
Abstract
Objectives:
Physician-assisted death (PAD), also known as medical assistance in dying, of patients with a psychiatric disorder (PPD) is a global issue of debate. In most jurisdictions that allow PAD, irremediable suffering is a legal requirement, how to apply the concept of irremediability to PPD remains challenging. The aim of this article is to identify the main arguments concerning irremediability in the debate about PAD of PPD and give directions for further moral deliberation and empirical research.
Methods:
Systematic searches in MEDLINE, Embase, and PsycINFO were combined with 4 additional search strategies. All conceptual-ethical articles, quantitative and qualitative empirical studies, guidelines, case reports, and commentaries that met the inclusion criteria were included, and a qualitative data synthesis was used to identify recurring themes within the literature. The study protocol was preregistered at the Open Science Framework under registration code: thjg8.
Results:
A total of 50 articles met the inclusion criteria. Three main arguments concerning irremediability were found in the debate about PAD of PPD: uncertainty, hope, and treatment refusal.
Conclusions:
Uncertainty about irremediability is inevitable, so which level of certainty is morally required should be the subject of moral deliberation. Whether PAD induces or resolves hopelessness is an empirical claim that deserves clarification. Treatment refusal in search of PAD raises questions about treatment efficacy in this patient group and about decision-making in the context of the physician–patient relationship. Going forward, more attention should be given to epidemiological research and to specific challenges posed by different psychiatric disorders.
Introduction
Physician-assisted death (PAD), also known as medical assistance in dying, is allowed in a growing number of jurisdictions, which include Canada, the Netherlands, Belgium, Luxemburg, Switzerland, Colombia, Japan, the United States, and Australia. 1 Other countries are debating legalization of PAD. Many jurisdictions explicitly or implicitly ban patients with psychiatric disorders (PPD) from accessing PAD, but this is not the case in the Netherlands, Belgium, Luxemburg, and Switzerland. 2 In Belgium and the Netherlands, the prevalence of PAD due to psychiatric suffering has increased over the past years. 3,4 In the Netherlands, 1.1% of all cases of PAD in 2018 was due to psychiatric suffering (67 psychiatric cases in total). 3
Most jurisdictions require that the patient is in an irremediable condition. This is one of the elements that make PAD of PPD more controversial than PAD of other patients. When can we say that a psychiatric disorder is irremediable? What arguments play a role regarding this core criterion for PAD?
In this scoping review, we systematically investigate the main arguments concerning irremediability in the debate about PAD of PPD. We will identify 3 core issues, namely, arguments concerning uncertainty of diagnosis and prognosis, arguments concerning hope, and arguments concerning treatment refusal. We will show that the debate on these issues is not conclusive and that there is a need for empirical research on the one hand and normative deliberation on the other hand.
Methods
While performing this systematic review, the PRISMA scoping review guidelines were followed. 5 The project was preregistered on the Open Science Framework on February 1, 2019, and can be accessed there. 6 Ethical approval or participant informed consent was not required for this study.
Search
A systematic search was performed in PubMed, MEDLINE, and PsycINFO on November 20, 2019. We based our search on the PALETTE guidelines. 7 The search strategy combined 3 components and their synonyms: psychiatry, irremediability, and physician assisted death. A list of search terms and the syntax for PubMed can be found in Online Appendices 1 and 2. No language or publication year filters were used. After completing the database search, 4 additional search strategies were performed; first, a backward citation screening on all articles from the database search that were included. Second, forward citation tracking in Google Scholar using the 2016 landmark paper by Kim et al. 8 Third, we screened the table of contents of the unindexed special edition on Medical Aid in Dying of the Journal of Ethics in Mental Health on November 20, 2019. This special issue contains relevant contributions to the debate on PAD for PPD. While appraising articles from this journal and when describing their results, we carefully assessed the quality of the papers. Fourth, we manually included Dutch and Belgian reports and guidelines that fall within the inclusion criteria but are not available in any online scientific database. If full texts were unavailable, we contacted the corresponding author for a copy.
Source Selection
We included all conceptual-ethical articles, quantitative and qualitative empirical studies, guidelines, case reports, and commentaries if they addressed irremediable suffering due to psychiatric illness to a background of PAD. We excluded non-English or non-Dutch articles, articles without an available full text, articles that only mention irremediability in passing, and articles addressing irremediable suffering due to nonpsychiatric illness. AR and SvV performed title and abstract screening; SvV performed full text evaluation.
Data Synthesis
After full text evaluation, text segments from all included articles addressing irremediability were extracted from the articles and anonymized. All authors separately coded these segments which lead to the identification of recurring themes emerged from the literature. All definitions of irremediability and all the viewpoints that were found most important and representative for the debate on PAD of PPD were included after discussion between all authors. Since most of the sources were conceptual essays, no structural data charting or systematic critical appraisal was indicated.
Results
The database searches yielded 105 unique records, and the additional search strategies yielded 143 records (Figure 1). After full text evaluation, 50 articles were included (Table 1). Through a qualitative synthesis of the literature, we found 3 main arguments concerning irremediability in the debate about PAD of PPD: acceptability of uncertainty, influence of hope, and role of treatment refusal.
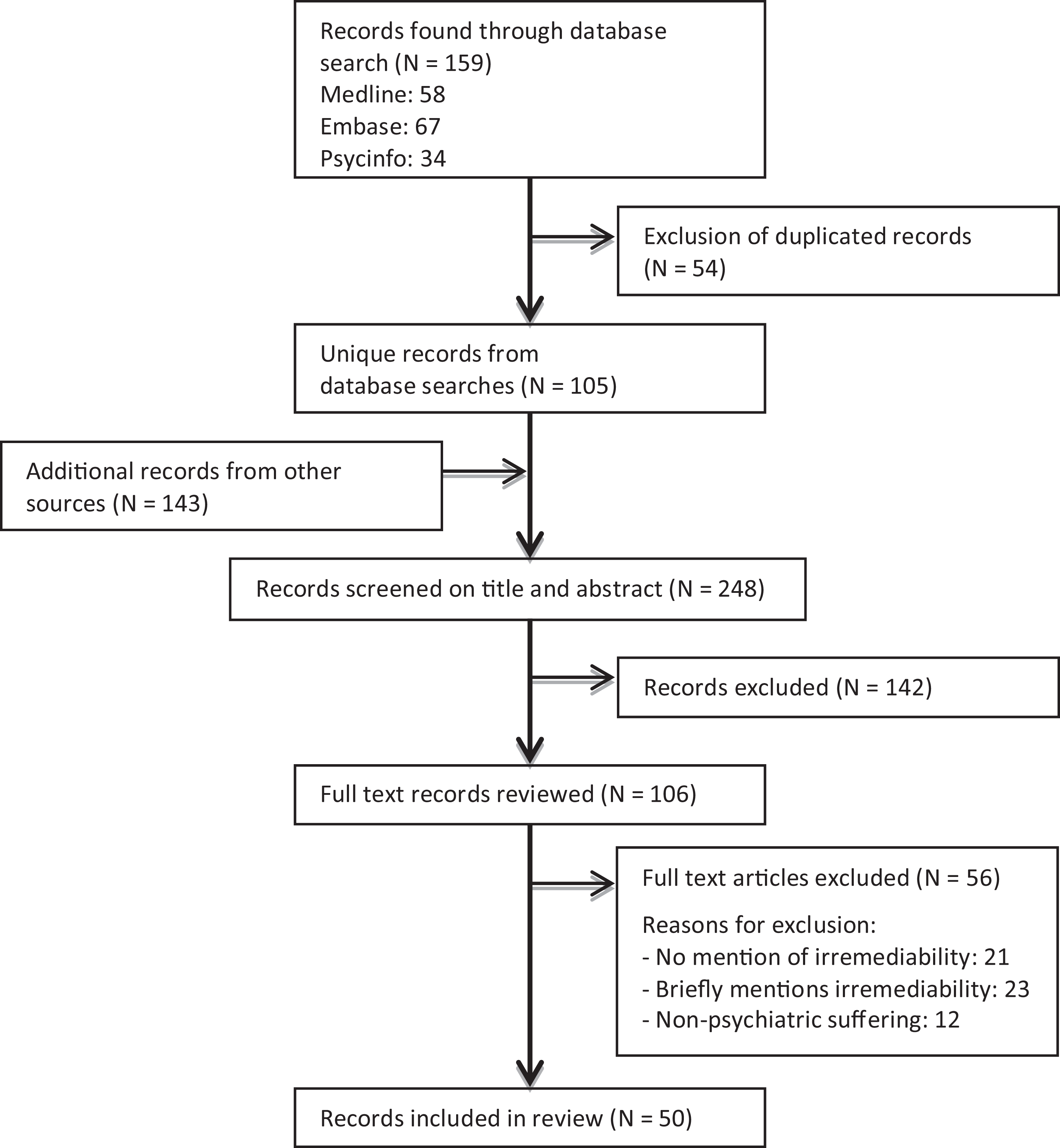
Flow diagram of the systematic search and study selection process.
Overview of Included Articles. Subdivided into Conceptual Studies, Legal Studies, Guidelines, and Empirical Studies.
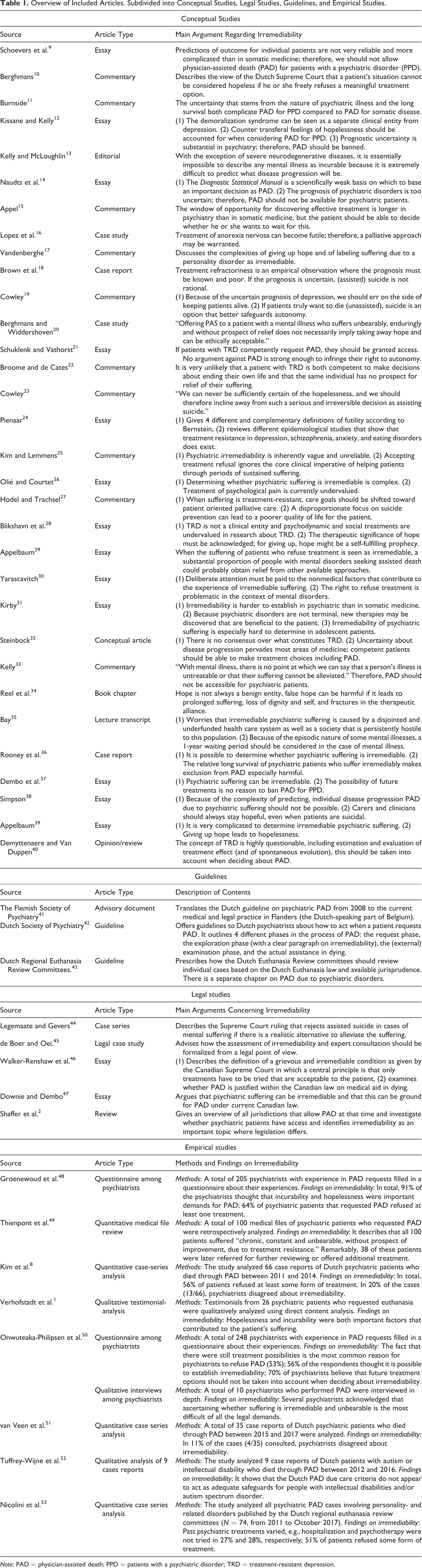
Note: PAD = physician-assisted death; PPD = patients with a psychiatric disorder; TRD = treatment-resistant depression.
Arguments Concerning Uncertainty of Diagnosis and Prognosis
Uncertainty of diagnosis and prognosis is a recurring theme in the debate about PAD of PPD. Empirical studies from the Netherlands show that there is disagreement about irremediability between psychiatrists in 11% to 20% of the PADs due to psychiatric suffering. 8,51 Several authors cite clinical studies that show that some psychiatric patients will never recover. 24,37,47 But whether these “truly irremediable” patients can be identified is subject of debate. Rooney et al. argue that irremediability can be predicted for individual depressed patients with help of staging models. 36 A questionnaire in 2016 among 248 Dutch psychiatrists found that 70% disagreed with the statement that it is impossible to assess whether a psychiatric patient suffers irremediably and unbearably, 12% agreed with this statement, and 17% was neutral. 50 In the ethical debate, however, many authors argue that it is impossible to reliably differentiate between patients who have a chance of recovery and those who do not. 9,11,13,17,26,28 Two reasons are often mentioned for questioning irremediability: the nature of psychiatric illness and the nature of psychiatric treatment.
The Nature of Psychiatric Illness
In the discussion on the irremediability of psychiatric suffering, often a comparison is made with cancer. Several authors argue that the distinction between remediable and irremediable forms of cancer is fairly straightforward for 2 reasons. First, cancer has a clear biological basis. Second, for most forms of cancer, it can be predicted whether and, within certain boundaries, when they will lead to death. 9,15,54,55 Various authors point out that psychiatric suffering differs in both aspects. First, the current psychiatric diagnostic model is said to describe syndromes and therefore offers no insight in the underlying biological, psychodynamic, or social factors, hampering the possibility of accurate prediction of disease progression. 9,14,28,30,40 Second, psychiatric disorders themselves are said not to be lethal, except maybe for severe eating disorders. 16 Therefore, patients may have a life expectancy of decades. 12,32 Various authors argue that it may be possible that in this period, new treatments are discovered, which can eventually help relieve suffering. 11,22 However, when asked about the possibility of future new treatments, 56% of 248 Dutch psychiatrists thought that this should not be taken into account when deciding about PAD, 22% thought it should be taken into account, and 22% were neutral. 50
The Nature of Psychiatric Treatment
The second reason for questioning irremediability is the nature of psychiatric treatment. First, it is argued that the broad range of biomedical and psychotherapeutic approaches offers so many (combined) treatment options that a claim about irremediability is practically impossible. 31 Second, authors argue that psychiatrists apply all these therapies dynamically, which can make it hard to determine when and why specific psychiatric treatments work and also when and why they stop working. 9 Third, authors mention that sometimes when therapists and patients stop trying to control symptoms, paradoxically, the chances of recovery improve. This is said to happen when a switch is made from a symptom reduction to an acceptance-based therapy. 26,27,28 It is also argued that a certain risk of self-harm may have to be accepted in order for the patient to recover. 56 Fourth, Tuffrey-Wijne et al. question whether medical terms such as ‘treatment refractory symptoms’ are suitable for life-long disabilities such as autism spectrum disorder. 52
Consequences for PAD of PPD
In the light of the uncertainty about diagnosis and prognosis on the one hand, and treatment on the other hand, authors reach different conclusions about the acceptability of PAD of PPD. Many authors want to restrict access to PAD for psychiatric patients. 9,12,18,19,23,33 In their view, the harm of assisting in the death of a patient who might recover justifies a ban on PAD for all psychiatric patients. As Cowley et al. put it: “if in any sort of doubt, a psychiatrist should avoid any irreversible decisions, and should err on the side of keeping her alive.”19 Proponents of PAD of PPD disagree with this assessment and argue that uncertainties are not a good enough reason to infringe on patient autonomy and continue unbearable suffering. 37,32 When a competent patient understands that it is uncertain whether their suffering is truly irremediable, it is up to the patient to decide whether or not to continue living with those chances. 15 Other proponents of PAD argue that the harm of letting a majority of truly irremediable patients suffer could be greater than the voluntary death of a minority that might recover spontaneously or benefit from future treatment. 21,24,36 Also, the nonlethality argument is disputed altogether, as patients may die through suicide, which may be regarded as worse than dying through PAD. 36 A third viewpoint balances these 2 positions, arguing that a reasonable level of uncertainty can be acceptable. 20,45 What counts as reasonable depends on the situation and has to be determined through dialogue between doctor and patient. This approach has a long tradition in the Netherlands. 57 It is embedded in the Dutch euthanasia law as well as in different guidelines addressing the subject of PAD of PPD. 42,43 However, worries about the Dutch system have been uttered, as it is said to be based on “inherently vague” criteria. 25
Arguments Concerning Hope
Hope is an often-discussed factor in the debate about PAD of PPD. Sometimes hopelessness is simply used as a synonym for an absent chance of recovery. 23,48 But more often hopelessness is seen as a state of mind, both for the patient and the doctor, not necessarily related to the actual prognosis. 12,17,28,38 A qualitative analysis of testimonies by psychiatric patients shows that feelings of hopelessness are an important and recurring reason for requesting PAD. 1
Remaining hopeful is seen as a basic therapeutic tool for the psychiatrist and as a basic condition for recovery of the patient. Opponents of PAD of PPD argue that it is unethical for psychiatrists to admit hopelessness through participating in PAD. 12,28,38 This is expressed in the following quote by Simpson et al.: “we must always seek the possibility of finding ways to help people with their suffering and help them see their ongoing life as valuable and vital, for themselves and for others who know them and love them.” 38 It is argued that the option of PAD entails a self-fulfilling prophecy: It will diminish hope in a patient, which further diminishes their motivation for treatment, which adds to the irremediability. 28 Furthermore, opening the door to PAD is seen as a dangerous message to all psychiatric patients, indicating that there indeed are hopeless conditions. 28,39 It is, however, also argued that hopelessness is already present in patients requesting PAD and is not introduced into a therapeutic relationship by discussing it. 36 Other authors argue that the possibility of PAD could give patients hope that there is an end to their suffering, thereby motivating them to pursue treatment. 17 One study found that 8 of the 48 psychiatric patients who were granted PAD in the end did not need it because “simply having this option gave them enough peace of mind to continue living.”49 Furthermore, it has been argued that giving false hope to patients contemplating death might lead to distancing from the therapist and therefore an increase in suicidality. 17 False hope may be harmful as is expressed in the following quote: “Although patients then may get support, attention, and care from others, the existential despair which is expressed in the request for PAS is not being seriously addressed.” 20 Also, authors worry that a psychiatrist who harbors false hope might resort to invasive and useless treatment that might significantly detract from the patient’s quality of life and lead to loss of dignity. 27,34
Arguments Concerning Treatment Refusal
A further theme concerns the role of treatment refusal in PAD of PPD. Treatment refusal is not only a theoretical issue; as early as 1997, in a questionnaire study among 204 Dutch psychiatrists who had experience with patients requesting PAD, it was shown that 64% of the patients who requested PAD refused a form of treatment. 48 More recently, in a 2016 study of 66 case summaries of Dutch patients who received PAD due to psychiatric suffering between 2011 and 2014, it was found that 56% of the patients had refused at least 1 treatment, ranging from psychotherapy to medication or ECT. Reasons for refusal were lacking motivation in 29% of all cases, concern about adverse effects or risks of harm in 18%, and doubts about efficacy in 15%. It was also reported that personality disorders play a common role in treatment refusal. 8 Another study from 2019 on the case summaries of patients with personality disorders found that 51% refused some form of treatment, suggesting that treatment refusal might actually be slightly lower in this subgroup. 53
Jurisdictions allowing PAD formulated different regulations concerning treatment refusal. In 1994, the Dutch Supreme Court ruled that a patient refusing appropriate treatment does not suffer irremediably, implying that in such a case, PAD is not justified. 10,42,43 Treatment is defined as appropriate if current medical opinion states that the condition of the patient can be alleviated within a reasonable time period and with a reasonable balance of burdens and benefits. 41,42,43 Again, consensus has to be reached through dialogue between the patient and physician for PAD to be justified. 42 Several Dutch authors defend this policy throughout the debate. 20,36 Canada’s assisted dying law is more patient-centered, stating that suffering is irremediable when all treatments acceptable to the patient have failed, thus leaving more room for PAD after treatment refusal. 2,41 This patient-centered view on irremediability is held by right-to-die societies and is supported by several authors throughout the debate. 2,44,46,47 Opponents of PAD of PPD argue that the patient-centered view on treatment refusal will most likely lead to deaths that could have been prevented by offering treatment. 29,30,39
Discussion
This systematic review synthesized literature addressing irremediability in the debate about PAD for PPD. The review shows that irremediability has been a central and recurring issue in this debate for over 20 years and that the arguments addressing it revolve around 3 main themes. First, whether uncertainty about irremediability can be sufficiently eliminated and how this influences the acceptability of PAD. Second, whether access to PAD introduces hopelessness in psychiatric patients and thereby contributes to irremediability. Third, whether patients who refuse certain treatments can be considered to be suffering irremediably.
Uncertainty
Absolute certainty about the prognosis of any psychiatric disorder is unreachable; psychiatry does not differ in this aspect from other medical fields. Although absolute certainty is impossible, knowledge about treatment options for individual patients can be improved. Precision psychiatry is promising in this respect. Machine learning algorithms, based on both clinical information and biomarkers, are increasingly capable of predicting treatment outcome. 58 These relatively new research methods can be used to quantify the recovery chances for an individual patient with a seemingly irremediable psychiatric disorder. This will help patients and psychiatrists to make informed decisions about PAD. It might also foster the development of new palliative psychiatric approaches that may prevent PAD. The development of new methods to reduce uncertainty will, however, not solve the issue completely. Even if knowledge of possible treatment options increases, a certain level of uncertainty will remain. Unless the proposition is a total ban of PAD, it seems reasonable to direct attention to the level of uncertainty that is morally admissible and the due diligence procedures needed to establish this level. Various safeguards might be explored, such as mandatory second opinions by psychiatrists specialized in the patient’s disorder or mandatory time between the request and performance of PAD. Qualitative research among psychiatrists with experience in PAD can provide insights and suggestions for safeguards.
Hope
It has both been claimed that PAD can induce hopelessness and that it can resolve hopelessness. A reason to doubt that PAD induces hopelessness is the finding that psychotherapists do not induce suicidal thoughts by discussing suicide with a patient. 59 Even more so, openly discussing suicidal ideation leads to better disease outcomes. 59 One might argue that the option of PAD can have the same function: By discussing PAD openly, recovery may become possible. The effect of PAD of PPD on hope requires further empirical research. This can be performed through surveys using hopelessness scales or through qualitative interviews among psychiatric patients who request PAD, or in jurisdictions that do not allow PAD, among psychiatric patients who appear to suffer irremediably. 60 Also interviewing patients who where granted PAD, but eventually choose against it, would be helpful in this respect. Such studies might help to better understand the phenomenon of hope in the context of discussing PAD with psychiatric patients. This may help psychiatrist to deal with expectations and experiences of patients. Yet, in individual cases, a clinical assessment of the reaction of the patient on the possibility of PAD in a jurisdiction will be needed, and the psychiatrist might require a second opinion and further deliberation with colleagues in order to come to a well-considered conclusion concerning the role of hope.
Treatment Refusal
Treatment refusal is a relevant issue in PAD of PPD since empirical research shows that in a considerable number of cases in which PAD was performed in PPD, the patient refused one or more treatment options. This raises questions concerning the relationship between refusal of treatment and irremediability of suffering. On the one hand, it can be argued that as long as treatment options exist, suffering is not irremediable. On the other hand, one can argue that demanding a patient to undergo different treatments for which he or she is not motivated may be ineffective and harmful, as motivation is an important determinant of treatment efficacy, especially when it concerns psychotherapy. 61 Further empirical research on reasons underlying treatment refusal is needed. Also, the efficacy of treatments that psychiatric patients who request PAD have to “undergo” in order to satisfy the requirement of irremediable suffering should be studied. This review shows that different jurisdictions allowing PAD have different ways of handling treatment refusal; the question underlying these policies is as follows: Who has agency to decide whether enough treatments have been tried before PAD is justified? If this decision is left entirely to the patient, based on the respect for their autonomous choice, patients may choose to refuse all treatment in order to candidate for PAD. Alternatively, the decision can be left to the psychiatrist, which can be seen as unduly paternalistic. A third approach is to find a balance between these options through shared decision-making; this approach is laid down in the Dutch euthanasia law. Policy-making concerning how to deal with treatment refusal in the context of PAD of PDD will require both empirical information on effectiveness of treatments and reasons for refusal and normative considerations concerning the physician–patient relationship. 62
Future Research
Our review shows that there is little empirical research available on psychiatric patients who request PAD. Until fairly recent, PAD of PPD was largely a theoretical issue, for it was only performed sporadically. The increase of PAD of PPD in certain jurisdictions offers an opportunity to further study this practice. Indeed, a few empirical studies have been performed (Table 1), but they have methodological shortcomings that are mentioned by the authors in the discussion paragraphs. The opportunity for thorough empirical studies on PAD of PPD is here now and should be used. When performing these empirical studies, researchers should not focus on “the psychiatric patient” as a single group but pay attention to differences between individual psychiatric disorders.
Strengths and Weaknesses
A strength of this review is that we performed a comprehensive and systematic study of the literature on irremediability in the context of PAD of PPD. A weakness is that the included empirical studies were of low quality; therefore, a critical appraisal of the evidence was of no added value, and the numbers mentioned should be carefully considered when used elsewhere.
Conclusion
Irremediability of suffering is an important aspect of any justification for PAD. Whether psychiatric suffering can and should be classified as irremediable has been an issue of debate for over 20 years. This systematic review showed that arguments about irremediability evolve around 3 main themes and provide suggestions for empirical research and normative deliberation. The first theme is uncertainty about irremediability. This calls for empirical research in order to diminish the level of uncertainty about irremediability as well as deliberation on what level of certainty is necessary for PAD of PDD to be acceptable. The second theme is hope. This calls for more research on the relationship between the option of PAD of PDD and the phenomenon of hope in patients and the need for deliberation in individual patient cases. The third theme concerns treatment refusal. This calls for further empirical investigation into which treatments are being refused, and why, and normative deliberation on the justification of decisions to forego treatment in the context of the physician–patient relationship. Finally, this review showed the lack of thorough empirical studies and basic epidemiological data on PPD who request and receive PAD.
Supplemental Material
Supplemental_material - Irremediable Psychiatric Suffering in the Context of Physician-assisted Death: A Scoping Review of Arguments
Supplemental_material for Irremediable Psychiatric Suffering in the Context of Physician-assisted Death: A Scoping Review of Arguments by Sisco M. P. van Veen, Andrea M. Ruissen and Guy A. M. Widdershoven in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.