
Abstract

Dear Sir,
Major depressive disorder (MDD) reportedly associated with γ-amino butyric acid (GABA) dysfunction is marked by altered levels and activity of GABA. 1 Yoga has shown promise in improving MDD symptoms and associated low GABA levels. 2 Also it modulates physiological response to stress through GABA-mediated receptors: GABAA and GABAB. 3 Transcranial magnetic stimulation (TMS) measures GABA-mediated cortical inhibition (CI) noninvasively. Current study comes from a larger prospective randomized controlled trial evaluating the effect of 12-week yoga therapy on various biological parameters including CI in MDD (DSM-IV) at a tertiary care centre in South India. Subjects were screened using Mini International Neuropsychiatric Interview. Seventy subjects (mean age = 31.5 ± 8.7 years) scoring ≥18 on 17-item Hamilton Depression Rating Scale (HDRS) and stabilized on antidepressants for at least 2 weeks were randomized to either yoga group (YG; n = 35) or waitlist group (WG; n = 35) using block randomization (blocks of 10). Sequentially numbered opaque-sealed envelope method was used for randomization with allocation concealment. Patients with comorbid medical or psychiatric disorder except nicotine dependence, treatment resistant depression, and/or practicing yoga ≥45 minutes/week in last 6 months or received ECT in last 3 months were excluded. Institute Ethics Committee of the National Institute of Mental Health and Neurosciences approved the protocol, and all participants provided written informed consent. Depression ratings were done using HDRS at baseline and after 4, 8, and 12 weeks. TMS measures of CI using Mag Pro R30 (MagVenture, Denmark) was obtained at baseline and 12 weeks by trained personnel. CI was assessed using cortical silent period (CSP) at 120% of resting motor threshold (RMT), short interval intracortical inhibition (SICI), and long interval intracortical inhibition (LICI). YG was taught a validated 1-hour yoga module for depression, 4 by a trained yoga instructor, for 12 sessions in the first 4 weeks, and two booster sessions in next 8 weeks were provided with monitored home-based practice—4 days/week. WG was offered yoga after the trial period of 12 weeks.
Statistical analysis was done using SPSS-16 (Table 1). Two groups were comparable at baseline on sociodemographic profile and clinical scores (all P > 0.3). In intent to treat analysis, linear mixed model analysis was performed, which showed significant time × group interaction for CSP, favoring improvement in YG (P < 0.01; within group Cohen’s d effect size—YG = 0.76 and WG = 0.48). No significant change was observed for LICI (P = 0.2; within group Cohen’s d effect size—YG = 0.25 and WG = 0.24) and SICI (P = 0.5; within group Cohen’s d effect size—YG = 0.12 and WG = 0.13), though there was a trend for improvement in the YG. No significant correlation was found between RMT and other TMS paradigms. Clinically both groups improved significantly over time (F = 116.99, P = 0.0001) with more improvement and higher remission rate in YG (8.94 ± 7.69 and 62.8%) than WG (10.41 ± 7.46 and 45.7%).
Change in Measures of CI from Baseline to Study End Point (3 Months) in the 2 Groups.
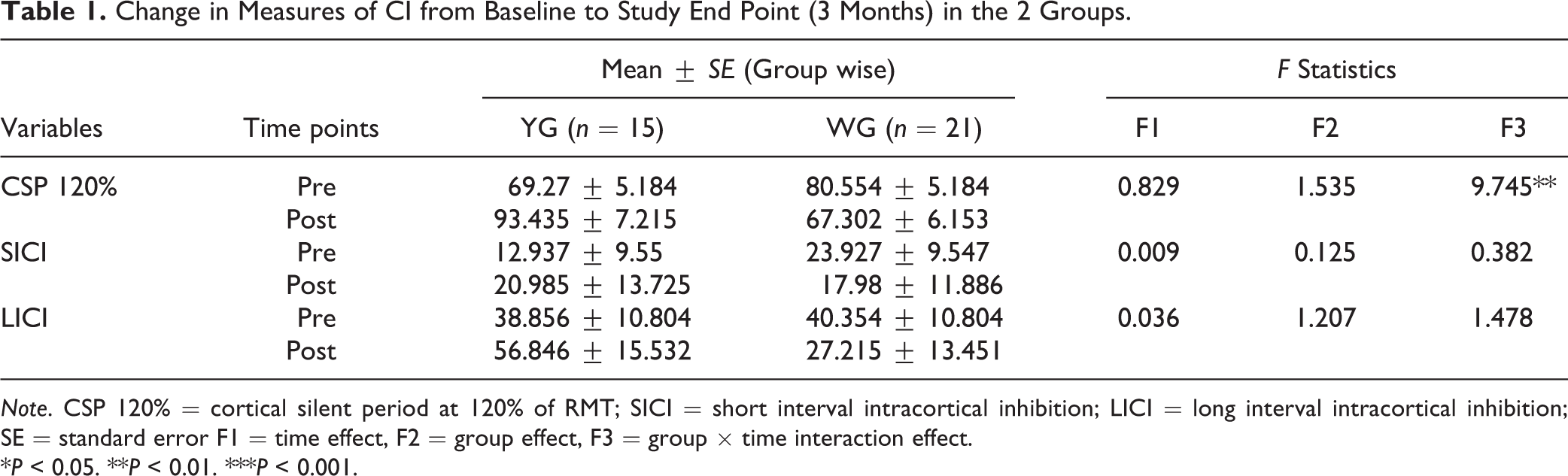
Note. CSP 120% = cortical silent period at 120% of RMT; SICI = short interval intracortical inhibition; LICI = long interval intracortical inhibition; SE = standard error F1 = time effect, F2 = group effect, F3 = group × time interaction effect.
*P < 0.05. **P < 0.01. ***P < 0.001.
Discussion
MDD is reportedly associated with reduced SICI and shortened CSP, involving both GABAA and GABAB receptor-mediated inhibitory neurotransmission deficits. 5 This altered function of GABAergic system has been considered as a potential biomarker of response to antidepressant treatment. 6 CSP and LICI are related to GABAB and SICI is related to GABAA receptor-mediated inhibitory postsynaptic potential. Our study showed significantly greater improvement in CSP in YG only, consistent with literature. 3 LICI and SICI also showed enhancement in YG more than WG, though not statistically significant. These findings are suggestive of the modulatory effect of yoga on GABA system. Although both groups improved on HDRS score, significant improvement in CI measures along with clinical improvement in YG is more suggestive of intervention effect. No subject reported any major side effect due to yoga practice. Three subjects had mild body ache initially, which subsided with continued practice. High drop-out rate in this study can be explained by 2 major reasons: long distance for the study center and change in contact details.
A recent magnetic resonance spectroscopy study on MDD subjects concluded that yoga improves mood by increasing the activity of the GABA system. 2 We found higher remission with add-on yoga associated with greater increase in GABA-mediated CI, suggestive of an enhancing effect of a course of yoga on GABA activity. 2,3 To the best of our knowledge, this study is the first to demonstrate increased GABA-mediated neurotransmitter activity using TMS, following a course of yoga with multiple therapy sessions in a clinical sample with MDD. These findings highlight plausible therapeutic role of yoga in enhancing recovery in patients with depression and can be considered for routine recommendation in clinical practice. Further, future studies with larger samples and long-term follow-up, controlling for influential limitations such as blinding of raters, may provide more conclusive evidence.
Supplemental Material
Supplemental Material, Consort_chart - Impact of a Course of Add-on Supervised Yoga on Cortical Inhibition in Major Depressive Disorder: A Randomized Controlled Trial
Supplemental Material, Consort_chart for Impact of a Course of Add-on Supervised Yoga on Cortical Inhibition in Major Depressive Disorder: A Randomized Controlled Trial by Praerna H. Bhargav, Preethi V. Reddy, Ramajayam Govindaraj, Kankan Gulati, Arya Ravindran, D. Gayathri, Sneha J. Karmani, Kaviraja Udupa, Ganesan Venkatasubramanian, Mariamma Philip, Monojit Debnath, Rose Dawn Bharath, T. N. Sathyaprabha, Bangalore N. Gangadhar and Kesavan Muralidharan (PI) in The Canadian Journal of Psychiatry
Footnotes
Acknowledgement
We acknowledge Dr. Bharath Holla, Assistant Professor (Psychiatry), Department of Integrative Medicine, NIMHANS, Bangalore for helping in analyzing the data.
Authors’ Note
Kesavan Muralidharan is the principal investigator of the study. The study is registered under CTRI vide no. CTRI/2017/07/00907.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge Department of Science and Technology, Government of India for financial support vide reference number: SR/SATYAM/351/2015, under Science and Technology of Yoga and Meditation (SATYAM) to carry out this work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.