
Abstract

The introduction of bipolar II disorder as a classificatory concept approximately 4 decades ago was an understandable and pragmatic solution to the clinical problem at the time. However, its persistence to the present day is puzzling and a pressing cause for concern.
When reviewing patient data from hospitalizations at the National Institute of Mental Health (NIMH) in 1960, it became apparent that there were 3 groups of patients with mood disorder histories: the first comprised patients who had experienced only depression, the second consisted of those who had been hospitalized for both manic and depressive episodes, and a third group constituted patients who had been hospitalized predominantly for depressive episodes but had also experienced subthreshold manic symptoms (i.e., hypomania) on occasion. 1 The first 2 groups were already recognized in third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III) 2 —as unipolar (major) depressive disorder and bipolar disorder, respectively—but the third group was not. Hence, bipolar II was devised to capture this “in-between” set of patients.
Patients with symptoms similar to bipolar II were classified under the broad diagnostic label of “atypical bipolar disorder” until the publication of the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) in 1994, when bipolar II was introduced as a formal diagnostic label. 3 The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published in 2013, made minimal revisions, and thus bipolar II remains defined by the occurrence of depressive and hypomanic episodes. 4 In the DSM-5, hypomania differs from mania in that it lasts for at least 4 days but less than 7 days (the latter marking the transition to mania) and, by definition, is not severe enough to cause marked functional impairment or hospitalization and does not feature psychotic symptoms. Similarly, the new International Classification of Diseases, 11th Revision (ICD-11) differentiates hypomania from mania on the basis of 7 days’ duration but, somewhat puzzlingly, sets the lower limit for hypomania at “several” days 5 (see Figure 1A).
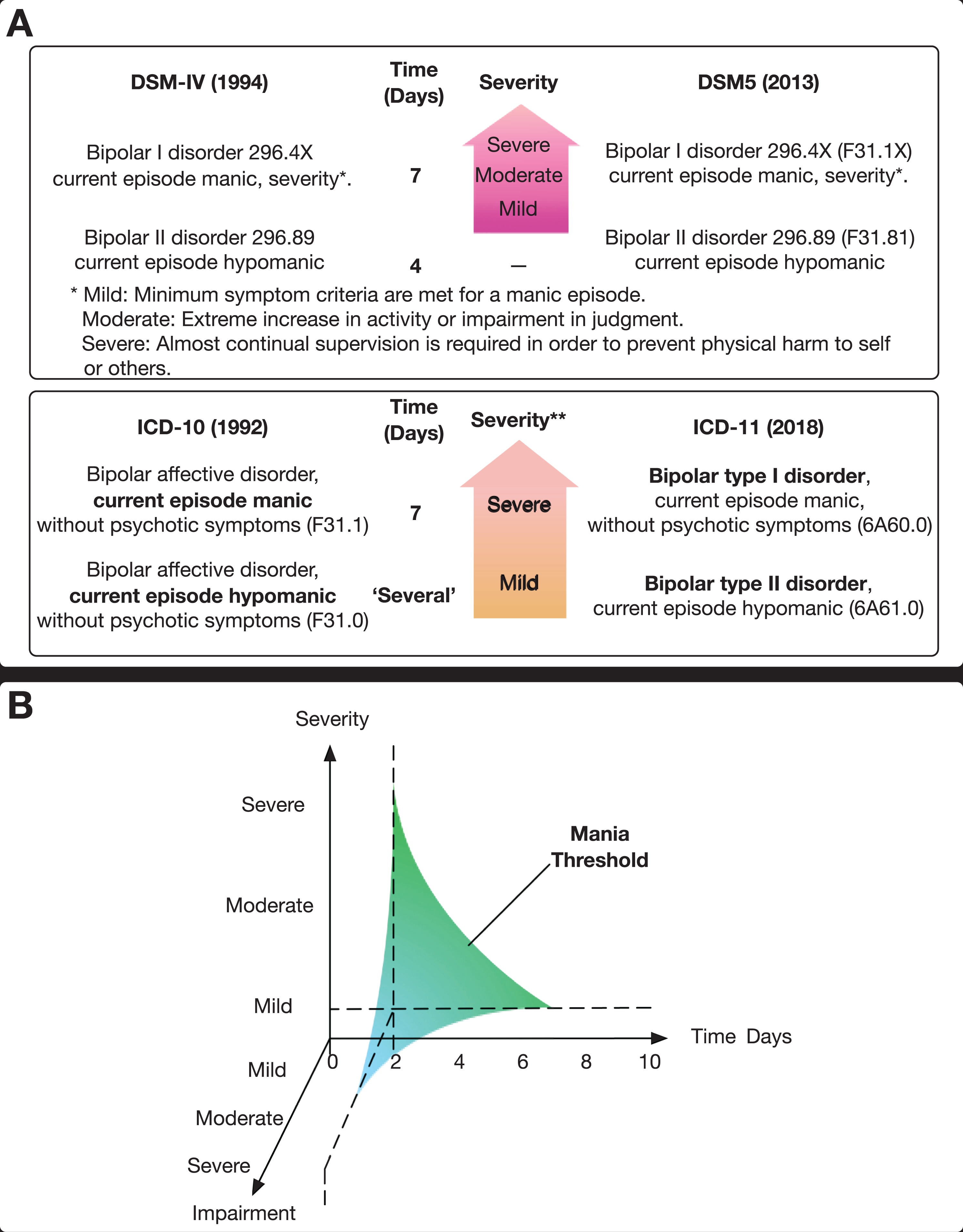
(A) Bipolar II disorder definitions in the International Classification of Diseases (ICD) and Diagnostic and Statistical Manual of Mental Disorders (DSM). This figure shows the criteria used to define bipolar II disorder in both major classificatory systems. Specifically, it illustrates the changes that have occurred from DSM-IV to DSM-5 and the proposed changes in ICD-11 as compared to the existing definitions in ICD-10. It also highlights the differences between the 2 taxonomies and the emphasis placed on duration of symptoms. It is noteworthy that, whilst both classification systems have adhered to an upper cutoff of 7 days to distinguish hypomania from mania, the lower cutoff, although somewhat arbitrary in the DSM-5 (4 days), is nevertheless specified as compared to the ICD-10 and ICD-11, which employ the rather vague descriptor of “several.” (B) Multidimensional threshold for mania. In addition to duration and severity, this figure illustrates the need to consider impairment as a separate dimension that contributes independently to the definition of mania and thereby the diagnosis and treatment of bipolar disorder. It is important to note that impairment cannot be inferred from either the duration of symptoms or the severity of the syndrome. Instead, it is an independent judgement of the degree to which functioning is compromised across domains such as work and relationships. Furthermore, whilst there is a duration cutoff (2 days) and whilst severity also has a lower boundary (bounded by “mild”), impairment is best regarded as a categorical state, such that either the individual is impaired or not. If the individual is impaired, then the degree of impairment can be judged to inform clinical decision-making, again making use of both categorical and dimensional assessment techniques.
At the time bipolar II was conceived, it made sense. It was increasingly apparent that there was more than just classic manic-depressive illness in the real world and that a careful reexamination of classification was needed. Indeed, some researchers went as far as proposing the introduction of 6 subtypes of bipolar disorder, 6 although the dichotomization of bipolar disorder is what has endured. The introduction of bipolar II disorder forced acknowledgement of the fact that bipolar disorder was a heterogeneous illness and encouraged closer examination of the various clinical manifestations of bipolarity. Arguably, the popularity of bipolar II has heralded a deeper understanding of the importance of depressive episodes in bipolar disorder as a whole, and we now have evidence that shows depressive episodes confer the most impairment on those with any form of bipolar disorder. 7 However, despite the benefits of having shone a spotlight on bipolar disorders, we feel that the concept of bipolar II has run its course and served its purpose, and research has failed to demonstrate that a distinct bipolar II subtype exists. Hence, we argue that the term should now be refined and removed from our lexicon.
Seeking Definition
As is the case with most psychiatric disorders, the absence of pathognomonic symptomatology means that the definition of bipolar II is contingent on defining its syndromic boundaries. For bipolar II disorder, these boundaries are poorly defined and do not reflect any true clinical or biological distinction, making it difficult to differentiate it from bipolar I and other psychiatric disorders and, indeed, from normalcy itself. 8,9 One such defining characteristic is the 4-day cutoff that is used to determine a diagnosis of hypomania—this boundary was chosen wholly arbitrarily, and the decision was guided mostly by concerns about overdiagnosis. 10 Notably, the upper limit of 7 days is equally subjective and lacks any psychological or biological basis. Concerning the lower boundary of 4 days, the DSM-5 initially considered lowering the number of days needed to qualify for hypomania but instead decided to introduce additional bipolar subtypes—including “short-duration” hypomania to bridge the gap from 2 to 4 days of manic symptoms. This move went against research studies and clinical experience that suggest mania can be reliably differentiated from “normal” bouts of sleep deprivation or drug-induced periods of high energy by employing a robust duration criterion of 2 days. 11,12
According to the DSM-5, the duration of symptoms is important when defining a disorder for classificatory purposes and for making a diagnosis in clinical practice, but at any time, factors related to severity can override those pertaining to duration. That is, the presence of psychotic symptoms, irrespective of the duration of other symptoms, automatically transforms an episode into mania. Remarkably, and somewhat bafflingly, hospitalization does the same—even though it is an extremely unreliable proxy of severity. 13
Beyond the criteria of duration and severity, there are little to no phenomenological, biological, or treatment factors that separate bipolar II as a disease entity from bipolar I. 14 On the other hand, the illogical definition of hypomania veers worryingly close to a nonclinical or nonharmful elevation of mood and energy. The DSM-5 criteria for hypomania state that the symptoms do not “cause marked impairment” and, indeed, a significant proportion of individuals with bipolar II do not engage in risky behaviours that are typical of classic mania. Instead, they report that they enjoy their brief periods of hypomania and associated increases in productivity or creativity. 15,16 This prompts the question of whether it is phenomenologically accurate and ethically appropriate to pathologize these periods. We argue that while such periods may serve as important clinical indicators when it comes to making decisions in the treatment of subsequent depressive episodes, the prescription of potentially harmful medication to counter brief periods of elevated mood, subjectively described as enjoyable and gainful, does not seem rational.
The difficulty in reliably diagnosing bipolar II is especially apparent when considering other psychiatric disorders that share (or at least appear to) some of its putative characteristics. For instance, bipolar II overlaps considerably with borderline personality disorder, and indeed, the two are frequently mistaken. 17,18 This opens the door to treatments that are unlikely to benefit the individual, such that they may be exposed unnecessarily to antidepressants, anticonvulsants, and antipsychotics. Some of these medications may even exacerbate the underlying illness or generate symptoms that give the impression of manic or depressive symptoms; for example, the triggering of manic symptoms by antidepressants 19 or the dulling and dampening of mood and energy by some antipsychotics. 20
The other major problem of inaccurately diagnosing individuals as having bipolar II is that they are effectively treading water as they wait to commence appropriate treatment. The delay that occurs before a correct diagnosis is made and the appropriate treatment is commenced is a significant loss. In instances when, instead of a manic process, the genuine aetiology of the individual’s symptoms is a personality disorder or substance misuse, successful treatment of these problems clearly requires different sets of interventions, which are also likely to have greater success the sooner they are administered. 21
The fuzziness of bipolar II boundaries has facilitated the expansion of the diagnosis and arguably provided a window of opportunity for pharmaceutical companies. Since the introduction of bipolar II in the DSM-IV, pharmaceutical companies have engaged assiduously in “education” and marketing strategies to promote the idea that it is more harmful to miss a diagnosis of bipolar II than it is to overdiagnose individuals without the illness. 10,22,23 This has contributed to the dramatic increase in the rate of bipolar diagnoses seen in the United States—up by as much as 50% in adults from 1996 to 2004 and more than quadrupling in children and adolescents over the same period. 24 Similarly, prescriptions of antipsychotics used in the treatment of bipolar disorders have continued to rise. For example, the prescription of quetiapine by general practitioners tripled between 2005 and 2012 in Canada. 25
In addition to concerns about the inaccurate diagnosis of bipolar II, there are also questions about its theoretical value. Studies examining bipolar II disorder over recent decades have failed to advance our understanding of the mechanisms involved in bipolar disorders. Instead, the diagnosis has focused attention on trying to find evidence that it really is distinct from bipolar I, an endeavour that has clearly failed. That is, studies have consistently been unable to identify any factors that reliably differ more than would be expected when examining 2 points on the same spectrum. 14 Indeed, a recent population study in Sweden found specific familial aggregation of bipolar I versus bipolar II diagnoses, suggesting that the subtypes differ in their aetiologies. However, they also demonstrated substantial genetic correlation between the 2 diagnoses, 26 meaning that they are not completely different entities. Taken together, these findings are in keeping with the hypothesis that bipolar severity aggregates in families, which is consistent with a dimensional model of bipolar disorders. Furthermore, when interrogating neurocognition 27,28 and using neuroimaging, 29 no reliable differentiation has been possible—hence why treatment specificity is also not apparent, with the same medications being used across the whole spectrum of bipolar disorders.
Nonetheless, supporters of the bipolar II diagnosis often draw on treatment specificity to support distinction of the disorder. Lamotrigine, for example, is said to have a specific and more pronounced antidepressant effect in the treatment of bipolar II than bipolar I. However, there are 2 problems with this assertion—first, there is scant evidence, if any, to support this supposition. 30 Second, the DSM-5 and ICD-11 definitions of bipolar II disorder include many patients who do not respond to lamotrigine. Just as lithium responsivity does not overlap perfectly with those diagnosed with bipolar I disorder, lamotrigine responsivity is prevalent in only a subset of bipolar II cases. If there were evidence that depression responds preferentially to lamotrigine when a patient has a history of hypomanic versus manic episodes, all this would demonstrate is that some depressive permutations are lamotrigine responsive—it would not justify the use of DSM-5 or ICD-11 bipolar II diagnostic labels.
Thus, bipolar II may have made sense when it was introduced, but it is now clear that it does not meaningfully inform clinical management and that adhering to the concept is hindering progress in advancing our understanding of the pathogenesis of bipolar disorder. Ultimately, arbitrarily separating bipolar disorders into bipolar I, II, and “unspecified” to capture the heterogeneity of the illness has proven to be of little use.
A New Dimension
A dimensional approach better captures the heterogeneity of bipolar disorders, an idea that has been espoused for years by experts in the field of mood disorders, 31,32 and nowadays even some proponents of bipolar II regard it as a stopping point along a spectrum of bipolar illness. 33 From a practical standpoint, implementing a dimensional diagnostic system simply involves using information that is already collected as part of routine practice. That is, we already quantify the number of days of mania to determine whether someone has bipolar II or bipolar I (although, in practice, this is often executed poorly). We could easily proceed one step further and simply specify the number of days of mania rather than forcibly applying artificial categories defined by arbitrary criteria. This would change little in terms of psychiatric and phenomenological enquiry and time spent gathering information from patients but would enhance specificity enormously.
This approach would mean that, rather than stating someone has bipolar I disorder or bipolar II disorder and defining their episodes as mania and hypomania, we could simply state the precise duration of manic symptoms in each case. For example, “the patient had 6 days of manic symptoms that severely impaired functioning.” However, this is not to say that categories are not needed at all. Some cutoffs, be they pragmatic or actual, are necessary in clinical practice and can be useful, since it is difficult and perhaps less meaningful to talk of how much of a disease one has when it has not even been established whether there is an illness in the first place.
Duration Criteria
For years, leading experts on bipolar disorders (e.g., Angst, Akiskal, Benazzi) and their colleagues have performed extensive diagnostic category validation studies that have demonstrated that a lower cutoff of 1 to 3 days meaningfully separates “normal” experiences of manic symptoms from those that are likely to be due to an underlying illness, 11,31,34,35 and in practice, this is most usefully captured by a 2-day threshold 12 (Figure 1B). This also has pragmatic value as it is not uncommon for people to have poor sleep for at least 1 night and possibly even 2, or for the need for sleep to be diminished because of substances that they may have ingested, the concomitants of which are also increased energy, drive, and feelings of euphoria. Experiences that are substance induced or have been caused by sleep deprivation are best not confused with mania per se, and so a lower limit of 2 days can be used universally to separate such symptom patterns from those that require further evaluation.
This system also means that an upper limit is not necessary (Figure 1B). A loss of interest in the pattern of illness and duration of mania after the number exceeds 7 days has meant that the dimensional aspects of the underlying illness have been overlooked, and both short- and longer-term patterns of mania are still poorly understood. For example, it is not known whether there is any meaningful prognostic difference between having mania for 5 days versus 5 weeks or whether the characteristics of manic symptoms when occurring in shorter epochs of 2 to 4 days are different from when mania is sustained for a longer period. These considerations are important as they likely reflect the underlying nature of the illness and may indeed hold the key to understanding the pathophysiology of mood disorders.
Severity and Impairment Criteria
In addition to the duration of symptoms, the severity of the syndrome is equally important and can be rated broadly as mild, moderate, or severe or more specifically using rating scales, such as those often employed in clinical trials. This would provide a gauge of the intensity of symptoms and the nature of the illness. Current taxonomies do not insist on such specificity, but worse still, the severity of the illness is conflated with its impairment. The latter is a critical dimension, and so once again, we advocate that this be evaluated separately (see Figure 1B).
Impairment concerns the effect the illness has on the individual in terms of functioning. In essence, it is the impact the illness has on aspects of their life such as work, their relationships, and their ability to engage in activities and execute their responsibilities. Functional impairment may coincide with severity and even duration of illness, but there will be instances when the impairment is tremendous but the symptoms themselves may not be severe. For example, even mild cognitive compromise (inattention, memory loss) would be devastating for an airline pilot. Hence, while it is possible to diagnose mania without considering impairment, we advocate that impairment be given separate deliberation and be weighted accordingly when determining whether a threshold has been reached for the purposes of treating mania.
Conclusion
It is time for psychiatry to explore new ideas. By continuing to regard bipolar II as a valid or useful diagnosis, we have inadvertently reified its status as a disease entity, despite there being little evidence to support its validity as a distinct syndrome, let alone an illness underpinned by a unique pathological process. Therefore, it is important for classification systems to examine the evidence and revise diagnoses, rather than hold on to an inaccurate diagnosis for fear of what changing it will bring. Hence, we propose the abandonment of bipolar I and bipolar II as diagnostic categories and suggest an evidence-based and pragmatic dimensional approach to the diagnosis of mania within the single disorder entity of “bipolar disorder.” It is important that science has the loudest voice, not economic or pragmatic concerns alone.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GSM has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, and Servier; has been a speaker for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka, and Servier; and has been a consultant for AstraZeneca, Janssen Cilag, Lundbeck, Otsuka, and Servier. TO and LI have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.