
Abstract

Lithium is recommended as a first-line treatment for bipolar disorder by contemporary clinical practice guidelines. 1 With a prevalence of bipolar disorder believed to be in the range of 1% to 2% in Canada, 2 expectation holds that lithium should be frequently used. However, its use is complicated by the need for safety monitoring and the possibility of adverse events.
The prevalence of lithium use in the Canadian population is unknown. Prescription data are, in principle, available from provincial databases in several provinces, but these do not provide national estimates. In the current study, we sought to estimate the frequency of lithium use in the household population using national survey data.
Several national surveys, based on representative samples of the Canadian household population, have collected data on psychotropic (and other) medication use. In this analysis, we used data from two national Mental Health Surveys: the 2002 Canadian Community Health Survey (CCHS) 1.2 and the 2012 CCHS-MH. We also used estimates from the Canadian Health Measures Survey, pooling two sets of estimates, 2009 to 2011 and 2013 to 2017. The surveys collected medication data by including questions about medication use, including asking respondents to collect and look at the bottles, tubes, or boxes containing their medications. Data are recorded using product identification numbers and recorded using Anatomic Therapeutic Codes (in the case of lithium, N05AN).
Methods employed in CCHS and Canadian Health Measures Survey (CHMS) are extensively documented on the Statistics Canada website. 3,4 Notably, the CCHS collected data on medication use in the 2 days preceding the interview, whereas the CHMS assesses past month use. We were interested not only in the most recent data but also in historical data in view of the possibility of secular trends. The final estimates derived from a recommended procedure using replicate bootstrap weights to account for survey design effects (such as clustering, unequal selection probabilities) and adjusting for nonresponse.
The estimates and their associated 95% confidence intervals are presented in the form of a forest plot in Figure 1. There is no obvious impression of increasing or decreasing prevalence over time. Consistent with this, heterogeneity was moderate (I 2 value = 55.1%, τ2 ≈ 0.0) and not statistically significant (heterogeneity χ2 = 6.7, df = 3, P = 0.083). We combined the estimates using random effects meta-analysis in Stata, Release 15. First, using the “metaprop” command, we employed a Freeman-Tukey double arcsine transformation for variance stabilization of the raw proportions. This procedure accounts for the dependence of the standard error of a proportion on its value, a potential source of bias with inverse variance weighting in meta-analysis. However, the transformation cannot be used with weighted proportions. In a second analysis, using “metan,” we pooled the untransformed weighted proportions. The results were nearly identical, so the pooled weighted proportions are reported here.
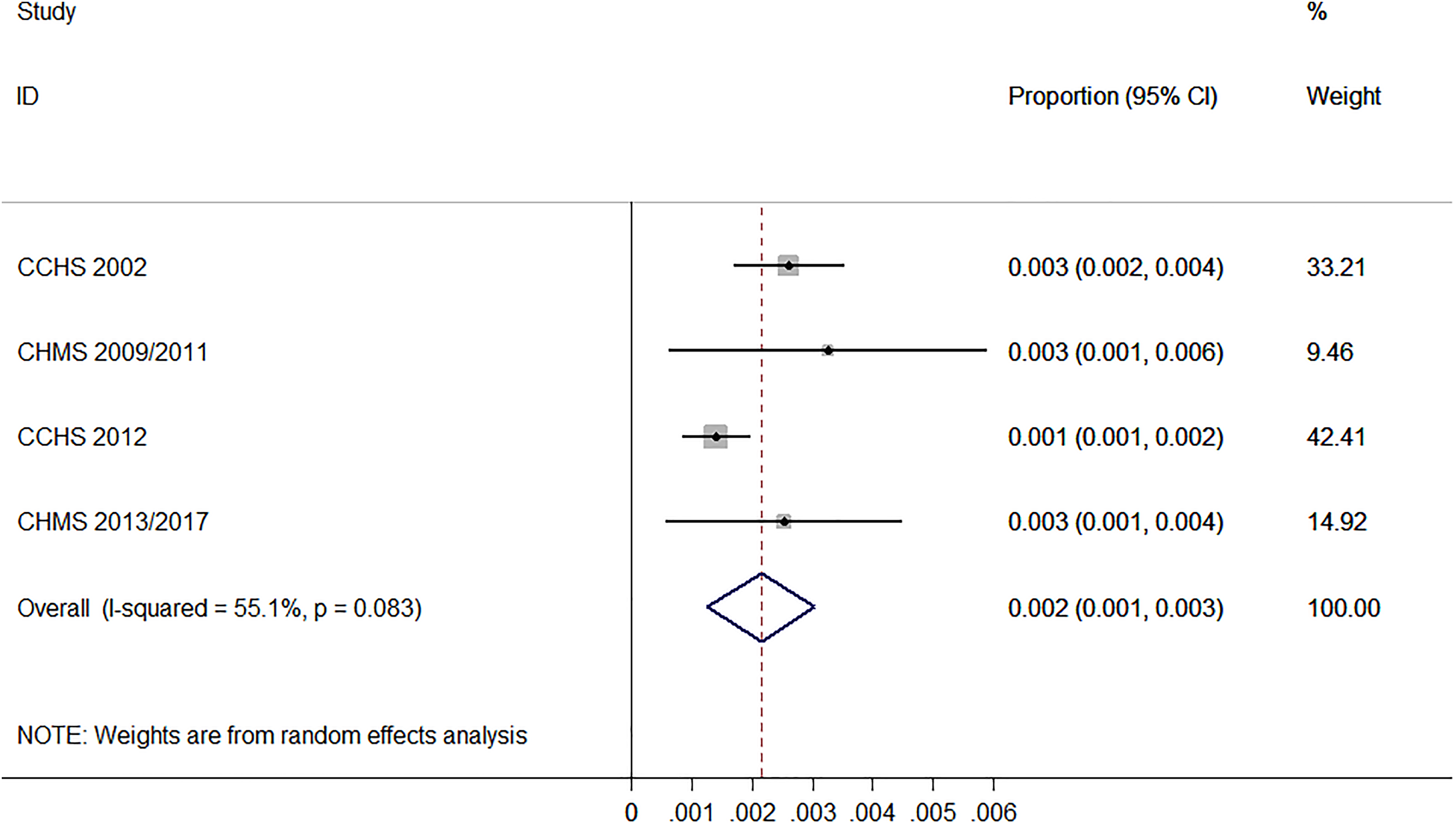
Reported lithium use in four population surveys.
The pooled prevalence of lithium in the Canadian household population was found to be 0.2% (95% CI, 0.1% to 0.3%), see Figure 1. The past month estimates from the CHMS appear to be slightly higher than the past 2 day estimates from the CCHS, and in each survey, the more recent frequencies appear slightly lower than the older estimates (i.e., CCHS 2002 > CCHS 2012 and the CHMS estimates from 2009/2011 > 2013/2017). However, with only four data points in the meta-analysis, the statistical significance of these trends could not be assessed.
Given the historically central role of lithium in the treatment of bipolar disorders, the frequency of lithium use is surprisingly low, although the estimates presented here resemble those previously reported for Denmark (0.17%), Norway (0.21%), and Sweden (0.25%). 5 A possible explanation is the availability of other first-line agents, or their more extensive marketing. Canadian Network for Mood and Anxiety Treatments lists seven other medications as first-line treatments. 1 It is conceivable that the observed frequencies represent an optimal frequency of lithium utilization based on its tolerability and effectiveness. However, there is also the possibility that the inconvenience associated with laboratory monitoring, exaggerated safety concerns, or a lack of familiarity with this medication among clinicians is resulting in underuse of the medication. Access to psychiatric care may be another factor, since nonpsychiatrist prescribers may be especially hesitant to use lithium. These latter possibilities should be explored in future research since, if confirmed, they may represent opportunities to improve the treatment of bipolar disorder.
Footnotes
Authors’ Note
Acknowledgements
The analysis was conducted at the Prairie Regional Data Centre, which is part of the Canadian Research Data Centre Network (CRDCN). The services and activities provided by the CRDCN are made possible by the financial or in-kind support of the SSHRC, the CIHR, the CFI, Statistics Canada, and participating universities whose support is gratefully acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Patten is supported by the Cuthbertson and Fischer Chair in Pediatric Mental Health at the University of Calgary.