
Abstract
Objective:
The Canadian 24-Hour Movement Guidelines for Children and Youth recommend at least 60 minutes of physical activity per day, 2 hours or less of recreational screen time per day, and 9 to 11 hours of sleep per night for 5 to 13 years old and 8 to 10 hours per night for 14 to 17 years old. This study examined the association between meeting these guidelines and psychological distress among adolescents.
Methods:
The present cross-sectional sample included 6,364 students aged 11 to 20 years from the 2017 Ontario Student Drug Use and Health Survey. This provincially representative school-based survey is based on a 2-stage cluster design. A confirmatory factor analysis (CFA) was first conducted to confirm the factor structure of the K6, and structural equation modeling adjusted for age, sex, ethnoracial background, subjective socioeconomic status, and body mass index z-score was used to investigate the association between meeting the 24-Hour Movement Guidelines and K6 factors among adolescents.
Results:
The CFA demonstrated that a 2-factor model (representing anxiety and depressive symptoms) of the K6 fit the data well. The anxiety and depression items demonstrated a composite reliability (Cronbach’s α) of 0.86 and 0.83, respectively, indicating a high level of internal consistency. Compared to meeting none of the recommendations, meeting all 3 movement behavior recommendations was associated with lower anxiety (β = −0.076; P = 0.028) and depressive symptoms (β = −0.067; P = 0.028). Meeting the screen time + sleep duration recommendations had the strongest association with anxiety (β = −0.157; P < 0.001) and depressive symptoms (β = −0.139; P < 0.001), followed by meeting the sleep duration recommendation only for both anxiety (β = −0.135; P < 0.001) and depressive symptoms (β = −0.106; P < 0.001).
Conclusions:
Meeting the 24-Hour Movement Guidelines was associated with lower anxiety and depressive symptoms among adolescents, and these associations appear mainly driven by meeting the sleep duration recommendation.
Introduction
Adolescent mental health problems are common, disabling, and have long-term consequences for individuals, families, and communities. 1,2 Psychological distress is often defined as a state of emotional suffering characterized by symptoms of depression and anxiety. 3 It is a risk indicator for common major psychiatric disorders such as depression and anxiety disorders. 4 Distress is common among adolescents; for example, the proportion of adolescents with moderate to high level of psychological distress was 24% in 2013 and increased to 39% in 2017. 5 There is a need to identify correlates of anxiety and depressive symptoms that are amenable to intervention strategies in this population.
The way school-aged children and adolescents spend their time over a 24-hour period has important mental health implications. 3 Unhealthy lifestyle behaviors, such as lack of physical activity, excessive sedentary behavior, and short sleep duration have been individually shown to be important determinants of anxiety and depressive symptoms among children and adolescents. 6 –10 However, little is known on how these behaviors may concurrently relate to mental health problems among adolescents. Indeed, the importance of an integrated approach that considers all behaviors across the movement continuum has been previously highlighted. 11 –13 The Canadian 24-Hour Movement Guidelines for Children and Youth were released in June 2016. These Guidelines provide specific recommendations on the amount of time during a typical 24-hour day that children and youth aged 5 to 17 should spend in moderate-to-vigorous physical activity (at least 60 minutes), recreational screen time (no more than 2 hours), and sleep (9 to 11 hours for 5- to 13-year-olds; 8 to 10 hours for 14- to 17-year-olds). 12 Because physical activity, sedentary behavior, and sleep duration are modifiable risk factors, there is great desire to optimize the healthy active living behaviors of children and adolescents to improve their mental health. However, it is unknown whether meeting all or some combinations of the movement behavior recommendations is more important to the mental health of children than meeting single behaviors.
The K6 scale is commonly used as a brief continuous scale of psychological distress. 14 –16 However, the 2-factor structure measuring anxiety and depressive symptoms, which represent the 2 most common forms of psychological distress, 17,18 has not been well established at the population level of adolescents. Although anxiety and depressive symptoms are highly correlated, 19,20 establishing whether these represent different constructs in our data would provide important information to guide intervention. It is also unclear whether movement behaviors may be differentially associated with symptoms of depression versus anxiety.
The purpose of this study was to examine the associations between meeting the recommendations from the 24-Hour Movement Guidelines and psychological distress in a large and representative sample of adolescents. 15 In order to achieve this objective, we sought to confirm the factor structure of the Kessler 6-item Psychological Distress Scale (K6), information that would also be important to inform intervention strategies of youth struggling with emotional distress.
Methods
The Ontario Student Drug Use and Health Survey (OSDUHS) is a population survey of Ontario students in Grades 7 through 12 in publicly funded schools. 21 Conducted biennially since in 1977, OSDUHS is the longest ongoing school survey in Canada and one of the longest in the world. The survey employs a stratified (region and school type), 2-stage (school, class) cluster sample design. The 2017 OSDUHS was approved by the Research Ethics Boards at the Centre for Addiction and Mental Health and York University as well as 31 school board research review committees. All participants provided their signed assent in addition to parentally signed consent for those aged under 18 years. In total, 11,435 students, from 764 classes, 353 schools, and 52 school boards, participated in the survey. Participation rates were 61% for students, 94% for classes, and 61% for schools. The response rates were above average for a survey of students requiring active parental consent. 22 Reasons for nonresponse among students included absenteeism (12%) and unreturned consent forms or parental refusal (27%). Analyses for this study are restricted to the random half sample of students (N = 6,364) who completed form A, which contained questions regarding psychological distress. Detailed information on the survey design and methods is available elsewhere. 21
Dependent Variable
The Kessler 6-item (K6) Psychological Distress Scale assesses symptoms of depression and anxiety occurring over the most recent 4-week period. 4,23 Responses were scored on a 5-point ordinal scale reflecting how often of over the past month respondents had experienced 6 symptoms, such as “feeling tired out for no good reason” and “sad or depressed.” The measure has 5 response categories ranging from 0 (none of the time) to 4 (all of the time). It has been widely used in research with adolescents. 15,24 –26 The psychometric properties of the K6 have been extensively examined among adolescents and young adults. 14 –16,27 Some investigators have confirmed a single factor using confirmatory factor analysis (CFA), 14 –16 while others found that a 2-factor model (representing anxiety and depression) fit the data best. 27 There is thus some uncertainty as to the true factor structure of the measure.
Independent Variables
Physical activity was measured using the following item: “On how many of the last 7 days were you physically active for a total of at least 60 minutes each day? Please add up all the time you spent in any kind of physical activity that increased your heart rate and made you breathe hard some of the time (some examples are brisk walking, running, rollerblading, biking, dancing, skateboarding, swimming, soccer, basketball, football). Please include both school and nonschool activities.” Response options ranged from 0 to 7 days. Screen time was measured using the following item: “In the last 7 days, about how many hours a day, on average, did you spend: watching TV/movies/videos, playing video games, texting, messaging, posting, or surfing the Internet in your free time? (Include time on any screen, such as a smartphone, tablet, TV, gaming device, computer, or wearable technology). Response options included none, less than 1 hour a day to 7 or more hours a day. Sleep duration was measured using the following item: “On an average school night, how many hours of sleep do you get?” Response options ranged from 4 hours or less to 11 or more hours. Students who reported being physically active 7 days per week, accumulating 2 hours or less of daily recreational screen time, and sleeping 9 to 11 hours per night for 11- to 13-year-olds; 8 to 10 hours per night for 14- to 17-year-olds, or 7 to 9 hours per night for those ≥18 years of age were classified as meeting the recommendations of the 24-Hour Movement Behavior Guidelines. 12 Single-item measures of physical activity and sleep have been demonstrated to provide reliable and valid assessments of physical activity and sleep among children and adolescents. 28,29 Self-report measures of sedentary behavior have also been shown to have acceptable reliability and validity in children and adolescents. 30,31
Although the 24-Hour Movement Guidelines we are referring to in this study are relevant for children and adolescents aged 5 to 17 years, we have included in our analyses students aged 18 to 20 years (n = 269) because they are still in high school and may still have most features of adolescent life. Regardless, we run a sensitivity analysis excluding students aged 18 to 20 years. Different combinations of movement behaviors examined in the current study include meeting none or any of the following recommendations: (1) physical activity only, (2) screen time only, (3) sleep duration only, (4) physical activity + screen time, (5) physical activity + sleep duration, (6) screen time + sleep duration, and (7) physical activity + screen time + sleep duration.
Covariates
Covariates included age (years), sex (male/female), ethnoracial background (White/Black/East and South-East Asian/South Asian/Other), subjective socioeconomic status (SES), and body mass index (BMI) z-score. Subjective SES was measured using a modified version of the MacArthur Scale of Subjective Social Status. 32
Statistical Analyses
Analyses were conducted in Mplus 8.2 and were weighted and accounted for the complex sample design of the survey using TYPE = COMPLEX function. Descriptive characteristics of participants are presented using mean, standard deviation, counts, and proportions. CFAs employing a weighted least squares means and variance-adjusted estimator were first carried out to examine the factorial structure of the Kessler 6 Scale. Items were treated as continuous variables. 4,23 We explored 3 competing models based on previous work 27 to determine which model was a better fit to the data and to be used in subsequent analyses. Specifically, Model 1 had all 6 items loading on a single factor representing psychological distress; Model 2 had the items loading on 2 correlated first-order factors representing depression and anxiety; and Model 3 had the items loading on 2 second-order factors representing depression and anxiety and having a second-order structure representing psychological distress. Composite reliability estimates of latent variables were tested using Raykov composite reliability. 33 Finally, structural equation modeling was used to examine both the measurement model and the hypothesized structural model. In the hypothesized structural model, anxiety and depression were modeled as latent variables, and movement behavior combinations modeled as observed variables. Covariates included age, sex, ethnoracial background, subjective SES, and BMI z-scores. Maximum likelihood estimation with robust standard errors was used to account for possible nonnormality in responses. Missing data were completely missing at random and were handled through full information maximum likelihood. Goodness of fit for the measurement models was determined using the root-mean-square error of approximation (RMSEA), comparative fit index (CFI), Tucker-Lewis Index (TLI), and standardized root square mean residual (SRMR). Model fit was considered acceptable if RMSEA and SRMR are below 0.08 and a good fit if they are less than 0.06, CFI and TLI values of 0.90 or above are seen as acceptable and 0.95 or above are considered a good fit, and AIC and BIC with smaller values indicate better model fit. 34 We did not rely on the χ2 test to examine model fit because current analyses used a large sample size, and χ2 is sensitive to sample size. 35 Statistical inferences were based on P values <0.05 and 95% confidence intervals (CIs).
Results
Participant Characteristics
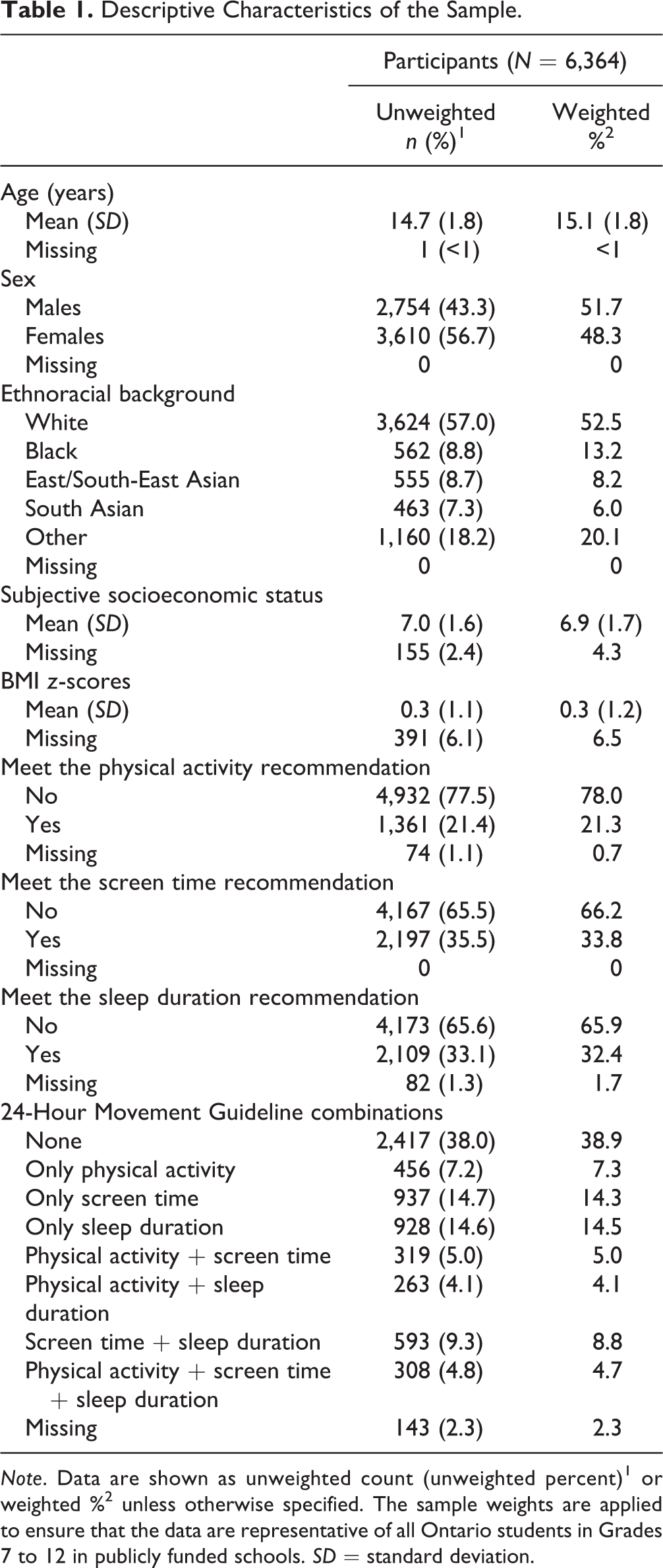
Descriptive characteristics of the sample are provided in Table 1. The mean age of study participants was 15.1 ± 1.8 years. Half of the sample was male (51.7%) and of White ethnoracial background (52.5%). Participants who met the physical activity, screen time, and sleep duration recommendations represented 21.3%, 33.8%, and 32.4% of the sample, respectively. We found that only 4.7% of participants met all 3 recommendations, whereas 38.9% met none of the recommendations.
Descriptive Characteristics of the Sample.
CFA and Internal Consistency
Results from the CFAs for 3 competing models are presented in Table 2. Model 1 had all 6 items loading on a single factor of psychological distress (Figure 1), whereas Model 2 had the 6 items loading on 2 correlated first-order constructs of anxiety and depression (Figure 2). Model 3 had 2 factors of anxiety and depression that have a second-order structure representing psychological distress (Supplemental Figure 1). While most of the indices were acceptable for Model 1, it showed a slightly high RMSEA value of 0.065. However, compared to the single factor model, the 2-factor model was a better fit to the data, as defined in the Methods section (RMSEA = 0.041; CFI = 0.995; TLI = 0.991; SRMR = 0.018). The model fit indices of the second-order 2-factor model (Model 3) of psychological distress indicated poor fit to the data. Therefore, the 2-factor model (Model 2) was retained for subsequent analyses. The anxiety and depression items demonstrated a Raykov composite reliability of 0.80 and 0.92, respectively, indicating a high level of internal consistency.
Confirmatory Factor Analysis Model Fit Indices.
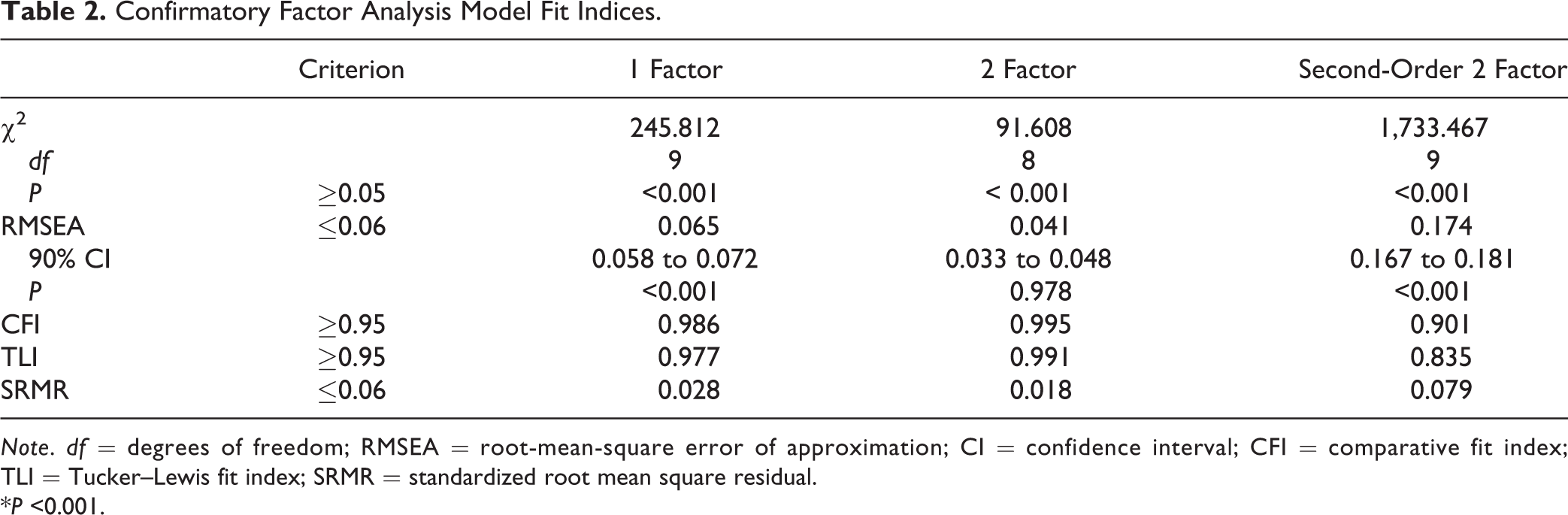
Note. df = degrees of freedom; RMSEA = root-mean-square error of approximation; CI = confidence interval; CFI = comparative fit index; TLI = Tucker–Lewis fit index; SRMR = standardized root mean square residual.
*P <0.001.
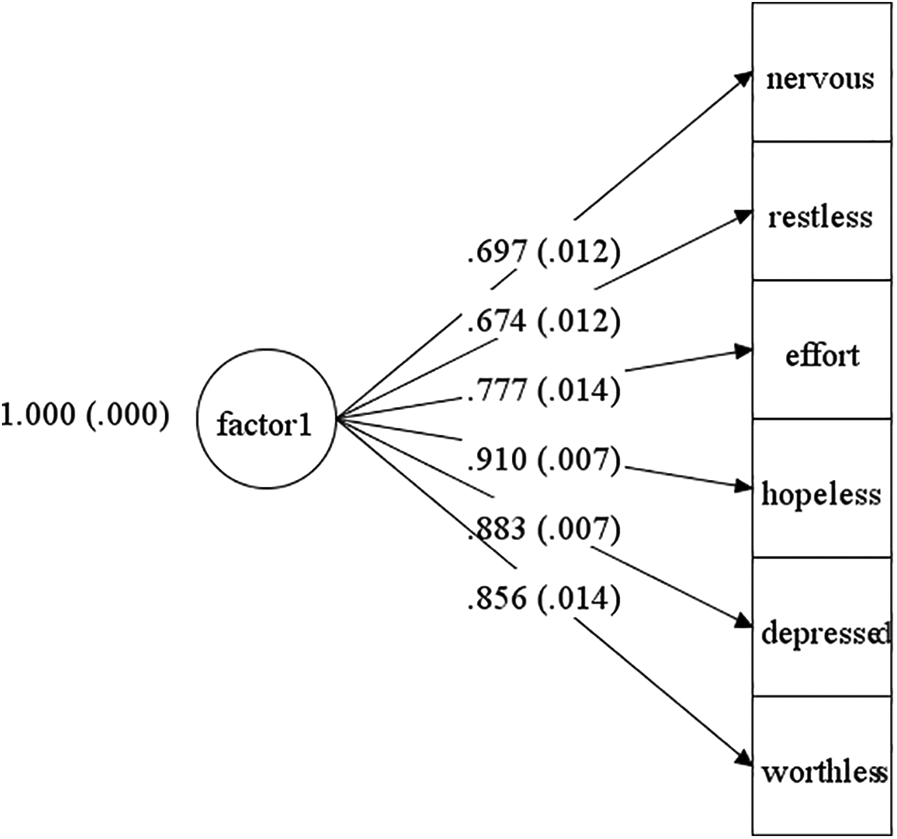
Confirmatory factor analysis of 1-factor model of psychological distress. Note. N = 6,364. Factor 1 = psychological distress.
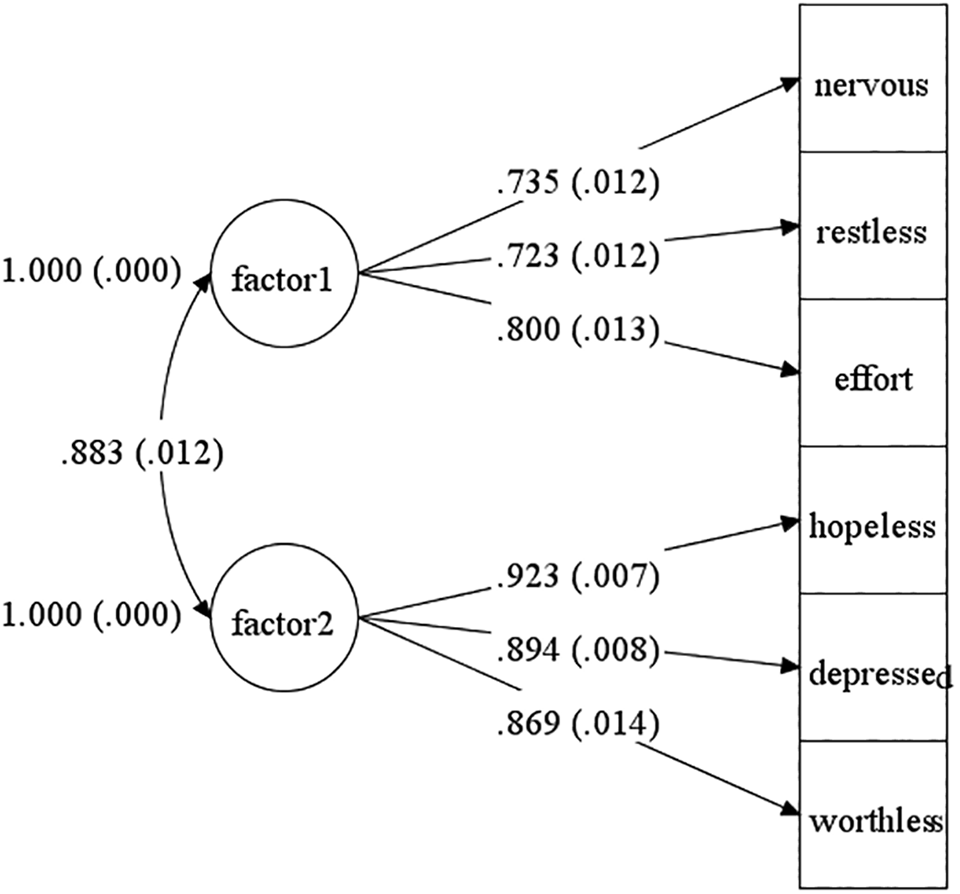
Confirmatory factor analysis of 2-factor model of depression and anxiety. Note. N = 6,364. Factor 1 = anxiety; Factor 2 = depression.
Meeting Different Movement Behavior Combinations with Anxiety and Depressive Symptoms
Results from structural equation modeling examining the associations of meeting different movement behavior combinations with constructs of anxiety and depression are outlined in Table 3. Meeting all 3 recommendations was associated with lower anxiety (β = −0.076; P = 0.028) and depressive symptoms (β = −0.067; P = 0.028) relative to meeting none. Meeting the sleep duration recommendation only (β = −0.135; P < 0.001), physical activity + sleep duration (β = −0.084; P = 0.001), and screen time + sleep duration (β = −0.157; P = 0.035) were associated with fewer symptoms of anxiety. Meeting all intermediate movement behavior combinations was also associated with fewer depressive symptoms, except meeting the physical activity only and the screen time only recommendations. Meeting the screen time + sleep duration recommendations had the strongest relationship with anxiety (β = −0.157; P < 0.001) and depressive symptoms (β = −0.139; P < 0.001), followed by meeting the sleep duration recommendation only for both anxiety (β = −0.135; P < 0.001) and depressive symptoms (β = −0.106; P < 0.001). Overall, any of the combinations that included meeting the sleep duration recommendation showed better mental health outcomes. The combinations that did not include meeting the sleep duration recommendation (e.g., physical activity only, screen time only, physical activity + screen time—except for depressive symptoms) were not associated with better mental health indicators.
Standardized Path Coefficients between Combinations of Movement Behavior Recommendations and Anxiety and Depressive Symptoms.
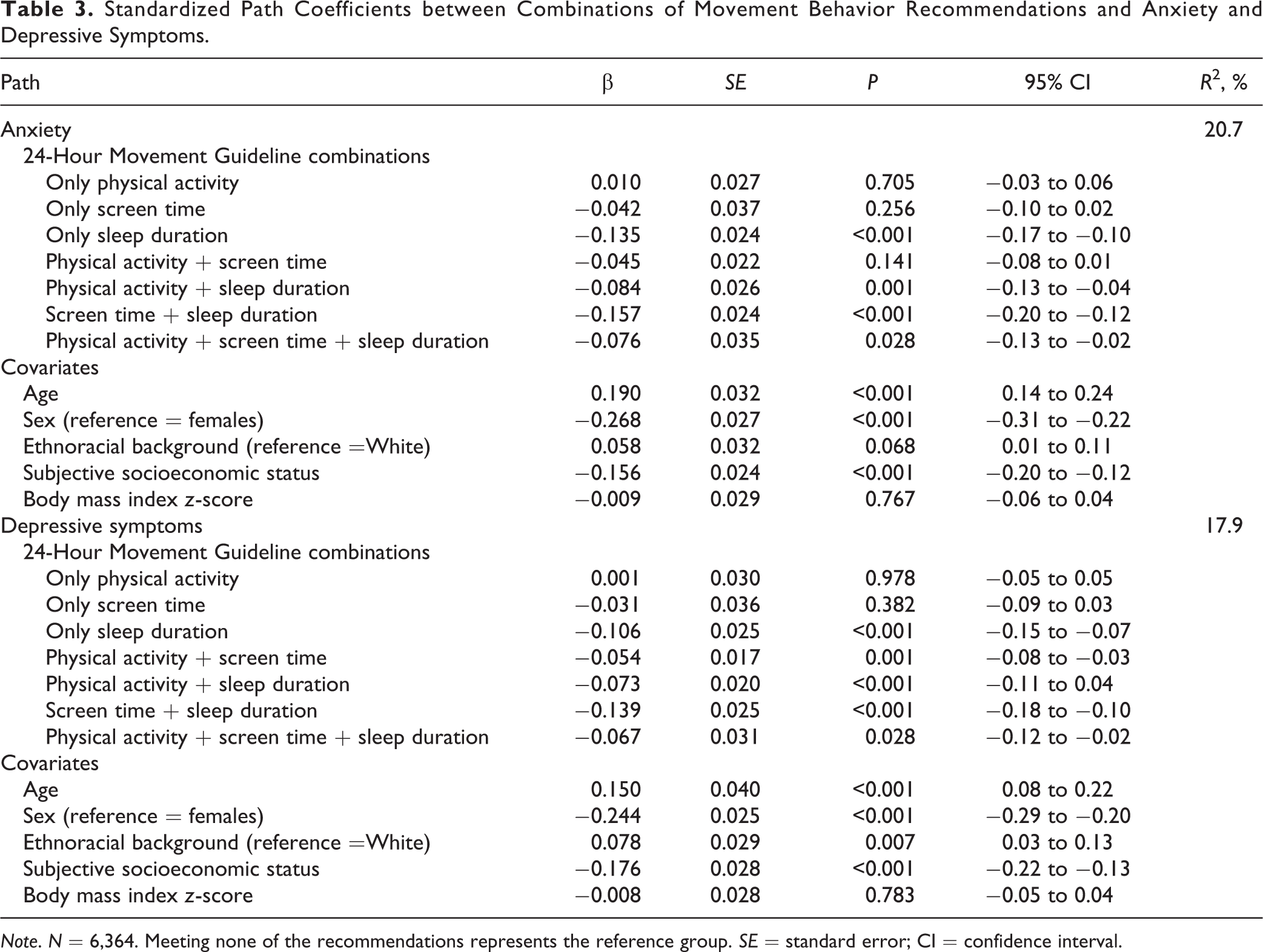
Note. N = 6,364. Meeting none of the recommendations represents the reference group. SE = standard error; CI = confidence interval.
Results of sensitivity analysis excluding students aged 18 to 20 years showed similar results (not shown).
Discussion
This study examined the association between meeting the 24-Hour Movement Guidelines and anxiety and depressive symptoms, as measured by the K6 in a province-wide representative sample of Canadian students in Grades 7 through 12. In order to achieve this objective, we first confirmed the factor structure of the K6 Psychological Distress Scale. Our analysis suggested a 2-dimensional structure of the K6 that assesses symptoms of depression and anxiety. We found that after adjusting for confounders, meeting all 3 movement behavior recommendations was associated with lower anxiety and depressive symptoms. However, this association appeared to be mainly driven by meeting the sleep duration recommendation, and to a lesser extent recommendation for screen time + sleep duration. Meeting the sleep duration recommendation alone was as beneficial for the outcomes as meeting all 3 recommendations (i.e., getting sufficient sleep + sufficient physical activity + low screen time).
Our results are consistent with previous studies that showed that meeting all 3 movement behavior recommendations is associated with lower risk of depressive symptoms. In a large and nationally representative sample of nearly 60,000 U.S. adolescents from the 2011 to 2017 cycles of the Youth Risk Behavior Surveillance Survey, Knell et al. 36 found that meeting all 3 movement behavior recommendations was associated with lower odds of depressive symptoms among adolescents. Similarly, Pearson et al. 37 found that meeting all 3 movement behavior recommendations was associated with lower odds of depressive symptoms in a sample of nearly 4,000 UK adolescents. These findings are in line with compelling evidence that accumulating sufficient physical activity, 38 limiting recreational screen time, 39 and getting enough sleep 40 are beneficially associated with a variety of physical, mental, and social health indicators among school-aged children and youth and provide further support to the 24-Hour Guidelines.
Previous studies have mostly examined the relationship between meeting all 3 recommendations only and depressive symptoms, whereas it is uncertain whether meeting a particular combination would be more strongly associated with depressive symptoms than others. There is only 1 study (by Zhu et al. 41 ) we are aware of that has examined the relationship between different combinations of movement behavior recommendations with anxiety and depressive symptoms among adolescents. Indeed, Zhu et al. 41 found that meeting all 3 recommendations was associated with significantly lower odds of depression and anxiety compared with meeting none of the recommendations among adolescents, which is consistent with our findings. They also found that meeting all 3 recommendations was always the best choice among adolescents compared to meeting any other combinations.
In contrast, our results showed that meeting the sleep duration recommendation, and to a lesser extent meeting the screen time + sleep duration recommendation, was as beneficial for the outcomes as meeting all 3 recommendations. Our findings are somewhat consistent with those of previous studies indicating that adherence to the screen time and sleep duration recommendations has generally more benefits for adolescent mental health than meeting the physical activity recommendation. Indeed, Walsh et al. 42 and Guerrero et al. 43 found that meeting the screen time and sleep duration recommendations was strongly associated with better cognitive function and less impulsivity in a representative sample of U.S. children, respectively, while physical activity was not. It is possible that other types of physical activity not measured in the OSDUHS nor the ABCD, such light physical activity be favorably associated with mental health outcomes. Regardless, physical activity should not be neglected, as it has proven to offer a variety of benefits on adolescent physical, mental, and social health. 38 Furthermore, previous evidence has shown that physical activity may prevent depression and/or alleviate its symptoms in children and adolescents. 44 –46 Given that excessive screen time, particularly around bedtime, has been identified as an important contributor to short sleep duration among adolescents, 47,48 it is important to address both screen time and sleep duration for mental health benefits. Future research, particularly from longitudinal studies, is needed to disentangle these findings and to confirm whether getting enough sleep would result in subsequent better mental health.
Sleep duration is the behavior that plays a bigger role in this study. This not surprising because sleep is well known as an essential component of healthy development and is required for optimal physical and mental health. 49 Several possible mechanisms could explain the associations of sleep duration with anxiety and depressive symptoms. Short sleep duration affects brain activity and neurochemicals that regulate mood and thinking. 50 It is associated with greater stress reactivity within the hypothalamic–pituitary–adrenal axis, thus increasing the risk of psychopathological disorder. 51 Finally, it can make the maintenance of a healthy lifestyle, such as physical activity, more difficult because of subsequent daytime sleepiness, fatigue, and tiredness. 52,53
With regard to distress, although K6 consistently showed very good reliability (as measured by Cronbach’s α) when treated as a simple continuous scale, 4,23 our results showed that a 2-factor model (representing anxiety and depressive symptoms) of the K6 had a better fit. These findings are consistent with previous studies indicating that a 2-factor model representing anxiety and depression fit the data best in young adults 27 and older adults. 54 The screening information derived from the 2-factor structure allows one to ascertain whether anxiety and/or depressive symptoms are elevated, thus providing richer information to guide intervention efforts compared to its traditional use as a continuous score of distress.
Strengths and Limitations
Strengths of this study include the use of a large and representative sample of adolescents and an assessment of the factor structure of the K6. While others have treated the K6 as a single scale as originally designed, our results showed that a 2-factor model (representing anxiety and depression) of the K6 fit the data better in our sample, information that is important to guide intervention strategies. Our study also highlights the importance of assessing different combinations of recommendations within the 24-Hour Movement Guidelines, whereas previous studies examining the relationship between meeting the 24-Hour Movement Guidelines and depressive symptoms among adolescents have mainly included meeting all 3 movement recommendations. 36,37 Finally, this study included a comprehensive set of covariates that statistically controlled for several confounding variables, strengthening the internal validity of the findings.
Our study has several limitations that should be recognized. First, the study is based on cross-sectional data and thus the temporal order of meeting the 24-Hour Movement Guidelines and psychological distress cannot be determined. It is possible that anxiety and depressive symptoms may have preceded movement behaviors rather than the reverse. Longitudinal studies are necessary to confirm temporality. Second, analyses are based on self-reported measures, thus subject to desirability and recall biases. Third, this study could not examine whether the observed associations varied with the severity of anxiety and depressive symptoms. This is an interesting research question that future research could answer. Fourth, it is worth mentioning that K6 measures anxiety and depressive symptoms, and it is not indicative of a diagnosed mental health disorder. Although they may indicate risk of a common mental disorder, 23 future research using diagnosed mental disorders is needed to examine the role of different combinations of movement behaviors. Finally, the possibility of residual confounding by unmeasured variable such as medication utilization that could influence both sleep duration and anxiety and depressive symptoms is not excluded.
Conclusion
To the best of our knowledge, this study is among the first to demonstrate that meeting the 24-Hour Movement Guidelines is associated with lower anxiety and depressive symptoms among adolescents. Our results further indicate that meeting the sleep duration recommendation could be the main driver of this association and to a lesser extent meeting the screen time + sleep duration guidelines. Our findings provide further support for heightened efforts to encourage adolescents to meet these guidelines, particularly to get adequate sleep as a possible means to promote adolescent mental health. It is important to intervene during adolescence because it is when many mental disorders emerge for the first time. 55 Further research using a longitudinal design is needed to confirm temporality and to elucidate the mechanisms linking sleep duration to mental health of adolescents. Future studies are also needed to confirm the validity of the 2- factor structure of the K6 in large and representative samples of youth.
Supplemental Material
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720970863 - The Canadian 24-Hour Movement Guidelines and Psychological Distress among Adolescents: Les Directives canadiennes en matière de mouvement sur 24 heures et la détresse psychologique chez les adolescents
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720970863 for The Canadian 24-Hour Movement Guidelines and Psychological Distress among Adolescents: Les Directives canadiennes en matière de mouvement sur 24 heures et la détresse psychologique chez les adolescents by Hugues Sampasa-Kanyinga, Jean-Philippe Chaput, Gary S. Goldfield, Ian Janssen, JianLi Wang, Hayley A. Hamilton, Mark A. Ferro and Ian Colman in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
This research paper was partly supported by the Research Council of Norway through its Centres of Excellence funding scheme, project number 262700 for Ian Colman. Ian Colman, Ian Janssen, and Mark Ferro are funded by the Canada Research Chairs Program. The funders were not involved in study design; collection, analysis, and interpretation of data; writing the report; or the decision to submit the report for publication. Our data cannot be made available in the manuscript, the supplemental files or a public repository due to the Centre for Addiction and Mental Health’s and The Ontario Public and Catholic School Board’s institutional Research Ethics Board agreements. Qualified, interested researchers may request access to the data at the Centre for Addiction and Mental Health.
Acknowledgments
The Ontario Student Drug Use and Health Survey, a Centre for Addiction and Mental Health initiative, was funded in part through ongoing support from the Ontario Ministry of Health and Long-Term Care, as well as targeted funding from several provincial agencies. The authors also would like to thank Dr. Michelle Guerrero for her assistance with the statistical analyses.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mark Ferro and JianLi Wang serve on the editorial board of the Canadian Journal of Psychiatry. The remaining authors have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research paper was partly supported by the Research Council of Norway through its Centres of Excellence funding scheme, project number 262700 for Ian Colman. Ian Colman, Ian Janssen, and Mark Ferro are funded by the Canada Research Chairs Program.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.