
Abstract
Objectives:
Mental health case managers comprise a large workforce who help patients who struggle with complex mental illnesses and unmet needs with respect to the social determinants of health. This mixed-methods capacity-building pilot examined the feasibility, experiences, and outcomes of training community-based mental health case managers to integrate evidence-based psychotherapy principles into their case conceptualization and management practices.
Methods:
Case-based, once-weekly, group consultations and training in applied therapeutic principles from mentalizing, interpersonal psychotherapy, motivational interviewing, and other evidence-based psychotherapies were provided to case managers over 8 months. A trauma-informed and culturally sensitive approach was emphasized to improve therapeutic alliances and to foster adaptive expertise and an appreciation of individual patient differences.
Results:
Qualitative analyses of focus groups and individualized interviews identified a shift toward being more reflective rather than reactive, with improved empathy, patient engagement, morale, and confidence resulting from the training (N = 16). Self-reported pre–post counseling self-efficacy changes revealed significant improvements overall, driven by improved microskills and an ability to deal with challenging client behaviors (N = 10; P < 0.05).
Conclusions:
This pilot demonstrated that case-based consultations and training of mental health case managers within a community-of-practice in trauma-informed, culturally sensitive application of evidence-supported psychotherapy principles were feasible and acceptable with scalable potential to improve case managers’ counseling self-efficacy, reflective capacity, empathy, and morale. Further research in this area is needed with a larger sample, and patient and health systems outcomes.
Background
Mental health (MH) case managers working with diverse patients with chronic, complex struggles with mental illness and unmet needs with respect to the social determinants of health, with limited social supports oft feel inadequately prepared to provide MH support. 1 Case management focuses on pragmatic problem-solving and navigation of health and social services within a time-limited frame. To do this, case managers must form trusting therapeutic alliances and gain agreement on goals with their clients who are struggling with distress and symptoms that interfere with problem-solving and resource connections. Augmenting case management with therapeutic strategies from evidence-supported psychotherapies (ESPTs) can potentially enhance case managers’ abilities to better manage these challenges. ESPTs such as cognitive behavior therapy (CBT) 2 and interpersonal psychotherapy (IPT), 3 effective, consensus guideline-recommended MH treatments, 4 –9 can be delivered by nonspecialists including trained lay health workers. 10 This project sought to deploy and integrate ESPT practices with an emphasis on therapeutic alliances 11 –13 into patient-centered case conceptualization and case management. The goals of this mixed-methods capacity-building pilot (October 2016 to May 2017) were to (1) examine the feasibility and experiences of capacity-building with community-based MH case managers within a community-of-practice (CoP), integrate a compendium of trauma-informed, 14 culturally sensitive 15 ESPT principles into case conceptualization and practice; (2) foster adaptive expertise 16 with an appreciation of individual client differences; and (3) increase case managers’ ESPT and facilitative interpersonal skills and confidence in response to case-based learning needs focused on improving the quality of the support provided to clients with MH problems.
Methods
Design and Theoretical Framework
This pilot with a cohort of frontline MH human service professionals and case managers who were working with clients with complex and chronic forms of mental illness builds upon earlier conducted capacity-building projects to disseminate ESPT practices. 17 –19 This project differs, however, in its emphasis on adaptative expertise 16 using trauma-informed, 14 culturally sensitive 15 case conceptualization and therapeutic engagement with responsiveness to individual client differences drawing from a compendium of ESPT models and common factor principles. 11 In an ESPT learning needs survey of participating case managers, dialectical behavior therapy (DBT) and IPT were the highest ranked, followed by CBT and motivational interviewing (MI). Rather than training in a single therapeutic model, the curriculum focused on integrating a range of ESPT principles in response to case-based transdiagnostic challenges. The mixed-methods evaluation included qualitative analysis of data from focus groups and individual interviews, and quantitative analysis of pre–post changes in self-reported counseling self-efficacy. Focus groups were conducted at the midpoint of the intervention and again at the conclusion of the intervention, with individual interviews as a means of exploring in greater depth the themes that had emerged from the focus groups. Combining quantitative and qualitative approaches in research can be challenging, given ontological and epistemological differences between the two methodological stances. 20 We describe the quantitative and qualitative findings in distinct sections of our analysis; however, the different approaches to data converge to inform one another.
Four theoretical frameworks guided the design and implementation of this educational capacity-building pilot: critical realism, “Promoting Action on Research in Health Services” (PARiHS), CoPs, and adaptive expertise.
Critical realism views effects in the world as arising from interactions between social structures, mechanisms, and human agency and highlights how quantitative methods can explore comparisons and/or causal mechanisms, and how qualitative methods can illuminate novel, complex relationships and experiences not captured by the predetermined quantitative categories.
21
This is particularly relevant for program evaluation.
The PARiHS framework conceptualizes successful implementation of research into practice as relying on evidence, context, and facilitation. Monitoring, feedback, and evaluation are sought in dissemination processes from multiple sources, including practitioner and patient/client preferences, clinical experiences, and local information. A team effort is required to develop a shared understanding of implementation benefits, challenges, and risks within a supportive learning organization and workplace.
22
CoPs are defined as groups who engage in collective learning from one another within a shared domain of human endeavor or practice—in this case, MH case management.
23
The final conceptual framework employed was the professional education concept of adaptive expertise,
16
defined as an ability to adapt and apply knowledge and expertise to uncertain, complex, or novel situations. In this pilot, the application of ESPT principles to practice was focused on cases that were complex and challenging with an appreciation of individual client differences.
Participants and Setting/Context
Case managers and program managers from two community-based MH agencies that provide services to individuals from catchment areas of a large urban center (Toronto) were recruited for participation in this ethics approved study. Inclusion criteria included any full- or part-time case manager and/or program manager within the organizations.
Typically, in these agencies, case managers use a strengths-based, problem-solving approach 24 to support 15 to 20 clients at a time, who have been referred to work toward recovery by identifying goals that are meaningful to them. Client contact is primarily in person in the client’s community, with occasional phone contact. Clients live in a wide variety of settings, some alone and others with family members. Historically, this service was open ended, and case managers served clients for many months and often years. More recently, a move to reduce waitlists and wait-times has resulted in efforts to be more goal focused and time limited with a service model of rapid case management (8 to 12 weeks).
Intervention
Weekly case-based in-person longitudinal small group consultations with training in ESPTs and relationship-based facilitative therapeutic principles were provided within a supportive workplace 22,25 and CoP 23 of MH case managers over 8 months. 26 A rotating schedule of participants’ presenting challenging cases provided a springboard from which relevant therapeutic principles were taught with peer support. Rather than using a singular model or preplanned specifically ordered topics, we flexibly responded to the clinical challenges presented, modeling processes of adaptive expertise 16 and chose didactic material from differing therapeutic models of relevance and salience. Therapeutic impasses or lack of client progress were framed in a nonblaming, nonshaming manner as opportunities for learning in which we brainstormed and generated alternate ways of conceptualizing and working with clients—to foster reflective practices 27 –29 and adaptive expertise. 16 We drew from five modalities—IPT, 3,30 MI, 31,32 mentalizing, 33 DBT, 34 and CBT, 35 along with attachment theory 36 and interpersonal facilitative skills such as using empathy with attention to repairing impasses in therapeutic alliances. 11,12 The multimodal interactive curriculum included viewing of captioned videotaped demonstrations and doing role-plays to practice and model use of ESPT principles and techniques. Training emphasized facilitative interpersonal skills for managing complex dynamics of therapeutic alliances with a culturally sensitive, relational- and affect-focused, trauma-informed understanding using attachment theory and mentalizing. 11,14,15,25,27
Measures
Counseling self-efficacy was measured via Larson and colleagues’ self-report Counseling Self-Efficacy (COSE) Scale, widely used in counselor trainee educational research. It has high total score reliability (Cronbach α = 0.93), test–retest reliability (0.87), and contains five subscales of Counseling Confidence in using Microskills, Attending to Process, Dealing with Challenging Client Behaviors, Cultural Competence, and Awareness of Ones Values. 37 The higher the score, the stronger the perception of counseling self-efficacy. COSE scores have been associated with counseling competence. 38,39
Focus group and interview guides utilized concepts from the PARiHS 22 and CoP 23 frameworks. Participants were asked to reflect on the experience of participating in the ESPT-focused training within the CoP model and the impact on their practice. Additional probes and questions were developed from initial focus group findings and utilized in subsequent interviews, such that emerging themes from one qualitative domain could be triangulated against other domains, through co-occurring data collection and analysis. Interviews and focus groups, all carried out by one researcher (SB), were audio recorded and transcribed verbatim.
Data Analysis
Quantitative
Changes in pre–post counseling self-efficacy were measured by changes in COSE over time tested using paired t tests. All effects were tested at the P < 0.05 levels. All quantitative statistical analyses were conducted using SPSS Version 23 (IBM Corp).
Qualitative
An interpretivist thematic analysis of interview and focus group transcripts was carried out in two stages. An initial open coding of all individual interview transcripts was independently completed by two researchers (SB and TK). SB performed open coding of focus groups. Codes were then compared and organized into larger themes and subthemes, with reviewing of codes (PR) for cogency and applicability, using a subset of transcripts. A thematic “map” was developed, and subsequently all transcripts were coded in an axial fashion by SB and TK using an iterative process of reading, coding, and rereading transcripts (re-coding as necessary). Relationships between themes and subthemes were established. Field notes completed by the facilitator (PR) and researcher carrying out interviews and focus groups (SB) were coded by TK as a way to further triangulate the data. A final coding meeting was held to determine the robustness and reliability of themes, and data related to each theme were extracted at that time. Member-checking with a subset of program managers and case mangers took place following this, increasing confidence in the interpretation of the qualitative data.
Results
Demographics and Quantitative Results
Sixteen case managers participated in interviews following completion of the case-based ESPT training. A sizable proportion of individuals who took part in the training also participated in the case manager focus groups (n = 14), held at the midway point of the training and at its conclusion. Additionally, program managers (n = 3) from the two participating agencies who had prior experience as case managers in the community participated in separate focus groups.
The majority of the participants had over 10 years of experience working in the field of MH and addictions (n = 9, 56.3%), while six (37.5%) had 5 to 10 years of experience, and one (6.3%) had 1 to 5 years. Half the sample (n = 8, 50%) held an undergraduate degree in a human service field of study (e.g., nursing, psychology, social work), six (37.5%) held a diploma, while two (12.5%) had a master’s degree.
Of the 10 (62.5%) participants who completed the COSE, 37 there were significant overall improvements over time in total COSE scores (P = 0.013), specifically driven by improvements in the subscales of “microskills” (P = 0.002), and dealing with challenging client behaviors (P = 0.017; Figure 1).
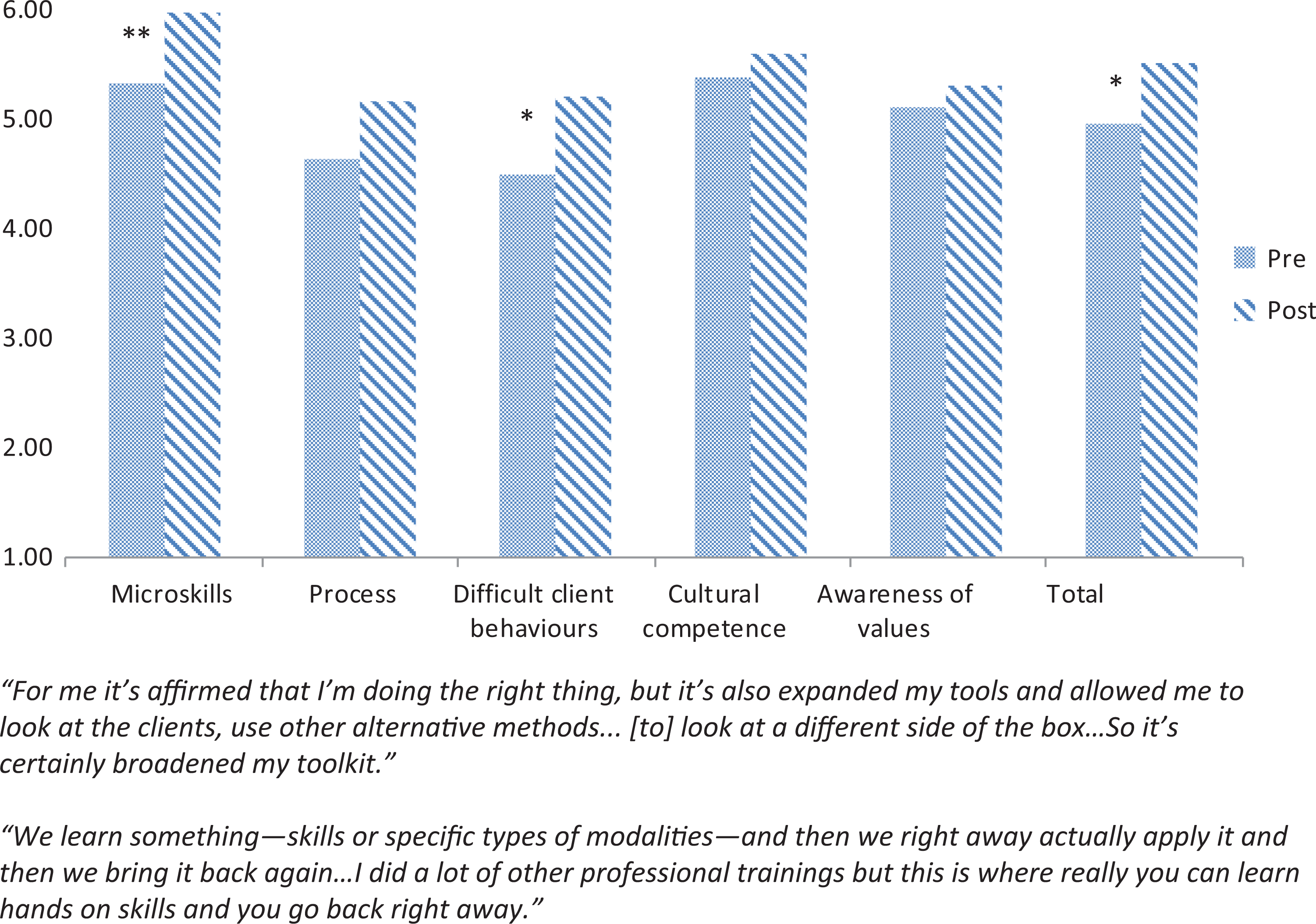
Counseling Self-Efficacy Inventory Questionnaire (COSE). Pre- and post-intervention total and subscale scores.
Qualitative Results
Focus groups and interviews identified a shift toward increased reflection, empathy, improved client engagement, morale, and confidence along with decreased reactivity to clients (See Table 1).
Themes from Case Managers Interviews and Focus Groups.
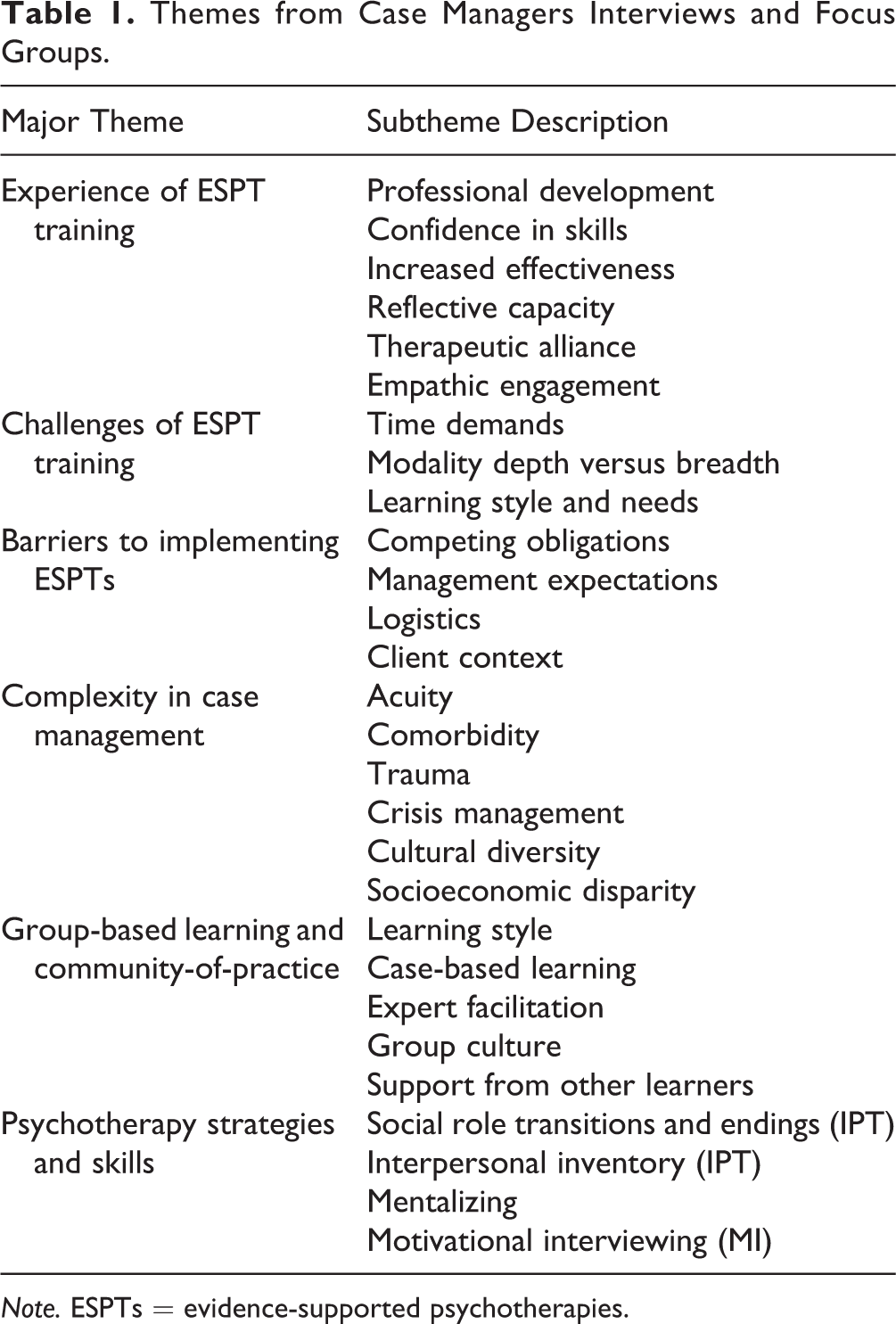
Note. ESPTs = evidence-supported psychotherapies.
ESPTs: Aiding Reflection, Building Confidence, Increasing Effectiveness
Both case managers and managers endorsed with wide agreement the benefits of this ESPT training, contrasting their work experiences “before” and after the intervention. Case managers felt, and were felt by management to be overall more effective in their work with clients. This was attributed in both groups to a shift in their overall approach to being more reflective and less reactive, with an improved ability for adaptive expertise to harness particular techniques and skills depending on the given client, situation, or issue they faced. I’m just more mindful…I am able to recognize my clients’ feelings a bit better now—I would do the same job before but I think now I am just more effective because I am able to recognize certain situations. (Case Manager R2) I think I’ve learned a lot from it [the training]…I think now I’m looking at other stuff—it has changed my way of looking at things beyond goals or beyond problem-solving solutions, but rather looking at what else is going on. As well, it also helps to client to think…(Case Manager R8) I think what struck me the most about everything was that it was really validating the tools that I was already using before I even started, and then giving me extra ways to do thing…it wasn’t really new to me, it may have a new name and I hadn’t used that name before, but I certainly knew the tool and I feel much more confident now than I did before…(Case Manager R5) Sometimes, no matter how experienced we are, there is always another way of doing things right, and to do it even more effective than they used to, even if they are already quite effective. (Manager RC)
Managing case loads and turnover
The shift to a rapid response paradigm in the workplace was new and distressing for case managers. Prior to beginning the ESPT training, they described struggling to envision how they would assist clients in a meaningful fashion within the newly implemented shortened time limits. Following the ESPT training, many expressed surprise that they were able to effectively engage in a “piece” of work with their clients, many of whom felt satisfied with what had taken place in the 8 to 12 weeks. Given work-related pressures of high referral volumes and frequent client turnover, the case managers’ experiences of acquiring confidence, validation, and professional growth were particularly significant in this rapid response service model. Before, I thought it [rapid response] wouldn’t work. Because of my experience—here I have a client for 3 or 4 years and not much progress, and within 8 or 10 weeks, what I am going to be able to do? But actually, working within that framework I was quite surprised that there are some clients—not all—there are quite a few clients who built a really strong therapeutic relationship even though we worked for two months. And some of the feedback I got from the client, they were very positive. (Case Manager, R7) All the cases were memorable for me but it was just helpful because you get different people’s input and knowledge and get more of an insight about what different [case managers] would do. So it gives you a lot of guidance as to where to go if you are kind of suck in a situation with someone (Case Manager R9)
Challenges and barriers
When asked about challenges or barriers to integrating ESPT skills in practice, participants described balancing pressures of time limits, workplace demands including reporting requirements, and simultaneously addressing clients’ pragmatic needs and resource connections while responding to their disabling symptoms associated with mental illnesses. Various case management tasks (e.g., mandatory paperwork) competed for time and attention during client meetings, with logistical challenges, such as commuting to the location of a client meeting, or facing traffic getting between clients. In addition, there were substantive issues that generated anxiety and uncertainty in case management encounters such as a client being in “crisis” at the same time as needing to work on “practical” goals, when client distress or symptoms were interfering with decision-making, motivation, or an ability to take action. These very issues were discussed during the consultations in which case managers could receive support and guidance from peers and facilitators, with relevant application of ESPT case conceptualization, utilizing the CoP case-based learning to manage such challenges. So for a long time I always felt like I was the only one doing this…it was like trying to re-invent everything every single time I met a new person…so the thing I noticed here—you can put a framework on it and still…still be compassionate and flexible and responsive and put some sort of framework or some kind of evidence behind what you do. (Case Manager R1)
Discussion
Significant gaps between the need for and equitable access to MH care have catalyzed initiatives to scale up MH care and ESPT treatments. 7,40 –42 In the 2013 Canadian Community MH Survey, counseling was the highest ranked MH need and the one least likely to be met. 43 This pilot sought to address this in part through capacity-building of MH frontline community-based case managers. Case managers comprise a large workforce who provide critically important support around the social determinants of health and care access navigation. This project aimed to deploy ESPTs in keeping with other initiatives to move the MH field away toward community-based, rather than institutional settings, 44 and mitigate problems with MH care access through capacity-building of an existing workforce vector for dissemination of ESPT practices—with frontline community-based MH and social service workers.
Psychotherapy process research has found that therapists’ interpersonal effectiveness and facilitative skills (e.g., using empathy, recognizing and repairing alliance tensions or impasses) that are common to all ESPT models strongly predict outcomes and these were emphasized in this training. 11,12 The goal of training was to integrate ESPT elements rather than achieving fidelity or adherence to the full treatment modality guidelines. There is debate on the merits and importance of fidelity to specific models in contrast to an eclectic, integrative approach that emphasizes therapeutic responsiveness and facilitative interpersonal skills. We chose the latter for two reasons: (i) to foster adaptive expertise using a repertoire of ESPTs in response to complex transdiagnostic challenges and individual patient differences and (ii) psychotherapy process research demonstrates that the therapeutic alliance and other common factors moderate outcomes, more than modality adherence. 11 –13 Modality-specific fidelity standards that define technical elements provide an important scaffold, roadmap, and structure with beginning, middle, and concluding phase tasks; however, technical elements must be delivered with attention to dyadic, patient–therapist processes and trauma-informed, culturally sensitive responsiveness to individual patient differences. Elements of ESPT models endorsed as most salient to case management practices included IPT, 3,30 mentalizing, 33 and MI. 31,32 It is possible that the IPT phase- and focus-specific structure facilitated goal setting within the conceptualization of social roles with a focus on important relationships and also provided pragmatic guidelines in the termination phase tasks for the rapid response, time-limited service model. Whereas mentalizing assisted case managers to recognize client interpersonal deficits and repair alliance tensions, and MI and motivational enhancement strategies offered an approach that aided client reflection, motivation, and goal setting with therapeutic alignment.
Strengths of this pilot include the context of its delivery within a CoP of MH case managers, 22,23 the use of a multimodal interactive case-based curriculum 25 to foster adaptative expertise, 16 applying knowledge translation principles within a supportive organization, 22 with mixed methods of evaluation. The training was widely endorsed as a useful adjunct to MH case management with improved counseling self-efficacy. Comparing our COSE results to earlier conducted training studies of singular therapy models (CBT, MI, or DBT), 14,15 we found similar improvements in the subscale of working with challenging patient behaviors, with additional improved microskills. COSE self-ratings have been associated with external ratings of therapeutic competence suggesting that along with the qualitative findings, this intervention did indeed build capacity. 38 Limitations of this pilot included the small sample size and lack of patient outcomes in the evaluation framework. Though a full curriculum of ESPT models were presented, allegiance bias is known to influence outcomes of psychotherapy research, and in this case, the facilitator’s ESPT expertise (PR) was situated in IPT and mentalizing; thus, it is possible that differing facilitators of a similar curriculum from a compendium of ESPTs may result in differing “takeaway” lessons learnt. Challenges with ESPT integration into MH case management included time constraints and competing priorities to help clients with distressing symptoms that interfered with addressing pragmatic needs around the social determinants of health.
Conclusions
This capacity-building pilot demonstrated that longitudinal training of MH case managers, within a CoP, in trauma-informed, culturally sensitive application of ESPT principles was feasible and has scalable potential to improve case managers’ counseling self-efficacy, reflective capacity, empathy, and morale. Future capacity-building ESPT research with a larger sample, external ratings of therapeutic effectiveness, and patient outcomes, including health utilization, is needed with potential to lessen the gap between the unmet needs and access to mental healthcare.
Footnotes
Acknowledgments
We wish to thank the participating case managers and managers, their clients, the Toronto North Support Services, COTA-Inspires, Catherine Chan, Norine Thompson, Eloise Ballou, and Isabelle Kim.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.