
Abstract
Objective:
The potential metabolic adverse effects of second-generation antipsychotics (SGA) need to be monitored. The Canadian Alliance for Monitoring Effectiveness and Safety of Antipsychotics (CAMESA) offers guidelines for this purpose. We aimed to evaluate the long-term rates of youths receiving monitoring in mental health clinics and document the factors that may influence them.
Method:
The charts of 180 patients (13.3 ± 3.1 years, 54.4% males) receiving SGA treatment for the first time between January 2016 and June 2018 were reviewed. Monitoring was divided into baseline and 1- to 6-month and 9- to 24-month periods. Population under study was stratified into children (4 to 12 years) and adolescents (13 to 18 years). Sociodemographic characteristics, psychiatric diagnosis and comorbidities, prescribed SGAs and comedications, anthropometric measures (AM), blood pressure (BP), blood tests (BT), electrocardiogram, and the psychiatrist’s years of practice were collected. Cross tables were used to present the monitoring rates. Categories were compared by covariate analysis. Rates of patients monitored across categories were compared using Fisher exact test.
Results:
Monitoring rates for AM, BT, and BP were 55%, 47.8%, and 46.7% at baseline; 50%, 41.7%, and 45.2% at 1 to 6 months; and 47.2%, 41.5%, and 40.6% at 9 to 24 months, respectively. Higher monitoring rates were significantly associated with adolescent status (baseline, 1 to 6 months), a diagnosis of psychotic and/or affective disorder (baseline, 1 to 6 months, 9 to 24 months), having ≤1 psychiatric comorbidities (1 to 6 months), high SGA dose (baseline, 1 to 6 months), and clinician’s experience (baseline, 9 to 24 months). Significantly lower monitoring rates were associated with the psychostimulant/atomoxetine comedication (baseline, 1 to 6 months, 9 to 24 months).
Conclusion:
Five years after publication of the CAMESA guidelines, metabolic monitoring is conducted for less than half of patients. In our sample, age, diagnostic category, psychiatric comorbidities, SGA dose, clinician’s experience, and comedications influenced the monitoring rates. Major progress still needs to be made before reaching a satisfactory level of monitoring.
Background
Antipsychotic (AP) use has increased dramatically in the pediatric population over the past 20 years worldwide. 1 In Canada, there was a 114% increase in AP prescriptions from 2005 to 2009 and a 33% increase from 2010 to 2013, 2 followed by a 10% decrease between 2010 and 2016. 3 Increased prescription has been associated with a higher frequency and longer duration of their use, 4,5 Canadian boys are far more likely than girls to receive second-generation antipsychotic (SGA) prescriptions and at a younger age. 4,6,7
Only aripiprazole is approved in the Canadian pediatric population for the treatment of schizophrenia in adolescents aged 15 to 17 years and lurasidone for bipolar disorder in 13- to 17-year-olds for manic or mixed episodes and depressive episodes. 8 However, SGAs are commonly used to treat multiple nonschizophrenic conditions in youths 9 : disruptive behavior associated with autism spectrum disorder (ASD), attention deficit hyperactivity disorder (ADHD), conduct disorders, tics, anxiety, depression, and anorexia nervosa 3,10 –13
Consequently, there has been increased concern about the risk–benefit profile of these medications, specifically for minors. 2 Olanzapine and clozapine carry a high risk, quetiapine and risperidone a moderate risk, and aripiprazole and ziprasidone a low but non-negligible risk. 4,14 –20 Metabolic adverse effects (AEs), including weight gain, dyslipidemia, hyperglycemia, type 2 diabetes, and metabolic syndrome, may be more pronounced in the pediatric than in the adult population. 21 Metabolic disturbances in childhood and adolescence are well established risk factors for further cardiovascular morbidity and mortality in adulthood. 21 –23 The metabolic risks observed in mental illness are also greater than in the general population. 24 –27
The United Kingdom, Canada, Australia, Belgium, and the United States 28 –32 have developed specific guidelines for the screening, monitoring, and management of metabolic complications. The Canadian Alliance for Monitoring Effectiveness and Safety of Antipsychotics in Children (CAMESA) has published specific guidelines to prevent, detect, and manage AEs of SGA use in the pediatric population. Monitoring recommendations include physical health and neurological examinations, assessment of anthropometric measures (AM; height, weight, body mass index [BMI], and waist size), blood pressure (BP), and blood tests (BT) (fasting plasma glucose, insulin, cholesterol, triglyceride, liver enzyme, amylase, prolactin, and thyroid-stimulating hormone [TSH] levels) at baseline and at 1-, 2-, 3-, 6-, 9-, and 12-month follow-up. 31 Beyond 12 months, monitoring recommendations are solely based on expert clinical opinion due to the absence of long-term studies. 31 Despite these recommendations, there are large gaps between what is prescribed and the quality of monitoring in clinical practice, 33 –36 especially in outpatient settings. 37 –40
There is limited research on long-term metabolic monitoring, although SGAs are increasingly prescribed for longer durations, 4,5 with adverse metabolic complications continuing to mount over time. 41 –46
The factors associated with assessing monitoring have not been robustly evaluated. Published studies have encompassed only short-term (6 to 12 months or less) follow-up and have reported limited and conflicting conclusions related to methodological limitations. 40,47 –50 A recent 12-month retrospective Canadian study exploring which patient, treatment, and health care utilization variables were associated with adherence to CAMESA metabolic guidelines in SGA-treated children and adolescents only highlighted factors associated with baseline monitoring. 39 Additional research over a longer period of follow-up is clearly needed. We aimed to evaluate the rates of metabolic monitoring in children and adolescents receiving SGA for the first time in mental health outpatient clinics for up to 24 months of treatment and document the factors that may influence them.
Methods
Study Design and Participants
Retrospective electronic records of 180 youths receiving care in outpatient psychiatric clinics at the Rivière-des-Prairies Mental Health Hospital, CIUSSS-NIM (Integrated University Health and Social Services Centers of North of Montreal Island), a child and adolescent mental health hospital in Montreal, during the study period of January 2016 to June 2018 were reviewed. To be included in the study, patients had to be 4 to 18 years old, treated with a SGA during the study period, and SGA-naive prior to the SGA prescription. “SGA-naive” was defined as having no SGA listed in the medical history before their baseline visit. Patients with diagnosed diabetes or dyslipidemia prior to SGA treatment were excluded in order to limit the confounding factors that could influence metabolic monitoring rates. 51 –53 Study procedures were approved by the CHU Sainte-Justine and CIUSSS-NIM ethics and research committees (MP-21-2016-1201). This retrospective study using data recorded in the medical charts was conducted with the approval of Director of Professional Services of CIUSSS-NIM. Participants were not required to give informed consent.
Data Collection/Assessments
Data on demographic characteristics (age and sex), psychiatric diagnosis and comorbidities (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition), prescribed SGAs type (immediate-release or extended-release formulations were grouped together), dose, AM, BP, BT, electrocardiogram (ECG), and the psychiatrist’s years of practice were collected. Monitoring was divided into baseline and 1- to 6-month and 9- to 24-month periods. The main diagnoses were grouped into: “psychotic and/or affective disorders” (psychotic, bipolar, depressive, and adaptation disorders), “neurodevelopmental disorders” (ASD, ADHD, tics/Tourette syndrome, and oppositional defiant disorder), and “personality, anxiety, and other disorders” (personality disorders, anxiety disorders, obsessive-compulsive disorder, post-traumatic stress disorder, and intermittent explosive disorder). Psychiatric comorbidities (behavioral problems, emotional dysregulation, insomnia, anxiety, tics, obsessive-compulsive, ADHD, and depressive symptoms) were separated between “0 to 1” and “2 to 4.” Clinicians’ experience was separated between <12 years and ≥12 years, as there is a clear gap at 12 years of experience in the physician population, in order to create more homogenous groups.
SGAs doses were converted in chlorpromazine dose equivalents. 54 For each subject, mean SGA dose during follow-up was calculated. SGA dose categories were based on the percentiles of distribution of the participants.
Comedication was regrouped by its possible effect on appetite/weight (anorexigenic [psychostimulants/atomoxetine], 55,56 neutral/orexigenic [α-2a-agonists/antidepressants/mood stabilizers], 56 –58 and absent) and by number of comedications prescribed (0, 1, and ≥2).
Based on the CAMESA guidelines, 31 AM (height, weight, and waist size), BT (glucose, insulin, lipids, prolactin, and TSH), BP, and ECG assessed at each time period were documented. Monitoring was considered to be complete if at least one assessment of AM, BT, BP, or ECG was reported within the defined monitoring periods.
Statistical Analysis
The study population was stratified into children (4 to 12 years) versus adolescents (13 to 18 years); main diagnostic categories (psychotic and/or affective disorders, neurodevelopmental disorders, and personality, anxiety, and other disorders); psychiatrist’s number of years in practice (<12 years and ≥12 years); SGA type (quetiapine, risperidone, aripiprazole, and others); SGA dose (low [<42 mg], medium [42-109 mg], and high [≥109 mg]); comedications ([anorexigenic, 55,56 neutral/orexigenic, 56 –58 and absent) and number of comedications prescribed [0, 1, and ≥ 2]); and psychiatric comorbidities (0 to 1 and 2 to 4). Monitoring rates were calculated for AM, BT, BP, and ECG at baseline and 1- to 6-month and 9- to 24-month periods. The sample characteristics are presented as the means and standard deviations for continuous variables, and frequencies and percentages for categorical variables (participant demographics, diagnosis, and treatment parameters).
Categories were compared by covariate analysis for age, main diagnosis, the number of psychiatric comorbidities, psychiatrist’ number of years in practice, SGA type, SGA dose, and comedications. Monitoring rates and the link with their covariates were ordered in cross tables. Fisher exact test was used to compare the rate of patients monitored across categories. To compare the monitoring rates across time periods, generalized linear mixed models was used. Target variables had a binomial distribution and were linearly related to the time effect with a logit link function. An unstructured covariance was used to take into account that repeated measurements are correlated. The significance level was set at a P value < 0.05. All statistical analysis was performed using SPSS, version 25.
Results
Participant Demographic and Treatment Variables
In total, 67.8% of the participants were adolescents and 54.4% were male. The most frequent diagnostic category was “neurodevelopmental disorders” (48.9%), followed by “psychotic and/or affective disorders” (26.1%), and “personality, anxiety and other disorders” (25%). Physicians’ experience ranged between 3 and 43 years (mean 10 ± 6 years); 63.9% of the participants were followed by psychiatrists with ≤9 years of practice, 20.6% by psychiatrists with 12 years of practice, and 15.6% by psychiatrists with ≥20 years of practice. Percentages of the participants by SGA type, SGA dose, and comedication categories are presented in Table 1.
Demographic, Treatment, and Clinical Characteristics of Participants.
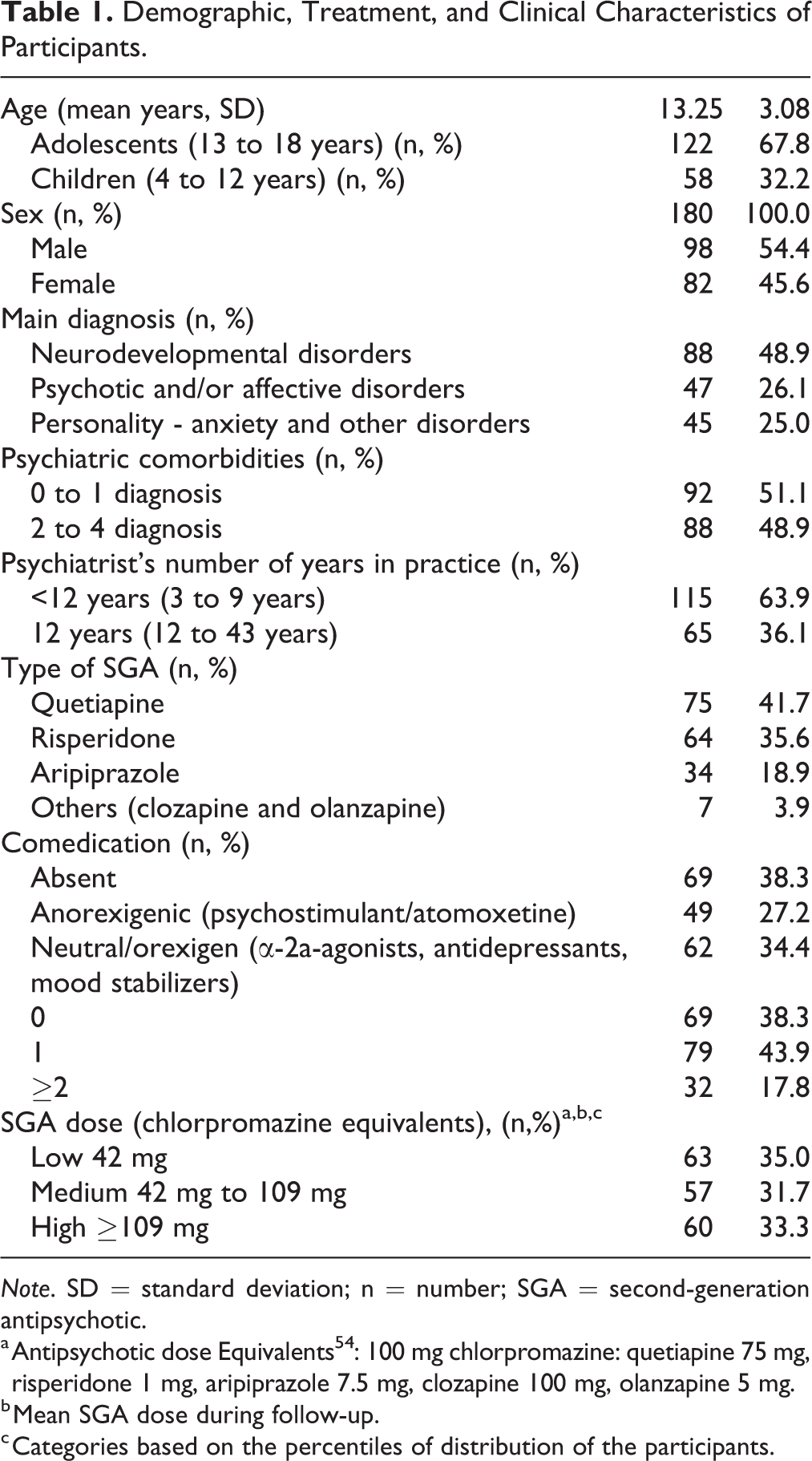
Note. SD = standard deviation; n = number; SGA = second-generation antipsychotic.
a Antipsychotic dose Equivalents 54 : 100 mg chlorpromazine: quetiapine 75 mg, risperidone 1 mg, aripiprazole 7.5 mg, clozapine 100 mg, olanzapine 5 mg.
b Mean SGA dose during follow-up.
c Categories based on the percentiles of distribution of the participants.
Follow-up of Monitoring Rates
In total, 128 (77.1%) patients benefitted from an SGA follow-up for at least 6 months and 81 (45%) were followed up for more than 12 months. The mean duration of SGA follow-up was 9.44 ± 6.94 months, without a significant difference between children and adolescents (9.74 ± 7.45 vs. 9.30 ± 6.71 months; Figure 1). Monitoring rates showed that only around half of the patients were monitored, from baseline to 1 to 6 months and 9 to 24 months for AM (55%, 50%, and 47.2% respectively), BT (47.8%, 41.7%, and 41.5%, respectively), and BP (46.7%, 45.2%, and 40.6%, respectively; Figure 2A to C). ECG monitoring rates were considerably lower (Figure 2D). None of the generalized linear mixed models reached statistical significance for the time effect.
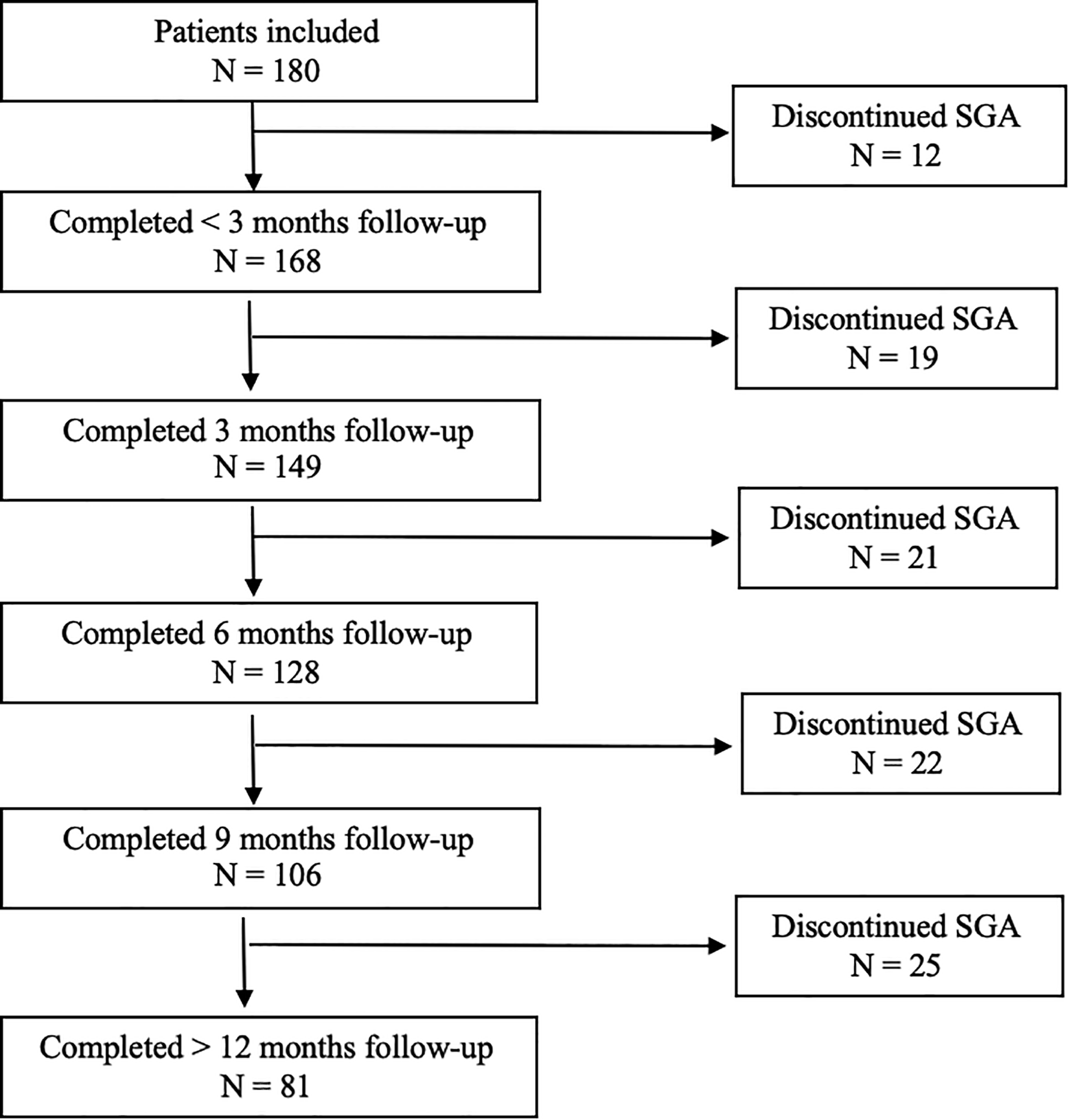
Duration of SGA follow-up. N = number of patients; SGA, second-generation antipsychotics.
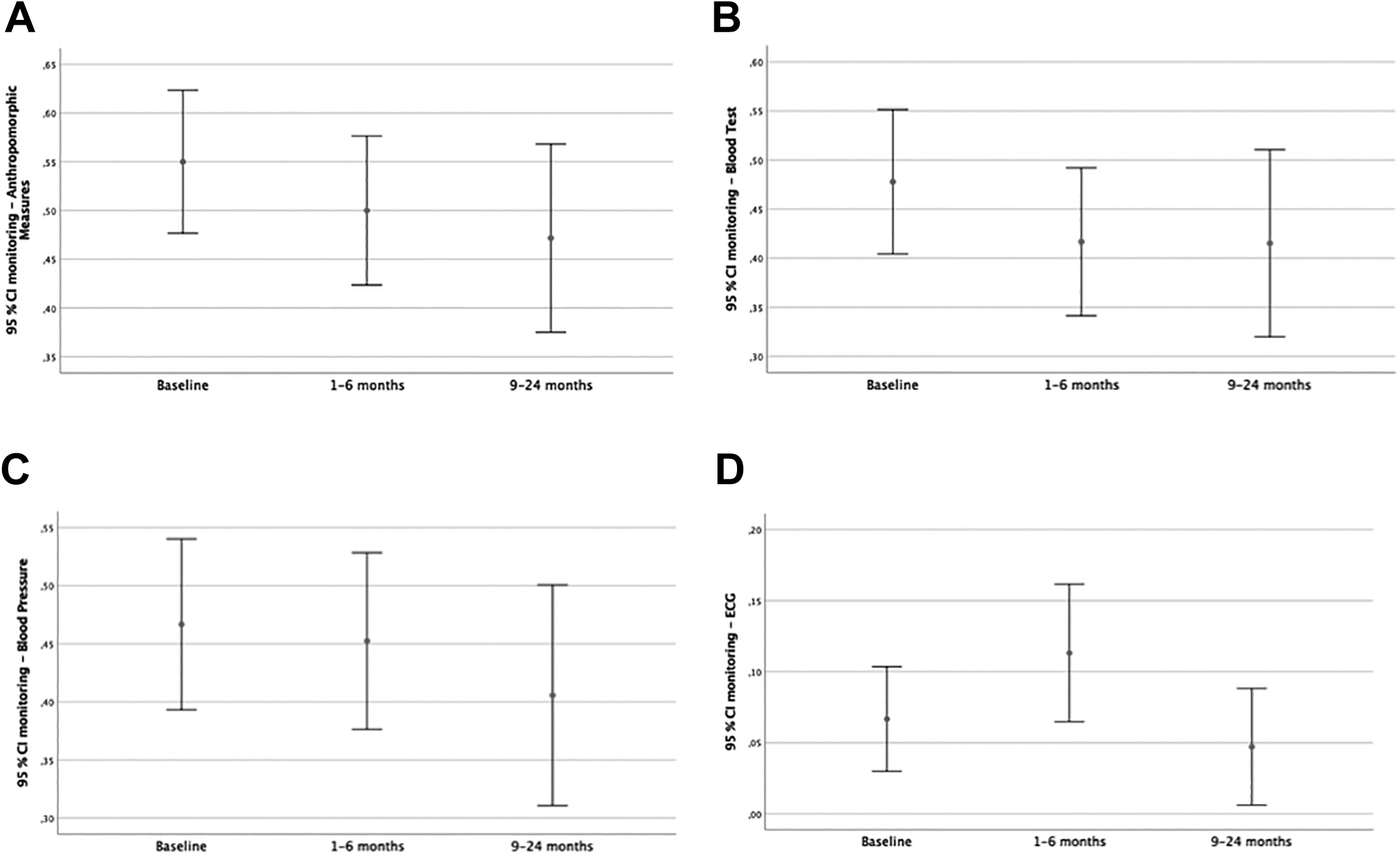
Metabolic monitoring rates during follow-up. A, Monitoring rate for anthropometric measures. B, Monitoring rate for blood tests. C, Monitoring rate for blood pressure. D, Monitoring rate for electrocardiogram (ECG).
Very low monitoring rates were observed for waist size and insulin (Table 2).
Metabolic Rates Stratified by Metabolic Parameters (AM and BT) During Follow-up.
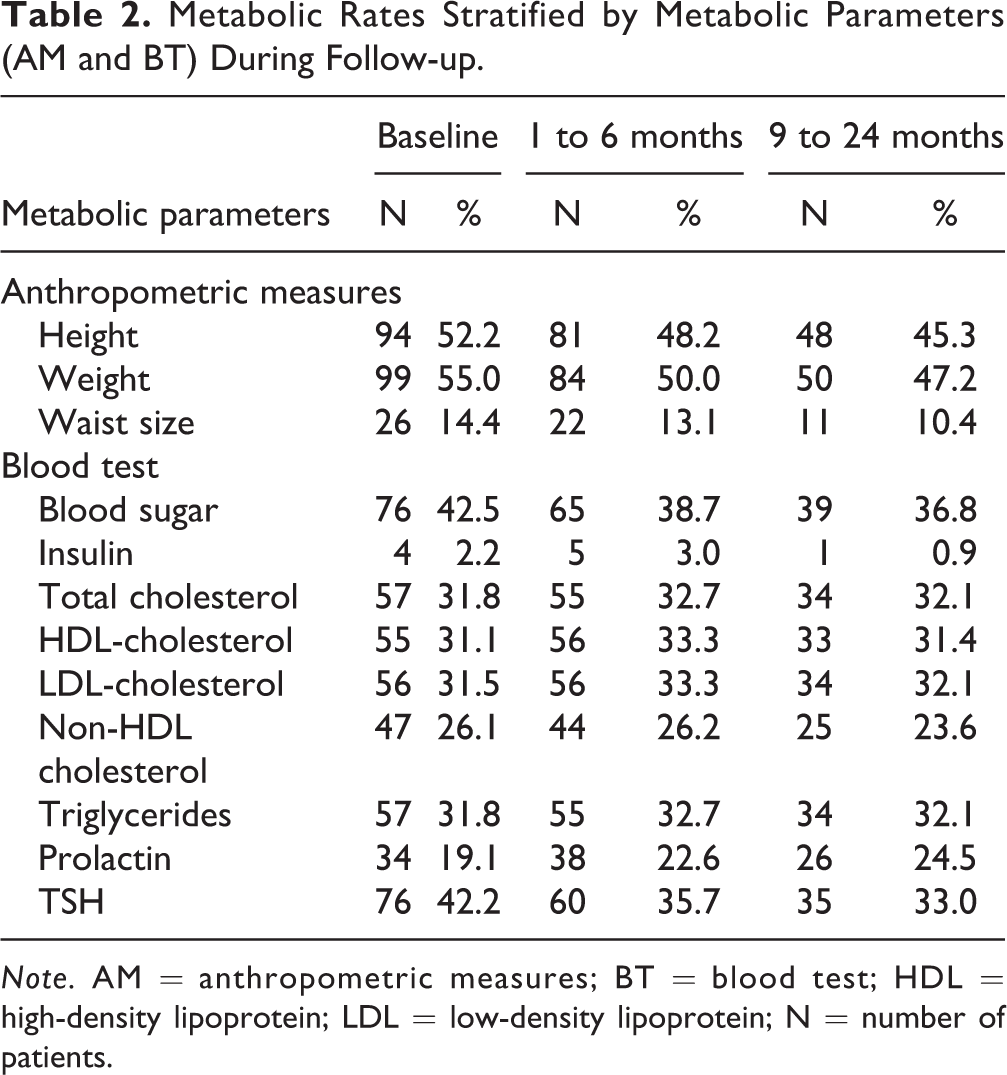
Note. AM = anthropometric measures; BT = blood test; HDL = high-density lipoprotein; LDL = low-density lipoprotein; N = number of patients.
Factors Influencing Monitoring Rates
Age
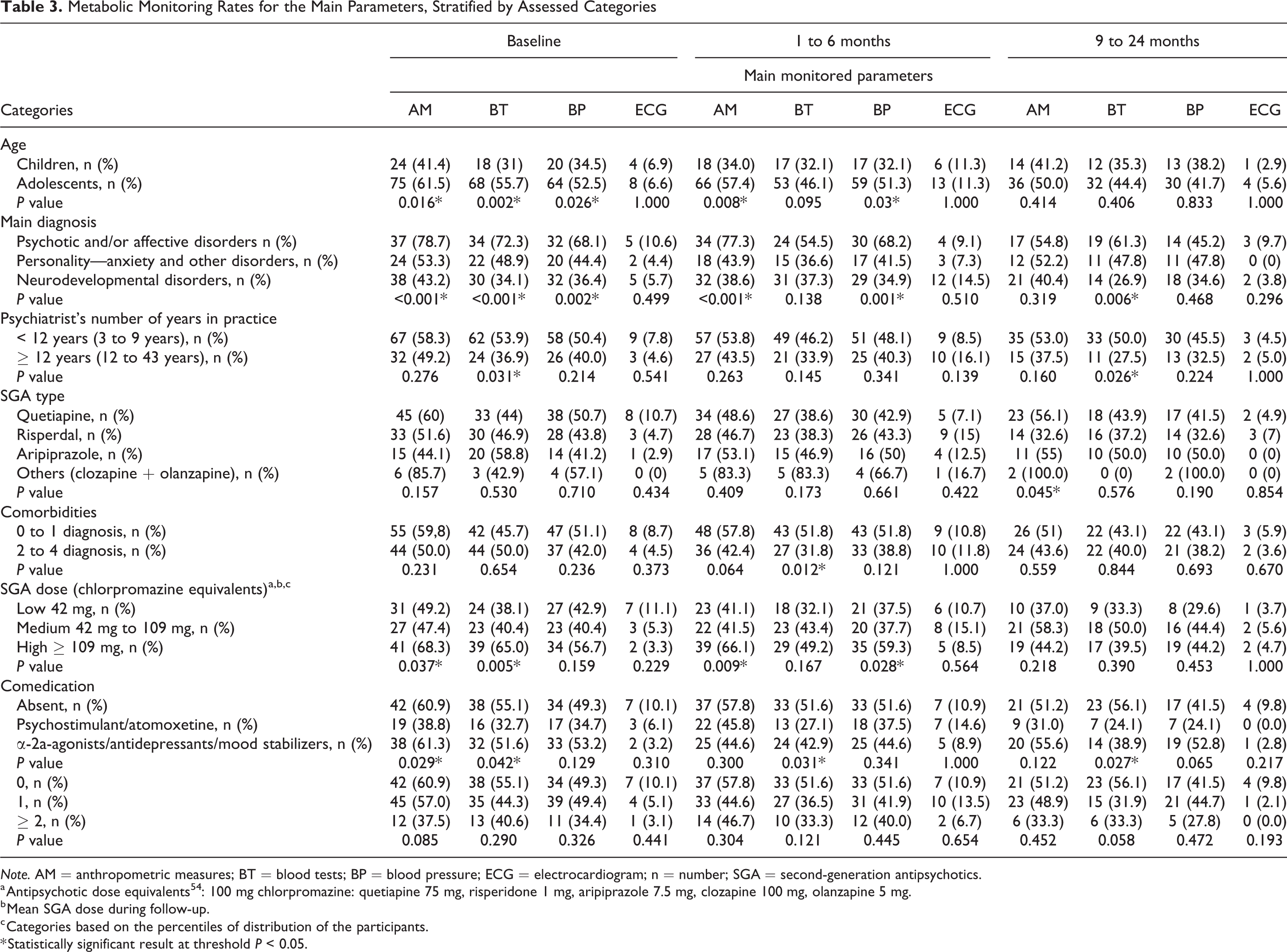
Stratification of the rates by compared categories showed significant differences between monitoring rates in children and adolescents at baseline for AM (P = 0.016), BT (P = 0.002), and BP (P = 0.026); 1 to 6 months for AM (P = 0.008) and BP (P = 0.03; Table 3).
Metabolic Monitoring Rates for the Main Parameters, Stratified by Assessed Categories
Note. AM = anthropometric measures; BT = blood tests; BP = blood pressure; ECG = electrocardiogram; n = number; SGA = second-generation antipsychotics.
a Antipsychotic dose equivalents 54 : 100 mg chlorpromazine: quetiapine 75 mg, risperidone 1 mg, aripiprazole 7.5 mg, clozapine 100 mg, olanzapine 5 mg.
b Mean SGA dose during follow-up.
c Categories based on the percentiles of distribution of the participants.
* Statistically significant result at threshold P < 0.05.
Diagnostic category
Monitoring rates were significantly higher for the “psychotic and/or affective disorder” category versus “personality, anxiety, and other disorders” versus “neurodevelopmental disorders” at baseline for AM (P < 0.001), BT (P < 0.001) and BP (P = 0.002); 1 to 6 months for AM (P < 0.001) and BP (P = 0.001); and 9 to 24 months for BT (P = 0.006; Table 3). Separate analysis of the disorder categories for each age range showed the higher rate of monitoring for “psychotic and/or affective disorders” to be maintained for both age groups.
Number of psychiatric comorbidities
The BT monitoring rate at 1 to 6 months was higher for patients with 0 to 1 than those with 2 to 4 comorbidities (P = 0.012; Table 3).
Clinician’s experience
Fewer years of professional experience was associated with a higher BT monitoring rate at baseline and 9 to 24 months for the participants followed by psychiatrists with <12 years in practice versus those with ≥12 years in practice (P = 0.031; Table 3).
SGA type
The AM monitoring rate at 9 to 24 months was higher for patients treated with clozapine/olanzapine versus aripiprazole, risperidone, or quetiapine (P = 0.045; Table 3). However, the very small size of the clozapine/olanzapine group limits the clinical significance.
SGA dose
Monitoring rates were significantly higher for the high dose than for medium or low dose categories at baseline for AM (P = 0.037) and BT (P = 0.005); 1 to 6 months for AM (P = 0.009) and BP (P = 0.028; Table 3). Doses of SGAs were significantly higher in the “psychotic and/or affective disorders” that those in the “neurodevelopmental disorders” or “personality, anxiety, and other disorders” (66%, 25.0%, and 15.6%, respectively, P < 0.001). Separate analysis of the disorder categories for each SGA dose range showed the higher rate of monitoring for “psychotic and/or affective disorders” to be maintained.
Comedications
Significantly lower monitoring rates were associated with the anorexigenic (psychostimulants/atomoxetine) comedication compared to neutral/orexigenic (α-2a-agonists/antidepressants/mood stabilizers) or absent comedication categories at baseline for AM (P = 0.029) and BT (P = 0.042); 1 to 6 months for BT (P = 0.031); and 9 to 24 months for BT (P = 0.027). Number of comedication categories were not significantly associated with the monitoring rates (Table 3).
Discussion
This retrospective study document long-term metabolic monitoring of children and adolescents treated for the first time with an SGA in outpatient psychiatric clinics as well as factors associated with the monitoring rates over 2 years of follow-up. Five years after publication of the CAMESA guidelines, metabolic monitoring was being conducted for less than half of patients, with no significant decrease over time. The age, diagnosis, psychiatric comorbidity, SGA dose, comedications, and clinician’s experience categories influenced monitoring rates.
Comparison of Our Sample with Those of Other Studies
More adolescents than children and a greater proportion of males than females were treated with an SGA, as reported by other authors. 7,10,34,37,39,59 Additionally, 48.9% of the SGA-treated patients in our sample fell under the “neurodevelopmental disorders” category, which is more represented by males. 59 Quetiapine was the most prescribed SGA (41.7%), in accordance with the results of a recent population-based Canadian adult and pediatric study, 60 whereas risperidone predominates in pediatric studies. 2,39,40 This could reflect preferential utilization of quetiapine to treat impulsivity, sleep problems, dysphoria, and anxiety associated with personality, affective, and anxiety disorders, as well as psychotic and affective disorders. The preference for quetiapine may also be due to the psychiatrist’s perception that this molecule presents a more favorable metabolic AE profile than risperidone, olanzapine, and clozapine, especially when prescribed at a lower dosage. 15,20 However, the reported metabolic risk profiles of quetiapine and risperidone are generally similar in the pediatric population. 4,14 –19,61
Monitoring Follow-up
Previous short-term studies reported low monitoring rates for several parameters, 34,38,39,47,50,62 –64 which decreased over 12 months. 34,38 This contrasts with our sample, where monitoring rates did not decrease significantly over 9 to 24 months. Although the metabolic AEs appear from the first months of AP exposure, 65,66 their effects persist over time 41 –45 and can result in enduring complications, justifying extended monitoring. 15,22 Our findings reveal better monitoring rates from baseline up to 9 to 24 months of SGA treatment than reported in previous pediatric Canadian studies conducted before 38 and even after 12,39 the implementation of the CAMESA guidelines. This could be explained by an increased awareness of psychiatrists, mental health nurse practitioners, and patients of SGA AEs following publication of these guidelines. 3,38,64 On the other hand, adult studies report superior monitoring rates, with only one-third of patients not receiving metabolic screening. 67 Monitoring rates for waist size and insulin were also low in our sample.
What Is Less Monitored?
Waist circumference monitoring was absent for almost 90% of patients. Other AMs were the best documented of the recommended tests, (see also the studies of Nolt et al., 37 Ronsley et al., 38 and Coughlin et al. 39 ). The discrepancy between monitoring rates of AMs could reflect inadequate medical/nursing habits or the lack of sufficient time for medical/nursing staff or clinical coordination and resources, as well as limited patient engagement/collaboration with these procedures 68 or interpretation issues. Waist circumference percentile curves are available for Canadian youth between 6 and 18 years of age, 69 but measure interpretation is confronted to unstable consistency and ethnic variations. 70 The very low assessment of waist circumference is a significant concern, as SGA-treated youths have a significantly increased long-term risk of developing metabolic syndrome. 26 Furthermore, a waist circumference measurement in the 90th percentile or higher for age and sex is a more sensitive screening tool for determining metabolic risk than a BMI in the 95th percentile or higher in these youths. 26
ECGs monitoring was not performed for almost 90% of the patients (see also the studies of De Hert et al. and Connolly et al. 15,63 ). Psychiatrists may omit prescribing an ECG for clinically stable patients with no symptoms or personal/family history of heart disease, in a context where ECGs can be performed locally. In addition, the CAMESA guidelines do not include recommendations for ECG monitoring, which is useful for AP-treated patients, especially in the presence of coexisting personal/family risk factors or a ziprasidone prescription. 71,72 Nevertheless, polypharmacy should be considered in the decision to perform ECG monitoring, as certain medications may prolong the QTc interval (i.e., citalopram, venlafaxine, bupropion, mirtazapine, and lithium). 73
Fasting insulin assessment was missing for at least 97% of our patients. Such monitoring is not recommended by the CAMESA guidelines for aripiprazole-treated youths. The psychiatrists may not consider medically necessary to measure fasting insulin when fasting glucose is monitored or when not familiar with this specific aspect of the guideline. A low rate for glucose monitoring has been frequently reported, 12,39,63 but studies assessing insulin monitoring are rare. Insulin screening rates may attain higher levels than those observed here, after implementation of a monitoring training program. 38 Assessment of fasting insulin appears to be clinically relevant in long-term SGA-treated patients, as the risk of developing type 2 diabetes increases with the cumulative dose of SGA and duration of treatment. 43 –45
Factors Influencing Monitoring
Adolescents had higher monitoring rates than children at baseline (AM, BP, and BT) and 1 to 6 months (AM and BP), in accordance with some 47 but not all 39,40 previous findings. This association may have been missed due to small sample size 40 or low monitoring rates during the studied period. 39
Monitoring rates for patients diagnosed with psychotic and/or affective disorders were higher than those diagnosed with personality, anxiety, and other disorders and neurodevelopmental disorders, as previously reported for glucose and lipid monitoring, 47 possibly related to their increased risk of developing obesity, type 2 diabetes, and metabolic syndrome, independently of SGA exposure. 15,44,45,58,74 Conversely, challenging behaviors associated with youths with ADHD 68 or an autism diagnosis 75 could explain the low monitoring rates in this later population.
A higher BT monitoring rate at 1- to 6-month period was found for patients with no or 1 comorbidity. This is surprising, as a higher number of comorbidities translates into more complex cases, which should be more vigilantly monitored. Having multiple mental health comorbidities increases the odds of glucose and lipid monitoring by more than 2-fold. 47 Nonetheless, with the exception of this significant association, other monitoring rates were similar concerning the number of associated comorbidities (0 to 1 vs. 2 to 4), extending the results reported by Coughlin et al. 39 and Javaheri and McLennan 40 to a longer period.
BT monitoring rates at baseline and 9 to 24 months were higher for patients treated by psychiatrists with fewer years in practice (<12 years) in accordance with the results of a large national survey, showing that more years in practice as a child and adolescent psychiatrist were associated with lower odds of lipid and glucose monitoring. 50 Clinicians with fewer years of practice could be more aware of the monitoring guidelines or more comfortable interpreting metabolic parameters, as physician barriers to monitoring include, among other factors, familiarity with ordering and interpreting results. 76,77
Participants in the high SGA dose category had higher monitoring rates at baseline (AM and BT) and 1 to 6 months (AM and BP) compared with those in the medium or low SGA dose categories, which had not been previously reported in the pediatric population. This is consistent with a previous adult study, reporting higher baseline monitoring associated with concurrent APs (but not specifically with high SGA doses) in patients with schizophrenia. 52 Given the dose-dependent relationship between the SGA dose and the metabolic risk of weight gain and dyslipidemia, especially for risperidone and olanzapine, 61 clinicians could have monitored these Participants more vigilantly. The diagnosis of psychotic and/or affective disorder was associated with higher monitoring rates independently of the SGA dose range received by these patients. Around two-thirds of all Participants in our sample received an SGA dose in the low or medium range during the follow-up period, which could explain their low monitoring rates.
Finally, patients treated with psychostimulants/atomoxetine comedication had lower monitoring rates at baseline (AM and BT), 1 to 6 months (BT), and 9 to 24 months (BT), compared to those who received an α-2a-agonists/antidepressants/mood stabilizers or no comedication. This is consistent with a previous Canadian study, 39 reporting overall (but not specifically for psychostimulant/atomoxetine) low monitoring rates among SGA-treated youth with a diagnosis of ADHD. Psychostimulants and SGAs have potentially reciprocal neutralizing AEs. 78,79 Psychostimulants in cotreatment with SGAs did not seem to attenuate SGA-induced weight gain. 17,80,81 The number of comedications did not influence the monitoring rates, unlike the findings that adolescents, taking other medications in addition to SGAs, were significantly more likely to receive baseline monitoring. 39
Limitations
Our sample size provided adequate statistical power to observe only medium and large differences between monitoring rates across categories of covariates. 82 Because of our relatively small sample size, generalized linear mixed models could not be used to take time into account in analysis of the factors influencing monitoring rates. These factors were instead separately analyzed for each time period with the Fisher exact test. For the same reason, possible confounding could not be addressed by multivariate analysis. The retrospective aspect of this study prevents controlling the quality and availability of the data and document the cause of discontinuing SGA treatment, the reasons behind missing monitoring parameters, such as absent or missed appointments, not prescribed or not completed monitoring, or the relationship between the monitoring rates and the number or frequency of clinical appointments. Furthermore, all participants were included from the outpatient clinics of a single child and adolescent psychiatric center, which can affect the generalizability of the results.
Conclusion
According to our 2 years of follow-up, up to one-half of patients remained unmonitored. Being adolescent, have been diagnosed with a psychotic and/or affective disorder, receiving a high SGA dose, having 0 to1 psychiatric comorbidities, and shorter clinician’s experience positively influenced the monitoring rates. Psychostimulant/atomoxetine comedication negatively influenced them. Although larger samples are required to validate these results, such low monitoring rates are a source of concern in youths because of the risk of metabolic morbidity and the long-term consequences. 21 –23 Prioritizing metabolic monitoring could prevent these consequences in SGA-treated patients through early detection, better management, education of the clinical team members and families about monitoring guidelines, as well as increasing involvement of nurses in clinical practice. 67,68
Footnotes
Authors’ Note
Data will be available from a third-party platform upon request.
Acknowledgments
We thank all our colleagues, psychiatrists, and mental health professionals from the CIUSSS-NIM for their assistance with this study and the support they offer to patients and their families, with special thanks to Marc Labonté and Laurence Cuillerier, mental health managers. We also thank, together with Sarra Jazi and Marie-Line Menard, CHU Sainte-Justine Foundation “Petits trésors” Foundation and Lenval Foundation for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by CHU Sainte-Justine Foundation. Sarra Jazi was supported by the Riviere-des-Prairies Mental Health Hospital Foundation “Les petits trésors”. Marie-Line Menard was supported by Lenval Foundation. The CHU Sainte Justine Foundation, the “Petits trésors” Foundation and the Lenval Foundation had no involvement or restrictions regarding this publication.