indicate that psychiatric emergency patients suffer more severe functional impairment than their non-emergency counterparts, results should be interpreted with caution given heterogeneity between studies and lack of sufficient comparative data.
Surprisingly, in our study, the psychotic disorders group did not score significantly higher than other groups nor did they exhibit more severe functional impairment than non-emergency patients with similar diagnoses in the literature. Psychosocial impairment is considered a core feature of psychotic disorders. 45 Individuals diagnosed with schizophrenia have difficulties with basic social roles, interpersonal relationships, and occupational activities, 46 and neurocognitive deficits are thought to be predictive of these impairments. 47 Schizophrenia has been associated with worse disability than bipolar disorder, 47,48 depression, 49 schizoaffective disorders, 49,50 anxiety disorders, substance abuse, and eating disorders. 38 Sjonnesen et al. also reported more severe disability associated with schizophrenia than depression (in the past 12 months, but not in the past month), generalized anxiety, and bipolar disorders. 14 In our study, those with psychotic disorders did not score higher than most other groups nor did they significantly differ from Sjonnesen et al.’s schizophrenia group (P = 0.56), 14 suggesting similar levels of impairment reported by emergency and non-emergency psychotic patients. A few explanations may account for these results. Individuals with psychotic disorders often experience a chronic course of illness where social and occupational impairments become more permanent states. 51 Thus, they may develop decreased awareness of their deficits and may underreport them. Reciprocally, previous studies suggest that individuals with depression experience increased awareness of their deficits and exaggerate their self-report. 52 The combination of these perceptual biases may explain why our mood disorders group is more functionally impaired than our psychotic disorders group. It is also possible that the WHODAS-2 items regarding occupational activities may not capture the long-term disability experienced by those with psychotic disorders since respondents evaluate difficulties over the past 30 days. Finally, psychotic patients admitted to emergency likely differ from their non-emergency counterparts on their level of insight. Participants in Sjonnesen et al.’s study may have greater insight since they self-reported their diagnoses, 14 while psychotic patients recruited in an emergency setting may have reduced insight and may have been admitted to the hospital by a third party. Previous studies report problems with self-reports of functioning in schizophrenia due to lack of insight, 53 and it has been suggested that the WHODAS-2 should be used alongside a clinician-rated measure for patients with psychotic disorders. 18
Psychometric Properties of WHODAS-2
This study confirms that the WHODAS-2 12-item version demonstrates good psychometric properties among psychiatric patients in an emergency context. Acceptable goodness of fit indices in a two-level CFA confirms the structure of the WHODAS-2 in six domains. The instrument presents high reliability for the global score and moderate to high reliability across domain subscores. Previous studies in individuals with physical and mental disorders have consistently supported good reliability of the 12- and 36-item versions of the WHODAS-2. 4,11,17,18,20,25,32 The reliability coefficients of the 12-item scale were previously found to be lower for the domain subscores than for the global score, likely explained by the few items per domain. 11
Consistent with previous literature, we found minimal ceiling effects, but floor effects were present in most domains suggesting that the 12-item scale may not differentiate among low levels of disability. 4,19 One may have anticipated higher disability scores in the cognitive and hygiene domains for the psychotic disorders group since those with schizophrenia often suffer from neurocognitive deficits and difficulties with basic life skills, 47,54 and self-care impairments tend to be associated with the most severe cases of mental illness. 13,19,27 However, in line with previous findings, we observed floor effects for hygiene, suggesting that this domain is largely reported to be unaffected in many individuals suffering from mental disorders. 4,19
Findings from our CFA are consistent with previous studies supporting the six-domain structure of the WHODAS-2 in both the 12-item and 36-item versions. 4,11,55 –57 Six first-order factors were found to best fit the data and to be most representative of the scale’s factorial structure. Our findings support the validity of the instrument’s theoretical framework 4 ; notably, the ICF’s biopsychosocial model of disability characterized by the interconnectedness of mental and physical health. The WHODAS-2’s robust construct validity may partly explain why a general measure of disability seems to align with the needs of mental health services.
Limitations of the Study
Our study did not include a control group representative of the general community. Based on normative data for the 12-item WHODAS-2 scale, however, all of our psychiatric groups except for the “other disorders” group scored in the top 10% of the population distribution of WHODAS-2 scores, suggesting clinically significant disability. 10 Further, all groups scored significantly higher on the WHODAS-2 than the community sample reported in the Sjonnesen et al. study (P < 0.0001). 14 Also, the specificity of our results is limited by the presence of comorbid disorders in psychiatric populations. Individuals with one mental disorder have increased odds of meeting the criteria of another disorder, and patients can sometimes be diagnosed with three or more psychopathologies. 58 Finally, our sample may not be entirely representative of all patients admitted to psychiatric emergency since it is likely that some of the most severely impaired individuals may have been unfit to participate.
Conclusion
Our findings could assist clinicians in interpreting WHODAS-2 scores in psychiatric populations and provide a more detailed portrait of disability profiles associated with common mental disorders. Findings may be particularly relevant for those working with more severe cases and at more acute stages of illness. Based on comparisons with previously reported normative data for the general population, the 12-item WHODAS-2 scale appears sensitive to functional disability associated with mental disorders, and psychometric properties remain adequate for use in psychiatric emergency settings. With its brief format and sensitivity to change in various psychopathologies, the 12-item WHODAS-2 offers promising clinical implications for the assessment of disability in urgent care. For those with psychotic disorders, given the potential self-report difficulties associated with reduced insight, global functioning would be likely best evaluated using a combination of the WHODAS-2 and other tools.
Footnotes
Acknowledgments
The authors thank the Signature Consortium of the IUSMM for making the Signature Bank data available to researchers and the psychiatric emergency patients of the IUSMM for participating in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Signature Bank is supported by a donation from Bell Canada Enterprises to the Foundation of the IUSMM and by a research grant from the Fonds de Recherche du Québec-Santé (FRQ-S). The Research Center of the IUSMM is supported by a grant from the FRQ-S. This study was supported by the IUSMM project. A.H. holds a doctoral award and C.M.H a salary award from the FRQ-S.