
Abstract
Background:
With the recent legalization of nonmedical cannabis in Canada, it is important to document previous associations between cannabis use and major depressive episode and suicidal ideation, as well as the extent to which these associations have changed over time.
Methods:
This study uses pooled data from the 2002 and 2012 Canadian Community Health Survey’s Mental Health Component, which are repeated cross-sectional surveys of nationally representative samples of Canadians 15 to 60 years of age (n = 43,466). Binary logistic regression was performed, applying weighting and bootstrapping, to examine the association between at least monthly use of cannabis and past 12-month suicidal ideation and major depressive episode (MDE).
Results:
At least monthly nonmedical cannabis use was associated with an increased odds of MDE and suicidal ideation, and both associations strengthened in 2012 compared to 2002. Canadians using cannabis at least once a month in 2012 had 1.59 (95% confidence interval [CI], 1.11 to 2.27) times the odds of experiencing suicidal ideation and 1.55 (95% CI, 1.12 to 2.13) times the odds of experiencing MDE compared to those who used cannabis at least once a month in 2002. This temporal change remained after controlling for other substance use.
Conclusions:
Monthly cannabis use was consistently related to both suicidal ideation and MDE, and these associations were stronger in 2012 compared to 2002. The findings of this study provide a baseline for the association between cannabis use and suicide and depression in the Canadian population that should be reevaluated now that nonmedical cannabis has been legalized.
Depression is the leading cause of global disability, with suicide being one of the leading causes of death. 1 Cannabis is one of the most commonly used nonmedical substances worldwide 2 and has been consistently associated with depression and suicide. 3,4 In a Canadian population sample, cannabis dependence was significantly higher in individuals with major depression (5.1% lifetime dependence, 2.9% past-year dependence) in comparison to those without depression (1.4% lifetime dependence, 0.4% past-year dependence). 5 Previous meta-analyses of longitudinal and case-control studies have found regular cannabis use at baseline to be associated with over 1.5 times the odds of experiencing depression, 2.5 times the odds of experiencing suicidal ideation, and over 3 times the odds of reporting suicide attempts at follow-up compared to those who did not use regularly. 3,4
Over the past 20 years, there have been important legal, social, and biochemical changes associated with cannabis use, which lead to questions about the impact on depression and suicide. Canada allowed for legal use of medical cannabis in 1999 with multiple changes in this policy over the years. 6 In October 2018, use of nonmedical cannabis became legal across Canada. The perceived risk of using cannabis has been decreasing, while its social acceptability has been increasing. 7 –10 Biochemically, the composition of nonmedical cannabis, which appears to play a role in the association between use and depression, 11 has changed over the past decade in the illicit market. 12 The amount of delta-9-tetrahydrocannabinol (THC), the primary psychoactive cannabinoid, in nonmedical cannabis has been increasing while cannabidiol (CBD) has been decreasing. 12 –14 Thus, it is important to document the extent to which associations between cannabis use and depression and suicide have changed over time in the Canadian population.
A limited number of studies have examined changes in the co-occurrence of substance use disorders (SUDs) and other mental disorders over time. For example, analyses of data from the National Survey on Drug Use and Health (NSDUH) in the United States comparing rates of co-occurring SUDs and other types of mental disorders over time found that, between 2008 and 2014, there was a significant decrease in the prevalence of co-occurrence among 18- to 25-year-olds, no difference in 26- to 49-year-olds, and an increase in 50-year-olds and older. 15 Among youth ages 12 to 17 years, the NSDUH found that the prevalence of co-occurring SUDs and major depressive episode (MDE) was similar from 2006 to 2014 but lower than 2004 and 2005. While informative, these findings focus exclusively on SUDs and not use in general and do not delineate changes over time in the co-occurrence of specific substances, that is, cannabis use and specific mental disorders (i.e., depression). Different approaches to measurement of mental disorders among adults across survey periods between 2002 and 2012 in the NSDUH limit comparability over time. Given these data come from a US sample, the results may not be generalizable to the Canadian context due to heterogeneity in policies related to medical and nonmedical cannabis between countries that may differentially affect the association between cannabis use and mental disorders. 16
The objective of this study was to examine the associations between cannabis use and MDE and suicidal ideation among Canadian adults and determine the extent to which these associations have strengthened between 2002 and 2012. The results of this study provide baseline evidence prior to nonmedical legalization in Canada and, if repeated after legalization, can provide critical evidence to help determine the effects of legalization of nonmedical cannabis on depression and suicidal ideation in the Canadian population.
Methods
Design and Sampling
This study is a secondary analysis of data that come from the 2002 Community Health Survey Cycle 1.2 Mental Health and Well-being (CCHS 1.2) and 2012 Canadian Community Health Survey’s Mental Health Component (CCHS-MH). These are repeated cross-sectional surveys of nationally representative samples of Canadians 15 years of age and older. 17,18 Individuals living on reserves, employed full-time in the Canadian Forces, or institutionalized were not included in the CCHS 1.2 or CCHS-MH (∼2%-3% of the Canadian population). 17,18 Please refer to the user guides for more details on the sampling approach. 17,18
Data were collected using standardized computer-assisted interviewing (CAI) by trained Statistics Canada interviewers. Most interviews (∼87%) were conducted in person in participants’ homes, with the remainder completed over the telephone. To minimize nonresponse, all selected participants received introductory letters, multiple visits at different times on different days were attempted, efforts were made to schedule interview times if visit times were inconvenient, interviews were offered in multiple languages, and individuals who first refused to participate received letters stressing the importance of participation, followed up by a second visit or call from a senior interviewer or supervisor to encourage participation. In 2002, there was an 86% (n = 41,560) household response rate, 89% (n = 36,984) individual response rate, and a combined Canadian response rate of 77%. In 2012, there was a 79.9% household response rate (n = 29,088) and 86.3% individual response rate (n = 25,113), creating an overall response rate of 68.9%. Total nonresponse is accounted for in weighting procedures. For more details regarding the design, sampling, and weighting procedures, see the CCHS 1.2 and CCHS-MH User Guides. 17,18 Note Statistics Canada does not provide incentives for participation.
The sample for analyses in the present study included individuals aged 15 to 60 years with complete data on study variables (n = 43,466; 97.5% of the sample). We did not include individuals over 60 years of age (n = 17,458) due to low prevalence of cannabis use (∼1% used at least once a month). All variables of interest were explored with minimal missingness for each variable: year, age, and sex (0%); suicidal ideation (0.1%); MDE (0.4%); cannabis (1.4%); chronic alcohol (0.2%); heavy drinking (0.4%); and other illicit drug use (0.4%). Cases were dummy coded where a complete case was coded “0” and an incomplete case (i.e., missing data on 1 or more variables) was coded “1,” and this dummy variable was regressed individually on each variable in the model to determine if model variables were meaningfully related to missingness. Individuals with missing data (n = 1173) were more likely to be male, report lower household income, be an emerging adult (15-24 years of age), engage in heavy drinking, use other illicit drugs, report suicidal ideation or attempts, and experience depression compared to those with complete data.
Measures
The surveys were developed in collaboration with Health Canada and the Public Health Agency of Canada, the Provincial Health Ministries, the Mental Health Commission of Canada, and academic experts and underwent pilot qualitative and quantitative testing. 17,18 Standard Statistics Canada procedures were used to minimize nonresponse of items.
Cannabis use
Response options to frequency of cannabis use in the past 12 months include never, less than once a month, 1 to 3 times a month, once a week, more than once a week, or every day. Preliminary analyses examining associations between frequency of cannabis use and depression, suicide, and psychological distress revealed overlapping confidence intervals (CIs) for use equal to or greater than monthly, and therefore, responses were collapsed into at least monthly (coded as 1) and less than monthly (coded as 0). It is important to note that both surveys were collected during the implementation of the Medical Marijuana Access Regulations allowing for people with certain conditions to obtain authorization to use cannabis for medical purposes. In the CCHS 1.2 (2002), participants were asked about their cannabis use without specifying if it was used for medical or nonmedical purposes, while in the CCHS-MH (2012), individuals were asked about nonmedical use. However, in 2003, only 605 Canadians were authorized for medical cannabis use; therefore, this difference in the operationalization of cannabis use does not pose a threat to validity of the analysis exploring associations with nonmedical cannabis use.
Suicidal ideation
The question was as follows: Have you thought about committing suicide or taking your own life? This question was worded slightly differently if the respondent entered the depression module. Statistics Canada collapsed multiple items to create variables for past 12-month suicidal ideation. In 2002, there was an error in the skip pattern, and not all respondents were asked suicide-related questions, and an imputation strategy was derived to assign values for 12-month thoughts. The Statistics Canada derived and imputed variables were used in this study. Individuals endorsing suicidal ideation in the past 12 months were coded as 1, and those who did not were coded as 0.
Major depressive episode
A Canadian adaptation of the World Health Organization World Mental Health Composite International Diagnostic Interview (WHO WMH CIDI, 2017) was used to assess past-year DSM-IV major depressive episode (MDE). This is a well-established measure, commonly used in epidemiological studies, with moderate concordance with the Structured Clinical Interview for the Diagnostic Statistical Manual (SCID). 19 Individuals meeting criteria for MDE were coded as 1, and those not meeting criteria were coded as 0.
Other substance use
Other substances were also accounted for, including a) chronic alcohol consumption, coded as 1 (drinking more than 12 drinks per week) and 0 (less than or equal to 12 drinks per week); b) frequency of heavy drinking (i.e., drinking 5 drinks or more on one occasion), from 0 (never) to 5 (more than once per week); and c) other illicit substance use, coded as 1 (use of any other illicit substance(s) in the past 12 months) and 0 (no use in the past 12 months).
Sociodemographic covariates
Other variables include year of data collection (0 = 2002, 1 = 2012), biological sex (0 = male, 1 = female), and developmental age group (0 = middle-aged adults ages 25-60, 1 = emerging adults ages 15-24). Age was captured dichotomously as the brain is not fully developed until approximately 25 years of age and THC may disrupt normal neuronal development. 20 –22 In addition, the prevalence of cannabis use is much higher among emerging adults than any other age group. 23
Statistical Analyses
All analyses were performed in SAS software version 9.4 (SAS Institute, Cary, NC) using survey weights and replicate bootstrap weights. Survey weights were normalised prior to analysis. Descriptive statistics (means and percentages) are provided for the samples stratified by year.
A series of binary logistic regression analyses were performed for suicidal ideation and MDE. Model 1 included developmental age, sex, cannabis use, year, and the interaction term between cannabis use and year. In the second set of models, interaction terms between cannabis use and biological sex (model 2A) and developmental age (model 2B) were added to the model. Significant interactions were retained and carried forward to a fully adjusted model, including alcohol (chronic and heavy use) and illicit drug use as covariates, to determine the independent effect of cannabis use over and above other substances (model 3). Clinically significant effect sizes were determined a priori: odds ratios (ORs) of 1.5 were considered clinically meaningful differences based on a Cohen of ∼0.2 24 and previous meta-analyses of cannabis use and mental health outcomes, which used an OR of 1.5 as the cutoff for clinically meaningful effects. 25,26
Results
Descriptive Statistics
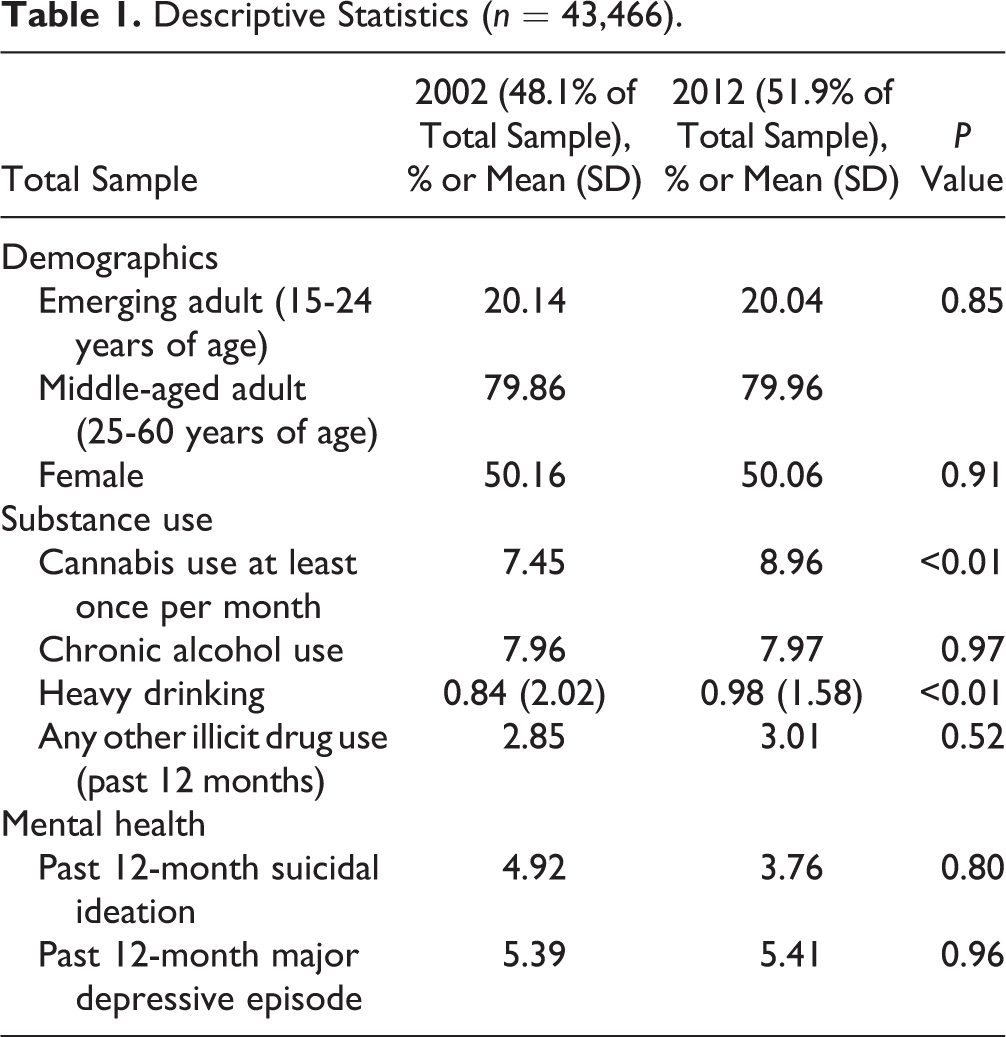
About 50% of both samples identified as female, and 20% were emerging adults. In 2002, 7.45% reported using cannabis at least once per month, 4.92% reported suicidal ideation in the past 12 months, and 5.39% met criteria for MDE in the past 12 months. In 2012, 8.96% reported using cannabis at least once per month, 3.76% reported suicidal ideation, and 5.41% met criteria for MDE (Table 1).
Descriptive Statistics (n = 43,466).
At Least Monthly Cannabis Use by Year
Table 2 presents ORs and associated 95% CIs from binary logistic regression models examining the association between at least monthly cannabis use and a) suicidal ideation and b) MDE. The odds of endorsing suicidal ideation were lower in 2012 compared to 2002. In model 1, adjusted for developmental age and biological sex, the association between cannabis use and suicidal ideation was stronger in 2012 compared to 2002 (OR, 1.59; 95% CI, 1.11 to 2.27). For individuals who used cannabis at least monthly in 2002, the odds of reporting suicidal ideation were 2.24 (95% CI, 1.82 to 2.76), while in 2012, the odds of suicidal ideation were 3.56 (95% CI, 2.49 to 5.08) (see online supplementary materials for interaction calculations). In 2002 and 2012, cannabis use was associated with clinically meaningful effects for suicidal ideation (i.e., OR and associated 95% CI >1.5).
Strength of the Association between Cannabis Use and Past 12-Month Suicidal Ideation and Major Depressive Episode.
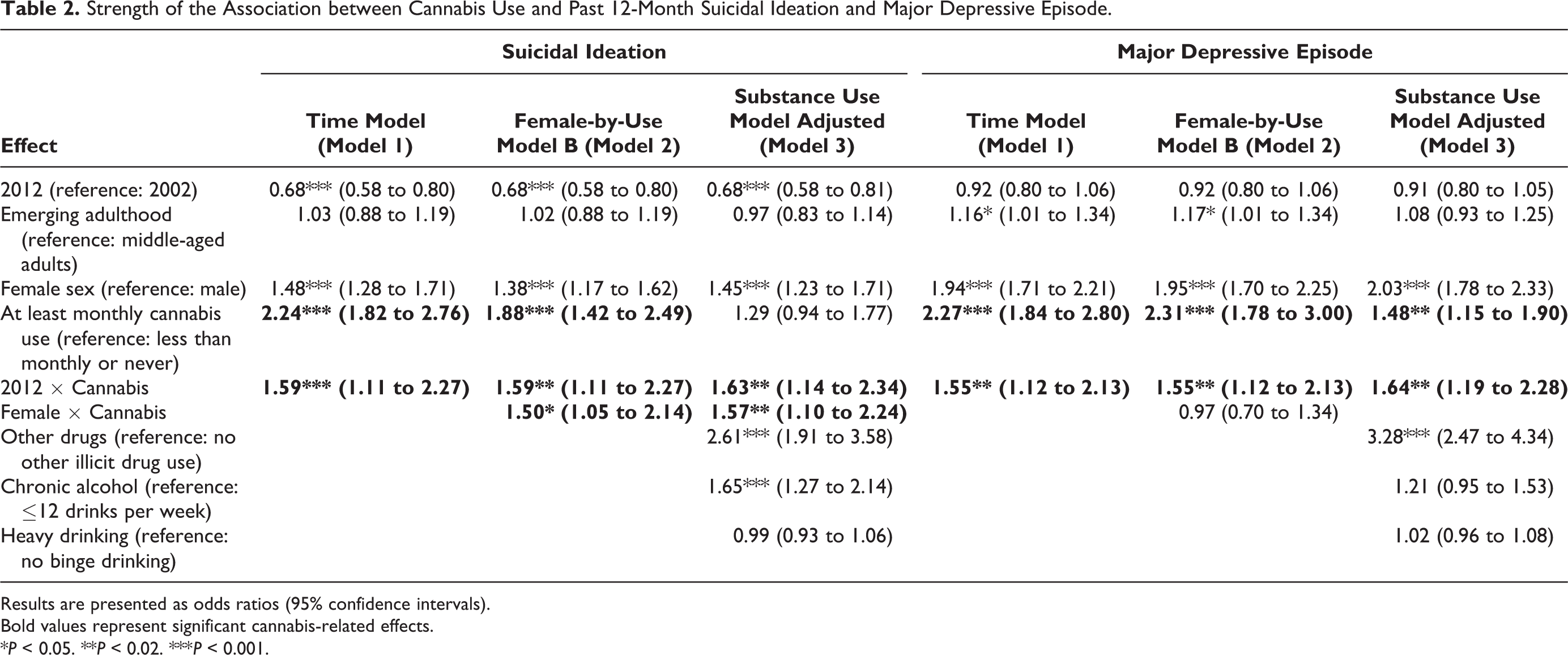
Results are presented as odds ratios (95% confidence intervals).
Bold values represent significant cannabis-related effects.
*P < 0.05. **P < 0.02. ***P < 0.001.
In the second series of models, the female sex-by-use interaction was significant (OR, 1.50), but the developmental age-by-use interaction was not significant for suicidal ideation. The main effect for at least monthly use of cannabis and the interaction term between monthly cannabis use and year remained statistically significant in model 2. Furthermore, a 3-way interaction term was examined between female sex-by-use-by-year, which was not significant. Therefore, females who used cannabis at least once a month were more likely to report suicidal ideation than males who used cannabis overall. The interaction term between monthly cannabis use and year remained statistically significant after adjusting for chronic and heavy alcohol use and other illicit drug use. After adjusting for other substance use, there was a reduction in the main effect of cannabis, but the magnitude of the interaction effect with year and sex remained relatively similar (see online supplementary materials for additional model results).
The patterns of results for MDE were similar to those for suicidal ideation, although no sex-by-use effects were found. There was no difference in the likelihood of MDE between 2002 and 2012 across all models. In model 1, there was a stronger association between at least monthly cannabis use and MDE in 2012 compared to 2002 (OR, 1.55; 95% CI, 1.12 to 2.13). For individuals who used cannabis at least monthly in 2002, the odds of experiencing MDE were 2.27 (95% CI, 1.84 to 2.80), while in 2012, the odds of MDE were 3.51 (95% CI, 2.75 to 4.48). These effects were also clinically meaningful. There were no significant interactions between sex-by-use or developmental age-by-use for MDE. The 2-way cannabis use-by-year effects remained after adjusting for other substance use in model 3.
Interpretation
Brief summary
Using a nationally representative sample of Canadians aged 15 to 60 years, at least monthly cannabis use was consistently associated with an increased odds of suicidal ideation and MDE. The association between cannabis use and each of these outcomes was stronger in 2012 compared to 2002. The temporal change in the strength of association between cannabis use and suicidal ideation and depression adds novel insights to the existing literature. Although not the primary objective of this analysis, there were many consistencies between this study and preexisting evidence. Similar to previous studies, rates of MDE remained similar over time, 27 while suicide-related outcomes decreased among middle-aged Canadian adults 28 but increased for younger Canadians. 29 We also found a consistent association between cannabis use and suicidal ideation and MDE that remained over and above other substance use. 3,4 In addition, females who used cannabis at least once a month were more likely to report co-occurring suicidal ideation, which has been found in previous studies (see Halladay et al. 30 ). Since exploring temporal changes in the association between cannabis and suicidal ideation and depression is novel, the cannabis use-by-year effects cannot be directly compared to existing evidence.
There are several plausible explanations for the increased strength of the association between cannabis use and depression and suicidal ideation between 2002 and 2012, particularly changes in the composition of cannabis and perceptions of use over time. Firstly, the potency of cannabis has been increasing over time, 12 –14 and previous research has demonstrated that higher levels of THC are associated with poorer mental health outcomes, especially when paired with low CBD. 31 –36 Alternatively, more individuals with preexisting depression or suicidal ideation may have been using nonmedical cannabis to cope with their symptoms in 2012 compared to 2002. Despite an absence of established evidence of therapeutic benefit for mental health concerns, 37,38 the perceived risk of using cannabis has decreased over time, 39 and about 50% of Canadians who use cannabis believe cannabis benefits their psychological well-being. 40 Although the data for this article focused on nonmedical use, there has been an increase in medical use of cannabis over time, with about 342,000 registrants in September 2018. 41 However, the cross-sectional nature of this study inhibits our ability to know what is driving the observed increased association over time.
Limitations
Due to the cross-sectional nature of the surveys, causality cannot be inferred, and therefore, the analyses focused on prevalence and temporal change in the strength of association between cannabis use and depression and suicidal ideation between 2 time points only. It is possible that there were fluctuations in the magnitude of the associations between cannabis use and internalizing disorders, rather than a consistent increase over time, between 2002 and 2012. While the present study adjusted for the most commonly cited confounding variables such as other substance use, developmental age and sex, other confounding variables that were not accounted for in this analysis (e.g., chronic pain) may result in a spurious association between cannabis use and depression and suicidal ideation. Also, cannabis and suicidal ideation were captured by single-item questions, which may affect the quality of reporting. However, large epidemiological studies regularly rely on single-item measures. For substance use outcomes, single-item questions have demonstrated acceptable sensitivity and specificity with structured interviews. 42 For suicide-related outcomes, in a large meta-analysis of risk factors for suicidal ideation and behaviours, the assessment approach (i.e., single item versus structured interview) did not moderate the effect size. 43 In addition, all data were captured through self-report measures, which are prone to recall and social desirability bias. Regarding cannabis use, respondents may have underreported, especially given nonmedical use was illegal during data collection 44 ; however, social acceptance of cannabis has increased over time, 7 –10 and this may have influenced how respondents reported. The direction and magnitude of self-reporting biases for substance use also differ depending on age and ethnicity. 44 It is also important to note that cannabis frequency items did not capture age of onset, previous substance use problems, composition of cannabis used, frequency of daily use, quantity of cannabis used, added tobacco, or method of delivery of cannabis product. Therefore, our operationalization of cannabis use refers to frequency of nonmedical use in general.
Conclusion and Future Directions in the Area of the Study
Our findings suggest that cannabis use and suicidal ideation and depression were more likely to co-occur in 2012 compared to 2002. Existing practice guidelines suggest that if an individual is presenting with either symptoms of depression or substance use, clinicians should be assessing, monitoring, and treating concurrent depression and substance use problems at all phases of diagnosis, treatment, and monitoring 45 –47 ; that is, if a patient presents with cannabis use, this should alert the clinician or nurse to conduct a more in-depth assessment of potential co-occurring depression and suicide risk. Although research on treatment of concurrent disorders is limited, it is also important to note that cognitive behavioural therapy is indicated for the treatment of both depression and cannabis-related problems and may therefore be an ideal treatment option for individuals presenting with both problems until further research is available. 45,46,48,49 In addition, there is an urgent need to differentiate nonmedical from medical use of cannabis. There are salient differences in the composition, delivery, and uses of medical compared to nonmedical cannabis (i.e., THC/CBD ratios), which may influence the association with depression, suicidal ideation, and practice recommendations.
Future research
The changes in the social and political landscape of substance use in Canada will likely result in different patterns of behaviours among groups trying and using cannabis. This study provides needed baseline evidence, which will allow future evaluation of the impact of legalization on associations between cannabis use and suicidal ideation and depression. Population surveys addressing both cannabis use and suicidal ideation and depression should be repeated early in the course of nonmedical cannabis legalization and several years later, in order to allow comparison to this study, which addressed early and later stages of medical cannabis legalization in the Canadian population. Future studies should collect more information regarding the composition of cannabis consumed and patterns of use (i.e., frequency and quantity, age of initiation, method of delivery, motives). Ensuring that measures of mental health and substances other than cannabis are measured in future epidemiologic studies of cannabis will be important. Longitudinal studies are needed to further elucidate the sequencing and causal mechanisms of comorbid substance use and mental health problems.
Conclusion
In conclusion, at least monthly cannabis use was consistently related to both suicidal ideation and depression, and these associations were stronger in 2012 compared to 2002. The findings of this study provide a baseline for the associations between cannabis use and suicidal ideation and depression in the Canadian population that should be evaluated again after nonmedical cannabis legalization.
Supplemental Material
Supplemental Material, Temporal_Change_Cannabis_Supp1 - Temporal Changes in the Cross-Sectional Associations between Cannabis Use, Suicidal Ideation, and Depression in a Nationally Representative Sample of Canadian Adults in 2012 Compared to 2002
Supplemental Material, Temporal_Change_Cannabis_Supp1 for Temporal Changes in the Cross-Sectional Associations between Cannabis Use, Suicidal Ideation, and Depression in a Nationally Representative Sample of Canadian Adults in 2012 Compared to 2002 by Jillian E. Halladay, Catharine Munn, Michael Boyle, Susan M. Jack and Katholiki Georgiades in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, Temporal_Change_Cannabis_Supp2 - Temporal Changes in the Cross-Sectional Associations between Cannabis Use, Suicidal Ideation, and Depression in a Nationally Representative Sample of Canadian Adults in 2012 Compared to 2002
Supplemental Material, Temporal_Change_Cannabis_Supp2 for Temporal Changes in the Cross-Sectional Associations between Cannabis Use, Suicidal Ideation, and Depression in a Nationally Representative Sample of Canadian Adults in 2012 Compared to 2002 by Jillian E. Halladay, Catharine Munn, Michael Boyle, Susan M. Jack and Katholiki Georgiades in The Canadian Journal of Psychiatry
Footnotes
Data Access
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ms. Jillian Halladay is supported by a CIHR Doctoral Research Training Award. Dr. Georgiades holds the David R. (Dan) Offord Chair in Child Studies.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.