
Abstract
Objective:
A substantial proportion of severely ill patients with obsessive-compulsive disorder (OCD) do not respond to serotonin reuptake inhibitors (SRIs) and are unable to practice cognitive behavioral therapy (CBT) on an out-patient basis. We report the short-term (at discharge) and long-term (up to 2 years) outcome of a multimodal inpatient treatment program that included therapist-assisted intensive CBT with adjunctive pharmacotherapy for severely ill OCD patients who are often resistant to SRIs and are either unresponsive or unable to practice outpatient CBT.
Methods:
A total of 420 patients, admitted between January 2012 and December 2017 were eligible for the analysis. They were evaluated using the Mini International Neuropsychiatric Interview, the Yale-Brown Obsessive Compulsive Scale (YBOCS), and the Clinical Global Impression (CGI) scale. All patients received 4 to 5 therapist-assisted CBT sessions per week along with standard pharmacotherapy. Naturalistic follow-up information at 3, 6, 12, and 24 months were recorded.
Results:
At baseline, patients were mostly severely ill (YBOCS = 29.9 ± 4.5) and nonresponsive to ≥2 SRIs (83%). Mean duration of inpatient stay was 42.7 ± 25.3 days. At discharge, there was a significant decline in the mean YBOCS score (29.9 ± 4.5 vs. 18.1 ± 7.7, P < .001, Cohen’s d = 1.64); 211/420 (50%) were responders (≥35% YBOCS reduction and CGI-I≤2) and an additional 86/420 (21%) were partial responders (25% to 35% YBOCS reduction and CGI-I≤3). Using latent class growth modeling of the follow-up data, 4 distinct classes were identified, which include “remitters” (14.5%), “responders” (36.5%), “minimal responders” (34.7%), and “nonresponders” (14.6%). Shorter duration of illness, better insight, and lesser contamination/washing symptoms predicted better response in both short- and long-term follow-up.
Conclusion:
Intensive, inpatient-based care for OCD may be an effective option for patients with severe OCD and should be considered routinely in those who do not respond with outpatient treatment.
Introduction
Obsessive-compulsive disorder (OCD) is a common 1,2 and disabling mental illness. 3 While outpatient treatment is the standard strategy for OCD, inpatient/residential programs that involve a combination of intensive cognitive behavioral therapy (CBT) with exposure and response prevention (EX/RP) and medications are being explored as potential treatment approaches for severe and often treatment-resistant patients. 4–6 CBT is effective, both as a first-line treatment for OCD 7,8 and as an augmenter in patients with poor response to serotonin reuptake inhibitors (SRIs). 9,10 However, many patients may not be able to participate in outpatient CBT, mainly due to intolerable anxiety. 11,12 About 20% to 30% of patients are known to drop out of EX/RP prematurely. 13,14 Inpatient care offers a unique opportunity to carry out intensive CBT that is perhaps more effective than less intense approaches, at least in the short-term. 15 –18
A meta-analysis of 19 studies of residential/inpatient/day-care programs involving 2,306 patients reported a significant reduction in the severity of illness with a large effect size. 4 However, long-term benefits of such an approach are unclear. Moreover, previous studies have failed to identify consistent predictors of outcomes mostly due to their small sample sizes. Given the high costs of these programs, it is important to examine long-term outcomes and their predictors in large samples.
A careful review of the residential/inpatient programs show that family members do not stay with patients during the period of hospitalization although involving them in treatment is vital for improving outcomes. Family accommodation plays a key role in the outcome and long-term prognosis of OCD. 19,20 Treatment programs that are “family-inclusive” are superior to those that are not. 21,22 The inpatient treatment program of the OCD Clinic at the National Institute of Mental Health & Neurosciences (NIMHANS), Bangalore, India, is unique in one way. The immediate family members (mostly a first-degree relative or the spouse) stay with patients during the entire course of hospital stay. This is a usual practice in all inpatient medical settings in India, which thus gives us an opportunity to involve family members in dealing with family accommodation, expressed emotions and proxy compulsions. This is especially relevant in our cultural context, where family accommodation is high and contributes to poor outcome. 23
We report the naturalistic short- (at discharge) and long-term (up to 2 years of follow-up) outcome and its predictors in a large sample of patients from the inpatient treatment program of the NIMHANS OCD Clinic in India. We also sought to look at clinical and sociodemographic characteristics that might predict response at discharge and at long-term follow-up.
Method
We reviewed the clinical charts of all inpatients with a primary diagnosis of DSM-IV-TR OCD from January 2012 to December 2017. The patients were admitted primarily for adjunctive intensive CBT treatment, in view of severe OCD which had little or no response to outpatient management. It is not the usual practice at our center to admit patients with a primary diagnosis of OCD for purposes other than adjunctive intensive CBT. For those patients who were admitted more than once for inpatient CBT, only the first admission was considered for analysis. As this is a chart review, no informed consent was obtained from the patients, but Institute Ethics Committee approved the study for ethical aspects. Out of a total of 451 unique cases, 31 (5.8%) were excluded because of very brief (<2 weeks) admission (16/31), inability to trace records (9/31), and inadequate clinical data (6/31). Hence, a total of 420 patients were included for the analysis.
Assessments
All patients underwent detailed clinical evaluation followed by a structured interview using the Mini International Neuropsychiatric Interview 6.0.0 (until 2016) and 7.0.0 (2017 onward). 24 In addition, patients were evaluated at the time of admission, discharge, and during the follow-up using the Yale-Brown Obsessive Compulsive Scale (YBOCS) 25,26 and the Clinical Global Impression (CGI) scale. 27 We administered the Structured Clinical Interview for DSM-IV for Personality Disorders 28 or the International Personality Disorder Examination-II 29 upon a clinical suspicion of the presence of personality disorder. All the assessments were performed by either postgraduate junior residents in psychiatry or postgraduate/doctoral students in clinical psychology or psychiatric social work. All raters received training sessions in administering the above-mentioned instruments every 3 months and were supervised by the senior residents or the consultants of the OCD clinic. The internal consistency (Cronbach α) of the YBOCS severity ratings at admission and discharge were found to be fairly high at 0.84 (obsessions) and 0.87 (compulsions), having a high convergent validity of the total score with the CGI-S ratings (r = 0.89).
Inpatient Care
All patients continued to receive SRIs along with intensive CBT (see Table 1) as per the existing standards. 30,31 Decisions to change SRI/add augmentation/adjust dosages were made after evaluating the adequacy of and response to the ongoing medication trial. These were made in the weekly grand rounds headed by one of the consultants of the OCD clinic.
Pharmacological Treatment Details of the Sample.
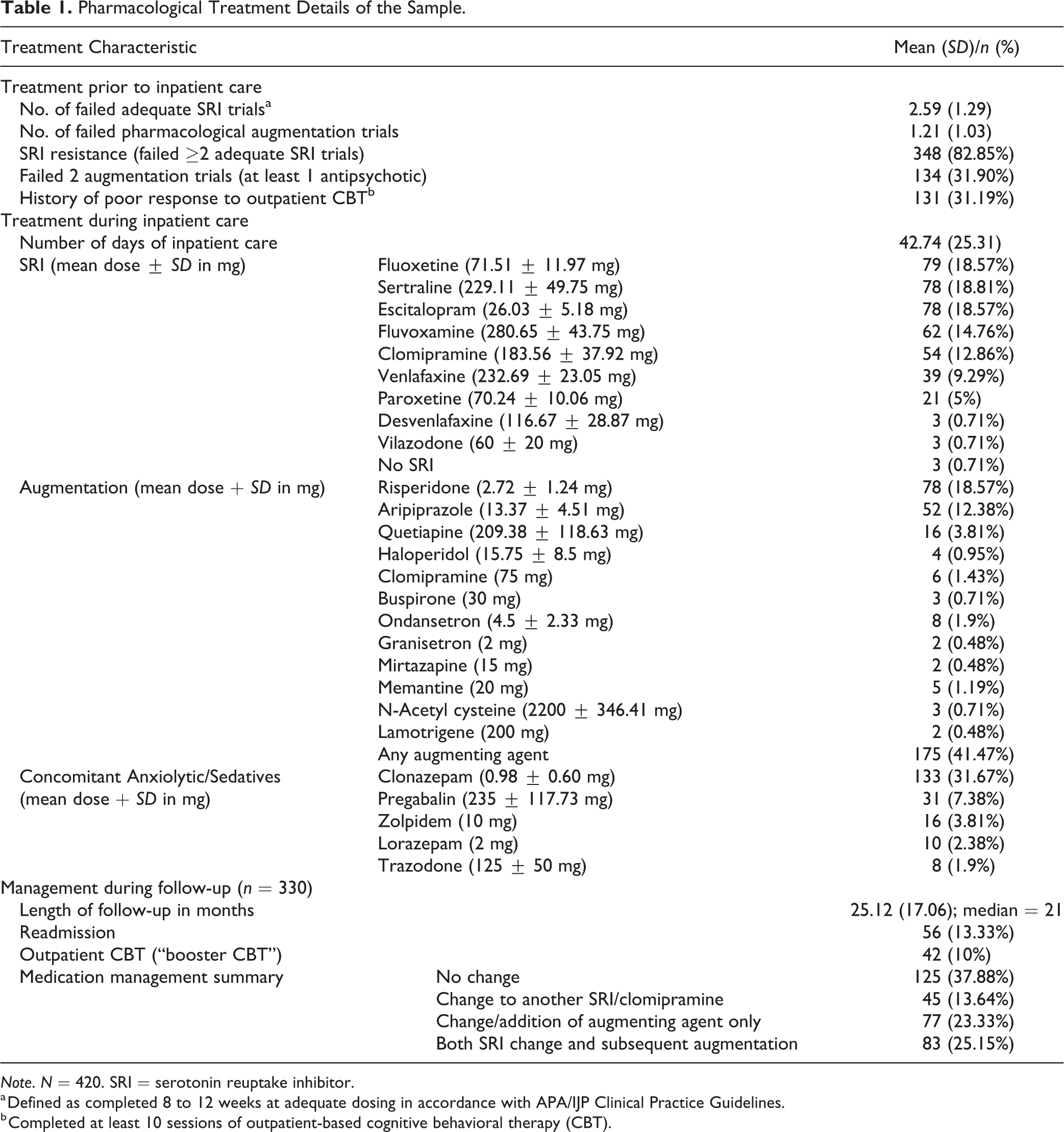
Note. N = 420. SRI = serotonin reuptake inhibitor.
a Defined as completed 8 to 12 weeks at adequate dosing in accordance with APA/IJP Clinical Practice Guidelines.
b Completed at least 10 sessions of outpatient-based cognitive behavioral therapy (CBT).
Intensive CBT (4 to 5 sessions/week, each session for 60 to 90 minutes) included psychoeducation, EX/RP with cognitive restructuring, psychoeducation, and relapse prevention. 32 Trained mental health professionals (psychiatry residents and doctoral students in clinical psychology or psychiatric social work) delivered CBT under the close supervision of a therapist with expertise in administering CBT for OCD. Following initial assessment and deciding upon the exposure hierarchy/goals, therapist-assisted EX/RP sessions were held daily for 1 hour, self-EX/RP homework tasks for 2 to 3 hours were included as part of a daily activity schedule.
Nearly all patients (409/420; 97%) stayed with a family member who was most often a parent (67%), spouse (23%), sibling (5%), or child/other relative (2%). The family member staying with the patient in the hospital was actively involved in the therapy. They were educated about OCD, theoretical rationale behind CBT (EX/RP in particular), and role of family accommodation in maintenance of symptoms. They were also frequently enlisted as co-therapists to aid in carrying out additional assisted EX/RP sessions and help in monitoring homework tasks. Progress in CBT was also reviewed in detail during the weekly grand rounds, in the presence of the therapist, patient, and family member.
Outcome Measures
Response was defined as ≥35% reduction in the YBOCS total score with CGI-I ≤2; partial response as 25% to 35% reduction in YBOCS total with CGI-I ≤3. 33 A YBOCS score of ≤12 with CGI-S ≤2 defined remission. 33
Follow-up
After discharge from the hospital, patients continued to receive treatment in a naturalistic setting (Table 1). Follow-up data were available for varying number of patients at 3 (n = 321, 76.4%), 6 (n = 262, 62.4%), 12 (n = 232, 55.2%), and 24 (n = 169, 40.2%) months. A total of 330 (78.57%) patients had at least 1 follow-up (median duration of follow-up = 20.5 [inter-quartile range 8 to 33] months).
Statistical Analysis
Chi-square/Fisher exact test and t test were used to compare categorical and continuous variables, respectively. We performed factor analysis of the main categories of the YBOCS symptom checklist (except miscellaneous) by principal component analysis with “varimax” rotation. Those components with eigenvalue greater than 1 were included, and items with factor loadings >0.5 were considered as representative of that particular factor. Factor scores (regression method) were generated for each subject for use in the subsequent analyses. For predictors of response at the time of discharge, binary logistic regression (enter method) was used. Independent variables were chosen based on extant literature on predictors of outcome of OCD 34 and of outcome of intensive residential treatment. 4 Additionally, variables with P < 0.2 in the univariate analysis were also included as predictors.
In order to assess longitudinal course of illness following inpatient treatment, we performed a censored-normal latent class growth analysis (LCGA) using MPlus (version 8.1). 35 LGCA is an approach to model classes of longitudinal treatment response trajectories based on the available data. 36 This method helps to identify whether the response patterns of individual patients fall under subclasses with distinct, homogenous trajectories. The YBOCS total scores measured at baseline, at the time of discharge, and at each follow-up were used for modeling the latent growth trajectories. The modeling procedure assumed a quadratic growth pattern underlying the response trajectories. Statistical measures like Bayesian information criterion (BIC), Akaike information criterion, sample size–adjusted BIC, Lo–Mendell–Rubin likelihood ratio test, and the bootstrap likelihood ratio test in conjunction with clinical meaningfulness of the results were used to determine the optimal number of latent classes. LCGA employs the expectation–maximization (EM) algorithm for determination of latent classes and their corresponding growth factors. This algorithm takes into account all available information on individual subjects at each time point; hence, all patients are included in the final model solution regardless of missing data. Therefore, there was no requirement for using any imputation procedure to account for the missing data. Baseline characteristics that were found to predict response at discharge were used as covariates in the subsequent conditional LCGA model, which uses a multinomial logistic regression to look for those factors that could predict “class-membership,” that is, long-term outcome trajectories.
Results
Treatment details and clinical characteristics of the sample are described in Tables 1 and 2, respectively. Principal component analysis of the YBOCS checklist items (excluding miscellaneous symptoms) resulted in a 5-component solution: PC-1 (symmetry/arranging): with robust loadings on symmetry obsessions (0.908) and arranging/ordering compulsions (0.924), PC-2 (contamination/washing): contamination obsessions (0.952) and cleaning/washing compulsions (0.947), PC-3 (hoarding/collecting): hoarding (0.946) and collecting (0.938), PC-4 (doubts/checking): pathological doubts (0.809) and checking (0.823), PC-5 (forbidden thoughts): religious (0.780), sexual (0.698), and aggressive obsessions (0.534). The 5 factors accounted for 68% of the total variance.
Clinical and Demographic Characteristics of the Sample at the Time of Admission.
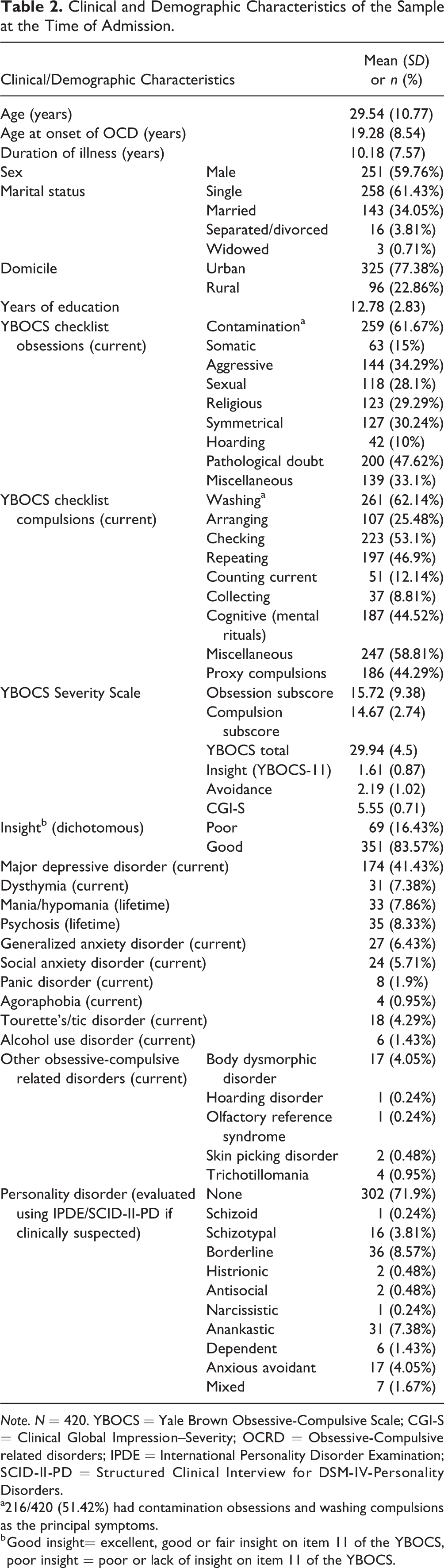
Note. N = 420. YBOCS = Yale Brown Obsessive-Compulsive Scale; CGI-S = Clinical Global Impression–Severity; OCRD = Obsessive-Compulsive related disorders; IPDE = International Personality Disorder Examination; SCID-II-PD = Structured Clinical Interview for DSM-IV-Personality Disorders.
a216/420 (51.42%) had contamination obsessions and washing compulsions as the principal symptoms.
b Good insight= excellent, good or fair insight on item 11 of the YBOCS, poor insight = poor or lack of insight on item 11 of the YBOCS.
Outcome at the Time of Discharge
The total YBOCS score declined significantly by the time of discharge, along with commensurate improvements in insight, and reduction of avoidance and global severity of illness (Table 3). More than half of the sample were “responders” at the time of discharge. Additionally, about a fifth of the sample was “partial responders.” In essence, about 70% of the sample was either “responders” or “partial responders” (297/420). In our study, about a third of our patients (n = 131) had a history of poor response to outpatient CBT. Among these, 65/131 (49.6%) were “responders,” and an additional 26/131 (19.4%) were “partial responders” at the time of discharge, similar to those who were CBT naïve (χ2 = 0.011, df=1, P = 0.961).
Outcomes at the Time of Discharge.
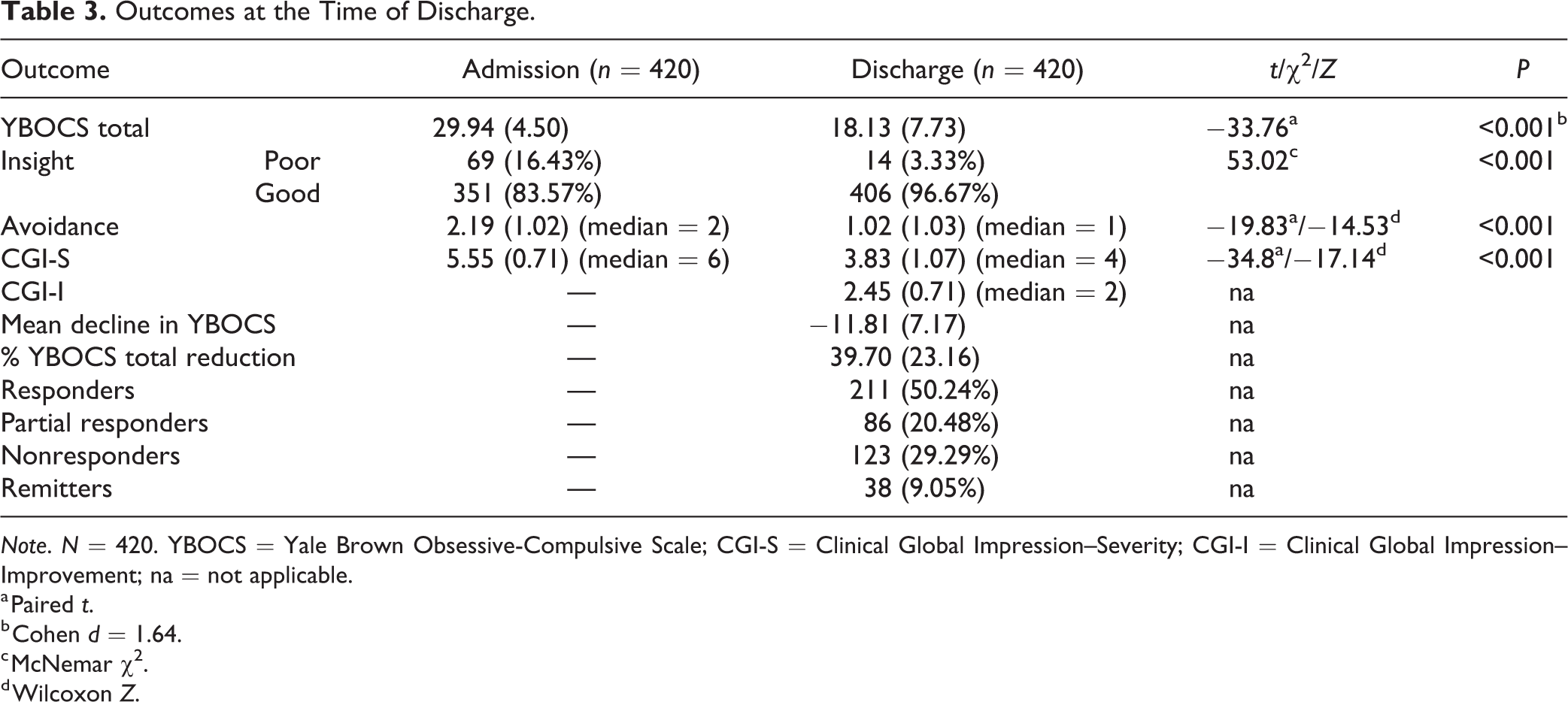
Note. N = 420. YBOCS = Yale Brown Obsessive-Compulsive Scale; CGI-S = Clinical Global Impression–Severity; CGI-I = Clinical Global Impression–Improvement; na = not applicable.
a Paired t.
b Cohen d = 1.64.
c McNemar χ2.
d Wilcoxon Z.
We compared baseline clinical characteristics (i.e., at the time of admission) of “responders” (includes “remitters”) and “nonresponders.” Compared to “responders,” “nonresponders” were overrepresented by males (138 [66%] vs. 112 [53%], χ2 = 7.306, df=1, P = 0.007), had an earlier onset of illness (18.31 [8.26] vs. 20.26 [8.73], t = 2.34, P = .020) along with a longer duration of illness (11.30 [8.01] vs. 9.11[6.97], t = 3.00, P = 0.003), poor insight (51 [24%] vs. 18 [9%], χ2=19.26, df=1, P < 0.001), more of contamination/washing (139 [67%] vs. 120 [57%], χ2=4.12, df=1, P=0.042), hoarding (25 [12%] vs. 12 [6%], χ2=5.146, df=1, P=0.023), less of current major depressive disorder (75 [36%] vs. 99 [47%], χ2 = 5.268, df=1, P = 0.021), greater lifetime psychosis (25 [12%] vs. 10 [5%], χ2 = 7.17, df=1, P=0.007), and a higher number of failed SRI (2.72 [1.46] vs. 2.46 [1.08], t = 2.063, P=0.039) and augmentation trials (1.33 [1.09] vs. 1.08 [0.95], t = 2.538, P = 0.01). In essence, they were perhaps more severely ill at baseline, also reflected in the global severity rating (5.67 [0.74] vs. 5.45 [0.67], t =3.18, P=0.002). Logistic regression analysis was then carried out using these variables and other clinically relevant factors (Table 4). The overall model had a prediction accuracy of 67.4% (Nagelkerke R2 = 0.183, P < 0.001). Significant predictors of better response at the time of discharge were female gender, shorter duration of illness, less of contamination and washing, and better insight.
Short-term and Long-term Predictors of Outcome following Inpatient Treatment.
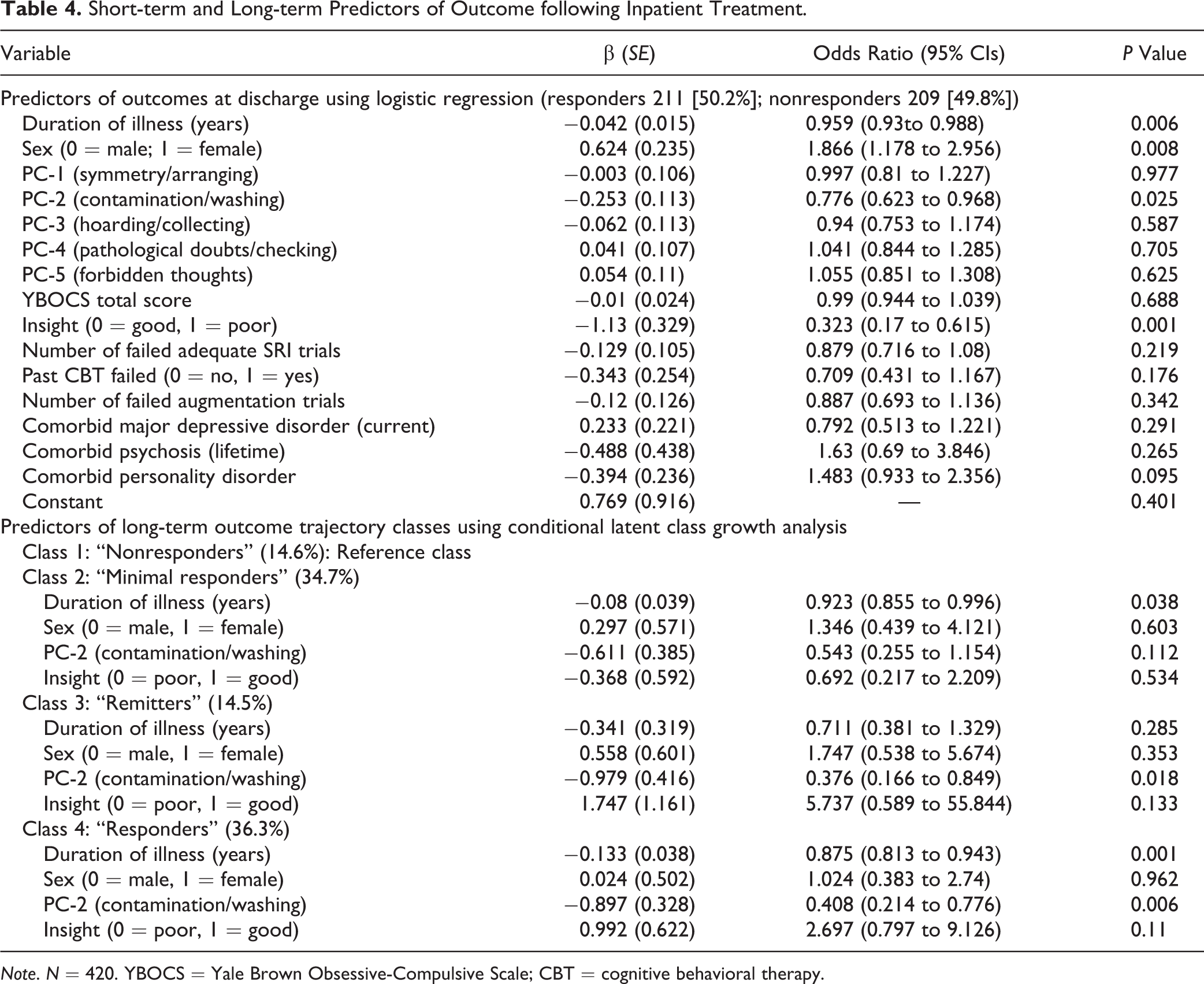
Note. N = 420. YBOCS = Yale Brown Obsessive-Compulsive Scale; CBT = cognitive behavioral therapy.
Outcomes at Long-term Follow-up
We examined whether those who were followed up (n = 330) differed from those who were not (n = 90) with respect to clinical characteristics and key outcome variables. A significant difference was found only in terms of age (younger age among those who did follow-up, P = .027). There were also no differences between the outcomes (response) at discharge in terms of YBOCS total score (t = .573, P = .567), percentage reduction in the YBOCS score (t = 1.005, P =0.315) or in the response rates (χ2 = 0.477, df=1, P = 0.515). Additionally, Little’s “Missing Completely at Random” test using EM algorithm was applied to the YBOCS total score at each time point and was not found to be significant (χ2 = 65.15, df = 49, P = 0.061).
Using the YBOCS total scores data at follow-up, latent class growth modeling was done to look for specific long-term outcome trajectories. A 4-class solution was found to have the best fit indices, with an entropy value of 0.76 which indicates a moderate level of fit. 36 As shown in Figure 1, 14.6% were classified under latent class 1 with a nearly flat trajectory (“LC nonresponders”), 34.7% in latent class 2 (“LC minimal responders”), 14.5% in latent class 3 (“LC remitters”), and 36.3% in latent class 4 (“LC responders”).
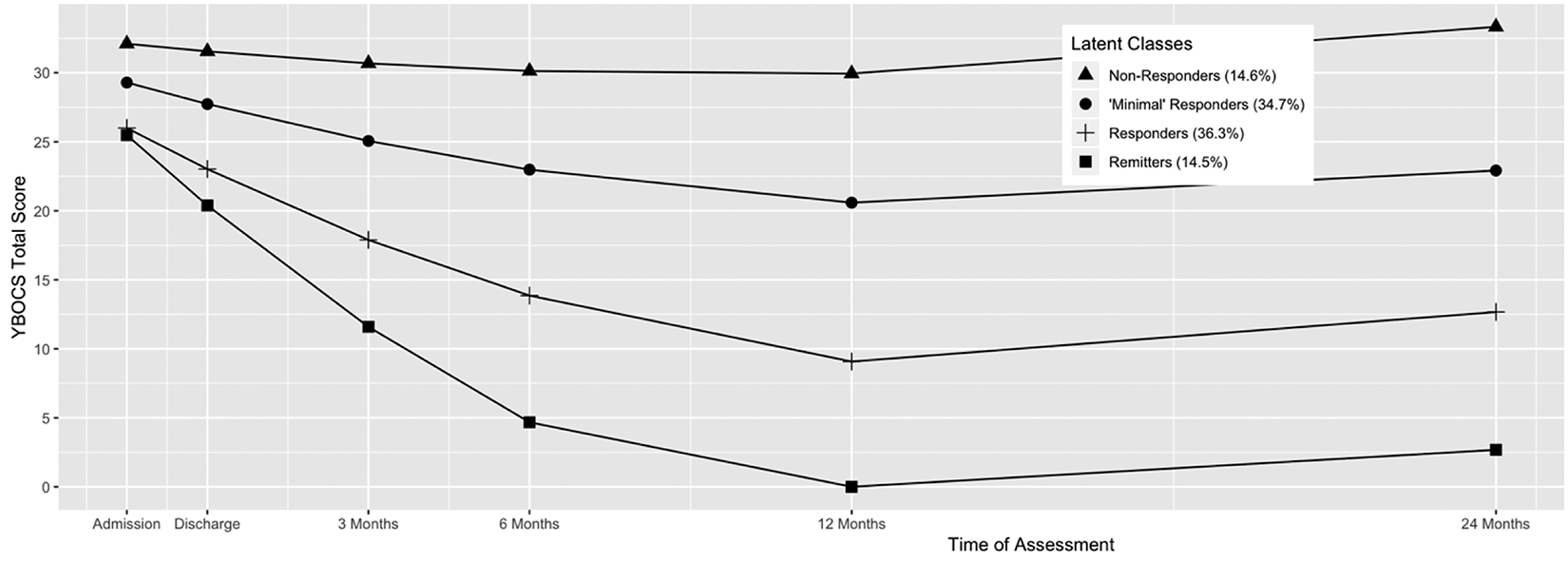
Growth trajectories of YBOCS total scores at admission, discharge, and long-term follow-up. YBOCS = Yale Brown Obsessive-Compulsive Scale. For the purpose of latent class growth curve modeling, the value of the time point “admission” was considered to be 0, and “Discharge” as 1.5 which was the mean duration of admission. Each subsequent time point—3, 6, 12, and 24 months were given the values 4.5, 7.5, 13.5, and 25.5, respectively.
Using latent class 1 (“LC nonresponders”) as the reference class, we examined whether predictors of short-term outcome (gender, duration of illness, contamination factor score, and insight) predicted long-term trajectories (Table 4). A shorter duration of illness and lesser contamination/washing (PC-2) were found to be associated with latent class 4 (“LC responders”). Lesser contamination was also found be associated with latent class 3 (“LC remitters”), and a slightly lesser duration of illness was associated with latent class 2 (“LC minimal responders”).
Since contamination emerged as one of the predictors of outcome both at discharge and at follow-up, we examined whether those with “principal contamination and washing” symptoms (n = 216, 51.4%) differed from those in whom contamination was not a principal symptom (n = 204, 48.6%). Those with principal contamination and washing were more severely ill in terms of the baseline YBOCS score (30.98 [4.55] vs. 28.84 [4.19], t = 5.013, P < 0.001), the CGI-S (5.7 [0.74] vs. 5.4 [0.65], t = 4.497, P < 0.001), the avoidance (2.47 [0.93] vs. 1.89 [1.03], t = 3.83, P < 0.001), the presence of proxy compulsions (136/216 [63%] vs. 50/204 [24.5%]; χ2 = 62.87, df=1, P < 0.001).
Discussion
Main findings of our study are as follows: (1) At discharge, about 70% had shown some response to inpatient care with a mean decline of about 12 points in the YBOCS total score. (2) During the long-term follow-up, latent class growth modeling showed that over 50% continued to retain treatment gains. (3) A shorter duration of illness, better insight, and less of contamination symptoms predict better response in the short- and long-term follow-up.
To the best of our knowledge, only two other centers have reported outcomes of such intensive residential/inpatient care in large samples, one being the McLean Hospital at Harvard in United States 5,37 –41 and the other being the National Health Service (NHS) in United Kingdom. 6 To put our findings in perspective, the similarities and differences in clinical characteristics of these two studies with those of our study have to be kept in mind. The sample characteristics in our study are somewhat comparable to those in the two large studies in that patients were severely ill and resistant to SRIs. However, the rates of comorbid illnesses, especially substance use, were much lesser in our sample similar to other studies published from our center. 42 –44 The characteristics of the interventions offered during inpatient management, that is, pharmacotherapy and intensive CBT also seem to be similar. The mean duration of inpatient stay was shorter in our study (42.7 days or 6.1 weeks) compared to that of other studies (10.4 weeks). 6 Another recent study from Norway 45 looked at the outcomes of a 3-week intensive inpatient program in a sample of 187 subjects, but this was a sample in which only 54.7% were described as “being on antidepressants,” with no other mention of the degree of their resistance to treatment. On the other hand, majority (83%) of patients in our sample were SRI-resistant. As mentioned previously, at our center, immediate family member(s) stayed with the patient in the hospital and participated in the treatment.
Outcomes
The outcome of inpatient care at discharge was highly robust (mean YBOCS reduction = 11.8 points; Cohen d = 1.64; Table 3, comparable to the finding of the meta-analysis (Mean YBOCS reduction of 10 points, and an effect size [Hegde g] of 1.87). 4 In terms of percentage of responders, the two other studies with large sample sizes also found similar rates of response, that is, 59.3% 37 and 43.2% 6 but used a 25% YBOCS reduction cut-off to classify responders, 46 whereas we employed ≥35% reduction in the YBOCS and a CGI-I score of 1 (very much improved) or 2 (much improved). 33 The recent study from Norway 45 found a much higher (79.9%) response rate using ≥35% YBOCS reduction criteria with a much shorter, 3-week intervention. This possibly could be due to lesser “treatment resistance” in their sample as mentioned earlier. Additionally, we have demonstrated that, in spite of the attrition, improvement seems to persist postdischarge from inpatient facility. The LCGA shows that about 50% of the patients were either “remitters” or “responders” during the follow-up period.
Encouraging findings of our study offer further support to routinely recommend intensive inpatient care to patients who are severely ill, resistant to SRIs, and unable to practice CBT on an outpatient basis. In our study, even those who had a history of poor response to outpatient CBT responded (responders = 49.6%, partial responders = 19.4%) following inpatient care, suggesting that inpatient care may be useful for even those who had a history of poor response to CBT in the past. It is also a common clinical experience that many patients with severe illness cannot practice EX/RP on an outpatient basis. It is in this context that findings of our study assume special significance. OCD is an illness that is typically managed on an outpatient basis, and several guidelines 47 –49 do not discuss inpatient/residential treatment explicitly as a potential alternative for severely ill patients. Only the National Institute of Clinical Excellence guidelines 50 and the Indian Psychiatry Society guidelines 31 recommend inpatient treatment before considering ablative surgery and deep brain stimulation.
Predictors of Outcome and Trajectories of Improvement
The strongest predictor of outcome both at discharge and at long-term follow-up was found to be insight. This is an important predictor frequently replicated both in naturalistic follow-up studies 51 –54 and in intervention studies. 34,55 Despite the fact that poor insight is associated with treatment challenges 56 and poorer outcome, 54 there is no controlled data that specifically address efficacy of various treatments or their combinations. Our finding further emphasizes the need to study treatment of poor insight OCD systematically.
None of the earlier studies of inpatient treatment have reported on the duration of illness being a predictor of response. However, several recent reports have found that duration of illness may be an important prognostic factor in OCD and that longer duration of illness may portend poorer outcomes. 57 –59 Hence, it is plausible that the duration of illness also has some bearing on the outcome of intensive inpatient treatment. Longer duration of illness also is known to correlate with greater illness severity, poorer insight, and worse psychosocial factors such as greater degree of family accommodation, 57 all of which are in turn known to predict poor outcomes in other studies. 60
Greater contamination and washing symptoms were also found to predict poorer response in the current study. Reasons for this is unclear as contamination/washing is known to be the “prototypical” OCD symptom and is the most common principal symptom in our sample. One possible explanation for this could be that in many patients with contamination OCD, due to the change in milieu, skills obtained in inpatient setting may not be generalizable to the patient’s own surroundings. 61 Washers in our study were also more severely ill and hence possibly gravitated toward inpatient care. This group of patients also reported severe avoidance and more proxy compulsions, the kind of symptoms that lead to more family accommodation and treatment resistance. 62
The other studies found that living alone, comorbid alcohol misuse, and higher hoarding symptoms were found to predict poor response. 4 As these factors were hardly represented in our sample, their impact on the outcomes could not be analyzed.
Strengths and Limitations
The strengths of the study include its large representative sample, systematic assessments using standard measures, and a relatively long duration of follow-up. Some of the limitations include its naturalistic design with the use of retrospective data, attrition at follow-up, uncontrolled concomitant pharmacological treatment and lack of measures of quality of life, and functioning. Even though the treatment program included participation of family members, there were no objective measures of family accommodation and functioning done. We assessed insight using a single item (YBOCS 11); a comprehensive assessment of insight using instruments such as the Brown Assessment of Beliefs Scale 63 could have been more useful.
Although it is reasonable to assume that intensive CBT played a major role since they were already resistant to SRIs and could not practice CBT on outpatient basis, one cannot attribute the outcome to only CBT because all patients received concurrent drug treatment as per the existing standards. One could even argue that the study demonstrates the efficacy of a multimodal intensive program that is a combination of rigorous CBT and optimal pharmacotherapy. Attrition rate was high, but less than in other studies, 6 and there were no significant differences in baseline clinical characteristics and time-of-discharge outcomes of those who dropped out and those who did not. Trained clinicians administered key outcome measures such as the YBOCS and the CGI, but no formal psychometric exercises were carried out.
Conclusion
Our study demonstrates that an intensive inpatient care that includes CBT and pharmacotherapy is an effective strategy in severely ill SRI-resistant patients, both in the short- and long-term. Even those who previously failed outpatient CBT seemed to benefit from inpatient care. Better response was found to be predicted by a shorter duration of illness, better insight, and less of contamination/washing symptoms. Intensive inpatient/residential treatment should be considered in resistant patients who do not improve with treatment on outpatient basis and also be a part of standard treatment guidelines. The findings of this study may have to be replicated in controlled studies.
Supplemental Material
Supplement_material - Long-term Outcomes of Intensive Inpatient Care for Severe, Resistant Obsessive-Compulsive Disorder: Résultats à long terme de soins intensifs à des patients hospitalisés pour un trouble obsessionnel-compulsif grave et résistant
Supplement_material for Long-term Outcomes of Intensive Inpatient Care for Severe, Resistant Obsessive-Compulsive Disorder: Résultats à long terme de soins intensifs à des patients hospitalisés pour un trouble obsessionnel-compulsif grave et résistant by Srinivas Balachander, Aakash Bajaj, Nandita Hazari, Ajay Kumar, Nitin Anand, M. Manjula, Paulomi M. Sudhir, Anish V. Cherian, Janardhanan C. Narayanaswamy, T. S. Jaisoorya, Suresh Bada Math, Thennarasu Kandavel, Shyam Sundar Arumugham and Y. C. Janardhan Reddy in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
The authors thank all the staff at the Medical Records Department at the institute for facilitating the data collection for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.