
Abstract
Objective:
The goal of this study was to validate the French version of the Quality of Life in Bipolar Disorder (QoL.BD) scale, a condition-specific measure for bipolar disorder (BD).
Method:
The QoL.BD scale was translated into French in accordance with the recommendations for transcultural adaptation. It was administered to 125 participants with BD living in Quebec, Canada. Construct validity was evaluated through correlations with other measures of self-reported quality of life (QoL), functioning, and symptoms. Factorial structure was examined through an exploratory factor analysis.
Results:
Internal reliability and test–retest reliability standards were met. Correlations in expected directions with other QoL, functioning, and depressive symptom scales supported convergent validity. The item loadings structure of the French QoL.BD largely replicated the original English version, with some modifications.
Conclusion:
The French version of the QoL.BD (full and brief) is comparable in its psychometric properties to the English version. It is a valid and sound measure for the evaluation of the QoL of French-speaking patients with BD.
Introduction
Bipolar disorder (BD) is a chronic mental health condition characterized by the experience of periods of mania (defined by extreme elation, expansiveness, and/or irritability, coupled with increased goal-directed activity) and depression. Internationally, the lifetime prevalence of BD has been estimated to be between 1% and 2% 1 and has been ranked by the World Health Organization as at 5th leading cause of disease burden among mental disorders. 2 Quality of life (QoL) instruments are increasingly used in BD research to assess a person’s functioning and satisfaction across a broad range of life domains. 3,4 Until 2010, studies of BD exclusively used generic instruments to assess QoL—while these assess areas of life considered to be important to the general population, they may not capture the particular priorities of individuals living with BD. 5,6 QoL instruments developed to assess domains impacted by a specific condition have been shown to be more responsive than generic tools 7,8 and are less likely to demonstrate “floor effects.” 9 As such, an important step forward in the BD QoL field was the development of the English-language version of the condition-specific Quality of Life in BD (QoL.BD) scale. 10 The QoL.BD was developed in consultation with individuals with lived experience of BD and assesses the cardinal impacts of BD symptoms (mood, sleep, physical health, cognition), role functioning (household management, finances, and two optional areas: work and education), and expressions of satisfaction and well-being (including the domains of leisure, relationships, self-esteem, spirituality, identity, and independence). When evaluated in a sample of English-speaking people living with BD in Canada, both the full 56-item and brief 12-item versions of the QoL.BD have demonstrated excellent internal reliability (0.79 to 0.95), appropriate test–retest reliability (0.46 to 0.87), and satisfactory construct validity when compared to other QoL measures 7 . Factor analysis on the core items (i.e., not including the optional work and study domains) supported a 12-domain structure. The QoL.BD has seen widespread use in clinical trials internationally, 11 –16 has been translated in over 20 languages, and has a validated web-based administration format. 17 Furthermore, the QoL.BD is ideally suited for case formulation and outcome assessment in clinical practice: A suite of self-management tools that address the QoL domains have been developed and evaluated, 18,19 and the full version of the instrument takes only 4 minutes to administer. 7
A number of Canadian Institute of Health Research (CIHR) grants have been granted to support the development of psychosocial interventions for BD incorporating the QoL.BD. 18,19 However, the lack of a validated French translation limits the ability to disseminate these interventions and findings across Canada, as well as internationally. This marks a significant limitation, given that 22% of the Canadian population report French as their first language. 20 It cannot be assumed that a direct translation of the QoL.BD will adequately represent QoL for a French-speaking population: For instance, given France is the 4th most secular country, 21 QoL as related to spirituality may be conceptualized differently. In light of the cultural differences that can pertain to a French-speaking population, the goal of this study was to perform a cross-cultural adaptation of the QoL.BD in French and to explore the psychometric properties of the full and brief French versions of the QoL.BD.
Methods
Procedures
Cross-cultural adaptation
Following the recommendations of Guillemin et al., 22 the translation of the questionnaire from English to French was done by two professional French-speaking translators. Then, a blind back-translation was done by two professional English-speaking translators. Next, a final version was reviewed by a committee of experts consisting of the developer of the English version of the scale, two bilingual researchers specializing in BD research and care, a bilingual patient with BD, and a bilingual facilitator. The wording of some items was revised to more appropriately embody the intent of the original QoL.BD scale in a French-speaking population. For example, the committee member with lived experience of BD suggested that the initial literal translation of the first item of the physical domain, “I have had plenty of energy” to “J’ai eu beaucoup d’énergie,” conveyed a sense of excessive (and potentially, clinically concerning) levels of energy. On the basis of this feedback, the item wording was changed to “suffisamment” to convey an appropriate level of energy for the individual’s needs.
The revised version was then field tested with a sample of 17 patients with BD residing in Paris, Geneva, and Montreal. Some pilot study participants reported difficulty responding to items assessing subjective, personal concepts (particularly in the identity, spirituality, and independence domains); further minor modifications were made to improve the clarity of these items. The final version of the full and brief scales is presented in Online Appendices 1 and 2, respectively.
Psychometric evaluation
One hundred and twenty-five participants (age 18 to 70) who had been diagnosed with BD of any type (I, II, nonspecified) were recruited in various hospitals in the province of Quebec. The project was approved by the research ethics committees of the hospitals concerned. Through the hospitals’ archives service, a letter introducing the project was sent to participants who had been identified by their consulting psychiatrist as having a diagnosis of BD. The letter enquired about their interest in participating in the project and asked for permission to be contacted by the research team. The French version of the QoL.BD was then sent by mail to those who consented to be contacted and again 2 weeks later in order to evaluate its test–retest reliability. Recruitment occurred between October 2014 and June 2015.
In total, 489 invitations were sent. One hundred and thirty-six participants agreed to receive the questionnaire and provided written informed consent, 125 returned the first set of questionnaires, and 114 returned the second set of questionnaires (see Table 1 for participant characteristics).
Descriptive and Clinical Characteristics of the Sample.
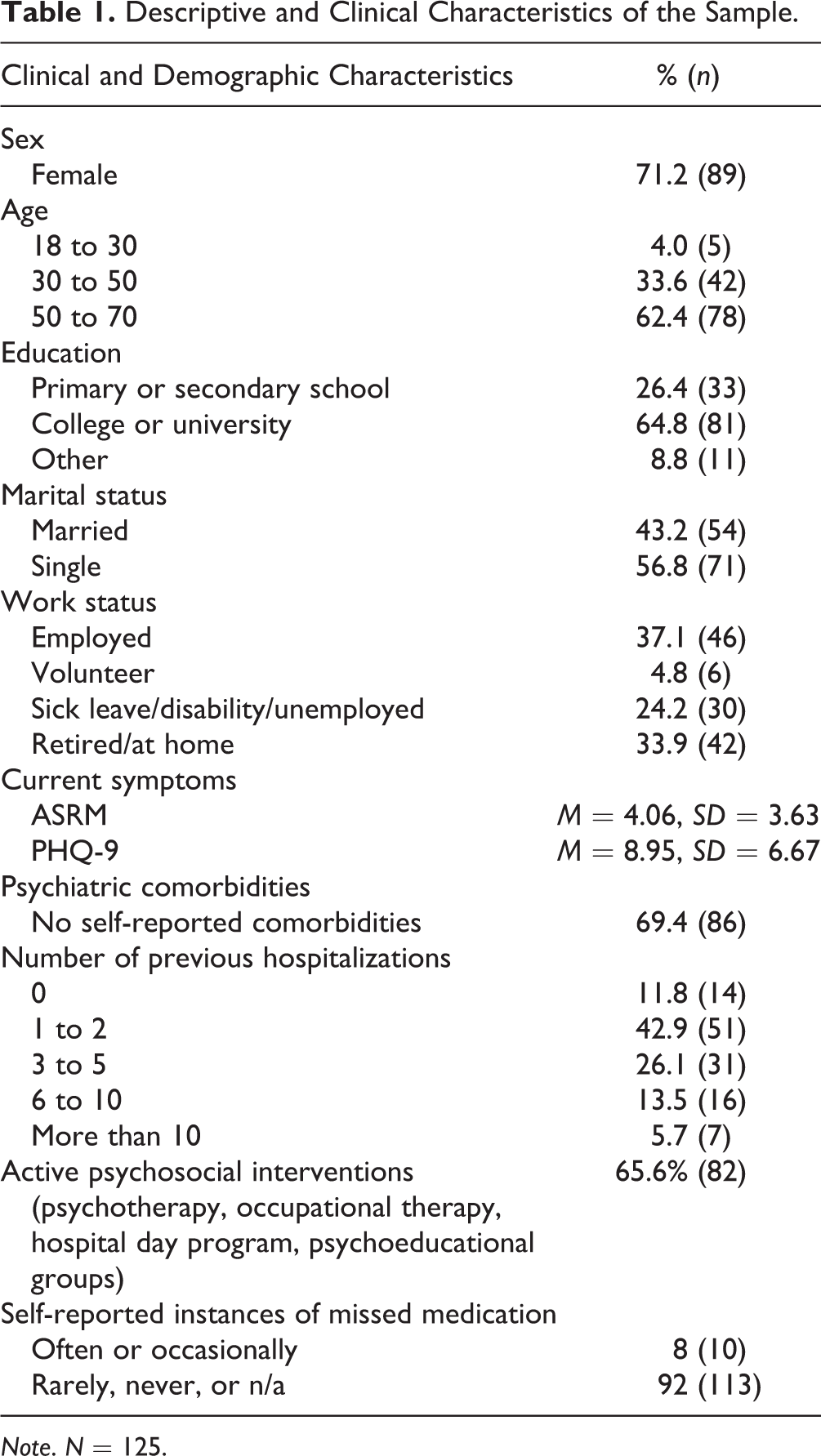
Note. N = 125.
Measures
The French version of the full (56 item) and the brief (12 item) Quality of Life in Bipolar Disorder (QoL.BD) scale was administered. The long version is divided into 14 domains: Physical, Sleep, Mood, Cognition, Leisure, Social, Spirituality, Finances, Household, Self-esteem, Independence, Identity, Work (optional), and Education (optional). Each domain has 4 items, and each item is scored on Likert-type scale (1 = strongly disagree; 5 = strongly agree). A global score can be calculated by summing scores for all items in the core 12 domains (range: 48 to 240). The brief version contains one item assessing each of the 12 core domains and is scored by summing responses to all items (range: 12 to 60).
To evaluate construct validity, the French versions of the following self-reported QoL and functioning measures were administered: the Quality of Life Enjoyment and Satisfaction Questionnaire—Short Form (Q-LES-Q-SF) 23 ; the 36-item Medical Outcomes Study Short Form (SF-36) 24 ; the World Health Organization Quality of Life BREF (WHOQOL-Bref) 25 ; and the World Health Organization Disability Assessment Schedule 2.0 (WHODAS-2.0). 26 Self-reported depression was assessed with the Patient Health Questionnaire 9 (PHQ-9), 27 and the Altman Self-Rating Mania Scale (ASRM) 28 was used to assess self-reported symptoms of hypomania.
Statistical Analyses
All analyses were done using version 9.4 of the SAS/STAT program. To evaluate reliability and construct validity, missing data were handled using domain-specific mean-score imputation. For the exploratory factor analysis (EFA), participants with missing data (n = 17) were excluded from the analyses.
For each QoL.BD domain, the Cronbach’s alpha coefficients were calculated as the measure of internal reliability with a minimal reference value of 0.70. 29 The construct validity was evaluated via Pearson correlations with the Q-LES-Q-SF, SF-36, WHOQOL-Bref, WHODAS-2.0, PHQ-9, and ASRM. Test–retest reliability was evaluated for each domain by calculating the intraclass correlation coefficient (ICC) between the initial administration of the QoL.BD and 2-week follow-up.
An EFA was conducted in SAS using the maximum likelihood method followed by an oblique (oblim) rotation using the FACTOR procedure. EFAs were conducted on (a) the 12 basic domains of the QoL.BD and (b) the Brief QoL.BD. For the EFA conducted on the 12 basic domains, a fixed number of factors (12) were extracted based on theoretical and pragmatic grounds. First, the qualitative interviews and literature review informing the original QoL.BD provide theoretical support for a 12 distinct, core domains relevant to QoL in BD. Second, CIHR-supported interventions have been developed based on the original QoL.BD structure; preserving the original structure of the QoL.BD where possible will support translation of these interventions in a French-speaking population. Similarly, for the Brief QoL.BD, one factor was extracted on theoretical and pragmatic grounds. Interpretability of the extracted factors was evaluated by examining primary factor loadings and cross-loadings greater than 0.32. 30
Results
Internal Reliability and Test–Retest Reliability
The majority of the instrument’s 14 domains showed good internal reliability, with all but the Physical domain (α = 0.67) exceeding the minimal acceptable Cronbach’s alpha score of 0.70. The ICCs of the domains scores and the total score for the brief version were relatively good (with ICCs between 0.54 and 0.75) and is similar to that of the English version (see Table 2).
Descriptive Statistics of the 14 Subscales of the Quality of Life in Bipolar Disorder (QoL.BD) Scale.
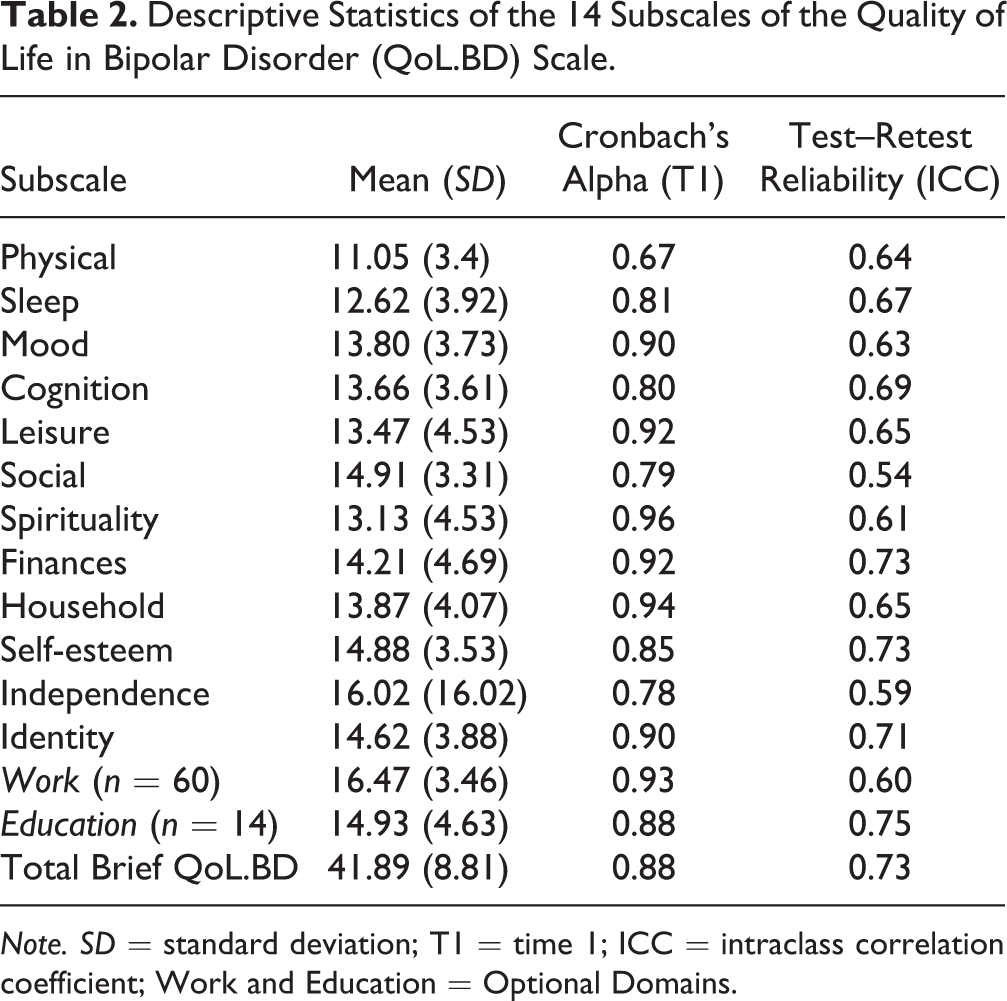
Note. SD = standard deviation; T1 = time 1; ICC = intraclass correlation coefficient; Work and Education = Optional Domains.
Construct Validity
The correlations between QoL.BD domain scores and the Brief QoL.BD total score to other self-reported QoL measures were strongly positive, especially with the WHOQOL-Bref total score (0.87), the Q-LES-Q-SF (0.86), and the general mental health score (GMH) of the SF-36 (0.71). Moreover, the correlations with the WHODAS-2.0 were negative (−0.61); a high score on this scale reflects poorer functioning. Correlations between Brief QoL.BD total scores and symptoms of depression (PHQ-9) were strongly negative (−0.74); a weak (0.25) but significant correlation between symptoms of hypomania (ASRM) was observed, suggesting that self-reported hypomania was associated with slightly better subjective QoL (see Table 3).
Quality of Life, Mood, and Symptom Correlates of Quality of Life in Bipolar Disorder (QoL.BD) Scale.
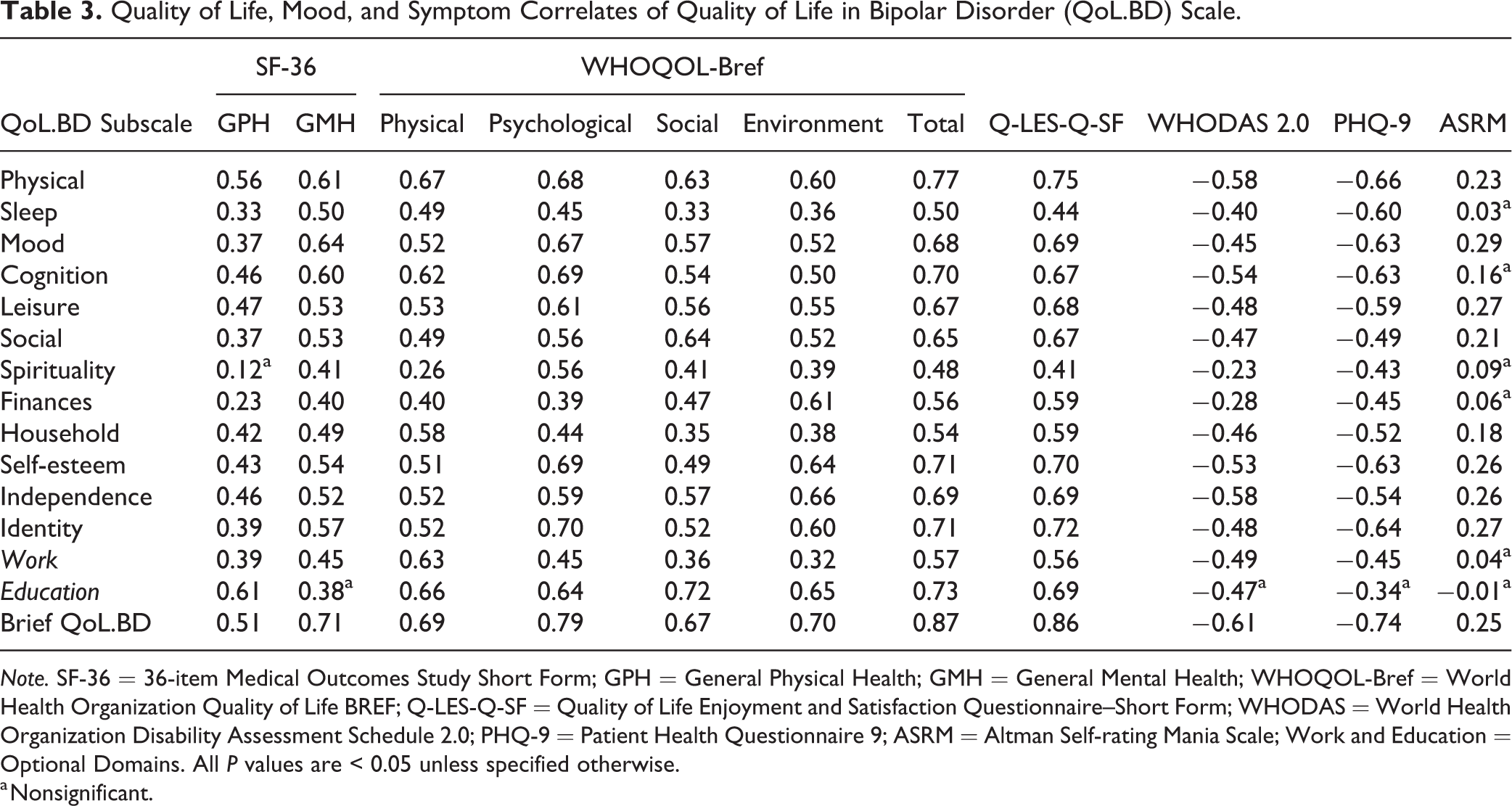
Note. SF-36 = 36-item Medical Outcomes Study Short Form; GPH = General Physical Health; GMH = General Mental Health; WHOQOL-Bref = World Health Organization Quality of Life BREF; Q-LES-Q-SF = Quality of Life Enjoyment and Satisfaction Questionnaire–Short Form; WHODAS = World Health Organization Disability Assessment Schedule 2.0; PHQ-9 = Patient Health Questionnaire 9; ASRM = Altman Self-rating Mania Scale; Work and Education = Optional Domains. All P values are < 0.05 unless specified otherwise.
a Nonsignificant.
EFA
The factorability of the data was confirmed: Bartlett’s Test of Sphericity was significant χ2(1128) = 4,857.9, P < 0.0001; and the Kaiser–Meyer–Olkin measure of sampling was 0.87, exceeding the recommended minimum value of 0.6. 30 Based on theoretical grounds and in order to explore the performance of the factor structure identified in the English version, a model with 12 factors was extracted for the full QoL.BD. Primary and cross-loadings above 0.32 are shown in Table 4. Items predominantly displayed primary loadings on the same factor as the original English validation study. Spirituality, Finances, and Household were strongly and clearly represented (with item loadings between 0.58 and 0.99). Mood was also well replicated, but with weaker loadings, between 0.47 and 0.72. Cognition, Independence, Self-esteem, and Social were likewise well replicated, with some slight modifications. The most notable change in factor loadings occurred over the Physical domain: Two physical items were observed to weakly load onto a factor with leisure items (0.32 to 0.45), and 2 physical item (“I have been content with my sex life”/“J’ai été satisfait(e) de ma vie sexuelle”; “I have had plenty of energy”/“J’ai eu suffisamment d’energie”) did not load strongly on any factor. Item loadings for the Brief QoL.BD ranged from 0.42 to 0.83, replicating the structure of the original English version (see Table 4).
Primary and Cross Loadings for the French-language Version of the Full QoL.BD.
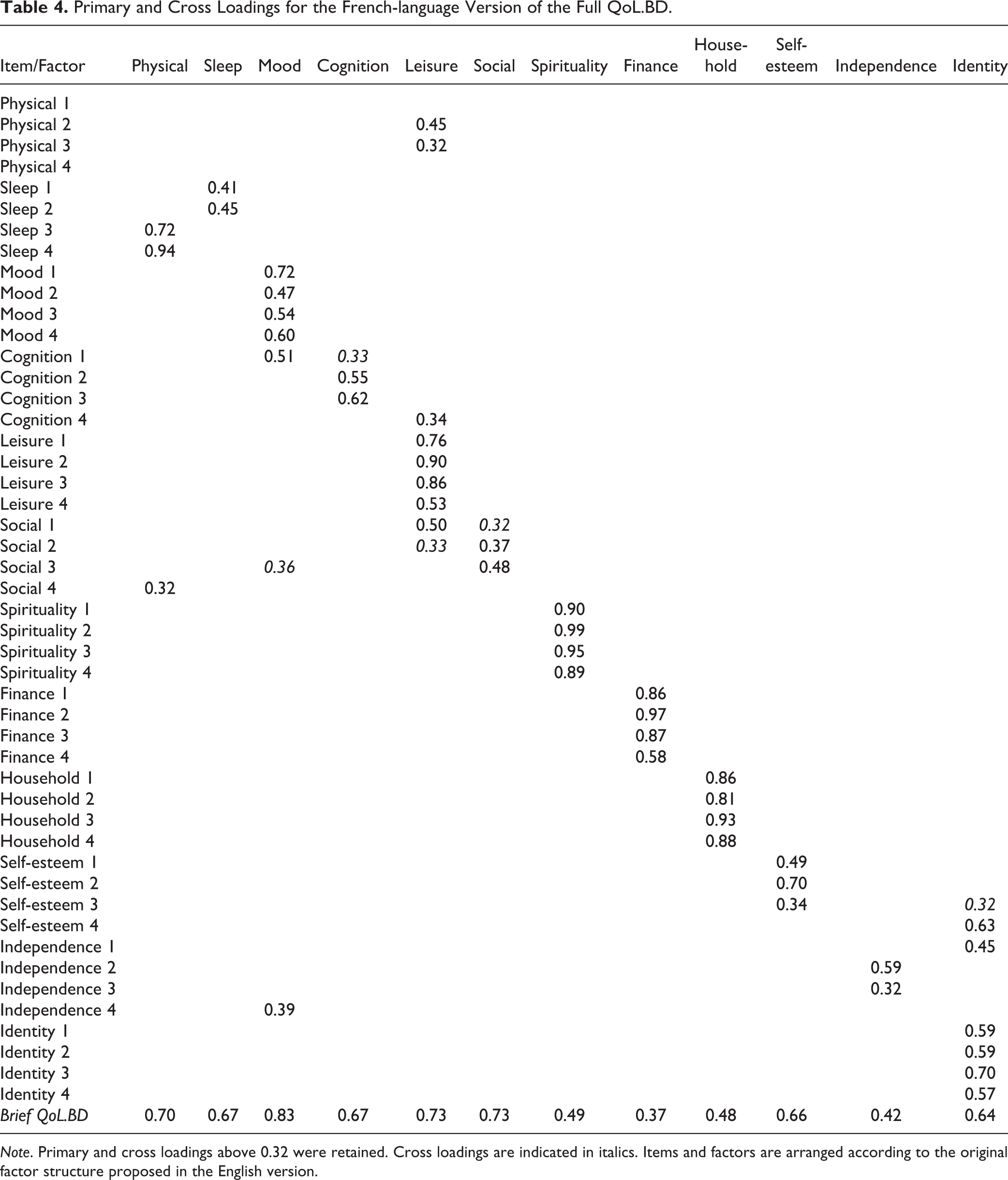
Note. Primary and cross loadings above 0.32 were retained. Cross loadings are indicated in italics. Items and factors are arranged according to the original factor structure proposed in the English version.
Discussion
The results obtained allow us to conclude that the French translation of the QoL.BD is a reliable and valid measure of QoL in French speakers living with BD. As with the original English version, 10 the internal reliability (0.67 to 0.96) and test–retest reliability (0.54 to 0.75) met appropriate standards, and the correlations between the subscales of the QoL.BD and the subscales of complimentary non-condition-specific QoL measures (i.e., SF-36, WHOQOL-Bref, Q-LES-Q-SF) were moderate to high. Overall, the item loadings of the French version were comparable to that of the English version for both the full and brief versions, with some slight modifications.
The psychometric properties described in this study accord with the findings of other cross-cultural adaptations of the QoL.BD, including the Chilean Spanish 31 translation of the full scale, and the Chinese 32 and Iranian 33 adaptations of the Brief QoL.BD. Internal reliability is excellent across the various formats of the brief QoL.BD, varying between 0.82 for the Chinese version and 0.88 for the French version. The test–retest reliability is also good, varying between 0.69 for the English version and 0.81 for the Chinese version. The correlations of the various Brief QoL.BD adaptations with other QoL scales are consistently moderate to high, varying between 0.31 and 0.71 for the SF-36 and between 0.41 and 0.89 for the Q-LES-Q. Importantly, these findings support potential use of the QoL.BD in large-scale international trials with diverse cultural groups.
As expected, given that depression has consistently been found to be a predictor of poorer QoL in BD, 34,35 QoL.BD overall and dimension scores demonstrated strongly negative correlations with self-reported depressive symptoms. Unexpectedly, higher levels of self-reported hypomania were associated with slightly higher self-reported QoL. Evidence regarding the relationship between mania and QoL is mixed: While some studies have found a negative impact of mania on QoL, 36 –39 others have found no relationship 40,41 or a positive influence. 42 Potentially, given the evaluative nature of the QoL.BD relative to the SF-36 (which assesses concrete aspects of QoL more closely related to functioning 4 ), it may be more impacted by the experience of elevated mood. Furthermore, as levels of hypomania in the present sample were mild, individuals may have been experiencing positive impacts to their QoL (such as increased enjoyment from social interactions, feelings of well-being) and not the significant negative consequences of mania.
The EFA of this study identified item loadings that were largely comparable to that of the original English version. However, some modifications were observed, most notably in the Physical domain. It may be expected that some physical health items would load with items from the Leisure domain, given that many leisure activities (e.g., team sports) are both social and active. Potentially, this may reflect cultural differences in leisure activity preferences between French-Canadians and the original English-speaking sample. To permit cross-cultural comparisons of QoL using this scale, and to facilitate the use of the QoL.BD as a tool to guide the application of specific evidence based self-management strategies, 18,19 we recommend that the French QoL.BD be applied and scored as per the original English version.
Limitations to this study should be noted. First, the sample size used for the EFA was 108—while this meets the minimum recommended sample size, 43,44 it is considered small for an EFA. 45 A larger sample size was sought (n = 489 invitations sent); however, the response rate (26%) was low. Further, the ratio between sample size (N) and number of items (p) was low for the full QoL.BD but appropriate for the Brief version. However, it should be noted that there is evidence to support adequate replication of factor solutions in much smaller samples and N: p ratios than common rules of thumb. 46 As such, our conservative recommendation for empirical research is to preferentially use the Brief QoL.BD in Francophone samples until a larger accumulated sample is available for validation.
A second limitation arises from sample composition, which was primarily women (71.2%) and people aged 50 and 70 (62.4%). Although the gender composition of this sample is consistent with two other psychometric evaluations of this scale in Canadian samples (the original QoL.BD validation study and recent web-based adaptation), the overrepresentation of women and older adults may limit the generalizability of these findings to men and young people with BD. There is some preliminary evidence to suggest that older age and female gender are associated with poorer QoL in BD; 47 however, the role of demographic variables in predicting QoL has received limited attention to date. Future studies should aim to recruit a larger, more representative sample. Finally, while the questionnaire was piloted with French-speaking individuals in Switzerland, Canada, and France, the EFA was conducted solely with a French-Canadian population, which may have cultural differences relative to French populations. As such, generalizability of the factor solution identified in this study should be interpreted cautiously.
Conclusion
In conclusion, the French version of the QoL.BD (brief and full) is comparable to the English version in its psychometric properties and represents as a viable and reliable measure of QoL in French-speaking patients with BD in both clinical and research settings. Of note, the feedback received by the patients with BD that completed the preliminary version of the scale was crucial in fine-tuning the meaning of specific items, thus reinforcing the importance of having people with lived experience of BD involved early in the research process itself. The cross-cultural adaptation of the QoL.BD into French is an important step toward better supporting the mental health needs and research participation of Francophone living with BD in Canada.
Supplemental Material
Supplemental_material - The Quality of Life in Bipolar Disorder (QoL.BD) Scale: Validation of a French Cross-Cultural Adaptation: L’échelle de qualité de vie dans le trouble bipolaire (QoL.BD) : Validation d’une adaptation française interculturelle
Supplemental_material for The Quality of Life in Bipolar Disorder (QoL.BD) Scale: Validation of a French Cross-Cultural Adaptation: L’échelle de qualité de vie dans le trouble bipolaire (QoL.BD) : Validation d’une adaptation française interculturelle by Martin D. Provencher, Emma Morton, Anne Sophie Beaudoin, Judith Guillemette, Evelyne Rheault, Chantal Mérette, Laurent Coque, Lisa D. Hawke and Erin E. Michalak in The Canadian Journal of Psychiatry
Footnotes
Data Access
In accordance with this study’s research ethics approval, de-identified data may be accessed via request to and approval from the principal investigator Dr. Martin D. Provencher.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was received from the Direction de l’enseignement et des affaires universitaires (DEAU), Centre intégré universitaire de santé et de services sociaux (CIUSSS) de la Capitale-Nationale, Québec, QC, for the training in research as part of the Residency Program in Psychiatry at Laval University. EM was supported by a postdoctoral award from the Marshall Scholars and Fellows Program in Mental Health, Institute of Mental Health, University of British Columbia.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.