
Abstract
Objective:
Clinicians may specify the diagnosis of conduct disorder (CD) as “with limited prosocial emotions” (LPE). This specifier is thought to identify youths with particularly severe and stable symptomatology. However, few studies have examined the clinical usefulness of the LPE specifier among children with childhood-onset CD. The current study examines whether the LPE specifier distinguishes children with particularly severe and persistent symptoms among those with childhood-onset CD. The study also aims to test whether the LPE specifier aids in identifying children with subclinical CD whose conduct problems are at risk of increasing.
Method:
Two hundred sixty-four children showing at least one CD symptom before age 10 were divided based on the presence of CD and the specifier. Children with and without the specifier were compared on number of CD symptoms (assessed at study inception) and trajectory of conduct problems (assessed over 4 years). The analyses controlled for oppositional defiant and attention deficit hyperactivity symptomatology.
Results:
Compared with children with CD but without LPE, children with CD and the LPE specifier did not differ on likelihood of endorsing most symptoms nor on total numbers of symptoms. Moreover, they did not show a more stable pattern of conduct problems across the 4 years. Children with subclinical CD with and without the LPE specifier were also similar in terms of their symptoms, severity, and evolution of their problems.
Conclusions:
Among youths with childhood-onset CD, the specifier appears to offer limited value in identifying those with particularly severe and stable CD symptomatology.
Introduction
Since the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 1 clinicians may add a “with limited prosocial emotions” (LPE) specifier when making a diagnosis of conduct disorder (CD). The LPE specifier is thought to delineate a distinctive subgroup among youths with CD who show a particularly severe and stable pattern of antisocial and aggressive behaviors. 1 –3 The indicators of LPE refer to specific traits from a broader construct often labeled as callous–unemotional traits. The DSM-5 indicators of LPE include lack of remorse or guilt, callous–lack of empathy, shallow or deficient affect, and absence of concern about poor performance at school or work. Two of these four symptoms shown persistently in more than one relationship or setting, as assessed from multiple informants, are needed to identify the presence of LPE.
Being able to detect the children most at risk of exhibiting persistent antisocial behaviors among those with CD is fundamental in order to prioritize the youths most in need of targeted interventions. To that end, several research reviews have now established that callous–unemotional traits can help to distinguish children and adolescents with a particularly severe and persistent pattern of antisocial behaviors. 3 –6 Some findings also support that children with high levels of callous–unemotional traits have a differential response to treatment in inpatient psychiatric settings. 7,8 The assessments of these traits vary substantially across studies, however, and often do not exclusively capture the four LPE indicators included in the DSM-5 (see Frick et al. 3 for a review). In addition, though the LPE specifier is conceptualized as a clinical category, callous–unemotional traits are most frequently assessed as a dimension. Further, while the clinical assessment of LPE requires a multi-informant assessment, 1 most studies used only one informant to evaluate these traits. 9 –13 These methodological variations limit robustness of the empirical support regarding the clinical usefulness of LPE as it is currently presented in the DSM-5.
Questions also remain on the usefulness of the LPE specifier over and above other CD subtypes. 14 –16 Of particular interest is the added incremental predictive benefit of the LPE specifier among youths with childhood-onset CD, which could have substantial subtyping overlap with LPE. 2,17,18 Youths with childhood-onset CD show at least one symptom of CD prior to age 10 and usually meet full criteria for CD before puberty. 1 Both children with childhood-onset CD and those who qualify for the LPE specifier are more likely to display an aggressive, severe, and stable pattern of antisocial behaviours. 1,6 Studies suggest that rates of LPE (or high levels of callous–unemotional traits) among children with childhood-onset CD vary from 25% to 32% in community-based samples 19,20 and may reach up to 60% in referred or clinical samples. 10
Research on the impact of the LPE specifier on the severity and course of antisocial behaviors among children with childhood-onset CD is scarce. In fact, most studies either did not precisely measure the DSM-5 LPE specifier or were not exclusively conducted with children presenting childhood-onset CD. Still, some studies showed that children with CD and LPE present more deceitfulness 20 and aggressive symptoms 19,20 than children with CD but without LPE. However, the few longitudinal studies on the impact of LPE or callous–unemotional traits on the course of antisocial behaviors produced mixed results. Some showed that callous–unemotional traits did not distinguish children presenting childhood-onset conduct problems on the stability of their future conduct problems, 21 nor did it predict later antisocial personality disorder 22 or violent and property-related recidivism. 23 Other studies reported a significant association between either LPE or callous–unemotional traits, and later antisocial outcomes among youths with CD 12,13,20 as well as among youths without CD. 24,25 This last result suggests that LPE could increase the risk of subsequently meeting full CD criteria among children presenting subclinical manifestations of the disorder. However, as a whole, results from previous studies need to be replicated in order to clarify the clinical usefulness of the LPE specifier in the childhood-onset subtype of CD.
Consequently, the current study examines whether the LPE specifier, as it is conceptualized in the DSM-5, distinguishes children with a particularly severe and persistent pattern of symptoms among those with childhood-onset CD. In addition, the study aims to test whether the LPE specifier aids in identifying children with subclinical CD whose level of conduct problems are at risk of increasing over time. Since studies have shown that symptoms of oppositional defiant disorder (ODD) and attention deficit hyperactivity disorder (ADHD) are closely related to LPE 19,20 and contribute to later CD, 25 symptoms of ODD and ADHD are controlled in the study.
Methods
Participants and Procedures
Participants are part of an ongoing longitudinal study on children receiving school-based psychosocial services for conduct problems. These children were recruited from 2008 to 2010 in eight school boards (155 elementary schools) located in four regions of the province of Québec (Canada). In Québec, children signaled at school for conduct problems are admitted to school-based psychosocial services after a formal professional’s (e.g., school psychologists or psychoeducator) assessment reveals the presence of significant difficulties which interferes with the child’s social or academic functioning. In order to obtain a roughly similar number of girls and boys in the sample, all girls less than 10 years of age receiving these school-based services, and approximately one out of four randomly selected boys were invited to participate in the study. The participation rate was 75.1% (N = 370). Participants did not differ from nonparticipants in proportions of girls, grade level, or deprivation index of school attended. The CD symptoms of all these children were assessed with the Diagnostic Interview Schedule for Children (DISC, see the Measures section), administered to the parent and teacher. To be included in the current study, children had to present at least one symptom of CD based on parent or teacher report. This procedure led to a final sample size of 264 children (40.5% girls; mean age = 8.5, SD = .91), including 103 who met full CD criteria (three or more CD symptoms), and 161 children who presented one or two symptoms of CD.
The conduct problems of these children were reassessed at four subsequent annual time points. At these subsequent assessments, data on conduct problems were available for 93.6%, 92.4%, 90.5%, and 89.4% of participants. Participants who did not complete the follow-ups did not differ from those who completed all follow-ups in terms of age at the first assessment, t(262) = 0.04, P = 0.97, sex, χ2(1) = 0.02, P = 0.89, and levels of conduct problems, t(262) = 1.06, P = 0.29.The treatment of missing data is addressed in the Data Analysis section.
The Institutional Review Board for Research in Education and Social Sciences of the Université de Sherbrooke (Québec, Canada) approved all procedures in the study. All parents provided a written consent to participate at every assessment and met with interviewers in their home. Following the parent’s consent, teacher information was obtained by telephone with a structured interview protocol. Participants received financial compensation at every measurement time point.
Measures
LPE specifier
The four indicators of LPE included in the DSM-5 were assessed at study inception with the four corresponding items from the French–Canadian translation of the Antisocial Process Screening Device 26,27 : (1) is concerned about how well he or she does at school (reversed score), (2) feels badly or guilty when he or she does something wrong (reversed score), (3) is concerned about the feeling of others (reversed score), and (4) does not show feelings or emotions. Items were rated on a 3-point scale ranging from 0 (not at all true) to 2 (definitely true). Consistent with the DSM-5 criteria, LPE was considered if at least 2 of the 4 items were rated 2 by either the parent or the teacher.
CD
CD symptoms were assessed using the French–Canadian translation of the DISC-Revised 2.25, 28,29 which was slightly modified in order to cover all 15 CD symptoms listed in the DSM-IV. 30 These symptoms still correspond to those listed in the DSM-5. A symptom was considered present if reported by either the parent or teacher. The number of symptoms comprised in the DSM-5 category “aggression to people and animals” (maximum of seven symptoms) and the total number of CD symptoms were also used as variables in the study to estimate the severity of CD.
Conduct problems
In addition to the diagnostic interview, the DSM-oriented scale for conduct problems from the Achenbach System of Empirically Based Assessment 31 was administered at study inception (T0). This scale was also used at follow-up assessments (T1–T4), to measure child conduct problems over time. The scale contains items that have been judged by psychiatrists and psychologists as being consistent with symptoms of CD. 31 The parent (17 items; α = .82 to .85 for the five measurement time points) and teacher (13 items; α = .85 to .88) versions of the scale were used in the study. The scale is scored on a 3-point Likert-type scale ranging from 0 (not true) to 2 (very true or often true). Total raw scores were converted into T scores following the age, sex, and informant appropriate norms of the scale. 31 Since conduct problems are known to be context-specific, 32 we retained the highest T score between parent and teacher at each time point in order to tap the full breadth of the child’s conduct problems.
Control variables
ODD symptoms
To measure ODD symptoms, the French translation of the DISC 2.25 28,29 adjusted for DSM-IV criteria 30 was also used at study inception with parents and teachers. No changes occurred in the eight symptoms of ODD included in the DSM-5. Each symptom is considered present if reported by either informant.
ADHD symptoms
ADHD symptoms were assessed using the Conners’ ADHD/DSM-IV Scales, 33 which directly correspond to the DSM-IV symptoms for ADHD diagnosis. Items were scored on a 4-point scale ranging from 0 (not true) to 3 (very true). A symptom is considered present if it received a score of 3 by either the parent or the teacher.
Data Analysis
Children were first divided into four groups following the presence of clinical (three symptoms or more) or subclinical CD (one or two symptoms), and of the presence of the LPE specifier (identified with a “+” if present and with a “−” if absent): CD−, n = 55; CD+, n = 48; subCD−, n = 94; subCD+, n = 67. There was no difference regarding the age, F(2.41, 213.89) = 0.978; P = .441, nor the proportion of girls between the four groups, χ2(3, n = 264) = .40, P = .94. There were also no differences in attrition rates across the four groups, χ2(3) = 5.95, P = 0.11. As expected, however, models of Poisson (ODD) and negative binomial (ADHD) regressions revealed that children in the CD+ group showed significantly more ADHD symptoms than children in the CD− group, β = 0.29, P = 0.01, and children with subCD+ presented significantly more ODD symptoms, β = 0.20, P = 0.02, and ADHD symptoms, β = 0.25, P = 0.01, than children in subCD− group. This supports our decision to control these variables in the analysis.
Logistic regression models were used to compare groups on dichotomous CD symptoms. Poisson regression models, which account for discrete variables, were used to compare groups on aggressive and total CD symptoms counts. An unconditional linear growth model was conducted to assess the stability of the children’s conduct problems over the five annual assessments. Two conditional linear growth models were then used to compare groups (CD− vs. CD+; subCD− vs. subCD+) on growth parameters (intercept and slope). Model 1 compared groups without including the control variables, while Model 2 compared groups controlling for ODD and ADHD symptoms counts. Full information maximum likelihood was used in these models in order to retain children with missing assessments in the analysis.
Results
Group Comparisons on CD Symptoms
Table 1 shows the descriptive statistics of CD symptoms among groups. Comparisons for symptoms with no occurrence in the sample (i.e., forced sex, run away) or in one of the two groups compared (i.e., CD− vs. CD+: sets fire, broken into house/car; SubCD− vs. SubCD+: sets fire, broken into house/car, stays out at night) could not be computed. Group comparisons revealed only one significant difference in the presence of specific CD symptoms. Among children with CD, those with LPE (CD+) showed a greater risk of having used a weapon to cause harm than children without LPE (CD−), P = 0.02, controlling for ODD and ADHD symptoms. The two CD groups showed, however, similar scores on aggressive and total CD symptoms. There was no difference regarding CD symptoms and total CD symptom count between the subCD+ and subCD− groups.
Group Descriptive Statistics and Comparisons.
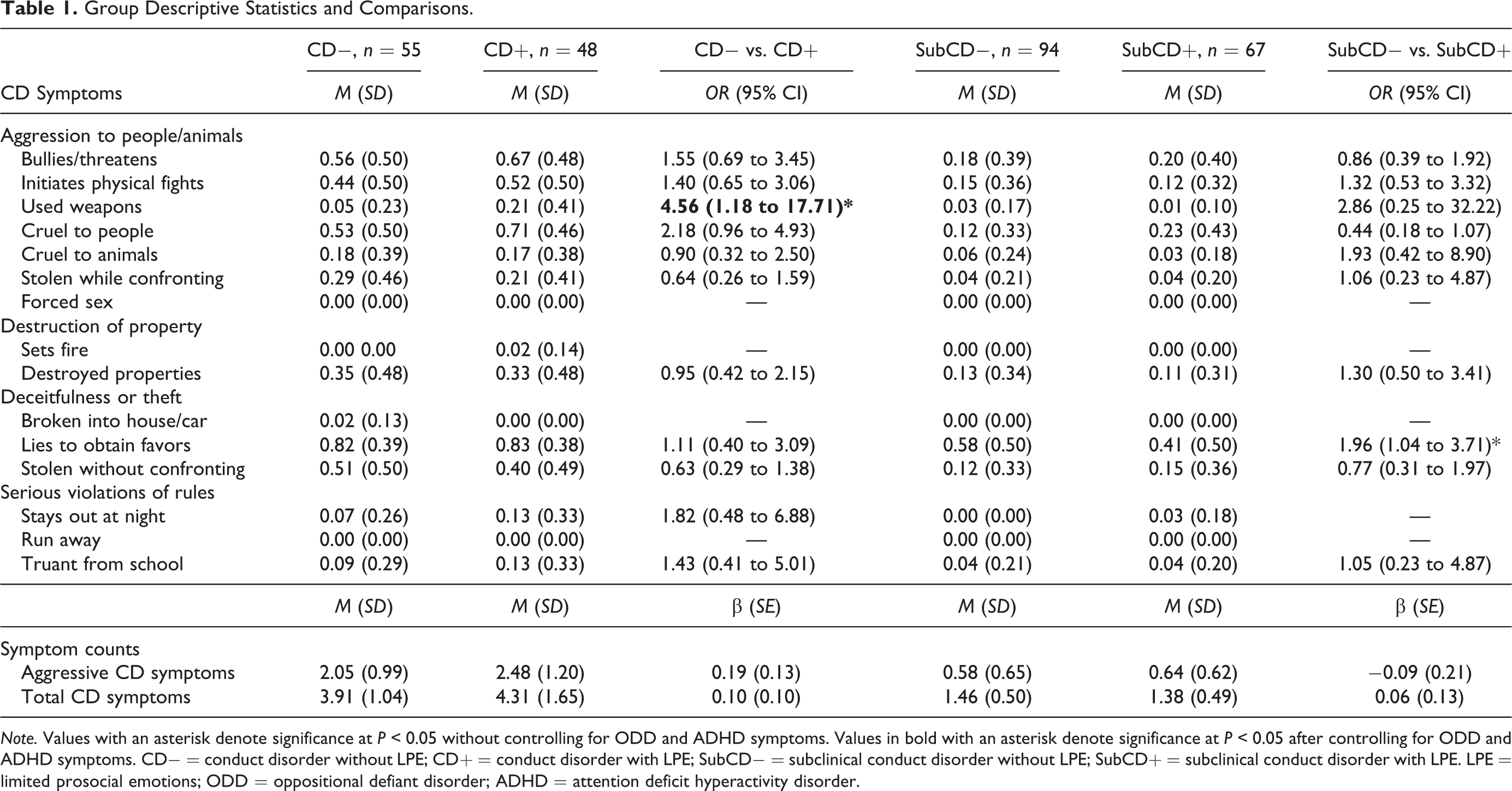
Note. Values with an asterisk denote significance at P < 0.05 without controlling for ODD and ADHD symptoms. Values in bold with an asterisk denote significance at P < 0.05 after controlling for ODD and ADHD symptoms. CD− = conduct disorder without LPE; CD+ = conduct disorder with LPE; SubCD− = subclinical conduct disorder without LPE; SubCD+ = subclinical conduct disorder with LPE. LPE = limited prosocial emotions; ODD = oppositional defiant disorder; ADHD = attention deficit hyperactivity disorder.
Group Membership and Conduct Problem Over Time
The unconditional growth model of conduct problems across the 4 years showed an excellent fit to the data according to Hu and Bentler’s accepted cutoffs 34 (Comparative fit index, CFI = 0.97, Root mean square error of approximation, RMSEA = 0.057). This model showed an average linear decline of conduct problem scores over time (mean intercept = 74.13, mean slope = −1.88, P < 0.001). Significant residual variance for the intercept and the slope (P < .001) was observed and suggested further investigation into the heterogeneity in conduct problem evolution.
Table 2 shows the intercept and slope of the conditional growth models (Model 1: group membership as a predictor; Model 2: group membership and ODD and ADHD symptoms as predictors). The two conditional models also showed acceptable fit to the data (Model 1: CFI = 0.97, RMSEA = 0.052; Model 2: CFI = 0.93, RMSEA = 0.069). Model 1 suggested that children from the CD+ group had a significantly higher intercept but a similar slope in their conduct problems trajectory when compared to children from the CD− group. Also in this model, children from the subCD+ group did not differ from children from the subCD− group in the intercept and slope of their trajectory of conduct problems. When including covariates of ODD and ADHD symptom counts (Model 2), ODD symptoms significantly predicted both the intercept and the slope of the conduct problems trajectory, while ADHD symptoms did not significantly predict the two growth parameters. In this model, the statistical difference of the intercept between children from the CD+ and children from the CD− groups fell under the level of statistical significance. These results suggest that LPE does not identify children with a more stable pattern of conduct problems over and above ODD and ADHD symptoms among those with clinical or subclinical CD.
Conditional Growth Models of Conduct Problems Over 4 Years.
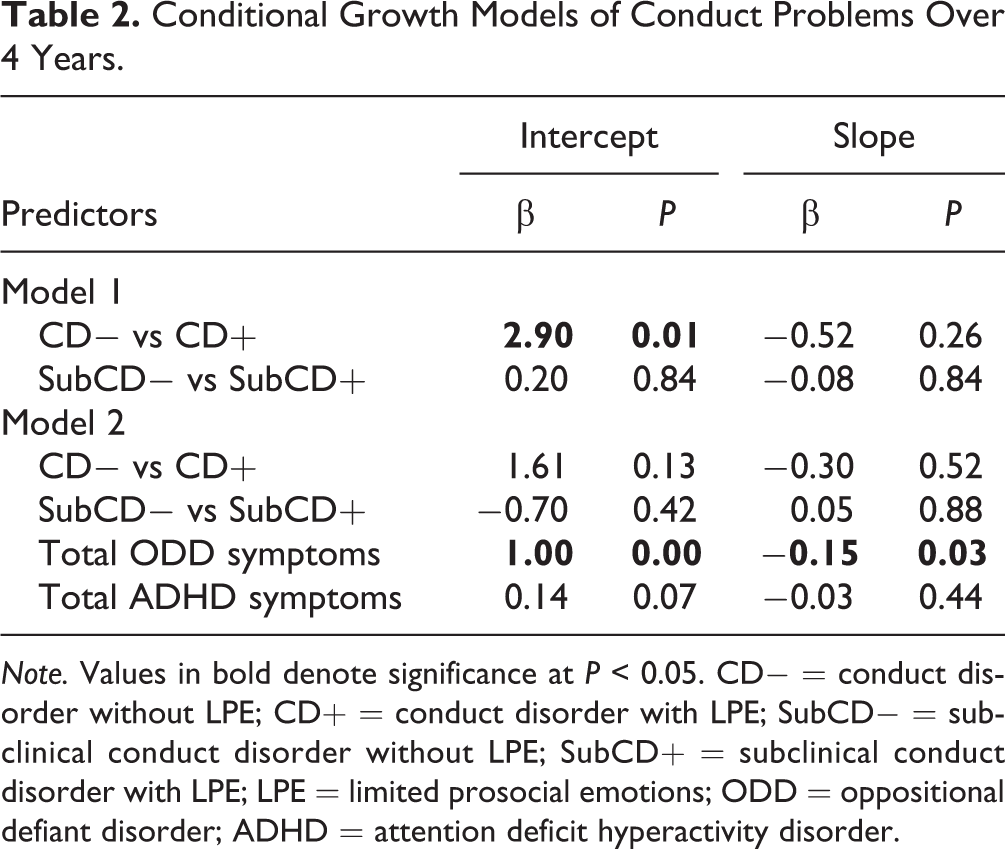
Note. Values in bold denote significance at P < 0.05. CD− = conduct disorder without LPE; CD+ = conduct disorder with LPE; SubCD− = subclinical conduct disorder without LPE; SubCD+ = subclinical conduct disorder with LPE; LPE = limited prosocial emotions; ODD = oppositional defiant disorder; ADHD = attention deficit hyperactivity disorder.
Discussion
Consistent with past research, 10,19,20 this study showed that children with the LPE specifier are numerous in our sample. Specifically, approximately 42% of children with subclinical CD, and almost one of two children with CD merited this specifier. Also consistent with past research, 19,20 the LPE specifier was associated with higher initial levels of conduct problems among children with CD and LPE, when compared to those with CD but without LPE. However, this difference disappeared when comorbid symptoms of ODD were taken into account. Further, results of our study did not lend support to the utility of the LPE specifier in the prediction of the longitudinal course of childhood-onset conduct problems.
First, with respect to symptoms, no differences were found on the number of aggressive symptoms, nor on the total number of symptoms, nor on most symptoms of CD between children with and without the LPE specifier. Although children with CD and the LPE specifier were more likely to present the symptom “has used a weapon that can cause serious physical harm to others,” 1 differences were not systematically observed between children with and without the LPE specifier. Given the number of statistical analyses, this result must be interpreted with caution given the possibility of Type 1 error. We have chosen to not correct for Type 1 error, as this may have exposed us to increased Type 2 error. These results are in line with those of Jambroes and colleagues 15 who have suggested that the LPE specifier may not be sensitive to differences in severe antisocial behaviors within clinical samples.
Second, with respect to the severity of the conduct problems, the growth curve analysis suggested that among children with CD, the initial level of conduct problems was higher in the presence of the LPE specifier. This may suggest that when we use a more sensitive scale, such as the DSM-oriented scale for conduct problems, which contains three response options instead of a presence/absence dichotomy, the differences are more evident and suggest that problems may be more severe in the presence of LPE. However, since this difference was no longer significant when controlling for comorbid symptoms of ODD and ADHD, the observed difference in the initial levels of conduct problems could in fact reflect more comorbidity among children with CD and LPE.
Third, concerning the trajectory of conduct problems, the higher initial level related to the presence of the LPE specifier did not appear to translate into changes in the trajectory of conduct problems over time. Indeed, no difference was observed in the slope of the conduct problems trajectory between children with CD and LPE and those with CD but without LPE. This result suggests that LPE does not distinguish children with a particularly stable pattern of conduct problems.
Finally, the idea that the presence of the LPE specifier may lead to increased conduct problems over time among children presenting with subclinical CD before age 10 also did not find support in our results. Children with subclinical CD with and without LPE appear very similar in our study. This is evident when looking at the nature and number of CD symptoms manifested by these children and at their initial levels and course of conduct problems.
Altogether, these results suggest that the clinical utility of the LPE specifier among children with either the full or subclinical presentation of childhood-onset CD is limited. These results are consistent with studies that have reported no effect of LPE or callous–unemotional traits on later antisocial outcomes, 10,21,23 but diverge from studies which have reported that children with CD and LPE showed a more severe and aggressive pattern of antisocial behaviors than children with CD but without LPE. 13,19 However, our study is among the few to examine LPE as defined in the DSM-5 within a sample with childhood-onset CD, while controlling for comorbid ODD and ADHD. Nevertheless, similar to others (such Colins et al. 35 ), our results support the idea that the LPE specifier may distinguish those children with CD who are most likely to present with comorbidities. As such, the specifier could indicate to clinicians a profile, which may extend beyond only CD symptoms, to ODD, ADHD, and other psychopathologies. LPE could therefore be useful in identifying children with CD among whom a wider mental health assessment could help identify specific treatment needs.
Since our sample is composed of children who have been referred in elementary schools for school-based services for conduct problems, our results do not necessarily reflect children who do not receive services. However, teachers are sensitive to conduct problems, and the majority of children with this level of conduct problem severity are referred to school services. In addition, our study did not control for the reception of school services over time. Nevertheless, studies on general services delivered in schools have concluded that they have little impact on the reduction of CP. 36,37 In addition, since all children in the sample received such services at study inception, their influence on the associations observed should be limited.
Conclusion
Our results suggest that the LPE specifier has limited clinical utility in terms of identifying a particularly severe group of children among those presenting with CD. The specifier also appears to have limited utility in identifying those at highest risk of developing CD among those with subclinical CD. Nevertheless, results suggest that the specifier may identify children with CD or subclinical CD who are more vulnerable to comorbidities. In this way, it would be important that further research distinguish the presence of the LPE specifier from the comorbidity with ODD or ADHD among children with CD or subclinical CD. Specifically, whether LPE is a marker for a more complex clinical picture (i.e., comorbidities) or whether it is an indicator of severity of childhood-onset CD should be clarified. Clarifying the role of LPE would be important considering the fact that this label may bring additional stigma to children with CD 38 and should therefore only be used if clinically necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Canadian Institutes of Health Research (82694) and the Social Sciences and Humanities Research Council (37890).