
Abstract
Objective:
Bilateral anterior capsulotomy (BAC) is one of the ablative neurosurgical procedures used to treat major depressive disorder or obsessive-compulsive disorder when all other therapies fail. Tristolysis, a reduction in sadness, is the most striking clinical effect of BAC and is seen in the first 1 to 2 weeks after surgery. This retrospective study measured regional cerebral blood flow (rCBF) following surgery to identify which cortical regions were impacted and could account for this clinical effect.
Methods:
All patients had their capsulotomies done in Vancouver by the same team. Pre- and postoperative single-photon emission computed tomography perfusion scans were analyzed for 10 patients with major depressive disorder and 3 with obsessive-compulsive disorder. rCBF was measured semiquantitatively by calculating the ratio between an identified region of interest and a whole brain reference area.
Results:
Decreased rCBF was found in the paraterminal gyri. Increased rCBF was found in the dorsolateral prefrontal cortices and in the left lateral temporal lobe.
Conclusions:
BAC causes hypoactivity in the paraterminal gyri and is the most likely explanation for its tristolytic effect, suggesting that the paraterminal gyrus is the limbic cortical locus for the emotion of sadness. Increased activity in the dorsolateral prefrontal cortices may be occurring via connectional diaschisis, and suppression by overactive paraterminal gyri during depression may account for some of the neurocognitive deficits observed during depressive episodes.
Introduction
Up to 10% to 15% of patients with major depressive disorder 1,2 and 40% to 60% of obsessive-compulsive disorder (OCD) 3 remain refractory to standard treatments that include psychotherapies, pharmacotherapies, and electroconvulsive treatment. Other extracranial neuromodulation therapies for depression (transcranial magnetic stimulation, transcranial direct current stimulation, and vagus nerve stimulation) are promising, still evolving, and with effect sizes that are generally small to moderate. 4 In OCD, the role of neuromodulation therapies remains even more uncertain. 5 Surgical strategies are the remaining option. Deep brain stimulation, an intracranial invasive neurosurgical intervention, is still experimental. Initial stimulation targets for the treatment of depression failed. 6 More recently, stimulation of the superolateral branch of the medial forebrain bundle seems encouraging. 7 When everything else has failed, ablative surgical interventions (anterior capsulotomy, cingulotomy, subcaudate tractotomy, and limbic leucotomy) remain as a last option. In 1998, the Vancouver Limbic Surgery Group was formed as a clinical program to offer surgical treatment for severe treatment-resistant depression (TRD) and treatment-resistant obsessive-compulsive disorder (TROCD) for patients living in British Columbia, Canada. Bilateral anterior capsulotomy (BAC) was selected as the target for both conditions. In this surgery, a substantial portion of the horizontal fibers in both anterior limbs of the internal capsules (ALIC) are destroyed by radiofrequency lesions. 8
Since its inception 20 years ago, 17 patients have undergone this procedure at our center: 12 for TRD and 5 for TROCD. The entry criteria, ethical approval, clinical and imaging monitoring protocols, and the outcomes for the first eight patients with TRD with follow-up data for at least 24 months have been reported previously. 9
The most striking effect of BAC is the rapidity of effect upon suicidality because of the reduction in sadness, the psychic pain associated with the depressive syndrome. This dramatic reduction in sadness is seen in the first 1 to 2 weeks after surgery, when clarity of thinking and the capacity to introspect returns presumably because the perilesional, bifrontal-located edema caused by the capsulotomies has sufficiently subsided (Supplemental Figure 1). To describe this phenomenon, we invented the term “tristolysis” (tristis: sadness; lysis: destruction of), as there was no existing term to describe this phenomenon 9 (Supplemental video clips—the tristolytic effect).
The aim of this retrospective study was to clarify which cortical regions are affected by severing fibers in the ALIC and which would account for the observed acute tristolytic effect. In the capsulotomy literature, the cortical targets of the severed axons have never been identified. There are no anatomical pathology studies. There are several studies of brain function after BAC using radiolabeled glucose or glucose analogs with positron emission tomography (PET). Only patients with TROCD and anxiety disorders have been studied and mostly 6 to 12 months after capsulotomy. The most common cortices that show reduced metabolism are the orbitofrontal/orbitomedial cortex and anterior cingulate gyrus. 10 –13 The effect of deep brain stimulation (DBS) of the ALIC has also been studied. The functional effect varies whether it is neuronal clusters or axons that are stimulated, with time and whether high- or low-frequency stimulation is applied. 14 –16 DBS cannot therefore be equated to an ablative procedure where the consequence is to immediately and permanently interrupt the targeted axonal pathways. Notwithstanding these uncertainties, fluorodeoxyglucose PET after ALIC DBS has been done and showed decrease in orbitofrontal/frontal metabolic activity. 17,18 Moreover, only patients with TROCD have been studied, sample sizes have been small (n = 3), and scans done at 3 weeks to 3 months after stimulation commencement. 17,18
BAC severs the majority of the horizontal fibers of the anterior capsule (Supplemental Figure 3). Based upon magnetic resonance imaging (MRI), the axonal fibers of the anterior capsule appear to originate primarily out of the anterior nucleus and also possibly the dorsomedial nuclei of thalamus. 8 Structural imaging by MRI was not able to identify the trajectory of the anticipated anterograde Wallerian degeneration, presumably because of fanning out of fibers as they travel rostrally. For MRI identification of Wallerian degeneration, there needs to be sufficient fibers that are consolidated into discrete tracts. 8 However, as part of the existing clinical and monitoring protocol, brain neuronal metabolic activity was assessed presurgically and after surgery with single-photon emission computed tomography (SPECT) with the goal of identifying the cortical targets of the transected fibers to explain benefit, account for any emergent side effects, and guide surgical technique.
The cortical regions linked to the severed fibers in the ALIC were expected to show altered metabolic activity due to severance of neural input or retrograde neural death from transection of axons arising from reciprocal neurons. The location of the target neurons was predicted based upon anatomical and historical considerations. 8,19 –21
Anatomically, the fibers of the ALIC are directed toward the cortex of the frontal lobe. 19 These fibers can be segmented into five general regions in a complex 3 level ventral to dorsal arrangement: ventromedial prefrontal cortex/orbitofrontal cortex, dorsal anterior cingulate cortex, ventrolateral prefrontal cortex, dorsomedial prefrontal cortex, and dorsolateral prefrontal cortex. 22 Capsulotomy targets only the horizontal fibers in the ALIC. MRI postcapsulotomy has identified two primary corticopetal tracts. 8 These lie in the ventral ALIC. The medial tract maps the anterior thalamic radiation. The lateral tract arises from the brain stem and maps the pathway of the medial forebrain bundle. 8,23 Since most, if not all, of the fibers of the anterior thalamic radiation originate out of the anterior nucleus of thalamus (ANT), this anatomical structure could be utilized to predict cortical connectivities. 8 Within the ANT, only the anteromedial nucleus has extensive reciprocal connectivity with the anterior cingulate and orbitomedial prefrontal cortex and is involved in executive and emotional functions. The anterodorsal subnucleus of the ANT has its chief connectivities to the postsubiculum retrosplenial cortex and the anteroventral subnucleus to the subiculum, presubiculum, and parasubiculum. 20 None of the ANT’s subnuclei have any known connectivity with the dorsolateral prefrontal cortex. 20,24
Historical neurosurgical interventions that have been utilized in the treatment of psychiatric disorders also shaped our search for the cortical targets of capsulotomy. Other than BAC, subcaudate tractotomy (SCT) and cingulotomy are the two other historical ablative surgical targets utilized in the treatment of TRD and TROCD. Stereotactic limbic leucotomy is a combination of bilateral cingulotomy and bilateral SCT. Historically, no surgical treatment has lesioned the frontal pole for TRD. 21
Comparisons concerning the relative efficacy of these three ablative surgeries is complex as series are small, only some studies are prospective, and outcome measures and duration of follow-up differ. Benefit may differ whether the indication is for TRD or TROCD, and it remains unclear why the same ablative surgeries are effective for TRD and TROCD, which are seemingly very different psychiatric disorders.
Among these three ablative surgeries, single bilateral cingulotomy is the least effective for both TRD and TROCD. 9,21,25 –27 Cingulotomy often requires up to three bilateral lesions, the transformation into a limbic leucotomy or is added to a preexisting anterior capsulotomy.
Capsulotomy may overlap anatomically with cingulotomy. Axons severed in capsulotomy may connect with the subcallosal extension of the cingulate gyrus independently or via the terminal cingulum. Subcallosally, the cingulate gyrus tapers to a narrow, medially located cortical ribbon as it approaches the septal area (Figure 1). MRIs completed by our group have shown that this overlap and potentially common primary cortical target is unlikely, as the Vancouver capsulotomy lies at the level of the anterior third of the cingulate gyrus and includes the full extent of the horizontal fibers of the ALIC (Supplemental Figure 4). Capsulotomies at other centers target the more ventral segment of the capsule, which also impinges upon the adjacent ventral striatum. 28,29 Our capsulotomy (4.8 to 5.8 mm in width and 14.2 to 14.8 mm in height) is however narrower and shorter than the Dundee and Stockholm capsulotomies (8 mm in width and 18 to 20 mm in height). 8,30,31 True ventrally confined capsulotomies have not however been effective, at least for TROCD. 29

Mid-sagittal section of the brain with relevant anatomy highlighted. 1 = corpus callosum; 2 = cingulate gyrus; 3 = subcallosal extension of cingulate gyrus; 4 = septal area; 5 = gyrus paraterminalis; 6 = orbitofrontal gyrus; 7 = frontal pole.
SCT involves lesioning the subcallosal white matter of the prefrontal cortex. 32,33 As with cingulotomy, it is unclear what are the critical structures that need to be ablated to provide therapeutic benefit. Recent lesion analysis of SCT has shown that this lesion includes damage to the paraterminal gyrus (PTG), the subcallosal extension of the cingulate gyrus, and the orbitofrontal cortex. 34
By refining these anatomical and historical data, we thus hypothesized that the maximal impact of BAC would be on the ventral prefrontal cortex (paraterminal or orbitofrontal gyri). Despite the size of the capsulotomy, visual inspection of SPECT scans of individual patients failed to demonstrate any areas of hypoperfusion post-BAC in these anticipated or any other cortical regions. This study was therefore undertaken retrospectively to determine whether it was possible to identify the cortical targets that were most impacted by BAC by semiquantitatively measuring relative regional cerebral blood flow (rCBF).
Methods and Materials
Pre- and postoperative SPECT perfusion scans were retrospectively analyzed. rCBF was measured semiquantitatively by calculating the ratio between an identified region of interest (ROI) and a whole brain reference area. The average activity in the ROIs postsurgery was compared to the average activity in the same ROIs presurgery to identify areas in which cerebral blood flow had changed. The study received ethics approval from University of British Columbia’s Clinical Research Ethics Board (#H10-00851 and #H16-01722).
SPECT Imaging
A Siemens Multispect 3 Camera (Siemens Healthcare, Munich, Germany) with an energy window of 20% centered at 140 keV was used. Patients underwent brain perfusion SPECT with Tc99m-ethylene cysteine dihydrochloride (ECD) (Neurolite, Lantheus Medical Imaging, N. Billerica, MA). If Tc99m-ECD was unavailable at the time of scan, Tc99m-hexamethylpropyleneamine oxime (HMPAO; Ceretec, GE Healthcare, Arlington Heights, IL) was used as the alternative. Patients were given an IV bolus of 740 MBq of Neurolite or 900 MBq of Ceretec 40 min before the scan in a quiet, dimly lit room where the patient could rest comfortably to minimize audiovisual stimulation. Patient demographics and scan data are given in Supplemental Tables 1 and 2. The initial monitoring protocol aimed at performing the postsurgical SPECT at 2 months after surgery, but due to logistical reasons, the scans were completed between 2 and 10 months postsurgery (Supplemental Table 2).
Both radiotracers measure rCBF, which is closely linked to regional cerebral metabolism under conditions of normal brain autoregulation. ECD and HMPAO are both lipophilic agents which passively cross the blood–brain barrier but are then trapped within neural tissue reflecting distribution at the time of administration. Measurement of rCBF (as a surrogate for neuronal metabolic activity) is typically done by visual analysis but can be measured semiquantitatively by calculating the ratio between an identified ROI and a reference area (ROI/reference area). This ratio provides an index of relative rCBF in the specified ROI and may be unchanged or show an increase or a decrease, indicating either hyperperfusion (hypermetabolism) or hypoperfusion (hypometabolism), respectively. ROI ratios can be compared within or between patients and between different studies. 35,36
Patients Characteristics
Fifteen patients are included. Our two most recent patients are not included as their data have not yet been analyzed. Of the 15 patients, 1 patient was excluded from the analysis because he did not return for his follow-up scan, and a second patient was excluded because the scan data were missing—see flow chart. Thirteen patients remained for analysis, 10 were TRD and 3 were TROCD. We analyzed them together as the surgery is identical and the surgical, anatomical, and physiological effects should be the same. Nine were females and 4 males, with an average age of 38.9 years (age range: 21 to 76); 12 were right-handed, and all had completed a minimum education level of high school. The full demographics are given in Supplemental Table 1.
This was followed by a subset analysis of eight patients to address our concerns that the data in five patients could confound the results owing to different slice thickness set by the imaging parameters at the time of the scan and/or that ECD and HMPAO were used as radiotracers either for the first or the second scans or for both pre- and postoperative studies (Supplemental Table 2). Different relative tracer distribution may occur with ECD and HMPAO. Semiquantitative comparisons using these two different radiotracers may thus be unreliable. 37
The subset of eight all had scan slice thickness of 3.56 mm and used ECD for both pre- and postoperative studies (Supplemental Table 2).
Image Analysis
Analysis of final SPECT images was performed using Xeleris software Version 2 (GE Healthcare, United Kingdom) for image sets gathered before and after surgery. Relative rCBF was estimated by normalizing the regional count densities to a reference whole brain slice. The SPECT scans were not coregistered against an MRI. Consequently, the thalamus was used as the central landmark. The software automatically coregisters the coronal, axial, and sagittal images to each other. The thalamus is easily identified on both axial and coronal slices. To optimize that the ROIs were placed in the same anatomical location, the midline of each scan set was identified using the coronal image where the mass of the thalamic nuclei appear to intersect (Supplemental Figure 5). Slice thickness varied between 2.21 mm or 3.56 mm for any given study and was study-dependent. The resolution was approximately 12 mm.
The whole brain reference ROI was measured from a freehand outline of the axial brain slice that coregistered with the intersecting thalami on the coronal slice. The ROIs were all 60-pixel rectangles superimposed upon the cortical ribbon. Ten ROIs were selected for each side of the brain in the sagittal and coronal planes (Figure 2) and were chosen to reflect the potential distribution of the anterior thalamic radiation and that could be reliably identified. PTG is clearly seen on the sagittal plane (Supplemental Figure 6) but is not obvious on the coregistered coronal slice, and this ROI placement was guided by the coregistered sagittal slice.
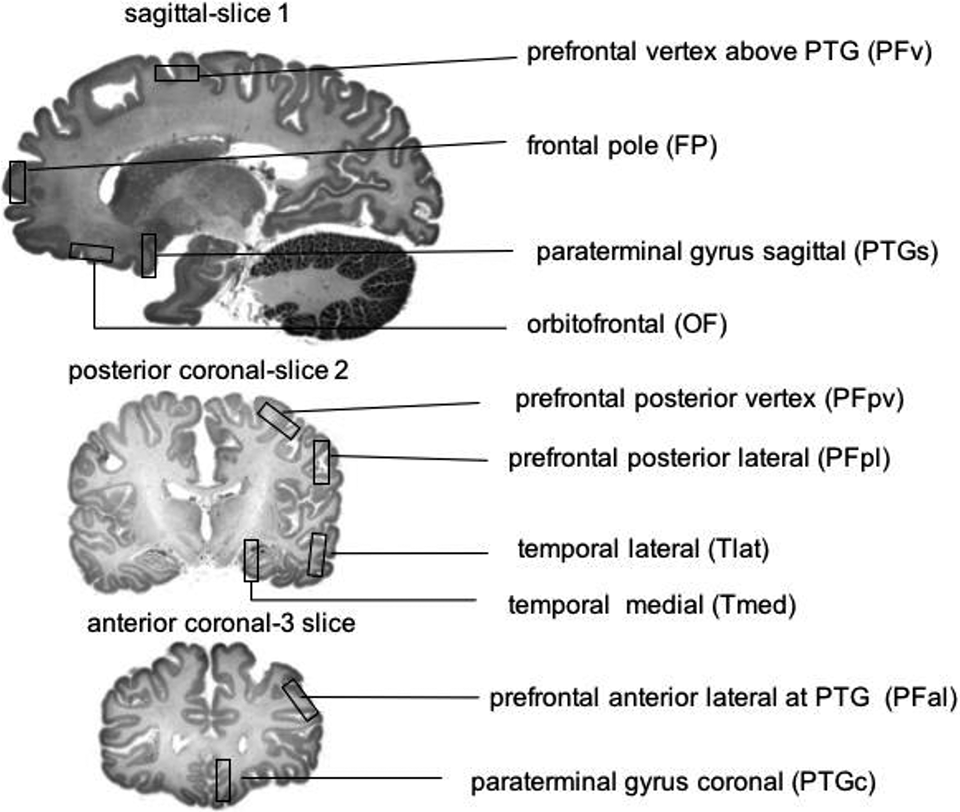
Regions of interest for SPECT analysis. Sagittal regions of interest were placed that corresponded to right and left paraterminal gyrus and orbitofrontal cortex, left and right frontal pole and left and right prefrontal vertex (sagittal—Slice 1).
PTG on the sagittal plane appears as a vertical bar contiguous with the orbitofrontal cortical ribbon (Supplemental Figure 6). As seen from the coregistered MRIs, the PTG lies medial and inferior to the capsulotomy with no overlap with the capsulotomy (Supplemental Figure 7). This ROI was placed approximately 10.5 mm away from the sagittal midline calculated on the basis of slice thickness and yielded optimal visualization of this structure. All other left and right sagittal ROIs were taken from this image slice. A posterior coronal slice was selected where the thalami nuclei appear to intersect (posterior coronal—Slice 2). On this slice, ROIs were placed that corresponded to the lateral and vertex prefrontal cortex and the lateral and medial temporal lobes. A second coronal slice was identified (anterior coronal—Slice 3). This slice lies anterior to the first coronal slice and coregisters to correspond to PTG on the sagittal slice. ROIs were drawn over left and right PTG in addition to another pair of ROIs on the lateral prefrontal cortices at this level (Figure 2).

The Xeleris software reports a count reflective of the number of γ rays emitted from a given region over the period of the scan. rCBF was obtained from the average count of the ROI normalized to the whole brain ROIs averaged across all subjects. All the primary data are available from the corresponding author. Counts of mean whole brain slices or a specified brain region have been previously used in SPECT studies for normalization of the data. 35,38
The average activity in the ROI postsurgery was compared to the average activity in the ROI presurgery using a paired two-tailed Student’s t test to determine whether there were significant increases or decreases in each ROI after surgery. Significance was defined as P < 0.05. As the ROIs to be measured were selected in advance to correlate with the known distribution of the fibers of the anterior limb of the internal capsule and the historical neurosurgical targets, no multiple testing correction was applied. The null hypothesis for each ROI was that there would be no change in rCBF after capsulotomy.
Additionally, to confirm the reliability of the SPECT method of analysis an interrater study was conducted. The calculated intraclass correlation coefficient was 0.90, 95% CI (0.88 to 0.92), indicating an excellent degree of interrater agreement.
Results
For the 13 patients, significant decreases in rCBF after surgery were found in the left and right PTG in the sagittal and coronal planes. A significant increase in relative rCBF was found in the dorsolatersal prefrontal cortex bilaterally.
For the eight patients with identical SPECT technique before and after surgery, significant decreases in rCBF after surgery were found in left PTG sagittal plane and right PTG coronal plane. Significant increases in relative rCBF were found in the dorsolatersal prefrontal cortex bilaterally and the left lateral temporal cortex (Table 1 and Figure 3). In every case, the effect size (Cohen’s d) was large (>0.8; Supplemental Table 3).
SPECT Data for n = 13 and n = 8.
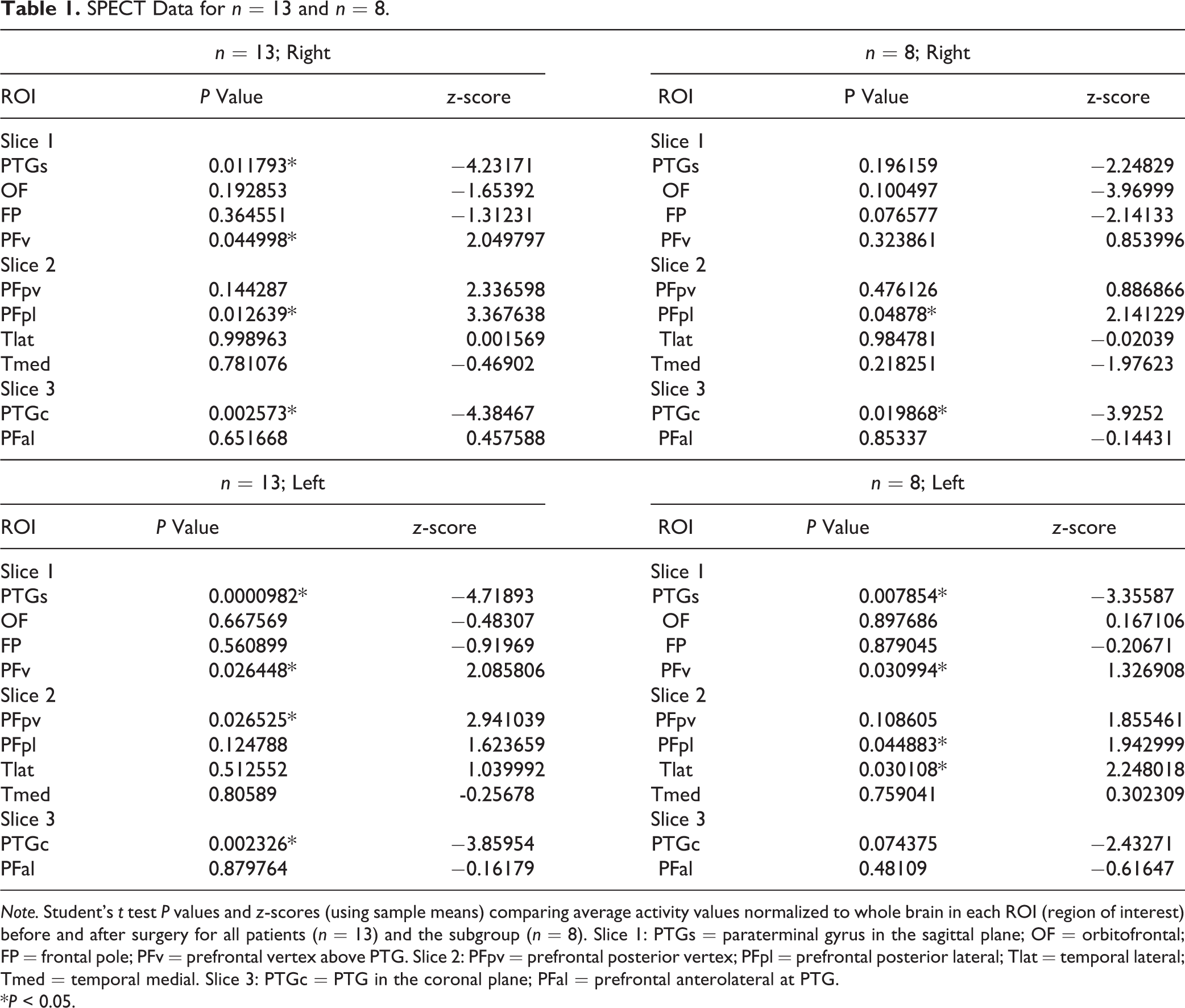
Note. Student’s t test P values and z-scores (using sample means) comparing average activity values normalized to whole brain in each ROI (region of interest) before and after surgery for all patients (n = 13) and the subgroup (n = 8). Slice 1: PTGs = paraterminal gyrus in the sagittal plane; OF = orbitofrontal; FP = frontal pole; PFv = prefrontal vertex above PTG. Slice 2: PFpv = prefrontal posterior vertex; PFpl = prefrontal posterior lateral; Tlat = temporal lateral; Tmed = temporal medial. Slice 3: PTGc = PTG in the coronal plane; PFal = prefrontal anterolateral at PTG.
*P < 0.05.
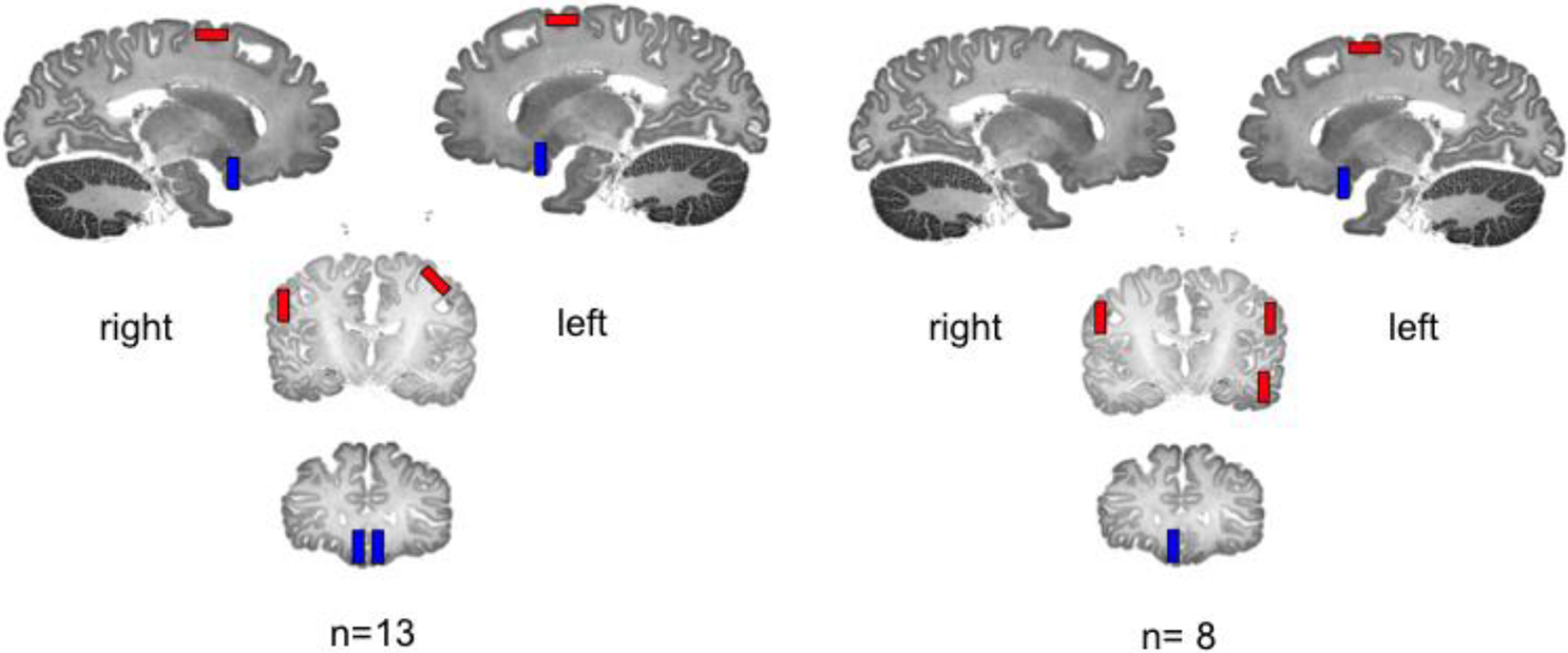
Changes in regional cerebral blood flow (rCBF). A decrease in rCBF in a given region of interest is shown as blue and an increase as red for all patients (n = 13) and for the subgroup with identical SPECT technique (n = 8).
Discussion
Severing a large bundle of reciprocally connecting axons should cause neuronal injury or death in the neurons of origin. Functioning in target neurons could be decreased or increased depending whether afferent fibers are either excitatory or inhibitory. 20 BAC appears to have its primary effect upon the corticopetal fibers originating out of the ANT with subsequent retrograde neuronal injury and presumably death as evidenced by nucleus atrophy. 8
This study of a unique sample of patients has shown that severing the ALIC results in a reduction in rCBF and by implication, cerebral cortical neuronal activity in the gyrus paraterminalis. The data from this study are most robust for the left side (P = 0.0000982). The PTG is the only cortical region that showed post-BAC hypofunction and is occurring in one of the regions predicted by historical and anatomical considerations. 8,19 –21
Our study was hypothesis-driven and specifically studied the PTG and is the first that we are aware of that identifies the PTG as the critical target of effective limbic surgeries. Other functional imaging studies after BAC have been done on patients with TROCD and anxiety disorders 6 to 12 months after capsulotomy. 10 –13 Most of these studied patients had TROCD. Our population is mostly patients with TRD and mostly studied less than 6 months after surgery.
In these other studies, the most common cortices that showed reduced metabolism were the orbitofrontal/orbitomedial cortex and anterior cingulate gyrus. 10 –13 None have specifically identified the PTG.
The anatomy of the subcallosal prefrontal region is morphologically complex and beset by terminological inconsistencies. 39 This is made even more confusing by using the Brodmann area classification to describe this region since Brodmann areas are defined by cytoarchitecture rather than topography and function connected to macroscopic and radiologically identifiable surface anatomy. 24
The subcallosal prefrontal region consists of two limbic cortical areas with their associated white matter: the subcallosal extension of the cingulate gyrus and the paraterminal gyrus 39 The anatomy here is easiest to understand when considering the embryology of the limbic lobe. The limbic lobe consists of two curved bands, an inner and outer arch, which surround the diencephalon and basal ganglia. The outer arch extends from the frontal lobe to the temporal lobe and successively includes, from anterior to posterior, the subcallosal extension of the cingulate gyrus, cingulate gyrus, parahippocampal gyrus, and uncus. The inner arch, from anterior to posterior, successively consists of the paraterminal gyrus, supracallosal gyrus (indusium griseum), fasciolar gyrus, dentate gyrus, and cornu ammonis (see Figure 4). 40
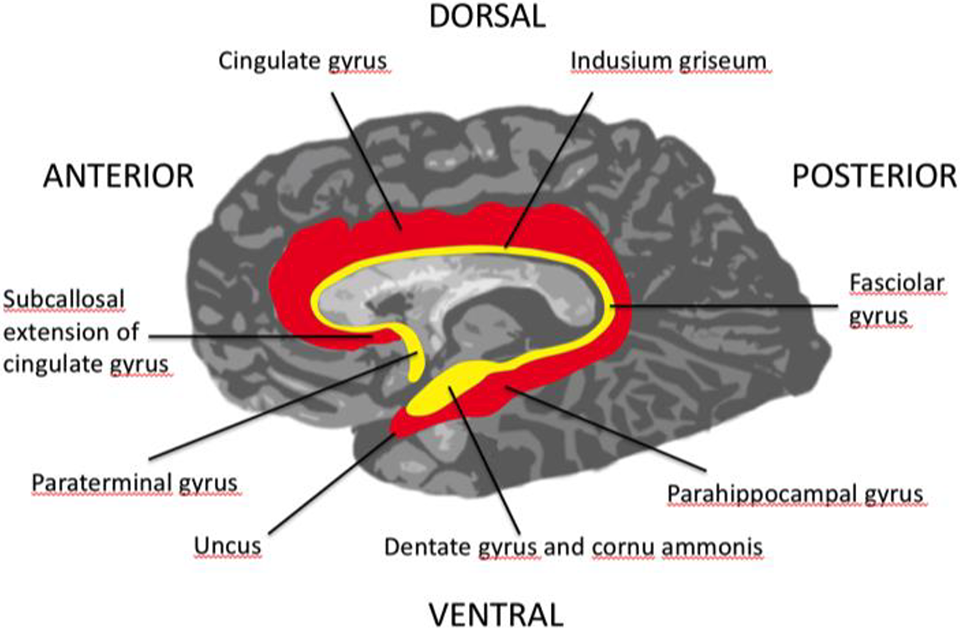
Arches of the limbic lobe. Inner (yellow) and outer (red) arches of the limbic lobe.
Surgical attempts to disrupt the outer arch via thermocoagulation of the anterior third of the cingulate gyrus (cingulotomy) or DBS of the subcallosal extension of cingulate gyrus have given limited results or have been unsuccessful. 9,21,25,26,27,41,42 Direct (subcaudate tractomy) and indirect (anterior capsulotomy) disruptions of the inner arch have produced the best results. This study via its indirect effect suggests that the psychotropic benefit of inner arch surgical interventions is derived from disruption of the function of the PTG.
Tristolysis is the most striking effect of BAC. The pathophysiological importance of tristolysis in depressive illness after BAC is that the effect is “immediate,” identifiable in the first 1 to 2 weeks after surgery when the brief stunning effect of the surgical procedure has worn off and then persists over time. BAC severs axons of passage, and the immediate clinical effect of tristolysis appears to stem from consequent hypofunctioning of the PTG. This is the reciprocal of the finding of increased rCBF in the subcallosal prefrontal region (subgenual cingulate—Brodmann Area 25) with the induction of sadness. 43 –45
This study is more anatomically specific, pointing to the PTG in the subcallosal prefrontal region as the locus of the emotion of sadness. The PTG moreover appears to be the end terminus of a circuit arising out of ANT. Using diffusion tensor MRI, we have recently demonstrated that BAC achieves optimal results by interrupting a pathway that lies medioventral in the ALIC. This pathway arises out of prefrontal thalamus (anterior and dorsomedial thalamus) and is directed to limbic areas that include the ventromedial prefontal cortex, subcallosal cingulate cortex, and the amygdala. Other diffusion MRI and animal tracing studies have confirmed such a circuit showing that the ventral ALIC carries fibers from the ventromedial PFC that project through to thalamus. 22,46
Sadness is only one of the symptoms of the depression syndrome but the source of most of the distress of this illness and is the engine that drives suicidal ideation and suicide. 47 The other components of the depressive syndrome implicate the hypothalamus and upper brain stem. Hypothalamic failure likely accounts for the neurovegetative disturbances seen in depression while the upper brain stem contains the nuclei of origin of the major monoamine neurotransmitters that serve as the target of antidepressant medications. Together, the available data strongly suggest that depressive illness is a neural network disturbance involving interconnected limbic, diencephalic, and upper brain stem structures, but the specific network nodes and circuitry remains to be elucidated. 48 –50
This study also showed increased rCBF in the dorsolateral prefrontal cortices (DLPFC), left more robust than right, and in the left lateral temporal lobe. These regions lie outside the fields of the horizontal fibers of the ALIC and should also show hypoactivity from a lesion that directly disrupts connectivity. If it is not a direct surgical effect, then one plausible explanation is via connectional diaschisis, 51 where a previously dysfunctional and overactive PTG has been inhibiting connected cortical nodes. These connected nodes now undergo postsurgical release disinhibition as the PTG becomes hypofunctional. Limbic–cortical interactions in negative mood states have been demonstrated in the past involving inverse activity in subgenual cingulate and DLPFC. During sadness, subgenual cingulate is overactive and DLPFC underactive. The pattern reverses with recovery from depression. 44
This inverse pattern of limbic–cortical functioning may explain the neurocognitive deficits in depression, particularly the problems with executive functioning 52 where an overactivated PTG suppresses function in the DLPFC.
Study Limitations
Our results need to be interpreted with caution. Even though this is a unique sample set, the sample size is small. In addition, the SPECT images were not coregistered against MRIs, which would have provided confirmatory anatomic localization. The pre- and postsurgical SPECT imaging intervals varied as did the slice thickness and radiotracer utilized. The analysis of the data was done to accommodate for slice thickness and radiotracer utilized, but this did not alter the fundamental findings. In drug-free patients, antidepressants can result in both increases and decreases in regional brain metabolism. 53 –55 All of our patients, given the severity and intractability of their illnesses, were on complex psychotropic regimens (a combination of antidepressants, mood stabilizers, antipsychotics, and benzodiazepines) for both pretreatment and postcapsulotomy SPECT scans with most medication regimens left unchanged or simplified by the time of the post-BAC scan. This makes it unlikely that the results obtained in this study were produced by medication effects.
Conclusions
BAC causes hypoactivity in the paraterminal gyri and is the most likely explanation for its tristolytic effect, suggesting that the paraterminal gyrus is the limbic cortical locus for the emotion of sadness. Increased activity in the dorsolateral prefrontal cortices may be occurring via connectional diaschisis, and suppression by overactive paraterminal gyri during depression may account for some of the neurocognitive deficits observed during depressive episodes.
Supplemental Material
Supplemental Material, 874181_supplemental_material - Hypoactivity in the Paraterminal Gyrus Following Bilateral Anterior Capsulotomy
Supplemental Material, 874181_supplemental_material for Hypoactivity in the Paraterminal Gyrus Following Bilateral Anterior Capsulotomy by Trevor A. Hurwitz, Christopher R. Honey, Kevin R. McLeod, Anujan Poologaindran and Annie J. Kuan in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
We wish to thank the BAC patients as well as Shilpa Shah, Kelly Bielby, Bella Vecina, UBC Nuclear Medicine team, Tanja Högg, Gillian Brangham, and Belinda Chen. Anujan Poologaindran would also like to acknowledge the Alan Turing Institute Doctoral Scholarship program for their support for him to conduct brain mapping studies.
Data Access
All primary data are available from the corresponding author
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the ERIN Fund, administered through the VGH and UBC Hospital Foundation, Vancouver, Canada.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.