
Abstract
This position paper has been substantially revised by the Canadian Psychiatric Association (CPA)’s Section on Transcultural Psychiatry and the Standing Committee on Education and approved for republication by the CPA’s Board of Directors on February 8, 2019. The original position paper1 was first approved by the CPA Board on September 28, 2011.
Introduction
Canada is a highly diverse society and, through policies of multiculturalism and a vigorous academic and research tradition of transcultural psychiatry, Canadian scholars and clinicians have been world leaders in efforts to understand the impact of culture on mental health. In response to the need for national guidelines for the integration of culture in psychiatric education and practice, an earlier version of this position paper was prepared by the Section of Transcultural Psychiatry of the Canadian Psychiatric Association (CPA) for the Standing Committee on Education. This revision updates the paper with new material reflecting advances in psychiatric education and cultural psychiatry, including competence-oriented training methods, recent research on cultural and social structural determinants of mental health and the introduction of cultural formulation interview (CFI) in DSM-5. The guidelines are based on a review of literature, experiences with existing training programs and expert consensus. This paper addresses issues relevant to general psychiatry as well as specific populations including immigrants, refugees, racialized and ethnocultural groups, as well as First Nations, Inuit and Métis.
Background
There is a large literature demonstrating the many ways that cultural variations affect the symptomatic manifestations and clinical presentation of the entire range of mental health problems including common mental disorders like depression, anxiety and trauma-related problems as well as psychoses and organic mental disorders. 2,3 These cultural variations have been shown to influence physicians’ ability to detect, diagnose and appropriately treat mental health problems. Cultural differences in health practices are also major determinants of illness behaviour, coping, treatment response and adherence, rehabilitation and recovery. There is strong evidence that cultural differences contribute to health disparities and unequal access to care and that cultural knowledge and identity are important determinants of treatment outcome. 4 –9 Inequity does not arise from cultural diversity per se but from the responses of health and social systems to diversity. Any mental health care system that aims to achieve equity must therefore address issues of cultural diversity. 10 This has been recognized by governmental and professional organizations in the United States, United Kingdom and other countries as well as Canada. 4,11,12
The Mental Health Commission of Canada, in its framework for a mental health strategy, included addressing the diverse needs of Canadians as the fourth of seven basic principles of a reformed mental health care system. 13 These diverse needs include those arising from culture and ethnicity, as well as from gender, sexual orientation, disability and other aspects of experience that interact with cultural values to influence crucial social determinants of health, access to care, quality of services and outcomes. 14,15
Cultural diversity is conceptualized in different ways in different countries based on local histories of migration, policies and ideologies of citizenship, and patterns of ethnic identity and social stratification. 16 -20 The Canadian context is distinctive in many ways. Since 1976, Canada has had an official policy of multiculturalism. 21 This formally acknowledges and promotes recognition of the diversity of Canadian society as a shared feature of collective identity. 22 It reflects and contributes to a social milieu in which attention to culture is positively valued and, indeed, required in order to respect and respond to individuals and ethnocultural communities. However, this explicit commitment to diversity is relatively recent, and the education of professionals generally has ignored the history of Eurocentric and racist policies and exclusionary practices that continue to have impact on individuals and communities. 23 –26 Recent years have seen greater recognition of the history of colonization and the devastating impact of the policies of forced assimilation on Indigenous peoples in Canada, along with appreciation of the resilience and vitality of First Nations, Inuit and Métis cultures, languages and traditions as resources for mental health and well-being. The final report of the Truth and Reconciliation Commission outlined measures to promote reconciliation, including specific changes to the health care system to ensure cultural safety. 27,28
Although Canada has been a culturally diverse nation from its inception, the geographic origin of newcomers to Canada has changed. Before 1960, over 90 per cent of immigrants were from Europe; by 2006, this had dropped below 19 per cent. At present, the majority of the more than 250,000 people who come to Canada each year are from Asia, Africa, the Middle East and Latin America—regions with great internal diversity and significant differences from the European cultures prevalent in earlier waves of migration. This new migration, in concert with recent geopolitical events, has challenged the complacency of multiculturalism, drawing attention to persisting and new forms of inequality that affect the mental health and access to services of Canada’s population. Understanding these issues is crucial for the training of psychiatrists and other mental health professionals.
Existing Training Programs and Initiatives
There have been significant efforts in the United States, United Kingdom and Australia to develop training guidelines and materials to enhance clinicians’ cultural competence. 29 -31 Most medical schools in Canada address general themes including the doctor–patient relationship, socioeconomic status and racism and provide information about the ethnocultural communities they serve, but few give adequate attention to issues of cultural or linguistic dimensions of health care access or delivery. 32 Recent efforts to address health disparities have argued for the importance of structural competency in medical training and practice. 33
Models of training in the United States have been organized in terms of the five ethnoracial blocs defined by the U.S. census (African American, Asian American and Pacific Islanders, Hispanic, American Indian and Alaskan Native and White). 17 This clustering of diverse groups into major blocs facilitated advocacy efforts of minority groups in the United States. 34 While this fosters a basic level of recognition of diversity, it downplays the heterogeneity and diversity of groups. Training based on broad cultural or geographic groups cannot address the high level of diversity in Canadian contexts, where the demographic composition is generally not that of large ethnocultural blocs but rather many smaller heterogeneous communities, including significant numbers of Indigenous peoples and refugees. 35 To respond to the diversity in Canada’s urban centres, clinicians must develop general strategies for culturally safe, competent and responsive care that can be adapted to work with diverse groups. 36,37
Surveys of training in cultural psychiatry in Canada have revealed uneven development across the country. 38 The majority of Canadian psychiatric residency programs offer limited exposure to cultural psychiatry. 39 This reflects the fact that regulatory bodies and organizations in Canada have not developed specific guidelines for training or clinical practice in cultural psychiatry. The only mention of cultural issues in the Royal College of Physicians and Surgeons of Canada (RCPSC) accreditation standards states: “Learning environments must include experiences that facilitate the acquisition of knowledge, skills and attitudes relating to aspects of age, gender, culture and ethnicity appropriate to psychiatry (p. 9).” 40 There is also mention that there must be facilities for supervised experience in community consultations. There is no mention of other specific topics or populations including immigrants, refugees, ethnocultural communities, or the use of interpreters. A CPA position paper on training for work in rural and remote areas makes brief mention of the importance of attention to local culture and of Indigenous mental health issues. 41 Earlier position papers on training in emergency psychiatry and substance abuse both acknowledge the relevance of sociocultural factors; however, no detail on curriculum is provided. 42,43
Key Concepts
There have been substantial advances in cultural psychiatry in recent years that can inform a basic curriculum. Work in developing curriculum, didactic methods and resources for training has been conducted at several universities in Canada. 44 -49 In this section, we summarize key concepts for a core curriculum.
Culture, Race and Ethnicity
The notion of culture covers a broad set of meanings that have shifted with changes in the configuration of societies and in our understanding of the nature of communities and traditions. 50 Culture includes all of the socially transmitted aspects of a way of life, from values and knowledge to social behaviours and practices. As such, institutions and bodies of technical or professional knowledge and practice like psychiatry are also imbued with culture. Cultures also produce forms of social identity, including racial categories and ethnicity, which may be ascribed to individuals. The process of racialization categorizes people on the basis of their appearance or some other characteristic. 51 -53 Although there is no coherent biological definition of race, racialization is important because of racism, which has been shown to have direct impacts on physical and mental health but also through the fundamental impacts that racism has on exposure to social determinants of health. Institutional racism, discrimination, social exclusion and oppression also can influence the way that groups perceive and interact with health services. 54 Ethnicity refers to the ways in which groups identity themselves as historical peoples or communities. 55 The dynamics of culture, race and ethnicity are not simply intrinsic to a group but depend on interactions among groups within a larger society. Canada has its own unique history and dynamics relevant to identity and mental health. 56
Cultural Biology and Cultural Neuroscience
Older notions of culture defined it in contrast to (human) nature, which was assumed to be rooted in a universal biology. There is increasing recognition that there are local biologies 57 that reflect culturally mediated differences in human populations, based on diet, ways of life and coevolution with selection for specific genetic polymorphisms. 58,59 These variations may contribute to behavioural differences across populations as well as to pharmacokinetic and pharmacodynamic differences in medication response. 60 Brain development depends crucially on the social environment, which is shaped by cultural practices. 61,62 A growing body of work in cultural neuroscience reveals ways in which differences in child-rearing and everyday social contexts influence neuropsychological mechanisms of attention, memory, cognition and emotion, self-representation and psychopathology. 63 -65
Social and Cultural Determinants of Health and Health Disparities
Cultural differences result in particular social statuses, identities and positions, which are associated with varying exposure to particular types of social determinants, adversity and access to resources, including health services. This results in substantial disparities in the prevalence of specific mental health problems and health outcomes. Local cultural values, practices and institutions interact with larger social determinants of health including globalization, migration and urbanization. Complex interactions between vulnerability, individual and community resilience, and the social determinants of health, influence the risk of specific mental health problems for different groups. As a result, there are significant differences in the rates of mental health problems between groups in Canada. 66 For example, in Ontario, the rates of psychosis are 60 per cent higher for Caribbean immigrants than they are for Canadian born or African immigrants; however, the rates of psychosis among those from the Philippines are 50 per cent lower. 67 Refugee populations tend to be at increased risk of both common mental disorders and psychosis, but the risk of illness is influenced as much by postmigration issues as it is by premigration factors such as exposure to violence. 68 A nuanced approach to understanding and considering these influences in assessment, treatment and research is most likely to produce better outcomes. 69
Racism, Prejudice and Discrimination
Among the most important social determinants of health are systematic exposure to discrimination and exclusion which may be associated with explicitly racist ideologies or with more implicit forms of bias and discrimination both at the level of individuals’ behaviour and as part of routinized institutional practices. 54,70,71 These forms of discrimination result in structural inequalities as well as in everyday practices of stereotyping, misrecognition, denigration and “microaggression” that may have negative effects on mental health and service delivery. 72
Institutional Racism
Institutional racism, defined as institutional failures to provide appropriate care and services because of culture, ethnic origin or race, is a particular concern in mental health care settings. Even where individuals are not explicitly racist, institutional racism can be seen or detected in attitudes and behaviours which amount to discrimination through unwitting prejudice, ignorance, thoughtlessness and stereotyping that can disadvantage minority groups. 73,74
Migration, Colonization and Mental Health
Migration and colonization may involve rapid culture change. When such change is forced and undermines core cultural values, it may contribute to acculturative and social stress, identity conflicts, family conflict and other mental health issues. 75 A literature on postcolonial psychology examines the social, political and mental health consequences of these histories for contemporary populations, including Indigenous peoples and many immigrant groups. 76,77
Cultural Influences on the Mechanisms of Psychopathology
Culture may contribute directly to the underlying mechanisms of psychopathology by influencing the neurobiology of mental disorders through developmental experiences, diet and other aspects of behaviour, as well as by shaping the form and content of cognitive and interpersonal processes. 78,79 Examples include the diverse types of panic disorder that depend on culture-specific interpretations of sensations 80 and the variations in the form and prevalence of dissociative disorders reflecting the use of dissociation in religious and healing traditions. 81
Illness and Help-Seeking Behaviours
Cultural understandings of the nature of sensations, symptoms, illnesses and other types of problems guide coping, help-seeking and health care utilization. Independently of their contributions to the mechanisms of psychopathology, cultural knowledge and practices are therefore important considerations in improving access to health care, recognizing and responding appropriately to patients' concerns, negotiating treatment and ensuring adherence.
Cultural Competence and Cultural Safety
A variety of frameworks have been developed to address the organization and delivery of mental health services in ways that are respectful of and responsive to the unique social, cultural and political situations of different groups. Much of this work has been framed in terms of notions of cultural competence, which includes awareness of the impact of the clinician’s own ethnocultural identity on patients, knowledge of the language and cultural background of groups seen in clinical practice and their interactions with mental health issues and treatment, the skills for working with particular groups, and the development of an organization or system that is capable of offering equity of access and outcome to diverse populations. 82 -84 In addition to cultural competence, the Mental Health Commission of Canada has embraced the framework of cultural safety, originally developed in New Zealand, which emphasizes the power differentials and vulnerability inherent in clinical situations involving dominant and subdominant groups in society. 85 -87 Cultural safety builds on knowledge of historical and political experiences of oppression and marginalization to give explicit attention to structural and organizational issues that protect the voice and perspective of patients, their cultures and communities.
Clinical Assessment and the Cultural Formulation
DSM-5 includes a cultural formulation interview (CFI) and Outline for Cultural Formation (OCF) for collecting and organizing clinically relevant cultural information into a diagnostic formulation. 88 The CFI is presented both in patient and key informant versions and 12 supplementary modules are available to assess specific domains (explanatory models, level of functioning, social networks, psychosocial stressors, spirituality, religion and moral traditions, cultural identity, coping and help-seeking, and the patient–clinician relationship) and issues related to specific populations (children, elders, migrants, caregivers) as well as detailed guidelines for conducting CFIs with patients and their families. 89 DSM-5 also introduced important constructs for assessing cultural concepts of distress including cultural explanations, idioms of distress, cultural syndromes and folk diagnoses. 90
Working with Interpreters and Culture Brokers
Over 20 per cent of the Canadian population has a mother tongue which is not English or French. They may want or need to use these languages in times of crisis or distress. Effective communication is essential to accurate diagnosis and the negotiation and delivery of effective treatment. In situations where patients and clinicians are not fluent in the same language, safe and effective care requires the use of professional medical interpreters. 91 Practical constraints and professional attitudes contribute to a reluctance to use interpreters. 92 As a result, trained interpreters continue to be underutilized in health care. Even when linguistic communication is established, cultural formulation may require the use of culture brokers or mediators, that is, resource people or professionals with in-depth knowledge of the specific cultural and social background of the patient as well as knowledge of the medical systems, who can function as go-betweens, brokering mutual understanding and collaboration. Interpreting in child psychiatry requires specific training both for the clinician and the interpreter in order to address the challenge of assessing development across cultures as well as intergenerational conflict within immigrant families. 93
Information and Communication Technologies and Social Media
The rapid development of information and communication technologies and social media have had substantial impact on many facets of mental health and service delivery and will become increasingly important in the years to come. There are at least four ways in which these technologies must be considered in training in cultural psychiatry, related to their impact on (1) individual development, identity and well-being; (2) changing social networks and communities (e.g., diasporic and transnational communities, groups formed around common interests or concerns including illness); (3) new forms of psychopathology (e.g., problematic Internet, cellphone or video game use) and (4) the delivery of mental health information and interventions. 94 -96 All of these domains interact with specific social factors and require expanding our notions of culture and context and addressing diversity to ensure equitable access and effectiveness.
Computational Psychiatry
Efforts to use bioinformatics and artificial intelligence to develop methods for more precise clinical assessment and targeted treatment must take into account social and cultural diversity. Current diagnostic and treatment algorithms generally pay little attention to diversity, and clinicians need to be trained in how to apply these tools in ways that integrate culture and context in a developmental and ecosocial frame. 97,98
Policy Issues
The design and implementation of culturally safe and competent mental health care systems and institutions requires attention to structural and organizational issues at multiple levels. 99 Overarching demographic patterns and social policies of immigration and integration shape these service responses. Human rights, multiculturalism, interculturalism and other approaches to diversity, influence the legal and economic support for, as well as the feasibility and acceptability of, specific models of service organization. 100,101
Global Mental Health and Human Rights
There is increasing recognition and effort to provide effective psychiatric services in low- and middle-income countries where mental health problems are major contributors to the burden of illness. Cultural issues are central in efforts to export and adapt interventions. Respect for culture, as essential to human identity and well-being, is also a human right. Culture itself raises complex ethical and human rights issues in the ways it defines such basic dimensions of social difference as developmental stage, gender and collective identity.
Indigenous Mental Health
Indigenous peoples constitute about four per cent of the Canadian population but bear a disproportionate burden of mental health problems. 102,103 Although there is wide variation across groups, the higher rates of psychiatric and substance abuse disorders found in many segments of the Indigenous population can be linked to the enduring effects of historical social, economic and political policies of forced assimilation, marginalization and discrimination. 104 -107 The Indian Act, the Indian Residential School system and the child welfare system have had profound effects on the mental health of Indigenous populations. 108 -110 These historical events have resulted in what has been termed “intergenerational trauma.” In response, Indigenous individuals and communities have developed unique resources and strategies of resilience reflecting culture, language, spirituality, and connections to family, community and place to mitigate the effects of intergenerational trauma and ongoing structural violence. 111
There is wide recognition of the need for training in cultural safety and competence to respond to the mental health needs of Indigenous peoples. 112,113 Many communities are located in remote regions posing logistical problems in delivery of care that require consideration of specialized approaches with close collaboration with community workers, mobile crisis and consultation teams and telepsychiatry. More than 50 per cent of Indigenous peoples in Canada live in cities where they may not have access to culturally appropriate services that respect and make use of their language, cultural and spiritual traditions. Indigenous organizations have identified cultural safety as an important framework for the development of training programs and institutional changes to improve the quality and appropriateness of mental health care. 114 -116 Cultural safety focuses on addressing the structural inequalities and power imbalances that make clinical encounters unsafe for Indigenous people. 87,117,118
The Indigenous Physicians Association of Canada and the RCPSC have developed core curriculum and clinical interviewing training materials for residents. 119,120 Training involves reading, discussion, role-playing and interaction with trainers from Indigenous communities to provide (1) basic understanding of the links between historical and current government practices and policies toward First Nations, Inuit and Métis Peoples and the social determinants of health, access to health services and intergenerational health outcomes; (2) reflection on trainees own cultural values and emotional responses to the history, identities and contemporary events involving First Nations, Inuit and Métis. The curriculum developed for family medicine residents also addresses specific clinical skills relevant to psychiatry including (1) cultural safety in clinical interviewing, (2) identifying culturally appropriate community resources for treatment and (3) developing an integrated treatment plan. Recent publications provide guidance on training in cultural safety and Indigenous mental health issues. 121,122
Core Competencies and Essential Skills
Cultural competence requires changes at the levels of systems, practitioners and interventions. 31,36 At the level of practitioners, cultural competence attitudes, knowledge and skills that enable a mental health professional to provide competent, equitable and effective care to meet the diverse needs of all patients. 123 This requires addressing basic cultural issues including (1) the clinician’s own identity and relationship to patients from diverse backgrounds; (2) communication skills and familiarity with how to work with interpreters and culture brokers; (3) conceptual models of how cultural context and background influence developmental processes, psychopathology, help-seeking, coping, and adaptation to illness, treatment response, healing, recovery and well-being, as well as moral and ethical issues; (4) specific knowledge of the particular populations and communities with which the clinician is working. 44,124 Practitioners also need to understand the importance of cultural adaptation of care pathways and interventions as well as how to advocate at the system level for equitable systems and indicators that allow the measurement of progress toward equity of access and outcome.
At the centre of cultural competence are relational skills and processes to build trust, mutual understanding and collaboration, integrated with understanding the phenomenology and situated meaning of symptoms and illness experience.
125
-127
Acquiring cultural competence requires didactic teaching, mentorship and supervised experience in appropriate clinical and community settings to address each of these domains. At a minimum, this would include: The opportunity to explore and reflect on one’s own cultural background and identity as a resource and a source of bias and to address the interpersonal and institutional dynamics of racism, power disparities, social exclusion and acculturative stress as they impact on mental health and clinical work. Basic knowledge of current research and conceptual models in cultural psychiatry, medical anthropology and cross-cultural psychology relevant for understanding social and cultural influences on the mechanisms of psychopathology as well as cultural variations in symptom expression, help-seeking, treatment adherence and response. Training in working with medical interpreters and culture brokers as well as immigrant settlement workers, community workers, counselors, helpers and healer.
128
Familiarity with the values, perspectives and experiences of local communities pertinent to psychiatric care, including ethnocultural and racialized groups, immigrants, and refugees across all age groups and life cycle stages (child, youth, adult and elderly), Experience collecting social and cultural information through individual and family interviewing and assessment and in preparing cultural formulations using the CFI and OCF in DSM-5 or comparable tools. Experience negotiating treatment with individuals, families and wider community networks relevant to care for patients from diverse backgrounds.
Each of these areas involves didactic teaching, clinical experiences, and the creation of specific learning and practice settings to allow ongoing discussion, reflection, and integration of attitudes, knowledge and skills.
An organizing framework is needed to articulate these training needs as specific competencies. One of the major advances in medical education has been the shift from Flexnerian model of structure and process-based training toward competency-based training. 129 The RCPSC initiated the Canadian Medical Education Directions for Specialists (CanMEDS) project in 1993, with revisions in 2005 and 2015. 130 CanMEDS shifted the focus of training from the interests and abilities of the providers to the needs of society. In addition to the traditional role of medical expert, the specialist physician’s roles include communicator, collaborator, leader, health advocate, scholar, and professional. The CanMEDS framework is particularly relevant for further development as a blueprint for cultural competence training. In the most recent update, cultural safety has been explicitly highlighted in the communicator role. 130 In Table 1, we link specific core cultural competencies to each of the CanMEDS roles and the corresponding enabling competencies.
Core Cultural Competencies and Milestones in the CanMEDS Frameworka

a Adapted from Rotation Specific Educational Objectives and Draft Milestones for Sociocultural Dimensions of Psychiatry developed by Fung K, Munshi A, Andermann L, and Pillar 4 Workgroup for the CBME Steering Committee, Department of Psychiatry, University of Toronto.
b A = attitude; K = knowledge; S = skill
c CanMEDS 2015 Enabling Competencies
In addition to capturing competencies as roles, the RCPSC is committed to a shift toward competency by design (CBD) for all postgraduate training. This differs from traditional medical training by shifting from a time-based, rotation-centred, knowledge acquisition curriculum toward a more learner-driven approach, with progress in training marked by attaining observable skills through frequent formative as well as summative assessments. 131 Pragmatically, most postgraduate programs will likely adopt a hybrid format retaining some form of clinical rotation structure with increased flexibility.
The CanMEDS Milestones outline the skills to be attained under each role at each stage of training. 132 The stages of training are divided into (1) transition to discipline, which may take the form of a “boot camp” ensuring that medical graduates from different medical schools inside and outside Canada are ready to begin residency training with standard basic skills (also see CPA position paper on IMG training); (2) foundations of discipline, junior residents foundational training; (3) core of discipline, senior residents training covering the majority of core competencies; and (4) transition to practice, senior residents training after the Royal College Examination in preparation for the transition to independent practice. In Table 1, we have developed draft milestones for the core cultural competencies to guide curriculum design, implementation and evaluation.
Another concept in CBD is the entrusted professional activities (EPAs), which describes observable clinical tasks that supervisors may entrust trainees to perform under varying degrees of supervision depending on their level of competence. Each delineated EPA integrates relevant enabling competencies from the different CanMEDS roles. For example, the clinical task of providing care to a refugee naturally encompasses competencies associated with medical expert, communicator, collaborator, professional and health advocate roles. While the use of EPAs and milestones vary, in Canada the current direction is toward the use of competencies and milestones to facilitate curriculum design and implementation of teaching, while EPAs may be used to facilitate assessments and feedback. There will be a relatively small number of EPAs being developed to assess each stage of training. Cultural competence and safety needs to be explicitly included in the EPAs with the corresponding competency milestones mapped on to them as there is a tendency to erroneously assume that the dominant discourse, considerations and approaches adequately address the needs of marginalized or minority communities.
There are a number of specific considerations in designing and implementing a CBD curriculum in cultural psychiatry. First, there needs to be a shift in emphasis toward the teaching and attainment of observable clinical skills, away from didactic knowledge-based teaching. In cultural psychiatry, attitudes, knowledge and skills captured by some of the competencies are complex and may not be readily taught or observed in everyday clinical encounters, especially as they vary depending on the particular clinical context. Experiential learning through individual or group reflective exercises, the use of a “flipped” classroom with online resources and the increased use of simulation for cultural psychiatry teaching need to be developed. Second, as frequent work-based assessment and feedback are required, clinical supervisors not traditionally involved in cultural psychiatry teaching may need to facilitate the teaching and evaluation of cultural competence and safety, reinforcing the need for faculty development. Interprofessional and community partners who will increasingly be involved as collaborators or teachers also need to be engaged in this process. Finally, indicators of cultural competence need to be thoughtfully integrated with the new tools being developed to evaluate EPAs and competence milestones, including brief clinical evaluation exercises (mini-CEX) and similar paper or online assessment tools.
To facilitate the design of a Cultural Competence Curriculum to fulfill the specified CanMEDS competencies, major organizing themes from the field of cultural psychiatry can be identified as basic teaching modules: Culture and Health; Culture, Illness and Psychopathology; Culture in Clinical Practice; and Culture and Health Care Policy, Services and Systems (Table 2). A model curriculum with specific learning objectives outlined for each of the four teaching modules is summarized in Table 3.
Core Themes in Cultural Psychiatry Curriculum

Learning Objectives in a Cultural Psychiatry Core Curriculum.

A = attitude; K = knowledge; S = skill
As the objectives involve development of trainees’ attitudes, knowledge and skills, a variety of pedagogical methods must be employed to facilitate learning, including: (1) individual or group reflective exercises and assignments in a safe environment to facilitate personal shifts in attitudes; (2) prescribed readings, didactic presentations and case studies to increase trainee’s knowledge in key concepts and issues of providing care for diveserse populations; and (3) role-playing, observed interviews, direct patient care, and family and community interventions and collaborations to provide essential learning opportunities for skill acquisition through modeling, feedback and supervision.
These three sets of approaches overlap and reinforce one another. For instance, direct experience in working with a particular patient population not only increases clinical skills but may also lead to increased working knowledge as well as attitudinal shifts, especially if facilitated by appropriate supervision. The first two groups of learning activities may be actualized strategically and expediently through cultural competence seminars, case conferences and rounds, while the latter is most effective if ecologically integrated and embedded with the various rotations throughout the entire residency. 133 This latter integrative approach is a particularly important element in order to avoid conflating basic cultural competence with cultural psychiatry as a subspecialty applicable only to cultural psychiatrists; rather, it reinforces the position that cultural competence is an essential and necessary core competence in every clinical encounter for every psychiatrist. 44 This training implication is that faculty members of all rotations need to receive training and support to maintain and improve their own basic cultural competence, as well as acquiring expertise to teach and evaluate it.
Community-based groups, institutions and organizations are important sources of knowledge and experience. They can offer support, guidance and information on the needs, illness models and histories of local groups which may be of significance in their exposure to risk factors for the development of health problems and their capacity to access and use services. They may offer specific services themselves that are more culturally consistent or, at times, may be a source of stigma and a barrier to people getting optimal mental health care. They are a potential useful ally in the development of culturally competent services as well as the individual development of knowledge. Knowing how to identify and develop working relationships with community-based organizations is an important skill in a diverse setting.
The reorganization of mental health services around shared care models calls for a shift in the role of psychiatrists who need to develop specific skills to become effective consultants for primary care professionals. This includes: (1) understanding the interinstitutional and systemic dynamics that influence partnership, referral, follow-up and joint care of patients; (2) the capacity to conduct an ecological appraisal of individual, family and community resources and translate this into a multisectoral intervention plan and (3) flexibility in shifting between different aspects of the consultant role while preserving a clear focus on the clinical goals.
Pedagogical Methods
Cultural psychiatry involves pragmatic and political issues of equity in health services as well as fundamental scientific questions about the nature of psychopathology. Training therefore needs to balance experiential learning that focuses on attitudes and enhances skills, with didactic and conceptual teaching that emphasizes models, methods and data. 38
Training in cultural psychiatry requires creating settings that encourage a self-reflective process in which trainees become aware of their own cultural and sociopolitical premises and assumptions. These may be grounded in their identity and personal history but also arise from aspects of collective experience of which they are unaware. For example, histories of colonization have shaped the identity of many peoples and the resultant attitudes toward authority and emblems of dominant and subordinate groups will influence attitudes and behaviour in the clinical setting.
Understanding and respecting the cultural background of the other involves attitudes of interest and humility—while there is a common core of human experience that allows empathy across cultures, important details of each individual’s background remain difficult to fully appreciate without extensive exposure over time to their social realities. 134 Thus, trainees who tend to be focused on mastery, acquiring professional authority and competence, must learn to tolerate ambiguity, uncertainty and not knowing—and develop the confidence to allow patients a measure of control over their own social positioning and gradual self-disclosure. The intercultural clinical encounter is a mirror of similar encounters in the larger society and brings with it all of the cultural and historical assumptions, tensions and expectations that frame such everyday interactions. Clinicians must learn to use their own identity, both in terms of self-understanding and with an awareness of how they appear to others given this social historical background, as a tool to explore patients’ identity, illness meanings, the social context of illness and adaptation and the clinical relationship itself. 135 This self-awareness is the focus of experiential learning and clinical training.
Capitalizing on the diversity of backgrounds among trainees and professionals themselves can provide an excellent way to foster positive attitudes and encourage more empathic understanding of the realities of immigrant and minority experience. This requires training and practice environments in which it is safe for clinicians to reflect on and discuss cultural issues. The development of a discussion and reflection group for trainees insulated from the formal evaluation processes of training can facilitate more open, personal exchange. Recognizing that clinicians each have their own unique life trajectories and cannot represent the diversity of any cultural group because of variations in social class, education and acculturation can reduce the tendency to stereotype.
To make use of their cultural knowledge, however, clinicians also need conceptual frameworks from cultural psychiatry and social sciences that make explicit the role of culture in health and illness. In addition to understanding how their own backgrounds influence the clinical interaction with others, trainees need to consider the ways in which the concepts and practices of psychiatry are based on specific cultural constructs and values. For example, the emphasis on autonomy and individual choice as indicators of psychological health and as goals for therapy reflects the dominant values of individualism. These are challenged by traditions that place a higher value of family or group harmony and consensus. Thus, the clinical setting can be seen as a space of negotiation between different cultural systems of knowledge and practice and different value systems. These reflect not only the ethnocultural backgrounds of patient and clinician but also to the implicit values and ideologies that structure medical knowledge and the health care system. 136 -138 Medical and psychological anthropology provide conceptual frameworks and comparative studies of health care systems that can inform clinical work in cultural psychiatry. Among existing models in psychiatry and allied mental health disciplines, the perspectives of family systems theory and family therapy are most readily adapted to understanding the particularity of migrant individuals and ethnocultural communities. The emphasis on systems or networks of relationships fits well with the values of people from many backgrounds.
Awareness of differences in cultural knowledge, values and orientations provides a foundation for learning the essential skills of cultural psychiatry: (1) establishing a working alliance in the context of power imbalances, divergent values and differing views of the world; (2) formulating problems in terms of specific social and cultural dynamics and (3) developing treatment plans that mobilize available resources and negotiating interventions with patients, their families and communities.
Intercultural work also requires tolerance for ambiguity. 126,139 This poses a challenge for models of professional practice that emphasize mastery and efficiency. There must be space for clinicians to acknowledge the uncertainty in assessment and treatment and time to clarify assessment and negotiate appropriate interventions. In training, this requires a supportive environment. In health care institutions, it requires structural changes to allow the additional time and resources needed to provide adequate care.
Ultimately, the wide implementation of culturally safe and competent practices depends on institutional changes. Clinicians may be key actors in initiating and promoting such change. Problem-solving with trainees around the construction of a support network (at the level of clinical team and institution) can support the shift in clinical practices from a model centred on professional expertise to one that is more patient- and person-centred and that can deal with uncertainty. 127
Pedagogical methods useful for training in cultural psychiatry include: Case studies: Clinical case conferences and other settings where individual cases are discussed provide a key method for learning the process and content of cultural formulation. Cultural formulations also serve to emphasize the importance of family, community and other social systems issues for many patients. The case study method, which is standard in medicine, can be used to analyze the complexity of cultural influences on patient presentation and evolution and also to identify the cultural dimensions of clinicians’ positions and to work on biases and unexamined premises. Education in pluralism: Cultural psychiatry rests on a basic respect for diversity in worldviews. This diversity includes notions of knowledge, authority and values that may be radically different. Working with such radical difference requires some understanding of philosophical and ethical notions of pluralism as well as skills in dialogical encounter that can be modeled and practiced in workshop settings with trainees and reinforced through clinical supervision. Experience with interinstitutional and intersectoral community work: Although multidisciplinary cooperation is common in clinical settings, practical teaching about systemic issues is still largely inadequate. Trainees need experience consulting on institutional and community issues. Addressing systemic issues can be taught through in-service seminars that bring together participants from multiple sectors and institutions for in-depth case discussions.
140,141
Fostering ethical reflection: The predicament of refugees, ethnocultural minorities, and other vulnerable populations or marginalized groups raises complex ethical issues, involving individual versus group rights, as well as frequent situations where professionals must consider modifying standard procedures and adopting positions of advocacy without appropriating the voice or experience of the other.
142
Training requires a setting where ethical issues can be made explicit and discussed from multiple perspectives.
With appropriate supervision, any clinical setting with a high diversity in the patient population can be useful for training in cultural psychiatry. In addition, certain types of specialized programs including cultural consultation and ethnospecific services can provide opportunities for more advanced training. 143,144 This may involve specialized inpatient, outpatient and community consultations as well as time-limited treatment. 145,146 These rotations usually involve clinical activities that include direct patient contact, consultation with referring clinicians and outreach to community referral sources. Because it emphasizes providing consultation to other professionals and requires openness to questioning the assumptions of standard psychiatric practice, a cultural consultation rotation is most appropriate for senior trainees. Much learning takes place from focused reading around cases and working closely with culture brokers. Group supervision and the self-disclosure of experienced clinician mentors are crucial to developing clinical skills, confidence and an effective clinical approach.
Research Training
Research in Canada has documented clear disparities in access to mental health services and outcomes for different groups. There is evidence that specifically addressing cultural differences can improve access to care and clinical outcomes. However, there is a need for more research on all aspects of the interplay of culture and mental health, including models of psychopathology, health services and recovery. This, in turn, requires a new generation of researchers trained to apply contemporary social science perspectives and diverse methods to the study of culture and psychiatry. To address issues of cultural diversity in mental health services, researchers require familiarity with a broad range of methodologies. The most sophisticated studies are multilevel and multimethod, integrating both quantitative and qualitative approaches, and require teams of researchers who can work together closely to consider the various levels at which culture has an impact, from the individual through to the broader society. Research with Indigenous populations raises particular ethical issues. Of particular importance for cultural psychiatry are community-based participatory research methods that engage communities in all aspects of research including design, recruitment, implementation, data gathering, interpretation and dissemination. Teaching research skills in cultural psychiatry requires a balance between methodological rigor and learning to question one’s own discipline through other perspectives. 48
Assessment in Training and Continued Medical Education
A well thought-out assessment process is an essential component to cultural competence training in residency as it not only provides a summative evaluation of the trainee but can also provide formative feedback that facilitates learning and a motivational incentive to continuously reflect, learn and make behavioural changes. Assessment and evaluation are the cornerstones of curriculum development. For trainees and practitioners, evaluation is a strong motivator for learning and can help the clinician to identify areas where they need additional experience. In the area of cultural psychiatry and cultural competence, developing valid and reliable evaluation tools can be a challenge as the real goal is to effect meaningful changes in attitudes and clinical skills that continue to develop through experience and persist long after the course materials have been delivered; testing factual knowledge delivered in the course is much more straightforward using traditional means. The concept of blueprinting, borrowed by educational scholars from the field of architecture, can be useful to map out in advance test construction against learning objectives (such as combining CanMEDS roles and the ASK [attitudes/skills/knowledge] model of cultural competence) with the objective of creating valid evaluation tools. 44
Attitudes can be assessed through reflective journaling and essays, as well as through clinical supervision and direct observation. Content-based knowledge, especially from seminars, workshops and case conferences, can be assessed efficiently through written multiple-choice or short-answer examinations. Skills can be assessed through Objective Structured Clinical Examinations (OSCEs), mini-CEX, observed or recorded interviews, direct supervision of care and chart reviews. Some examples of formative assessment tools that have been developed include the addition of cultural stems and statements for Royal College style oral examination score sheets, including thorough mention of cultural identity, need for interpreters, inquiry into explanatory models and awareness of areas where cultural factors may be present in the mental status examination, in addition to mention of culture where appropriate in the diagnosis and treatment plan. In Table 4, we present a sample template for evaluating specific cultural competency components of observed interview and case presentation because successful performance in oral examinations remains one of the core requirements for successfully completing psychiatric training. These components can be adapted and integrated with existing scoring sheets and can be used for formative feedback in regular practice interviews as well as final evaluative examinations.
Evaluation Template for Observed Interviews and Case Presentationa
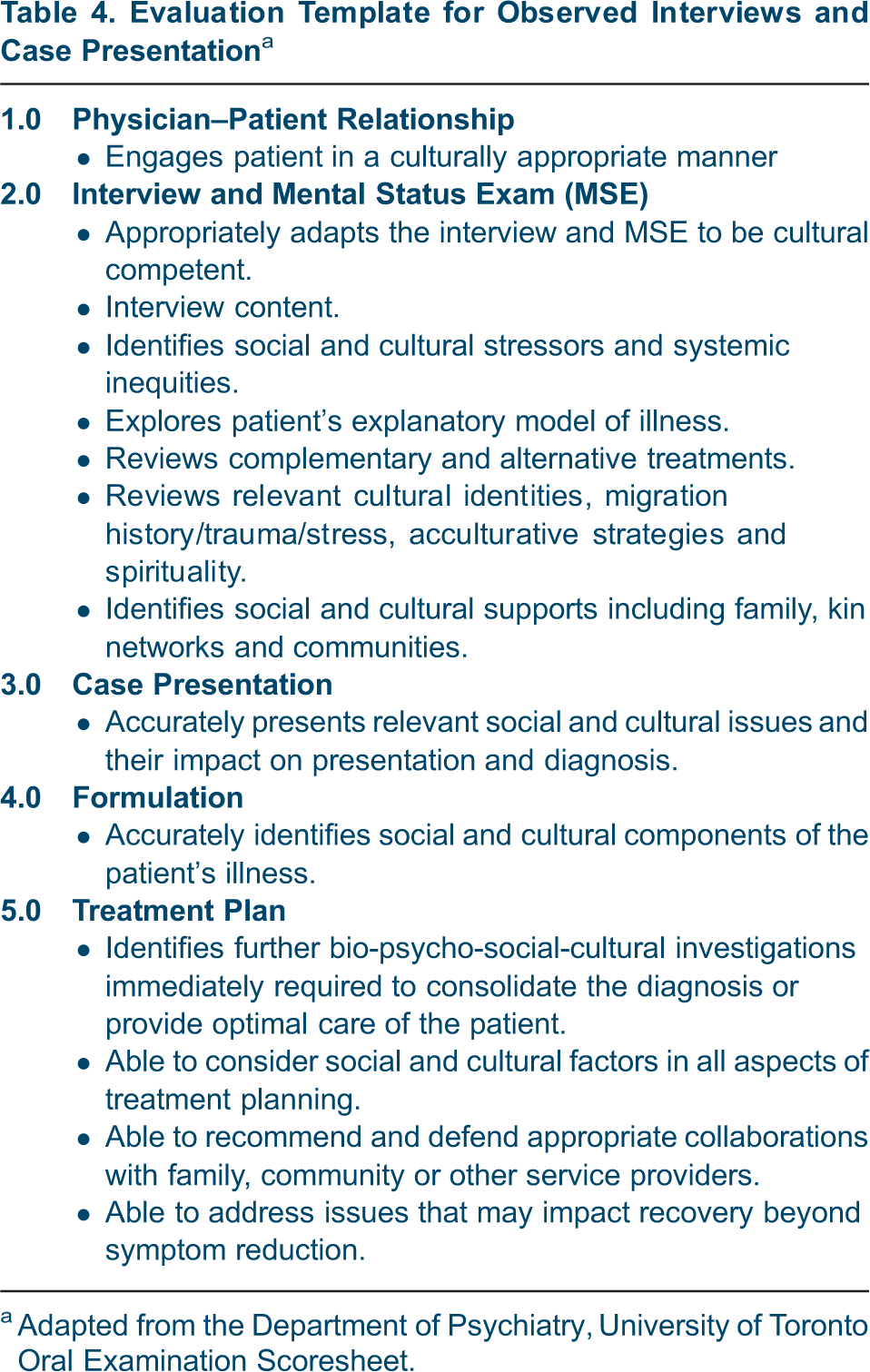
a Adapted from the Department of Psychiatry, University of Toronto Oral Examination Scoresheet.
Annual in-training evaluation reports are important opportunities to review the overall core cultural competencies under each of the CanMEDS roles, identify areas to improve on, and facilitate a learning plan. There is an emerging trend to employ multisource (“360-degree”) feedback as an evaluation methodology, and this is particularly relevant in assessing the core cultural competence of working with the diverse communities as a medical expert, collaborator, and leader. Depending on the rotations, the multisource feedback should include considerations of input from supervisors, interdisciplinary health professionals, relevant community partners, and if possible, patient and family feedback.
Faculty development is critical to the success of the cultural competence training. 147 With all the activity in postgraduate curricula in cultural competence training, offering CME programs to existing faculty becomes very important to enhance awareness of content and concepts within the expanded residency curriculum and to improve their supervisory skills by adapting cultural competence within their own specialty areas. The faculty themselves should be evaluated on their own cultural skills in clinical work and supervision. Cultural competence can be added as a heading on supervisor evaluation forms, where psychiatry residents can similarly rate their staff on inclusion and awareness of cultural issues during supervision, and this would include all mandatory clinical rotations, psychotherapy supervisors and electives. Cultural competence can also be assessed at the level of organizations. 148 This is an essential complement to efforts directed to practitioners.
Building Infrastructure to Implement Training
Implementing training in cultural psychiatry requires development of local infrastructure. However, most communities will have many of the key resources that can be brought together to support training. Three key ideas can guide this process: The leadership can and should be diverse. Senior faculty, junior faculty, residents and community members can be involved. The exact configuration will depend on local availability and the strategy for implementation, but the diversity does offer the possibility of different parts of the leadership being tasked with and owning different parts of the curriculum. Developing a common understanding in the leadership through a facilitated workshop focused on producing a local curriculum helps to fuse the leadership. The plan and implementation strategy flow from the CPA curriculum, local needs and the time and resources available, including the expertise that the leadership team has at its disposal. Resources needed for the plan are mainly the time of residents, faculty and community. The knowledge may be taught by a number of different methods including, text, lectures in person or via webinars and seminar series. Attitudes may be taught by various methods including self-reflection, group work and exposure over time to different communities. However, clinical skills are best improved by practice and coaching. This requires supervisors themselves to be conversant with approaches to cultural safety and cultural competence or for other sources of expertise to provide support to trainees on this issue. The amount of training of supervisors that is required will vary depending on their role. Exposure to the work of community groups and specific training or placements in settings that offer culturally specific care can be helpful with appropriate supervision. The introduction and refinement of a new curriculum requires ongoing evaluation. Part of implementation, therefore, is the development of a process to monitor the curriculum, obtain feedback and identify ways that training can be improved. Accreditation and other methods of local monitoring can insure that this information is used to improve training.
Conclusion
The accelerated exchange of knowledge and the confrontation of different value systems and perspectives that come with globalization are increasing the importance of cultural psychiatry as an academic discipline and a central pillar of clinical training and service delivery. Recognition that culture is central to identity and well-being and that certain groups suffer from marked inequities in mental health and access to services has spurred systematic attention to culture in psychiatry. At the same time, social sciences and cultural neuroscience can provide psychiatry with conceptual models for integrative understanding of mental health and illness.
The Section on Transcultural Psychiatry of the CPA has contributed to the Multicultural Mental Health Resource Centre (MMHRC; www.mmhrc.ca), an online knowledge exchange centre to support intercultural mental health care. In addition to material for patients and practitioners, the MMHRC has sections to share curriculum materials, interactional learning, and self-assessment tools, as well as models of clinical practice and organizational change. 149 Continued Professional Development activities in this area include the annual Summer Program and Advanced Study Institutes in Cultural Psychiatry organized by the Division of Social and Transcultural Psychiatry at McGill University and an annual Cultural Psychiatry Day, which is a nationwide accredited videoconference event, cosponsored by the Transcultural Section of the CPA. These initiatives support ongoing efforts to make cultural psychiatry a core component of the knowledge and skills of all psychiatrists. Of course, these professional competencies need to be coupled with institutional changes and monitored by accreditation bodies, to ensure that all Canadians benefit from a culturally safe and competent mental health care system that responds to the needs of our diverse society.