
Abstract
Objective:
Recent reports express concerns about a mental health crisis among postsecondary students. These assertions, however, often arise from surveys conducted in postsecondary settings that lack the broader context of a referent group. The objectives of this study were (1) to assess the mental health status of postsecondary students 18 to 25 years old from 2011 to 2017 and (2) to compare the mental health status of postsecondary students to nonstudents.
Methods:
Prevalence was estimated for a set of mental health outcomes using seven annual iterations of the Canadian Community Health Survey (2011 to 2017). Logistic regression was used to derive odds ratio estimates comparing mental health status among postsecondary students and nonstudents, adjusting for age and sex. Random effects metaregression and meta-analyses techniques were used to evaluate trends in prevalence and odds ratio estimates over time.
Results:
Over the study period, the prevalence of perceived low mental health, diagnosed mood and anxiety disorders, and past-year mental health consultations increased among female students, whereas binge drinking decreased among male students. With the exception of perceived stress, the odds of experiencing each mental health outcome were lower among postsecondary students compared to nonstudents.
Conclusions:
These findings do not support the idea that postsecondary students have worse mental health than nonstudents of similar age. The perception of a crisis may arise from greater help-seeking behavior, diminishing stigma, or increasing mental health literacy. Regardless, the observance of these trends provide an opportunity to address a previously latent issue.
Introduction
Mental health among postsecondary students is an important public health concern due to high rates of psychological distress and suicidal ideation on college and university campuses. 1 Nearly one in five postsecondary students experience mental health issues, with an estimated 11% reporting suicidal ideation in the past year. 2 Unhealthy behaviors related to substance use, physical activity, and poor sleeping habits are common among postsecondary students and are linked to mental illness. 3 –6 High prevalence of mental health concerns among postsecondary students, coupled with elevated enrolment, has led to what has been termed a “mental health crisis.” 7 –10
Widely referenced reports imply the state of student mental health is declining, with one report suggesting depression and anxiety is 6 to 7 times higher among graduate students than the general population. 8 Nonetheless, key threats to validity, such as the selection bias inherent in comparing a convenience sample of postsecondary students to a representative sample of the general population, can misrepresent the appearance of a crisis. Another report demonstrated a rise in feelings of depression, anxiety, and suicidality from 2013 to 2016 among Ontario postsecondary students; however, it is unclear if similar trends exist among nonstudents. 11
Methodologically sound studies that compare trends among postsecondary students and nonstudents are limited. While psychological distress and use of mental health services appear to increase over time, 9,12 postsecondary students continue to exhibit lower prevalence of mental disorders compared to nonstudents of similar demographics. 1,13 If it exists, a mental health crisis among postsecondary students may require higher prioritization in the provision of mental health resources. However, such decisions should be informed by epidemiologic data to avoid needless transfer of resources away from groups of similar need. To inform these decisions, this study quantifies the prevalence of mental health outcomes from 2011 to 2017 among postsecondary students aged 18 to 25 years and compares the odds of each mental health outcome between postsecondary students and non-postsecondary students in Canada.
Methods
Data Sources
The Canadian Community Health Survey (CCHS) is a series of cross-sectional health surveys that include a set of questions related to mental health. Detailed information is available from Statistics Canada. 14 In brief, the target population is Canadian household residents at least 12 years of age, excluding persons living on reserves, residents of health institutions, full-time members of the Canadian forces, and residents of remote areas (<3% of the national population). 14 A stratified multistage sampling design was applied, with survey and bootstrapped weights to account for unequal selection probabilities, clustering techniques and nonresponse. This study used seven cycles of the annual CCHS survey (2011 to 2017), restricted to individuals aged 18 to 25 years.
Measures
Student status
Postsecondary students were defined as 18- to 25-year-old current students who completed secondary school and were enrolled full time or part time. The referent group comprised nonstudents and the remaining sample who had not completed secondary school or equivalent.
Mental health outcomes
Outcomes were derived based on the following questions:
“In general, would you say your mental health is…?” Perceived mental health compared “fair/poor” perceived mental health to “excellent/very good/good” perceived mental health.
“How often do you have trouble going to sleep or staying asleep?” Persistent sleep trouble compared responses of “all of the time/most of the time” to “never/rarely/sometimes.”
“Thinking about the amount of stress in your life, would you say that most of your days are…?” Persistent stress compared “quite a bit stressful/extremely stressful” to “not at all stressful/not very stressful/a bit stressful.”
Past-year major depressive episode (MDE) was identified using the Composite International Diagnostic Interview–Short Form (CIDI-SF) for major depression, a validated semistructured interview based on Diagnostic and Statistical Manual of Mental Disorders–IV symptoms of MDE. 15 A cutoff composite score of 0.9 or higher indicated a past-year MDE.
A set of questions pertained to conditions diagnosed by a health professional. Lifetime mood and anxiety disorders were defined as a self-reported diagnosis by a health professional.
A set of questions pertained to suicidality. For example, “Have you ever seriously considered committing suicide or taking your own life…in the past 12 months?” Past-year suicidality was any experience of suicidal ideation or attempts in the past 12 months. Prevalence estimates were combined for 2011/2012, 2013/2014, and 2015/2016 to meet sample size requirements.
“How often in the past 12 months have you had five or more drinks on one occasion.” Past-year binge drinking was consumption of at least five drinks on one occasion in the past 12 months.
A set of questions pertained to illicit drug use. For example, “Have you ever used cannabis…in the past 12 months?” Past-year drug use was divided into two binary variables: (a) cannabis use or (b) other illicit drug use (excluding cannabis) in the past 12 months.
“In the past 12 months…have you seen or talked to a health professional about your emotional or mental health?” Mental health consultations were defined as at least one visit to a health professional in the past 12 months.
Statistical Analysis
Prevalence estimates for each mental health outcome were derived from each survey. Logistic regression was used to compare the odds of mental health outcome in current postsecondary students to non-postsecondary students, adjusted for age and sex. Survey weights and bootstrap techniques were applied to ensure the estimates were representative at the national level. A set of 500 to 1,000 replicate sampling weights was applied to survey-specific estimates for this study.
To account for sources of heterogeneity, including methodological changes, declining response rates, and optional content not collected by all provinces each year (e.g., CIDI-SF module), estimates were compared using random effects metaregression and meta-analysis techniques (α = 0.05). Heterogeneity between survey estimates was assessed by τ2 and I 2 statistics; however, an a priori decision was made to use a random effects model in the analysis since they resemble fixed effects models when heterogeneity is low.
Results
Table 1 reports sex-specific trends in mental health outcomes among postsecondary students from 2011 to 2017 (N = 14,500) Prevalence of perceived low mental health, mood disorders, anxiety disorders, and past-year mental health consultations increased significantly among females. Prevalence of suicidality also increased (2.1% to 6.3%) and prevalence of binge drinking decreased (31.7% to 26.9%), albeit neither was significant. Conversely, binge drinking decreased from 47% in 2011 to 28% in 2017 among males, with no evidence of a significant change in other mental health outcomes. For comparison, trends in the prevalence of mental health outcomes among individuals who are not postsecondary students (N = 20,600) are reported in Supplemental Table S1. Ninety-five percent confidence intervals are provided in Supplemental Table S2.
Metaregression and Meta-Analysis Output for the Prevalence of Mental Health Outcomes Among 18- to 25-Year-Old Postsecondary Students from 2011 to 2017, Stratified by Sex.
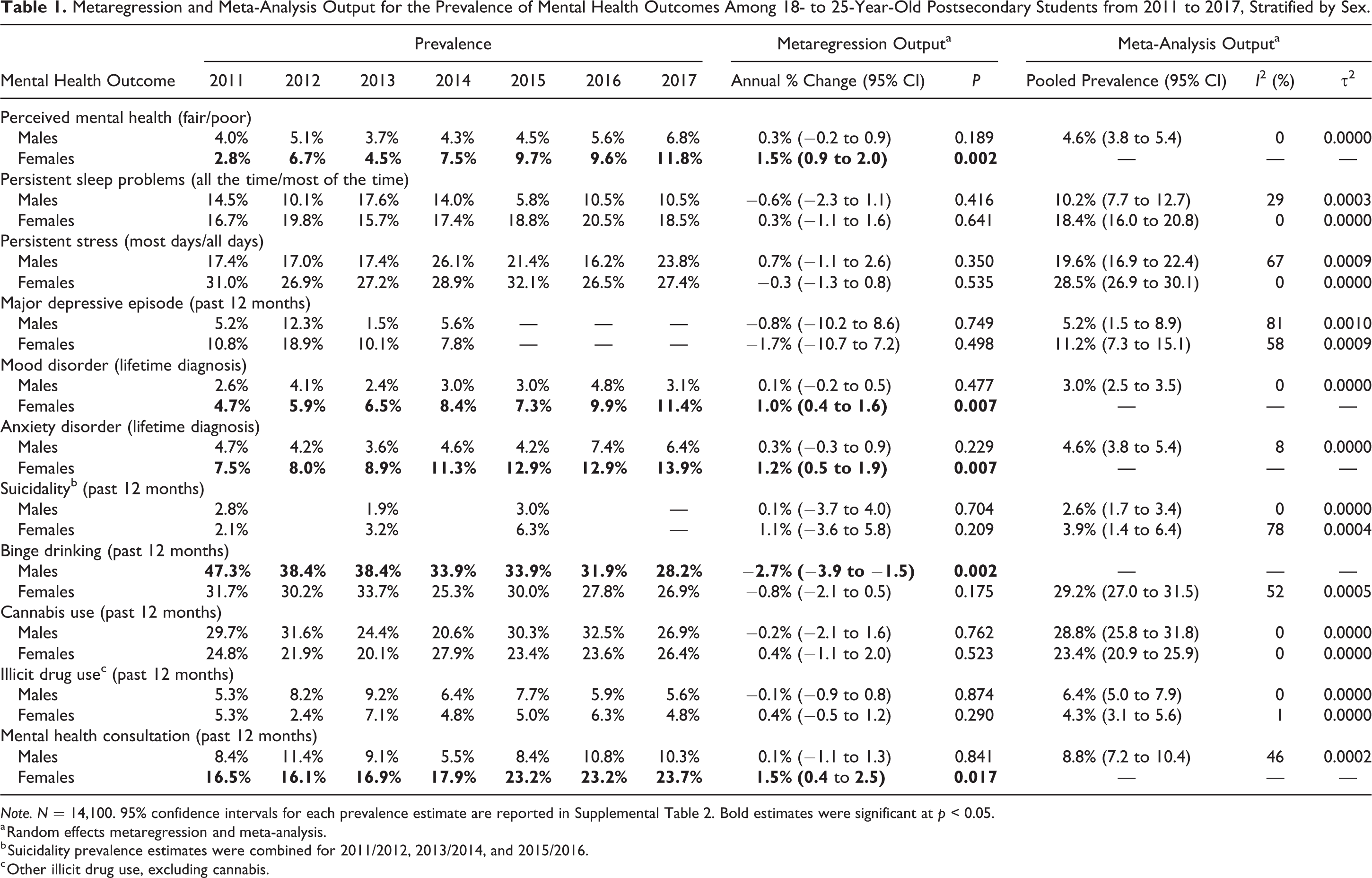
Note. N = 14,100. 95% confidence intervals for each prevalence estimate are reported in Supplemental Table 2. Bold estimates were significant at p < 0.05.
a Random effects metaregression and meta-analysis.
b Suicidality prevalence estimates were combined for 2011/2012, 2013/2014, and 2015/2016.
c Other illicit drug use, excluding cannabis.
With the exception of persistent stress (OR = 1.39; 95% CI: 1.28 to 1.52), the odds of experiencing each mental health outcome were lower among postsecondary students when compared to nonstudents (Table 2); odds ratio estimates ranged from 0.53 (95% CI: 0.47 to 0.61) for diagnosed mood disorders to 0.92 (95% CI: 0.85 to 0.99) for past-year binge drinking. There were no significant differences detected for past-year MDE, suicidality, or mental health consultations.
Meta-Analysis Output Comparing the Odds of Mental Health Outcomes among Students and Nonstudents 18 to 25 Years Old from 2011 to 2017.
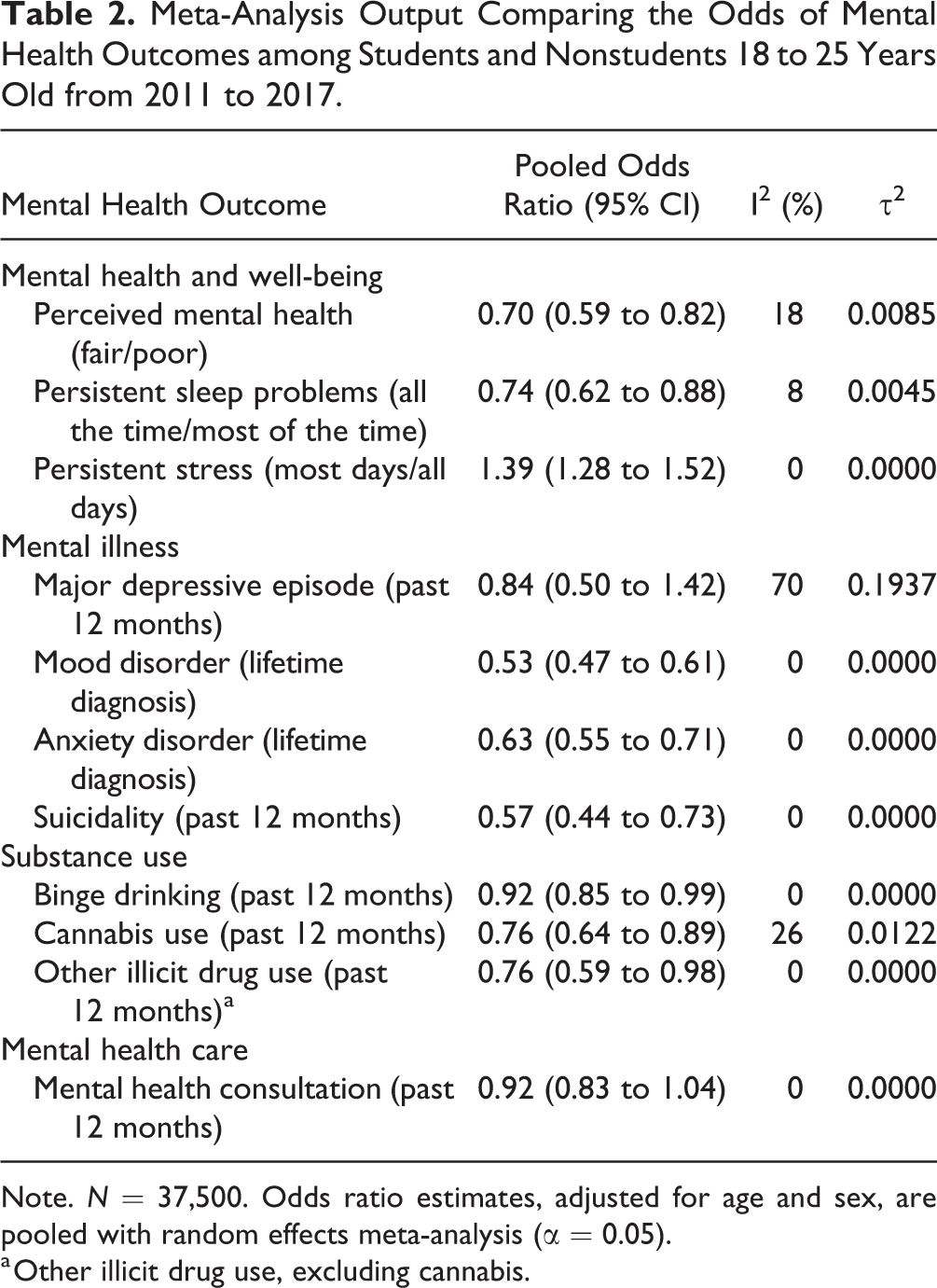
Note. N = 37,500. Odds ratio estimates, adjusted for age and sex, are pooled with random effects meta-analysis (α = 0.05).
a Other illicit drug use, excluding cannabis.
Discussion
The results do not imply the emergence of a mental health crisis among postsecondary students, but rather highlight the need for improved response to handle mental health issues among both postsecondary student and nonstudent populations. While a rise in diagnosed mood and anxiety disorders paralleled a rise in poor/fair perceived mental health and mental health consultations among female students, symptom-based measures of persistent sleep problems and stress levels remained stable over time. Likewise, a decrease in binge drinking was the only trend observed among male students. When compared to non-students, the odds of most mental health outcomes were lower for postsecondary students of the same age range. The perception of worsening mental health among postsecondary students may result from better recognition of mental disorders or help-seeking behavior, particularly among females. Research suggests females disclose mental health concerns more readily than males, which corresponds to the sex differences observed in trends over time. 16,17
This study has some limitations to note. As the target population consists of household residents, these findings may not represent postsecondary students living on campus residence. Further, certain mental health indicators were optional content, meaning not all outcomes were assessed in every province each year. Provincial differences may distort the results, however, previous work on trends in MDE reported this to have minimal, if any, effect on trends. 18 Finally, in the absence of a comprehensive set of mental health outcomes, this study selected variables based on their relevance to mental health and consistency of inclusion over time. An important variable, MDE, was only available from 2011 to 2014, and it is possible trends in later years were missed.
In conclusion, the findings suggest the assertion of a “mental health crisis” among postsecondary students is premature and not supported by epidemiologic data. One interpretation is that increased mental health literacy contributes to better identification of mental health issues; 19 however, the literature remains limited. 20 Even so, the implications are the same: a need for the health system to respond to the unmet mental health needs that are uncovered among both postsecondary student and nonstudent populations.
Supplemental Material
Supplemental Material, 874178_Supplemental_File - Mental Health among Canadian Postsecondary Students: A Mental Health Crisis?
Supplemental Material, 874178_Supplemental_File for Mental Health among Canadian Postsecondary Students: A Mental Health Crisis? by Kathryn Wiens, Asmita Bhattarai, Ashley Dores, Pardis Pedram, Jeanne V. A. Williams, Andrew G. M. Bulloch and Scott B. Patten in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
The analysis was conducted at the Prairie Regional Data Centre, which is part of the Canadian Research Data Centre Network (CRDCN). The services and activities provided by the CRDCN are made possible by the financial or in-kind support of the SSHRC, the CIHR, the CFI, Statistics Canada, and participating universities whose support is gratefully acknowledged. The views expressed in this article do not necessarily represent the CRDCN’s or that of its partners.
Data Access
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cuthbertson & Fischer Chair in Pediatric Mental Health held by Scott Patten and the Mathison Centre at the University of Calgary.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.