
Abstract
Objective:
Second-generation antipsychotics (SGAs) are used for a variety of mental disorders and are associated with cardiometabolic side effects in children. The objective of this study was to assess the cardiovascular health of children with mental disorders that are SGA-treated or SGA-naive.
Methods:
SGA-treated (n = 47) or SGA-naive (n = 37) children (aged 6 to 18 years) with mental disorders and control children (n = 83, no mental disorder) underwent assessment for cardiac function and morphology by echocardiography, aortic pulse wave velocity (PWV), and carotid intima-media thickness (cIMT). Body mass index (BMI) z-scores, waist circumference z-scores, systolic and diastolic blood pressure (BP) percentiles for height and sex, and fasting plasma glucose, insulin, triglycerides, and cholesterol were also assessed. Differences between SGA-treated, SGA-naive, and control children were assessed by linear and log-linear regression models.
Results:
SGA-treated children had greater BMI z-scores and overweight/obesity (BMI ≥ 85th percentile for age and sex) and hypertension than SGA-naive and control children. The PWV geometric mean was 11.1% higher in SGA-treated (95%CI, 3.95 to 18.77) and 12.9% higher in SGA-naive children (95% CI, 5.60 to 20.59) compared to controls in models adjusted for age, sex, BMI, and systolic BP percentile. Left ventricular (LV) end-diastolic dimension/body surface area (BSA), LV end-systolic dimension/BSA, and LV ejection fraction were lower in SGA-treated and SGA-naive children compared to controls in models adjusted for sex and age.
Conclusions:
Children with mental disorders have greater arterial stiffness and altered cardiac structure/function than children with no mental health diagnosis. SGA treatment in children is not associated with alterations in cardiovascular structure/function.
Introduction
In Canada, it is estimated that 14% (1.2 million) of children and youth under the age of 19 years are affected by a mental health disorder. 1 Similarly, 13% to 18% of children (8 to 18 years of age) in the United States are estimated to have a mental health disorder. 2 It is well-known that adults with mental health disorders, such as bipolar disorder or schizophrenia, have a greater risk of cardiovascular disease and cardiovascular mortality. 3 –5 Given that mental health disorders start in childhood, the cardiovascular damage associated with these conditions may also begin in childhood. This is concerning because the presence of cardiovascular damage, such as greater arterial stiffness or carotid intima-media thickness (cIMT), in childhood is predictive of poor cardiovascular health in adulthood. 6,7 Some indicators of cardiovascular damage have been reported in young adults with major depressive disorder and bipolar disorder prompting a scientific statement from the American Heart Association in 2015. 8 Further, symptoms of mental illness such as anxiety and depression have also been reported to be associated with indicators of endothelial dysfunction and arterial stiffness. 9 –12
Medication side effects may also contribute to the greater risk of cardiovascular disease in individuals with mental illness. In adults, treatment with second-generation antipsychotics (SGAs) is associated with cardiometabolic complications including rapid weight gain, dyslipidemia, insulin resistance, and hypertension. 13 Population-based studies have reported associations between risk of cardiovascular disease and SGA treatment in adults with mental illness. 5 Another study of adults with schizophrenia, mood disorders, or dementia reported greater risk of acute myocardial infarction with short-term SGA treatment. 14
SGAs are increasingly being prescribed to children and adolescents and are often used off-label as an effective treatment of a variety of mental health disorders including attention deficit hyperactivity disorder, anxiety disorder, bipolar disorder, and autism spectrum disorder. 15 –17 We and others have reported similar rapid weight gain, obesity, hypertension, and metabolic dysfunction in SGA-treated children, 18 –25 and compared to adults, there is evidence that these complications appear faster and to a greater extent in children. 26,27 Recent studies also estimate that SGA-treated children have a 3-fold greater risk of type 2 diabetes compared to untreated children. 28,29
There is a growing concern regarding the long-term health of SGA-treated children because of the metabolic complications. It is well-known that childhood obesity is associated with risk factors such as hypertension and dyslipidemia, but there is also evidence that childhood obesity has direct effects on cardiovascular structure and function. 30 Several studies in children have reported positive associations between adiposity and cIMT, 31,32 a subclinical indicator of atherosclerosis 33 ; greater pulse wave velocity (PWV), 34 a measure of arterial stiffness 35 ; and greater left ventricular (LV) mass, 36 which may lead to impaired long-term cardiac mechanics and function. 37 To date, only 1 study in adults has reported a positive association between SGA treatment and greater PWV compared to untreated subjects. 38 The objective of this study was to assess arterial stiffness, cIMT, and cardiac structure and function in SGA-treated children, children with mental illness who were not treated with SGAs (SGA-naive), and control children with no mental illness.
Materials and Methods
Study Design and Subject Recruitment
Children aged 6 to 18 years were recruited between August 1, 2012, and June 1, 2018, from inpatient and outpatient psychiatric units at BC Children’s Hospital in Vancouver, Canada. Written informed consent was obtained from parent(s)/legal guardian(s), and assent was obtained from subjects when capable. Ethics approval for this study was obtained from the University of British Columbia Clinical Research Ethics Board and the Children’s and Women’s Health Centre of British Columbia Research Ethics Board certificate H12-00954. From August 1, 2012, to June 1, 2018, a total of 115 children with a mental health diagnosis were recruited for this study. Of these, 84 children were studied: n = 37 in the SGA-naive group and n = 47 in the SGA-treated group. There were n = 31 children who were not studied due to changes in antipsychotic medication regimen, study noncompliance, and loss to follow-up of scheduling the study visit.
Enrolled subjects were categorized by SGA treatment as follows: SGA-treated, continuous treatment with an SGA for ≥ 3 months and SGA-naive, no current or previous treatment with an SGA. SGA-treated and SGA-naive children were often treated with other psychiatric medications such as antidepressants or psychostimulants. Data from SGA-treated and SGA-naive children were also compared to a group of age- and sex-matched children (n = 83), with no mental illness and no current or previous treatment with psychiatric medications, who underwent standard echocardiography at the BC Children’s Hospital Heart Centre. Data on the control subjects have been published. 39 Exclusion criteria for all groups of children included the following: any metabolic disorder (e.g., type 1 or 2 diabetes, polycystic ovary syndrome), any genetic disorder (e.g., Down syndrome, Prader–Willi syndrome), eating disorder, fetal alcohol spectrum disorder, treatment with medications known to affect metabolism (e.g., glucocorticoids, thyroxine, propranolol), and illicit substance use.
Anthropometric, Clinical, and Biochemical Analyses
Medical records were reviewed at the time of recruitment for sociodemographic information (sex and date of birth), medical and family history, medication use (history, dose, and duration), and psychiatric diagnoses as determined by the attending psychiatrist per the multiaxial evaluation system of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, Text Revision (DSM-IV-TR). 40 Interviews with participants and families were conducted to obtain information regarding self-reported ethnicity, smoking habits, and self-reported pubertal status according to Tanner staging. 41,42
Anthropometric data were collected by the research assistant. Height was recorded to the nearest 0.1 cm using a Seca 240 Stadiometer (Hamburg, Germany), and weight was recorded to the nearest 0.1 kg using a ScaleTronix 5002 Mobile Stand-On Scale (White Plains, NY). Body mass index (BMI) was calculated (weight [kg]/height2 [m2]), and z-scores and percentiles were determined by adjusting for age and sex as per the U.S. Centers for Disease Control and Prevention growth chart data. 43 Subjects were categorized into healthy weight (BMI < 85th percentile), overweight (BMI ≥ 85th percentile), or obesity (BMI ≥ 95th percentile). Hip (at maximal protrusion of the gluteus) and waist circumference (at the umbilicus) were measured to the nearest 0.1 cm using an Almedic measuring tape, and the average of 2 readings was recorded. As per the International Diabetes Federation criteria for metabolic syndrome, subjects were categorized by waist circumference as healthy (<90th percentile for age and sex) or elevated (≥90th percentile), and by waist-to-height ratio as healthy (<85th percentile for age and sex) or elevated (≥85th percentile). 44 Total body fat mass percentage was quantified by bioelectric impedance analysis using the BC-418 Tanita Body Composition Analyzer (Tanita Corporation).
Blood pressure (BP) was measured by a registered nurse as per clinical guidelines 45 . A GE Carescape V100 monitor (GE Medical Systems) was used to measure BP in children who were seated in a chair with feet resting on the floor with the right arm supported at the level of the heart. Systolic BP (SBP) and diastolic BP (DBP) percentiles adjusted for age, sex, and height were used to categorize subjects as normal, elevated, or stage 1 or 2 hypertension according to the 2017 American Academy of Pediatrics Clinical Practice Guidelines for Screening and Management of High Blood Pressure. 45
A blood sample was collected by venipuncture following an overnight fast. The following biochemical markers were quantified in plasma by the Children’s and Women’s Laboratory at BC Children’s Hospital: fasting glucose, fasting insulin, triglycerides, total cholesterol, low-density lipoprotein (LDL) cholesterol, and high-density lipoprotein (HDL) cholesterol. Insulin resistance was estimated by fasting glucose and insulin concentrations using the homeostatic model assessment-2 of insulin resistance (HOMA2-IR) calculator. 46
Echocardiography and Vascular Measurements
Standard M-mode, 2-dimensional echocardiography and Doppler imaging were performed by a clinical pediatric echocardiography technician using a Vivid system (GE Vingmed Ultrasound AS) and a 3.5-MHz transducer according to published standards. 47 Data from LV end-diastolic dimension (LVED) and LV end-systolic dimension (LVES) are expressed per body surface area (BSA), calculated using the Haycock formula. 48 LV ejection fraction and shortening fraction were quantified from the M-mode tracings. LV mass was calculated using the Devereux formula and was indexed to height (m)2.7. 49,50
The biophysical properties of the aorta were measured using a previously established echocardiographic Doppler method. 51,52 A pulsed-wave Doppler trace (interval from the Q wave on the echocardiogram to the onset of the Doppler envelope) was obtained from the proximal ascending aorta in a suprasternal long-axis view. The difference between the QRS signal and the onset of flow was time 1. A second pulsed-wave Doppler trace was then obtained in the descending aorta, and the difference between the QRS signal and the onset of flow was used to obtain time 2. Transit time was calculated from the difference between times 2 and 1. The length of the aortic arch between these 2 locations was measured. The following formula was used to calculate aortic PWV: aortic arch length/transit time.
cIMT was determined as previously described. 53 Briefly, the far wall of the right and left common carotid arteries, within 2 cm of the carotid bifurcation, were measured using GE EchoPAC software Version 113 (GE Healthcare, Chicago, IL). Measurements were performed over a uniform length of 10 mm (standard deviation of each measurement < 0.1 mm), and an average reading was obtained from a minimum of 3 cIMT measurements from each carotid artery (minimum of 6 measurements total).
Statistical Analyses
Categorical variables were presented as number and percentage and analyzed across groups using Pearson’s χ2-test or Fisher’s exact test as applicable. Continuous variables were presented as mean (standard deviation) or median (25th, 75th percentiles). Student’s t test or Wilcoxon rank sum test was used for comparisons between 2 groups. One-way analysis of variance or Kruskal–Wallis test was used for the comparison between the 3 groups as applicable. Following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, 54 hypothesis testing was not conducted to compare the demographic characteristics.
Linear regression models were used to assess the effect of SGA treatment on cIMT, LV ejection fraction, LVED, and LVES. Log-linear regression models were used to assess the effect of SGA treatment on log values of aortic PWV. The estimates from the log-linear models were transformed back and presented as geometric mean difference (%) for more intuitive interpretations. Models were adjusted for covariates selected a priori (age, sex, BMI, SBP percentile, LDL, heart rate). All statistical analyses were conducted in Stata statistical software Version 14.2 (StataCorp, College Station, TX).
Results
Demographic and clinical characteristics of the study population are presented in Table 1. The most common mental health diagnoses in the SGA-treated and SGA-naive groups were anxiety disorder, attention deficit hyperactivity disorder, and autism spectrum disorder. The most common SGA was risperidone (51%) followed by quetiapine (26%) and aripiprazole (23%). The median duration of SGA treatment was 15.0 months (7.3, 28.3 [25th, 75th percentiles]). The majority of the SGA-treated (87%) and SGA-naive (92%) children were taking other medications; the most common were antidepressants followed by psychostimulants. Data on self-reported ethnicity and pubertal status (Tanner stage) were not available from the control subjects. Most subjects were in Tanner stage II or III for pubertal development. The majority of subjects were of European descent. None of the children reported smoking.
Demographic Characteristics of the Study Population.
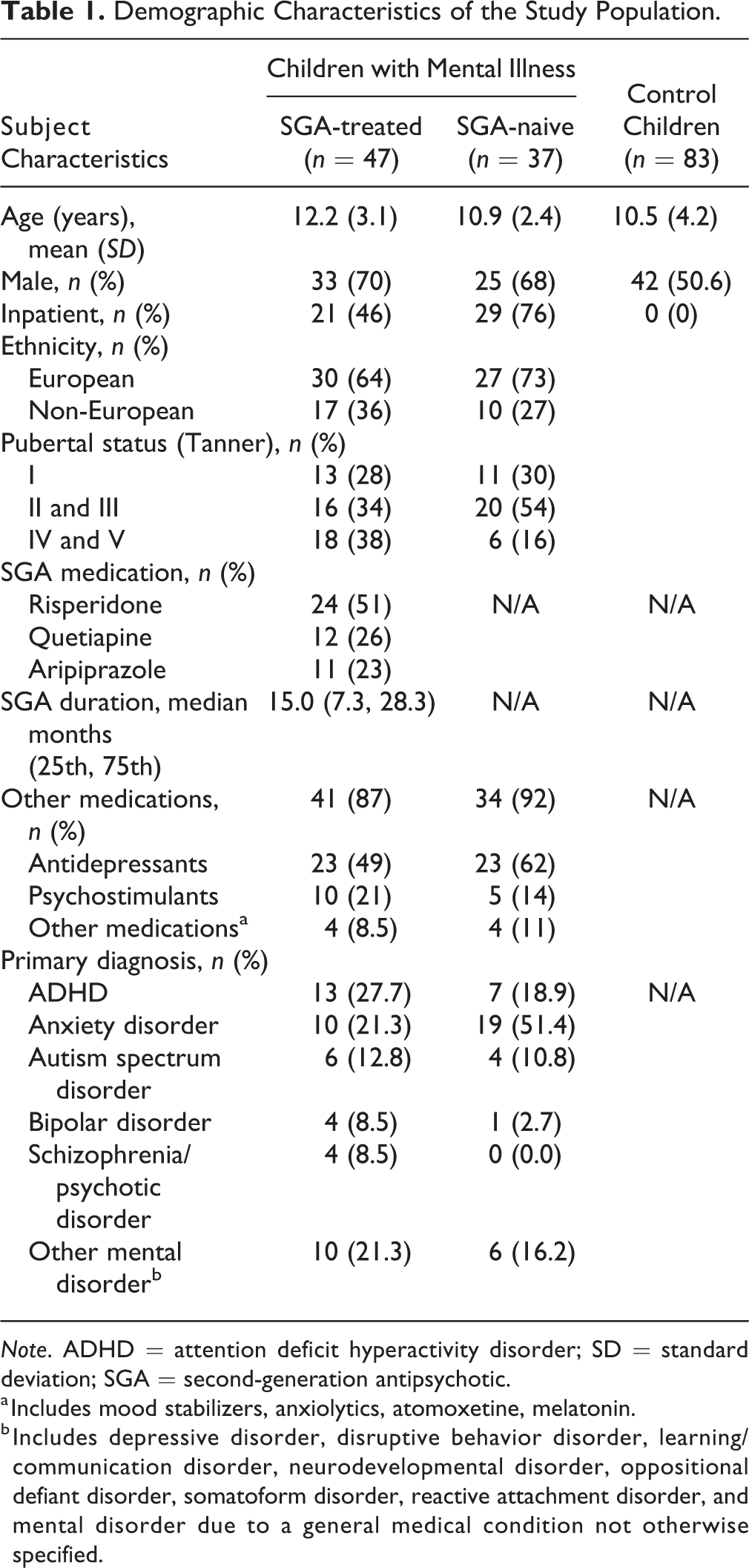
Note. ADHD = attention deficit hyperactivity disorder; SD = standard deviation; SGA = second-generation antipsychotic.
a Includes mood stabilizers, anxiolytics, atomoxetine, melatonin.
b Includes depressive disorder, disruptive behavior disorder, learning/communication disorder, neurodevelopmental disorder, oppositional defiant disorder, somatoform disorder, reactive attachment disorder, and mental disorder due to a general medical condition not otherwise specified.
The anthropometric and metabolic characteristics of the study population are summarized in Table 2. SGA-naive and SGA-treated children had higher BMI z-scores and a higher prevalence of overweight/obesity compared to control children. SGA-treated children had greater BMI z-scores, total body fat percentage, waist circumference z-scores, and waist-to-height ratio z-scores than SGA-naive children. No differences in plasma total, LDL, or HDL cholesterol or triglyceride concentrations were observed between SGA-treated and SGA-naive children. SGA-treated children had greater HOMA2-IR and a higher prevalence of elevated fasting plasma insulin concentrations than SGA-naive children (Table 2). More SGA-treated children were categorized as having elevated SBP or DBP (13%) or as having stage 1 or 2 hypertension (15%) compared to SGA-naive children (11% and 5%, respectively) and the control children (11% and 6%, respectively).
Anthropometric and Metabolic Characteristics in Children with Mental Health Conditions and Control Children.
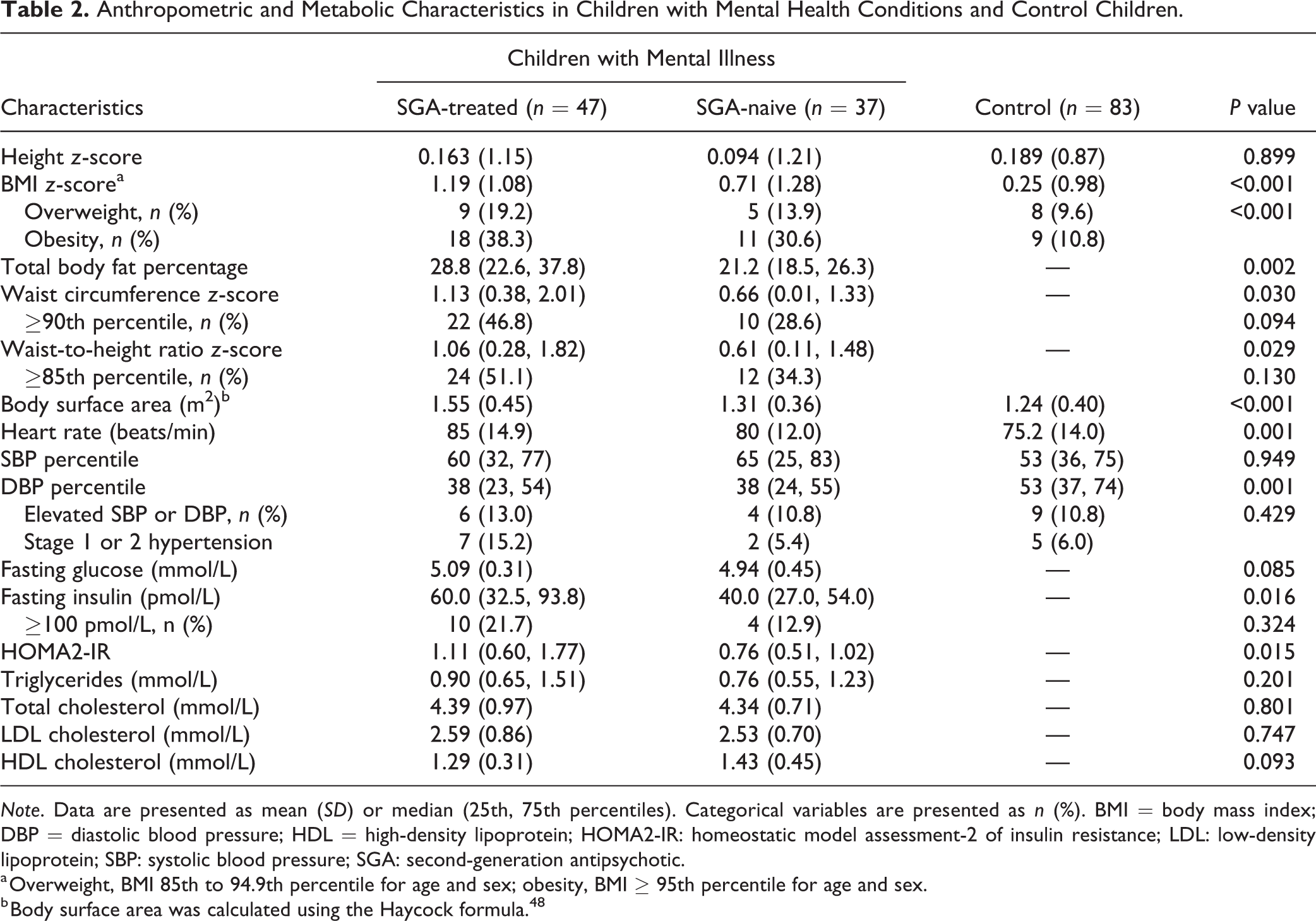
Note. Data are presented as mean (SD) or median (25th, 75th percentiles). Categorical variables are presented as n (%). BMI = body mass index; DBP = diastolic blood pressure; HDL = high-density lipoprotein; HOMA2-IR: homeostatic model assessment-2 of insulin resistance; LDL: low-density lipoprotein; SBP: systolic blood pressure; SGA: second-generation antipsychotic.
a Overweight, BMI 85th to 94.9th percentile for age and sex; obesity, BMI ≥ 95th percentile for age and sex.
b Body surface area was calculated using the Haycock formula. 48
Measures of vascular and cardiac structure and function are presented in Table 3. Aortic PWV was higher in SGA-treated and SGA-naive children compared to control children. After adjusting for age, sex, BMI, and SBP percentile, the geometric mean of aortic PWV was 12.9% higher (95% CI, 5.60 to 20.6; P < 0.001) in the SGA-naive children and 11.1% higher in the SGA-treated children (95% CI, 3.95 to 18.8; P = 0.002) compared to control children (Table 4). No differences in aortic PWV or cIMT were observed between the SGA-treated and SGA-naive subjects in adjusted or unadjusted models.
Cardiovascular Function in Children with Mental Health Conditions and Control Children.
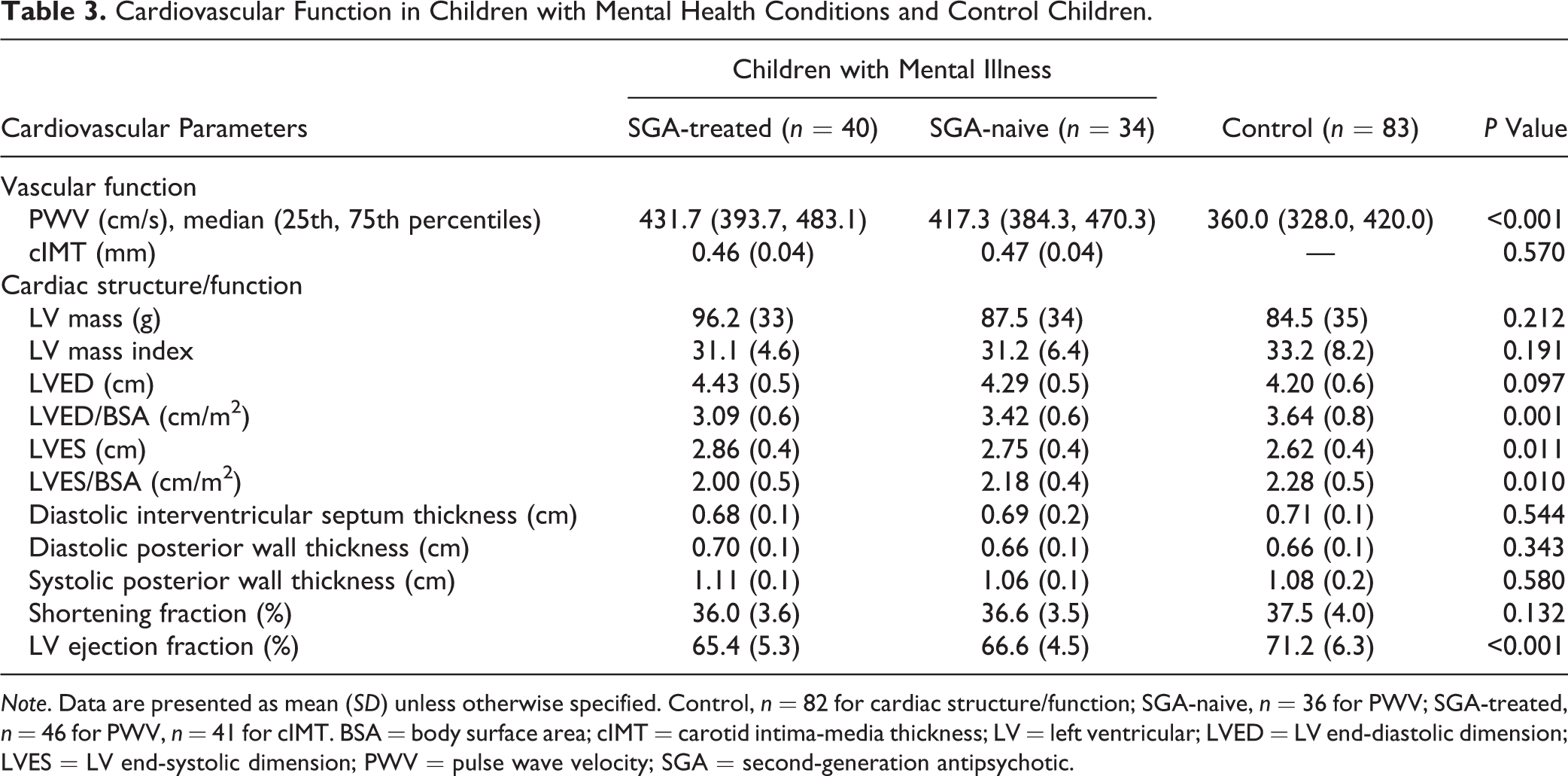
Note. Data are presented as mean (SD) unless otherwise specified. Control, n = 82 for cardiac structure/function; SGA-naive, n = 36 for PWV; SGA-treated, n = 46 for PWV, n = 41 for cIMT. BSA = body surface area; cIMT = carotid intima-media thickness; LV = left ventricular; LVED = LV end-diastolic dimension; LVES = LV end-systolic dimension; PWV = pulse wave velocity; SGA = second-generation antipsychotic.
Relationships between SGA Treatment and Cardiac and Vascular Structure and Function.
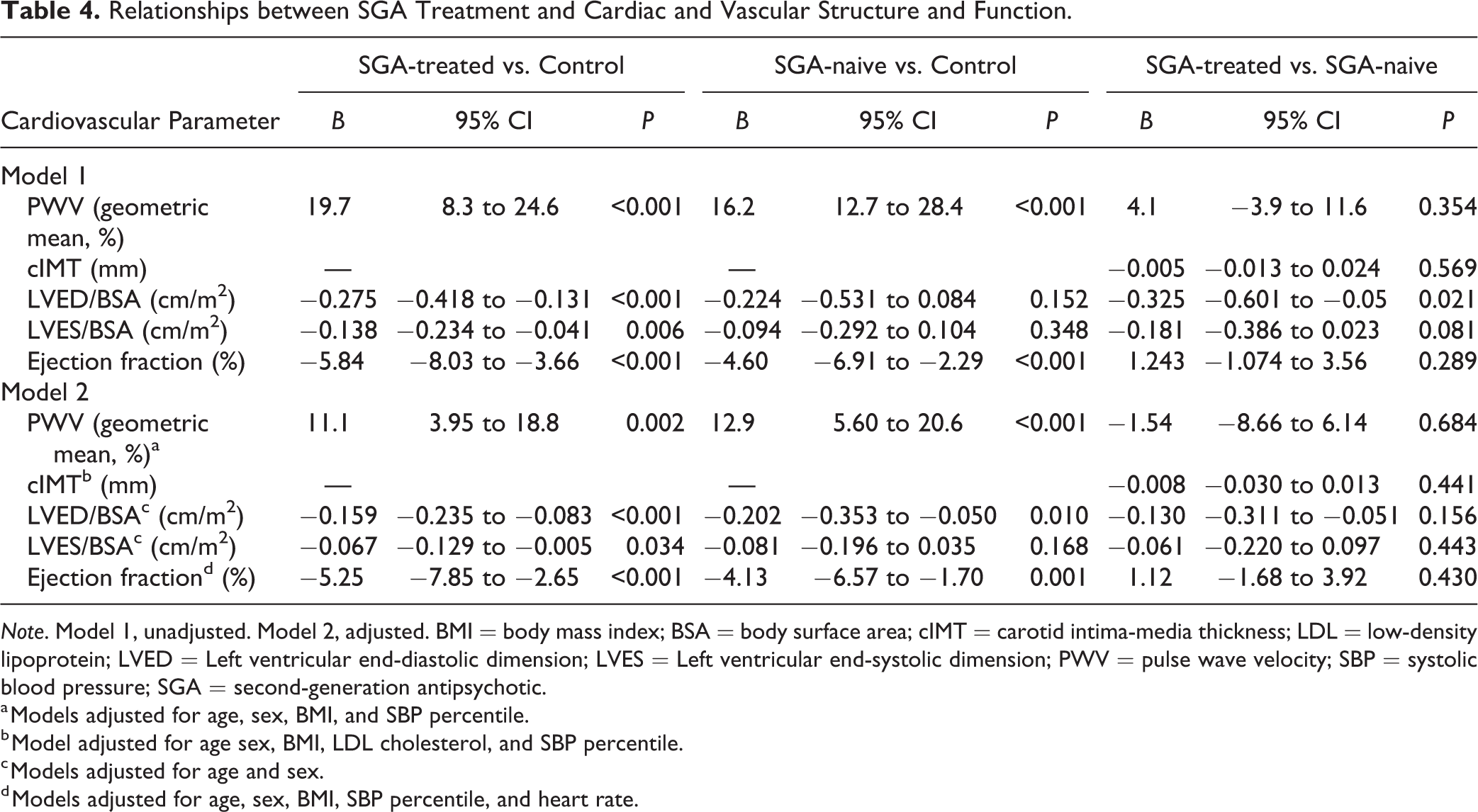
Note. Model 1, unadjusted. Model 2, adjusted. BMI = body mass index; BSA = body surface area; cIMT = carotid intima-media thickness; LDL = low-density lipoprotein; LVED = Left ventricular end-diastolic dimension; LVES = Left ventricular end-systolic dimension; PWV = pulse wave velocity; SBP = systolic blood pressure; SGA = second-generation antipsychotic.
a Models adjusted for age, sex, BMI, and SBP percentile.
b Model adjusted for age sex, BMI, LDL cholesterol, and SBP percentile.
c Models adjusted for age and sex.
d Models adjusted for age, sex, BMI, SBP percentile, and heart rate.
LVED/BSA, LVES/BSA, and LV ejection fraction were lower in SGA-treated and SGA-naive children compared to control children (Table 3). The differences in LVED/BSA and LVES/BSA between control children and SGA-treated children remained after adjustments for sex and age (Table 4); only LVED/BSA remained significantly different between control and SGA-naive children after adjustments for sex and age. LV ejection fraction remained statistically significant after models were adjusted for age, sex, BMI, and systolic BP percentile (Table 4). No differences in LVED/BSA, LVES/BSA, or LV ejection fraction were observed between SGA-treated and SGA-naive children. No differences in LV mass indexed to height2.7, diastolic interventricular septum thickness, or systolic or diastolic posterior wall thickness were observed among any of the groups (Table 3).
Discussion
The goal of this study was to assess whether treatment with SGAs is associated with cardiovascular dysfunction in children with mental health conditions in a cross-sectional population of children aged 6 to 18 years. We report that SGA-treated and SGA-naive children with mental illness have early indicators of cardiovascular dysfunction. We found that children with a mental health diagnosis have greater central PWV than children without a mental health diagnosis. Further, this relationship remained significant after adjustment for age, sex, BMI, and SBP, factors known to influence PWV. The greater PWV in these children was accompanied by lower LV ejection fraction and higher systolic LV dimension; however, these parameters were still in the physiologically healthy range.
There are no published data on the cardiovascular health of SGA-treated children despite the well-known cardiometabolic side effects that occur with SGA treatment. 18 –25 We assessed PWV and cIMT, as noninvasive indicators of vascular health and atherosclerosis, that are strongly associated with future cardiovascular events in adults. 35,55 Only 2 studies have been published that investigated vascular function in SGA-treated adults. 38 Adults (n = 56) with schizophrenia or bipolar disorder treated with an SGA for a mean duration of 2 years had higher upper-limb PWV than age- and sex-matched control adults (n = 40) with no mental illness. Similarly, greater aortic PWV was reported in adults with schizophrenia (n = 10) who were treated with SGAs compared to healthy controls (n = 10). 56 However, these studies did not include subjects with mental illness who were SGA-naive and did not adjust for metabolic variables, such as BMI and BP, in the analyses. As such, it is difficult to interpret these studies because it is unknown whether the greater arterial stiffness is due to the SGA treatment or the mental illness.
We compared SGA-treated children and SGA-naive children with mental illness to distinguish the effects of mental illness from SGA treatment. Our finding that both SGA-treated and SGA-naive children have higher PWV than control children suggests that the underlying mental illness affected the vascular health of the children. However, our study is confounded by the fact that SGA-treated children likely have different psychiatric symptoms than untreated children and hence the indication for use of these medications. Larger longitudinal studies are required to definitely address the effects of SGA treatment on cardiovascular health in SGA-treated children.
Little is known about the cardiovascular health of children with mental illness. One cross-sectional study in adolescents (n = 364), mean age 14.7 years, found no association between self-reported negative mental health symptoms and mean arterial pressure, carotid-femoral PWV (using a SphygmoCor XCEL device), or cIMT. 9 In contrast, another study reported that adolescents (n = 157) aged 16 to 21 years who experienced severe depressive symptoms had higher carotid-femoral PWV (by Doppler tracing) but had no differences in cIMT. 10 The latter study parallels our findings that mental health conditions are associated with elevated PWV in youth. However, there are a few differences between these studies and our study that make comparisons difficult. We recruited subjects with diagnosed mental health disorders as per the DSM-IV-TR, whereas the studies by Lycett et al. 9 and Dietz and Matthews 10 determined the relationship between self-reported or self-assessed mental health symptoms and vascular health in adolescents without a diagnosed mental health condition. Several different techniques and locations can be used to assess PWV/arterial stiffness, further making comparisons between studies difficult. We used the well-established and reliable method of echocardiographic Doppler ultrasound traces from the thoracic aorta. 51 This method is advantageous as it allows for assessment of aortic PWV and cardiac function/structure measurements simultaneously, whereas Lycett et al. 9 and Dietz and Matthews 10 analyzed carotid-femoral PWV. Further, it should be noted that another study reported no relationship between levels of psychosocial stress and depression and carotid-femoral PWV in children (n = 520) at baseline (mean age 11.6 years) and at follow-up 4 years later. 57
Childhood obesity is associated with altered cardiac morphology and function. 30 Several studies have reported greater LV dimensions and mass in children with obesity compared to children with a healthy BMI. 36,39,58 As such, we predicted that SGA-treated children may have altered cardiac morphology and function because of the metabolic complications. We observed no differences in LV mass, posterior wall thickness, or interventricular septum thickness among any of the children. However, we did find lower LVED/BSA, LVES/BSA, and LV ejection fraction in SGA-treated and SGA-naive children compared to control children. This suggests that the greater arterial stiffness in SGA-treated and SGA-naive children may be associated with increased afterload and early diastolic dysfunction resulting in a lower ejection fraction. There is little published data on the effects of antipsychotic medications on cardiac structure/function in children or adults. Only 1 recent small study reported that SGA-treated adults with schizophrenia (n = 14) had lower indexed LV mass but no differences in ejection fraction, determined by cardiac MRI, compared to untreated controls (n = 17). 59
SGA-treated and SGA-naive children also had lower DBP than control children. Arterial stiffness is an independent predictor of longitudinal changes in SBP and incident hypertension. 60,61 In the current study, we did not observe the effects of SGAs or mental illness on SBP but did observe lower DBP in SGA-treated and SGA-naive children compared to healthy controls. With greater arterial stiffness, the ability of vessels to cushion and accommodate blood flow during systole and then recoil during diastole is impaired. This may lead to higher SBP and lower DBP as previously reported in adults with metabolic syndrome. 62 In our study, we observed no differences in SBP. However, it is possible that the elevations in PWV we observed in the SGA-treated and SGA-naive children may indicate early vascular structural changes that contribute to a lowering of DBP but precede alterations in SBP.
Limitations
This study must be interpreted within the context of its limitations. The cross-sectional design of this study limits our understanding of how SGA treatment may affect cardiovascular health over time in regard to changes in other cardiometabolic parameters, body composition, and other factors such as duration of SGA treatment. In our cohort, we observed a wide range of SGA treatment duration (from 3 to 96 months). Thus, it is difficult to accurately assess how SGAs may alter cardiovascular health over time. Further, we recognize that the majority of the children with mental illness were treated with other medications (e.g., antidepressants, psychostimulants) and that there is the possibility that these medications affect cardiovascular parameters. We also did not make use of research diagnostic interviews or scales to collect data on the severity of the mental health disorder or symptom severity, both of which could also affect cardiovascular health. We recognize that SGA-treated children likely had different psychiatric symptoms than SGA-naive children. However, these data were not collected and were unable to account for this in the current study. Family history of cardiovascular disease was not considered, and the children with mental illness may have a greater predisposition to cardiovascular disease than the control children. Additionally, because data for the control group were collected retrospectively, some data were unavailable for certain anthropometrics, cIMT, and circulating lipid concentrations. Therefore, we were unable to make comparisons between SGA-treated and SGA-naive subjects to age-and sex-matched control for these measures. Future prospective studies are warranted to further investigate how SGAs affect cardiovascular health in children and youth over time.
Conclusions
Overall, our findings provide evidence that SGA-treated and SGA-naive children with a mental health diagnosis have greater arterial stiffness than children without mental illness. The mechanisms underlying these effects are still unknown, and further investigations are pertinent for preventing long-term health complications. SGA treatment was not associated with alterations in cIMT, arterial stiffness, or cardiac structure/function in children. Long-term prospective studies are required to understand the pathology and progression of the cardiovascular dysfunction in children with mental illness. This will inform intervention trials designed to mitigate the cardiovascular dysfunction in these children and improve their long-term health outcomes.
Footnotes
Authors’ Note
Amanda M. Henderson analyzed the data and wrote the manuscript. Constadina Panagiotopoulos and Angela M. Devlin designed the research and supervised the study, wrote the manuscript, and had primary responsibility for final content of the manuscript. Nazrul Islam analyzed the data and critically revised the manuscript. George G. S. Sandor provided expertise on cardiovascular assessments and interpretation of data and critically revised the manuscript. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Acknowledgment
The authors thank Lindsey Williams for assistance with echocardiography and Astrid De Souza for assistance with data from control subjects.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the British Columbia Mental Health and Substance Use Services (to Angela M Devlin and Constadina Panagiotopoulos). Angela M Devlin is supported by an Investigator Grant from the BC Children’s Hospital Research Institute.