
Abstract
Objective:
Parental psychopathology is a significant risk factor for mental health challenges in offspring, but the nature and magnitude of this link in Indigenous Peoples is not well understood. This systematic review examined the emotional and behavioral functioning of the offspring of Indigenous parents with mental health challenges.
Method:
We searched MEDLINE, EMBASE, PsycINFO, CINAHL, and Web of Science from their inceptions until April 2020. Studies were included if they included assessments of emotional, behavioral, or other psychological outcomes in the offspring of Indigenous parents with a mental health challenge.
Results:
The 14 studies eligible for review were focused on parental substance misuse (n = 8), maternal internalizing (i.e., depression, anxiety) issues (n = 5), and poor overall parental mental health (n = 4). In 11 studies, parental substance misuse, depression, and/or overall mental health challenges were associated with 2 to 4 times the odds of offspring externalizing and internalizing behaviors as compared to offspring of Indigenous parents without mental health challenges.
Conclusion:
The findings suggest higher risks of mental health challenges among offspring of Indigenous parents with psychiatric difficulties than among Indigenous children of parents without similar difficulties. Knowledge of these phenomena would be improved by the use of larger, more representative samples, culturally appropriate measures, and the engagement of Indigenous communities. Future studies should be focused on both risk and resilience mechanisms so that cycles of transmission can be interrupted and resources aimed at detection, prevention, and treatment optimally allocated.
Introduction
The presence of mental health challenges in a parent increases the risk of offspring mental health challenges by up to 5 times, one of the most potent risks known. 1 –5 When parents are successfully treated, rates of mental disorders in offspring decrease, 6 highlighting the importance of detection and treatment in interrupting the intergenerational transmission of psychopathology.
The rearing environment plays an important role in this transmission. Those facing structural barriers such as institutionalized racism, poor access to health care, and forced dislocation to areas with minimal food availability, crowded housing, and inadequate transportation infrastructure can be more profoundly impacted by these social origins of disease than those not exposed. Indigenous Peoples, the original owners and inhabitants of their lands with diverse cultures within and across country borders, often face structural disadvantages due to the shared impact of historic and ongoing colonization and oppression. 7 –10 This trauma differs from typical trauma because it is colonial in nature, transgenerational, and cumulative due to current systematic barriers and structural racism. 11
Intergenerational colonial trauma and violence has caused patterns of land dislocation, institutionalization, and cultural erasure contributing toward Indigenous identity loss, breakdown of family units, historical trauma, and ultimately poor mental health outcomes. 11 –16 The intergenerational transmission of mental health challenges may be mediated by epigenetic changes, alterations occurring in gene expression that take place without changes in the underlying DNA sequenece. 17,18 For instance, parental stress and trauma are associated with a downregulation of glucocorticoid receptor genes, those implicated in the stress response in offspring. 17,19
Synthesizing the literature on the children of Indigenous parents with mental health challenges can enable a better understanding of the challenges facing Indigenous youth, as well as optimizing screening processes, identifying challenges at an early age, and guiding the development of targeted family interventions. It can also help us understand the degree to which Indigenous research methodologies are applied. Contemporary researchers need to safeguard against questions and methodologies that have been developed and utilized in the absence of input by Indigenous communities as these threaten to perpetuate colonial systems. 12,19 Indigenous research priorities and input need to be valued, honored, and protected. 20 Given this background, the aim of this systematic review was to examine emotional and behavioral functioning in the offspring of Indigenous parents with mental health challenges.
We would like to thank Mr. Troy Hill who is Mohawk from Six Nations of the Grand River Territory where he is an educator and Dr. Jacob Burack for sharing his learning and experiences collaborating with educators, students, and community leaders of the Naskapi Nation of Kawawachikamach. This article was written on the traditional territories of the Haudenosaunee and Mississaugas of the Credit First Nations and is within the lands protected by the “Dish with One Spoon” Wampum agreement.
Method
Search Strategy
The study protocol guiding this systematic review was published on January 25, 2019, and is available online through PROSPERO (2019 CRD42019121301). Guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Meta-Analysis of Observational Studies in Epidemiology (MOOSE) statements were followed. 21,22
A systematic search of electronic databases (MEDLINE, EMBASE, PsycINFO, CINAHL, Web of Science) was conducted from their inceptions until April 15, 2020. Searches were developed in collaboration with a health sciences librarian (please see Supplementary Files for our complete search strategies). The reference lists of relevant articles were hand-searched.
Eligibility Criteria
Studies were included if (1) ≥1 Indigenous parent(s) had symptoms of a mental health challenge(s); (2) offspring of Indigenous parents were 0 to 18 years old; and (3) offspring emotional, behavioral, and/or other psychological outcomes were reported.
Since self-identification and the right for self-determination is central to the concept of Indigeneity, and because definitions are frequently entrenched in a colonial framework, we identified Indigenous Peoples as those who have roots to traditional lands prior to colonization and distinct cultural norms from the dominant’s society. 23,24 Notwithstanding the significant heterogeneity in lived experiences, many Indigenous Peoples from around the world share a collective history of colonization, forced removal from land, and systematic oppression which result in common health and social inequities. 7,25 –28 Examining Indigenous groups sharing these experiences helps us to draw conclusions regarding similarities between Indigenous Peoples. We recognize that some past terms used to describe Indigenous Peoples (e.g., Indians, Natives, Aboriginal) are currently considered disrespectful. However, if a term was used to identify Indigenous Peoples in a specific study, we continued to use that term to honor the self-identification and self-determination of the participating Indigenous Peoples. 24
Data Extraction and Methodological Bias Assessment
Two independent reviewers (MF, HZ) screened abstracts and titles, and any disagreements were adjudicated by a third reviewer (SO). The data extraction file containing information on the studies’ methods, outcomes, measures used, Indigenous population, and parental mental health challenges was piloted with 5 randomly selected studies.
Study methodological bias was assessed using National Institutes of Health Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies and the Newcastle-Ottawa Quality Assessment Scale (NOS). 29,30 The first (used for studies without a comparison group) grades the design, sample size, outcome measurement, and statistical analyses with overall study quality rated as Good/Fair/Poor. The NOS is used when observational studies include a comparison group and grades selection, comparability, and outcome bias using a star system (more stars correspond to higher methodological quality/lower the risk of bias).
Results
Search Results
Our search strategy identified 4,105 potentially relevant articles with 2,341 articles remaining after duplicate removal. Of these, 56 were taken to full-text. Thirteen met our inclusion criteria and one more was found through hand-searching (total = 14). The interrater reliability was substantial (κ = 0.68). 31 All included articles were available in English. See Figure 1 for the PRISMA flowchart outlining the search process.
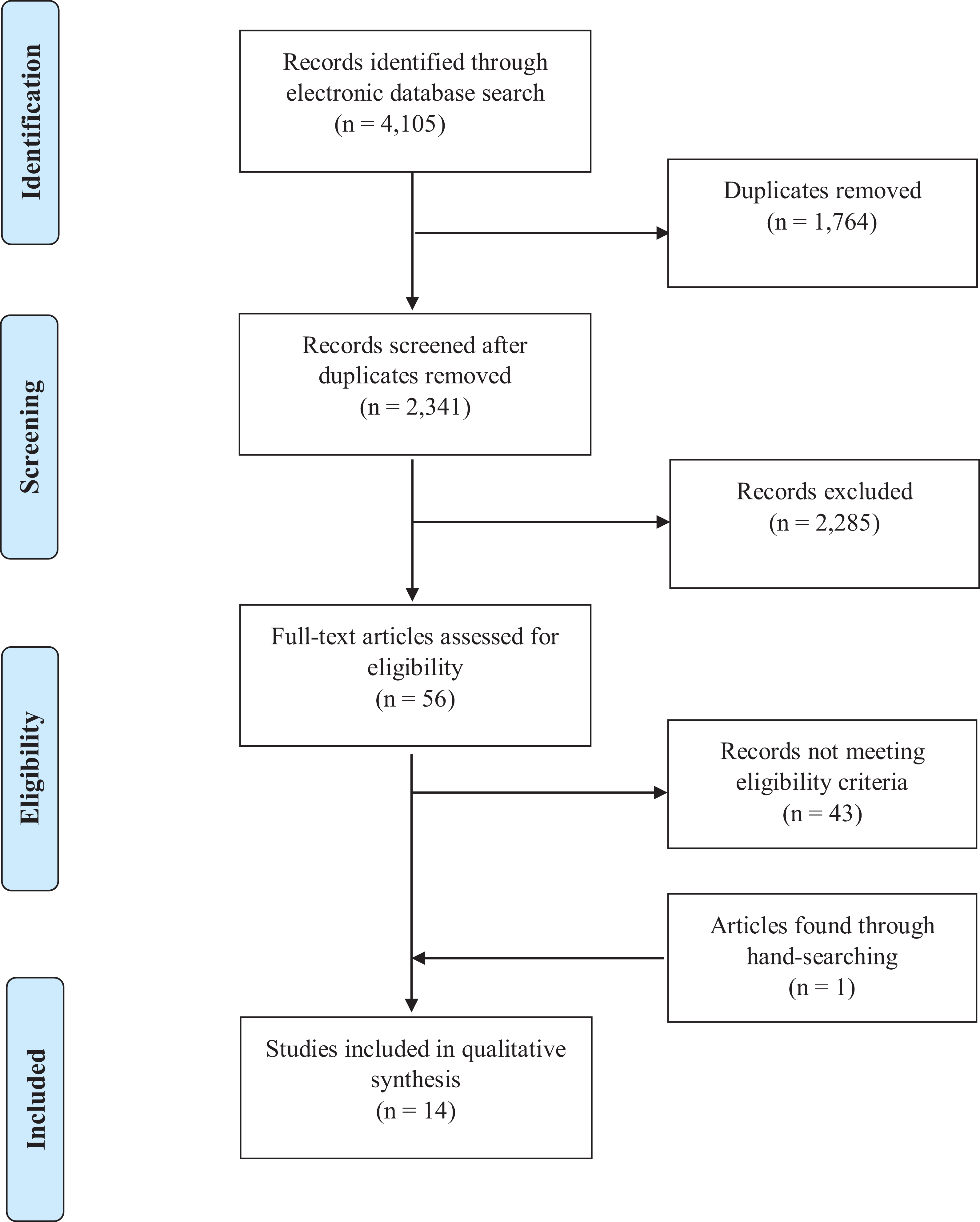
Flowchart displaying the number of articles identified, screened, deemed eligible, and included in the systematic review and meta-analysis.
Characteristics of Included Studies
Only 2 studies included a non-Indigenous comparison group, and the outcome measures differed between them. 32,33 As a result, we were unable to meta-analyze relative rates of mental health challenges in the offspring of Indigenous parents with mental health challenges and offspring of non-Indigenous mothers and/or fathers with similar issues. Since the other 12 studies did not contain a non-Indigenous comparison group, meta-analysis was also not possible, and so a narrative synthesis of all 14 studies is provided below.
Participant characteristics
A total of 7,557 offspring were included; 6,486 of which were Indigenous. Offspring ranged in age from 0 to 18 years. Parental Indigeneity was identified in different ways across studies. In 7 studies, parents had to identify as members of a specific tribe/Nation, or live on or near a reserve/reservation. 32,34 –39 A reserve (reservation in the USA) is a tract of land that is specifically for use by Indigenous Peoples as governed by historical treaty rights. 24 In 3 studies, parents self-identified as Indigenous. 40 –42 In 2 studies, participants were recruited from health services that specifically provided care to Indigenous groups. 43,44 In the remaining 2 studies, parental Indigeneity was determined through offspring self-identification. 33,45 Tables 1, 2, and 3 contain descriptions of included studies, categorized by parental mental health challenge (i.e., poor parental mental health [broadly defined], parental substance misuse, and maternal internalizing issues and arranged in ascending order of offspring age [youngest to oldest] with studies containing non-Indigenous comparison groups being listed first).
Characteristics of Studies that Examined Poor Parental Mental Health (Broadly Defined) and Offspring Psychopathology.
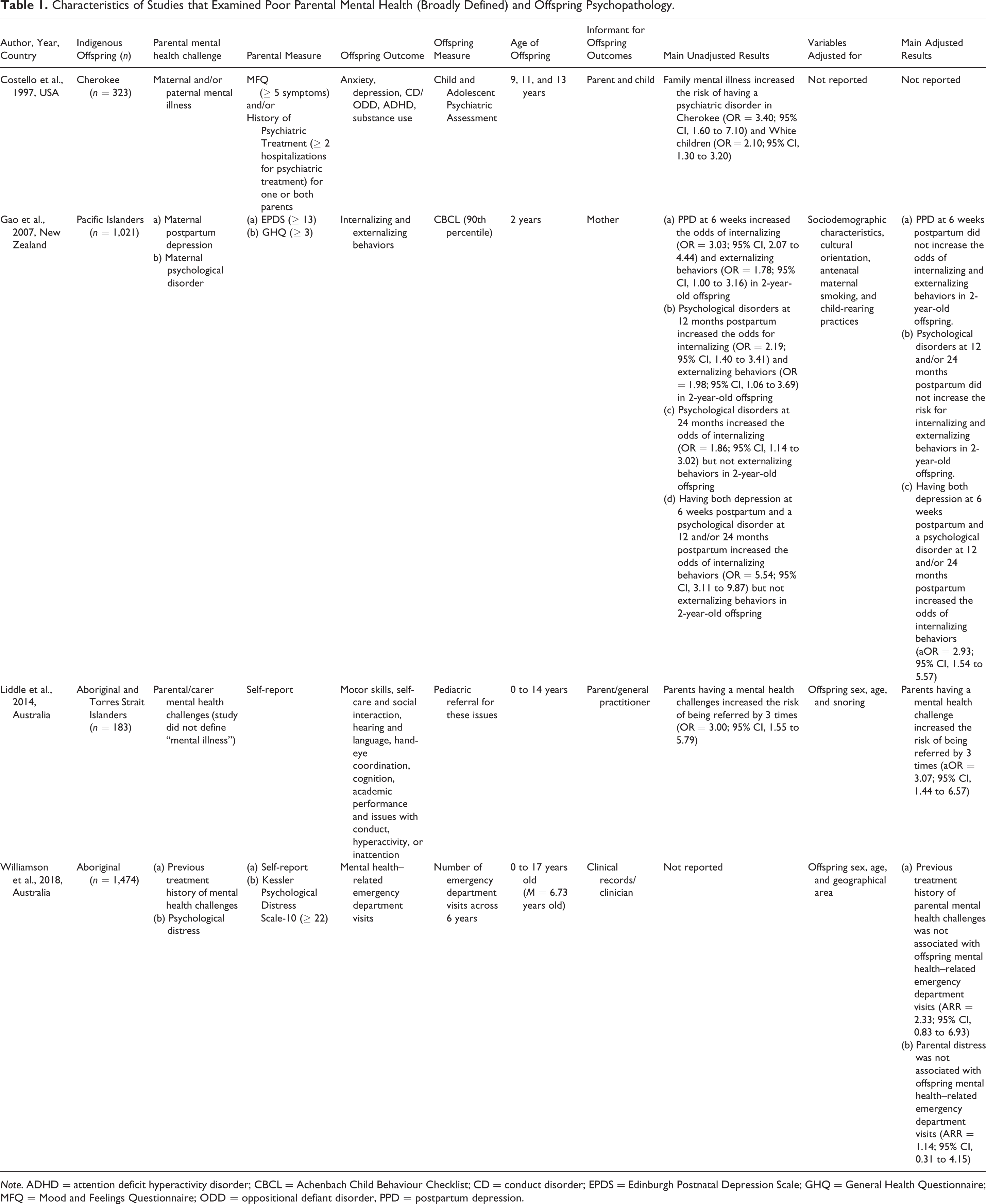
Note. ADHD = attention deficit hyperactivity disorder; CBCL = Achenbach Child Behaviour Checklist; CD = conduct disorder; EPDS = Edinburgh Postnatal Depression Scale; GHQ = General Health Questionnaire; MFQ = Mood and Feelings Questionnaire; ODD = oppositional defiant disorder, PPD = postpartum depression.
Characteristics of Studies that Examined Parental Substance Misuse and Offspring Psychopathology.
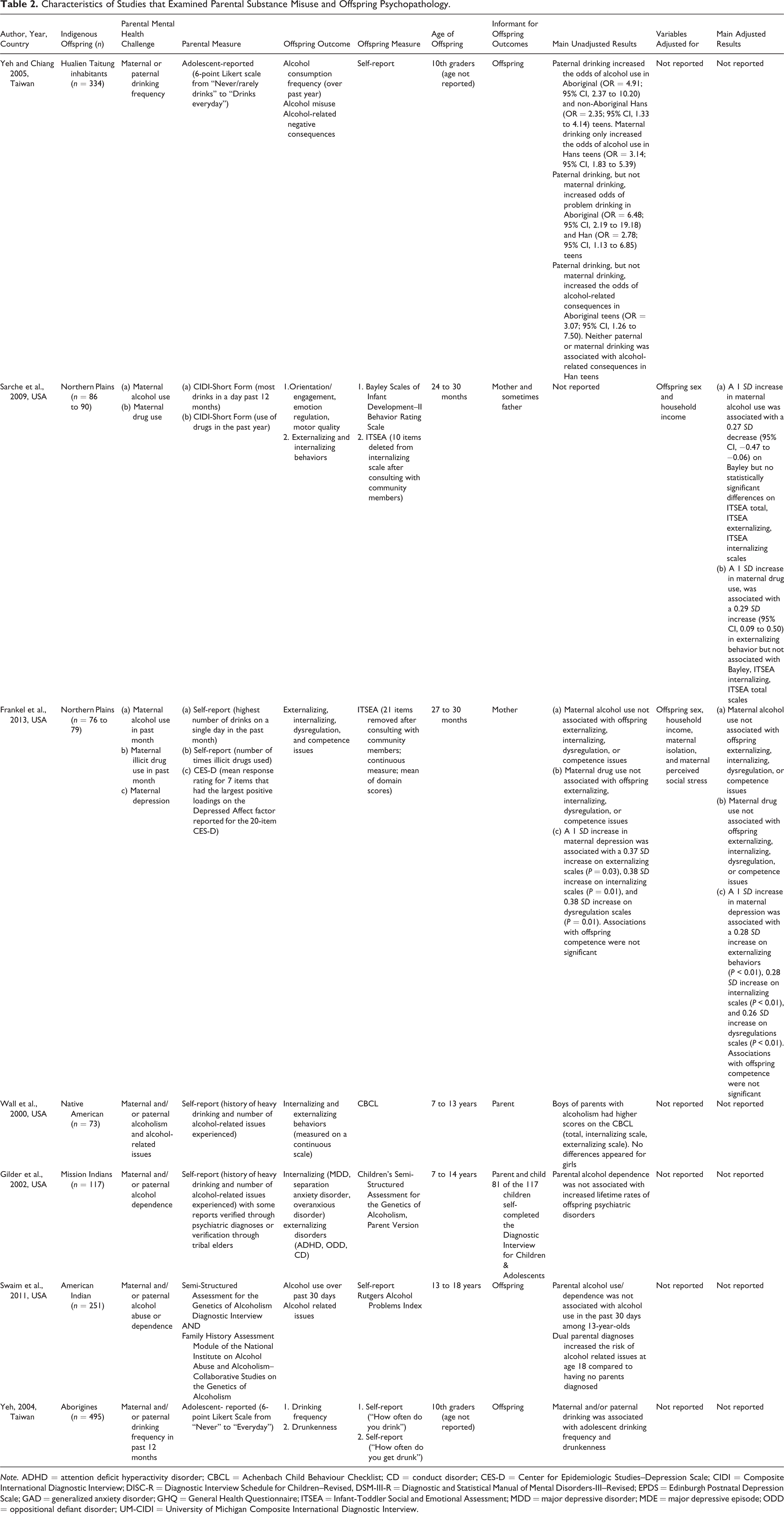
Note. ADHD = attention deficit hyperactivity disorder; CBCL = Achenbach Child Behaviour Checklist; CD = conduct disorder; CES-D = Center for Epidemiologic Studies–Depression Scale; CIDI = Composite International Diagnostic Interview; DISC-R = Diagnostic Interview Schedule for Children–Revised, DSM-III-R = Diagnostic and Statistical Manual of Mental Disorders-III–Revised; EPDS = Edinburgh Postnatal Depression Scale; GAD = generalized anxiety disorder; GHQ = General Health Questionnaire; ITSEA = Infant-Toddler Social and Emotional Assessment; MDD = major depressive disorder; MDE = major depressive episode; ODD = oppositional defiant disorder; UM-CIDI = University of Michigan Composite International Diagnostic Interview.
Characteristics of Studies that Examined Maternal Internalizing Issues and Offspring Psychopathology.
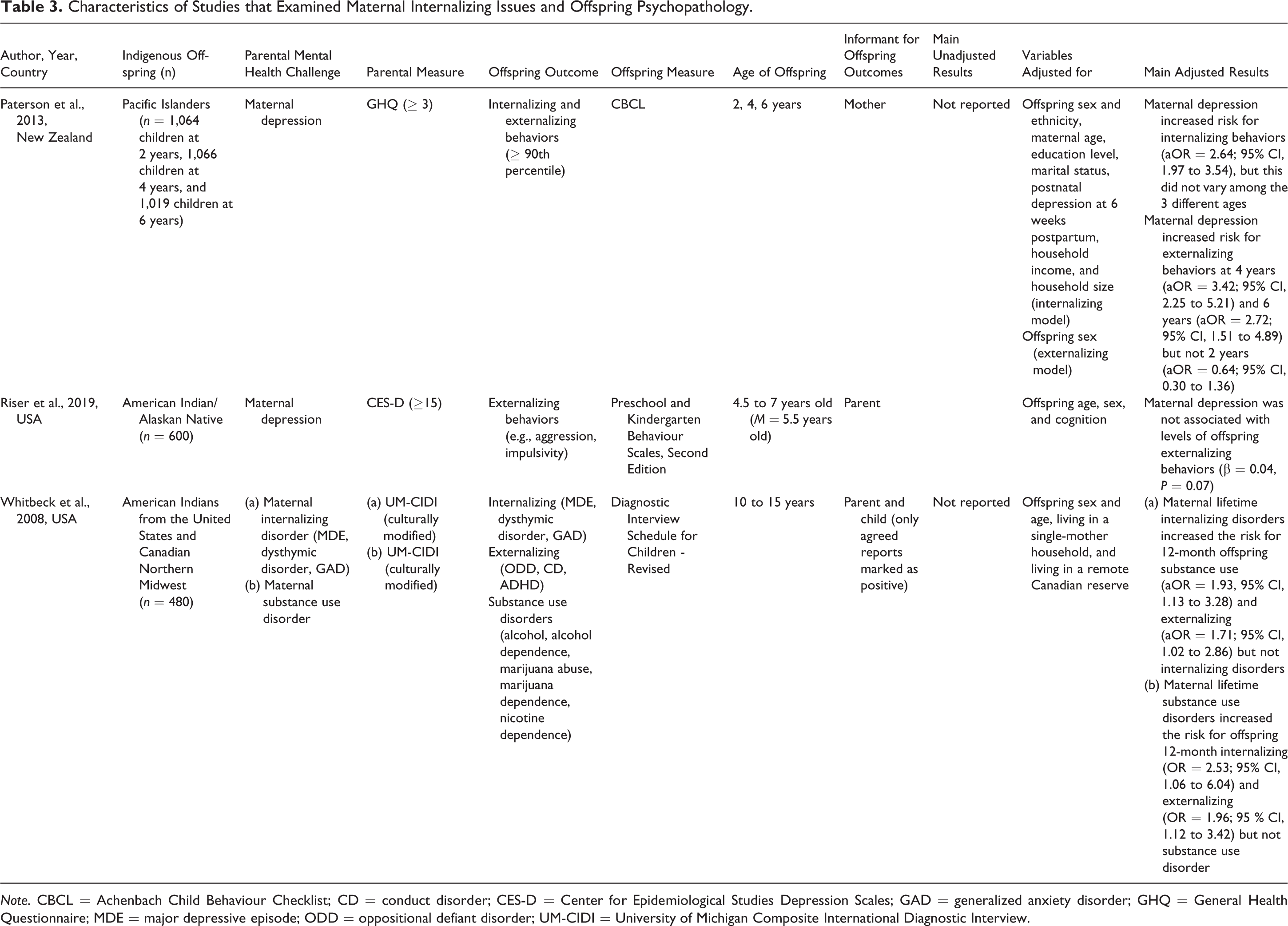
Note. CBCL = Achenbach Child Behaviour Checklist; CD = conduct disorder; CES-D = Center for Epidemiological Studies Depression Scales; GAD = generalized anxiety disorder; GHQ = General Health Questionnaire; MDE = major depressive episode; ODD = oppositional defiant disorder; UM-CIDI = University of Michigan Composite International Diagnostic Interview.
Study characteristics
Seven studies were conducted in the United States, 32,34 –38,42 and 2 each in Taiwan, 33,45 New Zealand, 40,41 and Australia. 43,44 One included Indigenous groups from Canada and the United States. 39
Five studies included measurements of both maternal and paternal mental health, 32,33,36 –38 6 of maternal mental health only, 34,35,39 –42 and 3 studies did not specify whether parental mental health was that of mothers, fathers, or both. 43 –45
The most common parental mental health problem examined was substance misuse (n = 8) including alcohol use by ≥1 parent(s), 33,36 –38,45 maternal drug use, 34,35,39 and maternal alcohol use. 34,35 Five studies included assessments of maternal internalizing issues, with maternal depression being measured in 4, 35,40 –42 and maternal depressive episodes, dysthymic disorder, or generalized anxiety disorder in the other. 39 Four studies were focused on poor parental mental health (more broadly defined). 32,41,43,44
Parental mental health was assessed in 3 studies using structured clinical interviews, 34,38,39 while the remainder utilized questionnaires or other self-report methods. The clinical interviews included the Composite International Diagnostic Interview (CIDI) 34,39 and the Semi-Structured Assessment for the Genetics of Alcoholism Diagnostic Interview. 38 Questionnaires used most commonly included the Edinburgh Postnatal Depression Scale (EPDS), General Health Questionnaire (GHQ), Center for Epidemiologic Studies–Depression (CES-D), and the Mood and Feelings Questionnaire (MFQ).
Internalizing and externalizing behaviors in offspring were examined in all 14 studies. These were assessed in 9 studies using questionnaires, 3 used structured interviews, and 2 used clinical records. Specifically, 3 studies used the Child Behaviour Checklist (CBCL) 36,40,41 or another self-report measure (please see Table 1 for full details), 33,38,45 and 2 utilized the Infant Toddler Socioemotional Assessment (ITSEA). 34,35 One study each included the Child and Adolescent Psychiatric Assessment, 32 Diagnostic Interview Schedule for Children–Revised, 39 Children’s Semi-Structured Assessment for the Genetics of Alcoholism, Parent Version, 37 Preschool and Kindergarten Behavior Scales, Second Edition, 42 pediatric referrals for offspring behavior and socioemotional issues, 43 and mental health related-emergency department visits. 44 Sarche et al. also measured orientation/engagement, emotion regulation, and motor quality using the Behavior Rating Scale of the Bayley Scales of Infant Development–II.
Six of the 14 studies included a culturally modified measure of offspring outcomes and/or consulted community members to ensure their questionnaire and/or interview protocols were culturally appropriate. 34,35,39 –41,44 Most often, the measures were modified by removing questions that were deemed to be offensive, part of regular Indigenous infant development, or thought to potentially cause confusion in respondents.
Study Methodological Bias
Using the National Institutes of Health Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies, 3 studies were rated as “Good,” 35,39,44 6 studies were rated as “Fair,” 34,38,40 –42,45 and 3 studies were rated as “Poor.” 36,37,43 The most common factor increasing the risk of bias was outcome assessors not being blinded to exposure status (i.e., clinical status of parents). The 2 other studies assessed using the NOS were found to have a low 32 and high risk of bias. 33 Tables 4 and 5 contain descriptions of the risk of methodological bias across the 14 studies.
Study Methodological Bias Assessment Using the National Institutes of Health Quality Assessment Tool for Observational Cohort and Cross-sectional Studies.
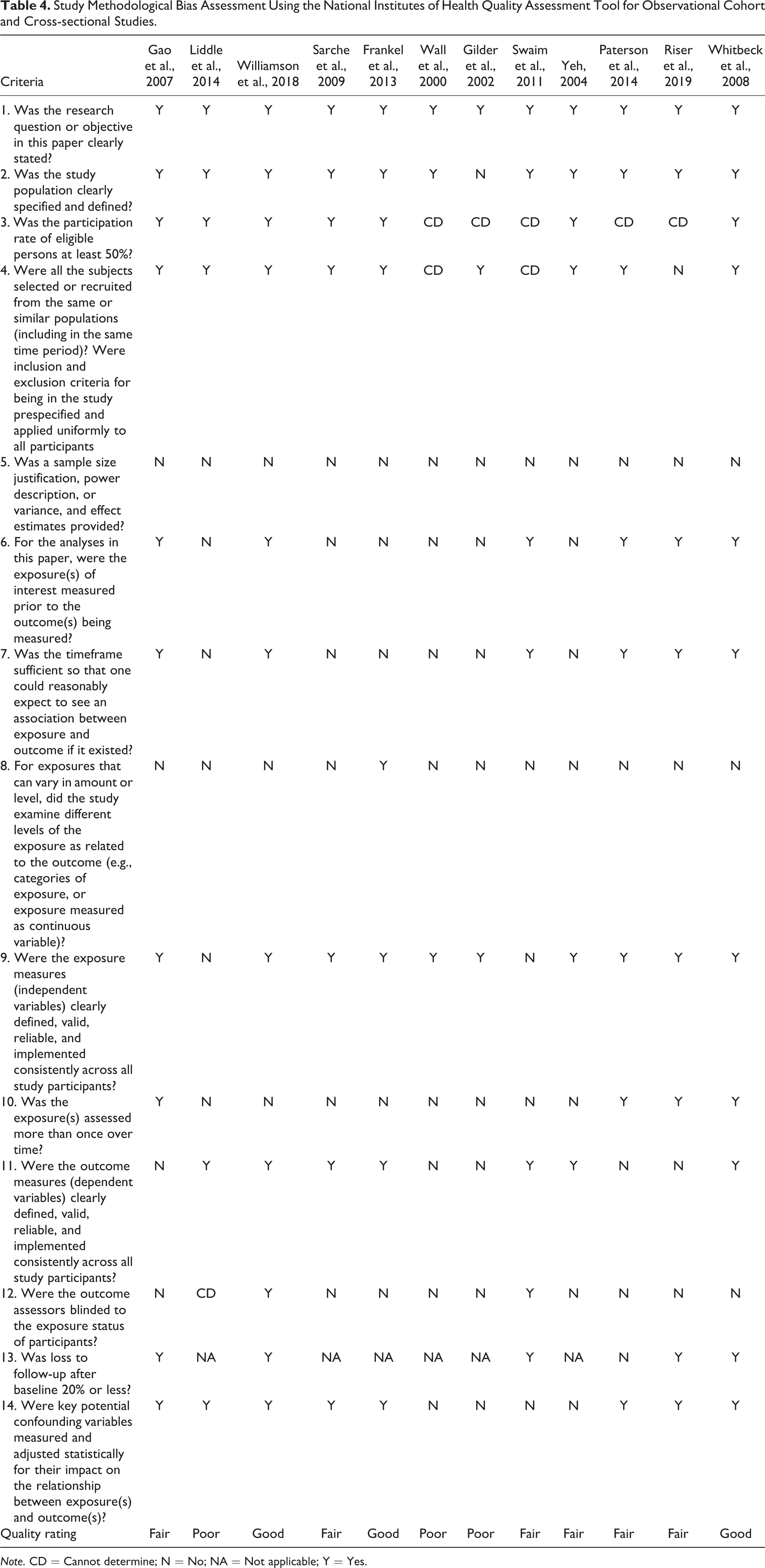
Note. CD = Cannot determine; N = No; NA = Not applicable; Y = Yes.
Study Methodological Bias Assessment Using the Newcastle-Ottawa Quality Assessment Scale.

Note. The asterisks represent ‘Yes’.
Narrative Synthesis of Results
Unadjusted results were reported for 6 of the studies, results adjusted for covariates were reported for 5 of the studies, and both unadjusted and adjusted estimates were reported in the other 3 studies. We report adjusted results below, but in the absence of such data, we report unadjusted findings.
Overall Parental Mental Health (Broadly Defined)
The overall mental health of parents was examined in 4 studies, with an association between poor overall parental mental health and offspring psychopathology identified in 2. Costello et al. examined 3-month prevalence rates of anxiety, depression, oppositional, and attention deficit/hyperactivity disorder using parent and child reports for Indigenous (n = 323) and non-Indigenous youth (n = 933) living in North Carolina. They found that if one or both Indigenous parents were treated for a psychiatric disorder on ≥2 occasions and/or had a MFQ score ≥5, their offspring were over 3 times more likely to have a psychiatric disorder (OR = 3.40; 95% CI, 1.60 to 7.10) compared to Indigenous offspring of healthy parents. 32 Poor parental mental health also increased the risk for Caucasian offspring by 2-fold when compared to the Caucasian peers of parents without mental health challenges. While results are unadjusted, this study was rated to have a low risk of bias.
Liddle et al. conducted a cross-sectional examination of associations between parental self-reported mental health challenges and the prevalence of a pediatric specialist referral for developmental and/or behavioral issues in 183 Indigenous children living in Australia aged 0 to 14 years. 43 Those who had parents with mental health challenges were over 3 times more likely to be referred for behavioral issues, compared to the offspring of Indigenous parents with no self-reported mental health challenges. Although, this study should be interpreted with caution due to its high risk of bias. In contrast, in a study of associations between symptoms of a maternal psychiatric disorder (GHQ ≥ 3) at 12 and 24 months postpartum, and maternal reports of offspring behavior at 24 months postpartum using the CBCL (≥ 90th percentile), Gao et al. found no statistically significant links when maternal age, ethnicity, household income, prenatal cigarette exposure, marital status, and education level were adjusted (fair methodological risk of bias). 41 In a study rated to have a low risk of bias with 1,474 Aboriginal children aged 0 to 17 years old living in Australia, Williamson et al. found no associations between offspring mental health–related emergency department visits and prior parental treatment for mental health challenges or current parental distress when offspring age, sex, and geographical area were adjusted statistically. 44
Overall, poor overall parental mental health was associated with an increased risk of offspring psychopathology in 2 studies (one with a low risk of methodological bias, the other with a high risk of bias) and but not in 2 other studies (low to fair risk of bias).
Parental Substance Misuse
Eight studies examined parental substance misuse including drug and/or alcohol issues. Yeh and Chiang examined the influence of parental drinking on adolescent drinking frequency, drunkenness, and drinking-related problems among Han (non-Aboriginal) and Aboriginal 10th graders living in Taiwan. Paternal drinking increased the odds of alcohol use by almost 2-fold in the Aboriginal versus non-Aboriginal teens (OR = 1.90; 95% CI, 1.33 to 2.73). 33 Furthermore, paternal drinking increased the odds of problem drinking over 3-fold in the Aboriginal versus the non-Aboriginal teens (OR = 3.10; 95% CI, 1.91 to 5.20). 33 These results were unadjusted and the study was rated to have a high risk of bias.
In a study with 96 Mission Indian children aged 8 to 13 years living on or near one of the 6 reservations in California, Wall et al. examined the impact of excessive parental alcohol use on offspring behavior. In unadjusted analyses, 23% of Indigenous offspring had behavioral problems compared to 8% of children of healthy parents. Male, but not female offspring of Indigenous parents with excess alcohol use also scored higher on the internalizing, externalizing, and total behavior scales on the CBCL as compared to the Mission Indian children of parents engaging in healthy drinking patterns. This effect was particularly strong for paternal alcohol misuse. 36 In a cross-sectional study of the same group of Mission Indian children (n = 117), Gilder et al. examined the prevalence of psychiatric diagnoses among the offspring of parents with alcohol dependence. 37 Based on combined parent and child reports, parental alcohol dependence was not associated with an increased risk of any lifetime psychiatric disorder in these 7- to 14-year-olds. 37 Both studies were rated to have a high risk of bias.
Among 480 adolescents from Canada and the United States, Whitbeck et al. found that a lifetime substance use disorder in Indigenous mothers increased the odds for internalizing (aOR = 2.53; 95% CI, 1.06 to 6.04) and externalizing behaviors (aOR = 1.96; 95% CI, 1.12 to 3.42), but not substance use disorders in adolescents as compared to the offspring of Indigenous mothers without a substance use disorder. These findings were adjusted statistically for offspring sex, age, single parent status, and the experience of living in a remote location, and the study was rated to have a low risk of bias. 39
Sarche et al. conducted a cross-sectional study with 90 mother–children dyads from a Northern Plains reservation (fair study quality). Analyses adjusting for offspring sex and household income found that maternal alcohol use was associated with lower levels of offspring orientation/engagement, but not externalizing or internalizing behaviors in 2-year-olds. Furthermore, maternal drug use was associated with increased levels of symptoms of externalizing behaviors in 2-year-old children, but not orientation/engagement or internalizing behaviors. 34 In contrast, Frankel et al., rated to have a low risk of bias, examined associations between maternal alcohol or drug use and offspring emotional and behavioral difficulties among 79 toddlers from a Northern Plains reservation. They found that neither maternal alcohol use nor drug use was associated with levels of offspring internalizing, externalizing, dysregulation, or competence issues. 35
In a prospective cohort study with 251 American Indian teenagers, Swaim et al. found that when both parents had an alcoholism diagnosis, risk for alcohol-related problems in their 18-year-old children was increased, but that this was not associated with alcohol use in the past month among the 13-year-olds. 38 In a cross-sectional study, Yeh found that adolescent-reported maternal and/or paternal drinking was associated with self-reported adolescent drinking and drunkenness frequency in 495 Aboriginal children living in Taiwan. 45 Both were judged as having fair study quality. In sum, parental substance misuse was associated with offspring internalizing and externalizing behaviors in 6 studies but not in 2 others (one rated as high risk of bias).
Maternal Internalizing Issues
Associations between maternal internalizing issues (i.e., depression, dysthymia, or generalized anxiety disorder) and offspring socioemotional outcomes were examined in 5 studies. Frankel et al. conducted a cross-sectional study with 27- to 30-month-old Northern Plains (USA) toddlers using maternal reports of a culturally modified version of the ITSEA. Current maternal depression was associated with more offspring dysregulation, and internalizing and externalizing behaviors after adjusting for offspring sex, maternal isolation, stress, and negative social influences. 35 Similarly, in a study of over 1,000 mother–offspring dyads at 2, 4, and 6 years of age, and rated to have a fair study quality, Paterson et al. found that current maternal depression increased the odds of offspring internalizing behaviors by more than 2-fold when compared against children of asymptomatic Pacific Islander mothers. 40 Current maternal depression increased the odds of offspring externalizing behaviors in 4-year-olds (aOR = 3.42; 95% CI, 2.25 to 5.21) and 6-year-olds (aOR = 2.72; 95% CI 1.51 to 4.89), but not among 2-year-old children when compared to the offspring of Pacific Islander mothers without maternal depression. 40
Whitbeck et al. reported that lifetime maternal internalizing disorders (i.e., major depressive episode, dysthymic disorder, or generalized anxiety disorder), as assessed using a culturally modified version of the CIDI, increased the odds of a 12-month prevalence of externalizing and substance use disorders by nearly 2 times in 480 Indigenous youth living in Canada and American Northern Midwest when compared with adolescents of healthy Indigenous mothers. Offspring sex, age, living in a single-mother household, and living in a remote location were statistically adjusted and the study was rated to have a low risk of bias. 39 In contrast, Gao et al. found no association between maternal depression at 6 weeks postpartum (EPDS ≥ 13) and maternal reports of offspring internalizing and externalizing behaviors at 2 years of age using the CBCL when adjusting for maternal age, ethnicity, household income, prenatal exposure to cigarettes, marital status, and education level. 41 However, somewhat consistent with the other studies, increased chances of internalizing behaviors were evident when the mothers had persistent mental health challenges (depression at 6 weeks postpartum and symptoms of a psychological disorder at 12 and/or 24 months postpartum).
In a study with 600 American Indian/Alaskan Native kindergarten-aged children, Riser and colleagues found no statistically significant association between self-reported severe maternal depression (CES-D ≥ 15) and parent-reported offspring externalizing behaviors when offspring sex, age, and cognitive skills were adjusted. 42 The study was judged to have a fair study quality.
In sum, maternal internalizing issues were found to be associated with offspring internalizing and externalizing behaviors in 4 of the 5 studies with 2 of these studies rated to have a low risk of bias.
Discussion
Associations between parental psychopathology and offspring emotional and behavioral outcomes were examined in 14 studies of Indigenous parents and their offspring across 5 countries. In 11 of these 14 studies, associations were found between parental mental health challenges and offspring emotional and behavioral challenges. Of these 11 studies, just 2 included non-Indigenous comparison groups. These 2 studies provided limited data to suggest that the offspring of Indigenous parents with mental health challenges were more susceptible to their adverse effects than those born to non-Indigenous parents. 32,33 While data comparing risk in the offspring of Indigenous and non-Indigenous parents with mental health challenges are scarce, and no conclusions regarding causality can be made, these findings raise the possibility that Indigenous offspring may be more susceptible to the adverse effects of being raised by a parent with a mental health challenge. Why this might be is unclear, but factors such as identity loss and environmental stresses could be implicated. Indeed, identity loss due to ongoing colonial trauma in Indigenous Peoples has been shown to amplify mental health risk. 26,46 Colonization resulted in forced dislocation from familiar, traditional lands to unknown, remote lands and placement with individuals different from their Nation. 13,26 Accordingly, Indigenous Peoples did not have access to familiar food sources nor to their kinship network which contributed to identity loss. 26 Further, assimilation practices such as residential/boarding schools or placement of Indigenous children in the care of Caucasian families resulted in the breakdown and disconnection of family units. 8,25,27,47 During these critical developmental periods, children rarely observed or learned the cultural and parenting practices of their heritage. 7,47
Disconnection from cultural lands or social status in their community may also be particularly deleterious when the identity loss occurs during childhood or adolescence. Since some Indigenous groups hold sociocentric identities, offspring mental health challenges can be further exacerbated if the mental health of their parents, kin, or community is suboptimal. 8,25,48 For example, parents suffering from mental health challenges may be unable to provide sufficient support, nurturance, and socioemotional development to their children. 49 If environmental stressors such as chronic poverty, precarious housing, food insecurity, and other structural disadvantages that are often faced by Indigenous Peoples are concurrent with mental health challenges, then psychopathology among family members can be further exacerbated. 50 The mechanisms underlying this transmission have yet to be elucidated, although a growing area of research includes examining epigenetic changes among Indigenous Peoples, particularly those who are descendants from survivors of residential schools. 51,52
However, caution must be exercised in drawing conclusions about amplified risk transmission in these individuals, particularly since this is based on just 2 studies (one of which did not include a direct comparison of Indigenous and non-Indigenous groups) and because many questionnaires and structured interviews are neither developed with Indigenous families in mind nor tested and validated in these populations. The lack of Indigenous research methodologies (e.g., symbol-based reflection) in these studies further requires us to interpret these results with caution. 53
In the remaining 12 studies, in which no non-Indigenous comparison group was included, associations between parental mental illness and offspring psychopathology were found in 9, with rates comparable to general population samples, raising the possibility that the transmission rates may not be stronger in Indigenous families. For example, studies in the review suggested that the offspring of Indigenous parents with substance use issues are 2 to 3 times more likely to have a mental health challenge. Evidence from large general population samples indicate that exposure to parental substance use increases the risk for offspring psychiatric morbidity anywhere from 2 to 8 times. 54,55 We calculated effect sizes for our included studies on maternal depression and offspring emotional and behavioral issues and found small effect sizes for offspring internalizing (d = 0.23 to 0.26) and externalizing difficulties (d = 0.13 to 0.29). 56 Comparable effect sizes were reported in a meta-analysis of 193 studies of general population samples where the strength of the association between maternal depression and offspring behavior across all ages was small for internalizing (g = 0.23) and externalizing (g = 0 .21) behaviors. 57
Due to the ongoing structural disadvantages that Indigenous Peoples face, the similarity of effect sizes with non-Indigenous groups may be surprising. 10 However, this may be due to reclamation of Indigeneity or collective resilience which have been associated with a more positive well-being. 26,58,59 Indeed, parents’ cultural connectedness was found to protect offspring against the development of externalizing and internalizing behaviors in studies included in our review. 34,40 This is consistent with seminal findings by Chandler and Lalonde that the greater the cultural continuity (degree to which culture was transmitted from generation to generation) of a First Nations community, the lower the risk of suicide among the member of that community. 60 Therefore, Indigenous youth who retain a cultural identity within and beyond their community may be protected against the development of mental health challenges. Further, Indigenous groups that practice traditional parenting techniques like alloparenting, provide opportunities to the children to have decreased exposure to parental psychopathology, and ample opportunity for socioemotional development through modeling, which may reduce the transmission of psychopathology. 61 In addition, engaging in collective resilience (e.g., political activism or group participation in cultural traditions) may help to optimize mental health in Indigenous Peoples. 62 Even if offspring may be experiencing individual adversities, the social solidarity they receive from community members may prevent the development or worsening of mental health challenges.
However, the findings of these studies may also be biased toward the null hypothesis by studies’ methodological limitations that restrict our full understanding of the risks and their precipitants that Indigenous offspring may experience. These include issues related to Indigenous engagement, sampling, measurement, and analysis among others. 63 Indeed, Indigenous groups did not appear to have been consulted in 8 of the 14 studies, and so the recruitment of participants could have been biased toward those who are more trusting of researchers who use Western-dominant research methodologies, resulting in the misestimation of mental health challenges among Indigenous offspring. The lack of Indigenous partnership may also have prevented Indigenous definitions of mental well-being from being applied where well-being is viewed as wholistic, strength-based (rather than solely highlighting deficits), interconnected between mind, body, spirit, and land; acknowledges culture-bound syndromes; and advocates for reclamation of cultural traditions as a form of healing. 8,64,65 Failing to uphold Indigenous views on well-being and healing could result in misestimation of mental health challenges and hinder the identification of issues that are relevant for Indigenous Peoples.
Further, the sample size was not justified in any of the 14 studies, and so no discussion is provided as to whether these studies were adequately powered to detect differences in their primary outcome. In addition, some Indigenous groups may restrain their expression of extreme emotions or have different rules of behavior that can be reflected in measurement tools. 49,66 Thus, researchers who collaborated with Indigenous communities were advised to remove the ITSEA item “[child] is constantly moving” (a symptom of externalizing behavior), as exploration, independence, and autonomy are very much encouraged in Indigenous cultures. 34 However, in only 6 of the 14 studies were the questionnaires either adapted for use in Indigenous populations or the Indigenous communities were consulted prior to the onset of the research. Studies with measures that are not normed with Indigenous populations may misinterpret and overestimate the rates of externalizing behaviors in Indigenous offspring. 49 Aside from a lack of cultural validity, clinical interviews to measure parental mental health challenges were used in only 3 of the 14 studies, while the remainder of studies used questionnaires and cut-offs not normed to Indigenous groups. Using self-report questionnaires with low thresholds may not provide valid associations between poor parental health and offspring outcomes. Finally, 4 of the 14 studies were found to have a high methodological risk of bias and so results must be interpreted with caution.
Future Directions
In order to determine whether offspring of Indigenous parents with a mental health challenge are at a higher risk compared to their non-Indigenous peers, it is important that future studies recruit representative samples including non-Indigenous comparison groups, utilize measures that have been adapted and validated among the Indigenous group they are working with, and collaborate with Indigenous stakeholders to ensure the appropriate development and application of such measurements.
In future studies, researchers should aim to recruit representative samples from Indigenous communities along with matched controls from non-Indigenous populations. Representative samples may provide more accurate estimates of mental health challenges in Indigenous groups along with more accurate relative risks when non-Indigenous participants are recruited. These descriptive studies should be carried out with the ultimate goal of developing and tailoring interventions to the Indigenous Nation being examined. 67 Describing prevalence rates may also guide appropriate earmarking of government funding and resources. Culturally appropriate questionnaires (and their cut-offs) and structured interviews must also be developed for use in different Indigenous populations to ensure that symptoms of psychopathology in parents and children are accurately captured and useful screening, intervention, and treatment protocols developed.
Paramount to the recruitment of representative populations and adaptation and validation of measurements is the full partnership of Indigenous researchers, leaders, and communities in all stages of research including research question formulation, data collection and analysis, and data dissemination. 68 Collaboration will ensure that items on standardized questionnaires are applicable for Indigenous child development. Community-level control of data should be provided for capacity-building, empowerment, and appropriate resource allocation. 26,68 Further, to facilitate the development of intervention and treatment protocols for Indigenous offspring and their parents, variables that mediate and/or moderate the relationship between parental and offspring psychopathology must be examined. Particular attention should be paid to elucidating resilience mechanisms and applying a strengths-based perspective. 8,53 The diversity of Indigenous Peoples must be acknowledged in the development of interventions as the same intervention may not demonstrate the same effects across Indigenous groups. 26
Limitations
In addition to the issues raised above, the majority of studies were cross-sectional, which precludes us from drawing inferences on the temporal relationship between parental and offspring psychopathology. Moreover, only 2 studies included a non-Indigenous comparison group, so point estimates could not be calculated. Finally, child outcomes in all but 2 studies were examined using only maternal or child reports of questionnaires that can be colored by parental clinical status, leading to the overestimation of offspring internalizing and externalizing behaviors. 69
Conclusion
The findings from this systematic review indicate that parental psychopathology is associated with offspring emotional and behavioral challenges among Indigenous populations, much as it is with non-Indigenous populations. However, whether the offspring born to Indigenous parents with mental health challenges have higher rates of psychopathology than children born to comparable non-Indigenous parents remains unclear. More studies are needed to better understand resilience and risk factors that may lead to suboptimal Indigenous child development, and future studies should recruit large, representative samples, utilize culturally adapted measurements, and engage Indigenous stakeholders. Findings from these studies can then help identify children at risk for psychopathology and isolate targets for intervention to help improve the mental health of families and future generations.
Supplemental Material
Supplemental Material, CINAHL_Jan212019_ChildOutcomes - Psychopathology in the Offspring of Indigenous Parents with Mental Health Challenges: A Systematic Review: Psychopathologie des descendants de parents autochtones ayant des problèmes de santé mentale: Une revue systématique
Supplemental Material, CINAHL_Jan212019_ChildOutcomes for Psychopathology in the Offspring of Indigenous Parents with Mental Health Challenges: A Systematic Review: Psychopathologie des descendants de parents autochtones ayant des problèmes de santé mentale: Une revue systématique by Sawayra Owais, Mateusz Faltyn, Hanyan Zou, Troy Hill, Nick Kates, Jacob A. Burack and Ryan J. Van Lieshout in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, Embase_Jan212019_ChildOutcomes - Psychopathology in the Offspring of Indigenous Parents with Mental Health Challenges: A Systematic Review: Psychopathologie des descendants de parents autochtones ayant des problèmes de santé mentale: Une revue systématique
Supplemental Material, Embase_Jan212019_ChildOutcomes for Psychopathology in the Offspring of Indigenous Parents with Mental Health Challenges: A Systematic Review: Psychopathologie des descendants de parents autochtones ayant des problèmes de santé mentale: Une revue systématique by Sawayra Owais, Mateusz Faltyn, Hanyan Zou, Troy Hill, Nick Kates, Jacob A. Burack and Ryan J. Van Lieshout in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, Medline_Jan212019_ChildOutcomes - Psychopathology in the Offspring of Indigenous Parents with Mental Health Challenges: A Systematic Review: Psychopathologie des descendants de parents autochtones ayant des problèmes de santé mentale: Une revue systématique
Supplemental Material, Medline_Jan212019_ChildOutcomes for Psychopathology in the Offspring of Indigenous Parents with Mental Health Challenges: A Systematic Review: Psychopathologie des descendants de parents autochtones ayant des problèmes de santé mentale: Une revue systématique by Sawayra Owais, Mateusz Faltyn, Hanyan Zou, Troy Hill, Nick Kates, Jacob A. Burack and Ryan J. Van Lieshout in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, PsycINFO_March162019_ChildOutcomes - Psychopathology in the Offspring of Indigenous Parents with Mental Health Challenges: A Systematic Review: Psychopathologie des descendants de parents autochtones ayant des problèmes de santé mentale: Une revue systématique
Supplemental Material, PsycINFO_March162019_ChildOutcomes for Psychopathology in the Offspring of Indigenous Parents with Mental Health Challenges: A Systematic Review: Psychopathologie des descendants de parents autochtones ayant des problèmes de santé mentale: Une revue systématique by Sawayra Owais, Mateusz Faltyn, Hanyan Zou, Troy Hill, Nick Kates, Jacob A. Burack and Ryan J. Van Lieshout in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, WoS_Jan212019_ChildOutcomes - Psychopathology in the Offspring of Indigenous Parents with Mental Health Challenges: A Systematic Review: Psychopathologie des descendants de parents autochtones ayant des problèmes de santé mentale: Une revue systématique
Supplemental Material, WoS_Jan212019_ChildOutcomes for Psychopathology in the Offspring of Indigenous Parents with Mental Health Challenges: A Systematic Review: Psychopathologie des descendants de parents autochtones ayant des problèmes de santé mentale: Une revue systématique by Sawayra Owais, Mateusz Faltyn, Hanyan Zou, Troy Hill, Nick Kates, Jacob A. Burack and Ryan J. Van Lieshout in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
We would particularly like to thank Mr. Troy Hill (Mohawk, Six Nations of the Grand River Reserve) and Dr. Jacob Burack for their collaboration. Mr. Hill provided his perspectives on Indigenous ways of knowing while also reminding us of the significant and rich diversity of Indigenous Peoples. Dr. Jacob Burack shared his learning and experiences during a more than 2 decades long collaboration with the educators and students of the Jimmy Sandy Memorial School and the community leaders of the Naskapi Nation of Kawawachikamach, Québec, Canada, as well as from a similarly long academic association and friendship with Dr. George Blacksmith, a Cree educator and scholar whose collection of first-hand accounts of the multigenerational effects of the residential schools on the Cree of northern Quebec is essential reading in the history of the Indigenous Peoples living in Canada. 70 We would like to acknowledge Jo-Anne Petropoulos for her help in reviewing the search strategies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.