
Abstract
Objective:
Mental health recovery narratives are often shared in peer support work and antistigma campaigns. Internet technology provides access to an almost unlimited number of narratives, and yet little is known about how they affect recipients. The aim of this study was to develop a conceptual framework characterizing the impact of recovery narratives on recipients.
Method:
A systematic review of evidence about the impact of mental health recovery narratives was conducted. Searches used electronic databases (n = 9), reference tracking, hand-searching of selected journals (n = 2), grey literature searching, and expert consultation (n = 7). A conceptual framework was generated through a thematic analysis of included articles, augmented by consultation with a Lived Experience Advisory Panel.
Results:
In total, 8137 articles were screened. Five articles were included. Forms of impact were connectedness, understanding of recovery, reduction in stigma, validation of personal experience, affective responses, and behavioural responses. Impact was moderated by characteristics of the recipient, context, and narrative. Increases in eating disorder behaviours were identified as a harmful response specific to recipients with eating disorders.
Conclusions:
Mental health recovery narratives can promote recovery. Recovery narratives might be useful for clients with limited access to peers and in online interventions targeted at reducing social isolation in rural or remote locations, but support is needed for the processing of the strong emotions that can arise. Caution is needed for use with specific clinical populations. Protocol registration: Prospero-CRD42018090923.
Mental health recovery narratives are first-person accounts of recovery from mental health problems that refer to events or actions over a period of time. 1 They are referred to as recovery narratives throughout the remainder of this article whilst recognising that this term is used elsewhere in health care research and practice (e.g., in narratives of recovery poststroke). 2
Recovery narratives can be live (given in the context of a real-world or online relationship) or recorded (presented in invariant text, video, or audio). Live recovery narratives feature in peer work, where professional training typically encourages the selective disclosure of personal experiences, as part of an ongoing relationship with a client. A US national survey has identified helping others through the narrating of recovery narratives as a feature of the work of peer specialists, 3 and Davidson et al. 4 have argued that the disclosure by a peer worker of their own transition to a “hero of their own self-journey” (p. 124) can instil hope in others.
Substantial numbers of recovery narratives are publicly available, distributed through books, 5,6 online collections, 7 and digital media hosting services. 8 Creating narratives can provide benefits for narrators, 9 who might be motivated by sending messages of “hope, courage and survival” (p. 68), 10 a form of indirect emotional support provision. 11 Campaigns that aim to reduce stigma, 12,13 such as Bell Let’s Talk, 14 have used recorded recovery narratives 15 as a mechanism for creating social contact 16,17 between people with experience of mental health problems and others. Narratives used for antistigma purposes can also have a beneficial impact on help-seeking behaviour, 18 and organizations such as Here to Help 19 and the Scottish Recovery Network 20 have created online collections with the explicit intent of supporting recovery in recipients. These might be seen as specific initiatives within a larger effort to incorporate information and communication technologies into mental health practice, motivated by challenges such as limited access to in-person mental health treatment in rural 21,22 and First Nations 23 communities and for people with social anxiety disorders. 24
Despite widespread interest, a knowledge gap exists about how live and recorded recovery narratives make an impact. No systematic review has been conducted on this topic. A realist review considered the broader question of how sharing experiences of health conditions on the Internet might affect the health of those sharing and receiving material; it identified mechanisms such as 1) the recipient finding useful information in the experiences of others with similar health difficulties or 2) feeling supported through an understanding that others have encountered and overcome related challenges. 25 This review drew on a range of empirical and nonempirical sources. Its authors note a need to strengthen the scientific evidence base, given an “explosion of web resources that feature experiences posted by patients themselves” (p. 219). The authors note that receiving experiences had the potential for positive and negative impact.
Other studies have identified specific harms that can be associated with receiving online health material, especially in the case of conditions that are isolating or stigmatised. 26 Examples include “pro-ana” websites, which enable online interperson interaction that sustains anorexic behaviours and beliefs. 26 An experimental study of 235 female undergraduates showed that viewing a proanorexia website increased negative affect and lowered social self-esteem relative to a comparison website. 27 A qualitative study demonstrated that proanorexia sites can sustain anorexic behaviour by enabling the sharing of hints and tips. 28 Neither study was specific to narratives but included websites using narrative material.
Mental health recovery narratives are becoming more widely available, so an evidence-based understanding of how they make an impact on recipients is needed, especially given known harms associated with online health material. The aim of this review was to develop a conceptual framework characterizing the impact of live or recorded recovery narratives on recipients.
Method
A systematic review of documents providing empirical evidence for the impact of recovery narratives on recipients was conducted. The systematic review protocol was registered at http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018090923.
Recovery narratives were defined as first-person nonfiction accounts of recovery from mental health problems, including 1) elements of adversity/struggle and 2) self-defined strengths/successes/survival, and which 3) refer to events or actions over a period of time. 1 “Receiving a narrative” was defined as viewing, reading, or listening to someone else’s recovery narrative. Impact was defined as the processes by which receiving recovery narratives causes benefits or harms to the recipient and the outcomes generated by these.
Inclusion criteria: 1) presents empirical research, with at least 5 participants as recipients of recovery narratives; 2) presents evidence relating to the impact of recovery narratives on participants, including evidence of no impact; 3) draws on nonfictional narratives with a clear mental health and recovery component; and 4) the full text of the publication was available in English.
Exclusion criteria: 1) narratives were told second-hand (e.g., by a health care professional or carer) and 2) narratives were a component of a complex intervention and it was not clear whether the impact was due to the narrative or to other components of the intervention. The latter was included due to scoping searches locating studies in which recovery narratives were just one part of a multicomponent intervention evaluated as a whole and where the impact of individual components could not be disambiguated. An example was a 2-component antistigma campaign 29 that used recovery narratives and educational workshops.
Search Strategy
Electronic databases
Research into recovery narratives is multidisciplinary, and hence searches were conducted across a broad range of publication databases. Selection was informed by scoping searches. Selected databases were AMED, EMBASE, MEDLINE, PSYCINFO (all via OVID). ASSIA, MLA, PILOTS, CINAHL, and Web of Science. To avoid a risk of omitting relevant material, scoping searches identified a range of terms that might be loosely synonymous for recovery narrative, including memoirs and autobiographies.
Database search terms were piloted and then defined against AMED (via OVID), to generate a reference search strategy presented in the digital supplement. This was specialized to each database. Publications were included from inception until August 31, 2018.
Publications were filtered by title and abstract by K.M., with concordance checking by S.R.E. on a sample of 10% of titles and 20% of abstracts. Concordance was 96% for title filtering and 95% for abstract filtering. Remaining articles were retrieved. Inclusion was decided by K.M. and S.R.E., with disagreements resolved by discussion with other authors. If a candidate publication did not use the term recovery narrative, it was included if definitive evidence could be assembled from the abstract or full text that the narratives it considered were recovery narratives. This involved inspecting specific narratives listed in publications for mental health and recovery content.
Hand searching of journals
The 2 journals containing articles included through database searches (Advances in Eating Disorders: Theory, Research and Practice and Journal of Nervous and Mental Disease) were hand-searched from inception to August 31, 2018.
Grey literature searching
Google and Google Scholar were searched using the terms impact of mental health recovery narratives and impact of mental health recovery stories. The first 100 hits were hand-searched.
Expert consultation
Seven researchers with expertise in mental health recovery were sent the list of included articles and asked to identify additional candidates for inclusion.
Citation tracking
Reference lists of all included articles and of a relevant review 13 were hand-searched. Forward citation tracking of included articles and this review was conducted using Google Scholar.
Data Abstraction
A data abstraction table (DAT) was designed and piloted, and it is presented in the digital supplement. The DAT presents details of each included study: country of lead author, design of study, characteristics of narratives, characteristics of participants, time of impact assessment, and social interaction around the narrative. It also presents knowledge about the impact of recovery narratives generated by each study, grouped by categories refined through the piloting process: form of impact, consequences of impact, facilitators to impact, and barriers to impact. Included qualitative articles presented rich narrative descriptions of impact. This meant that the work of data abstraction involved producing short textual summaries of narrative descriptions. Summaries were agreed by the 2 lead authors and led by the language of the source publication.
Quality Assessment
Included studies were critically appraised. Results are included in the DAT. The Critical Appraisal Skills Programme Qualitative Checklist 30 was used for qualitative studies, using established thresholds to indicate high-, moderate-, or low-rated quality. 31 Quantitative studies were assessed using the 15-element McMaster Critical Review Form for Quantitative Studies, 32 with bespoke labels: high (13-15), moderate (11-12), and low (0-10).
Narrative Synthesis
A narrative synthesis was conducted following an established methodology. 33 This consisted of 1) a preliminary synthesis of abstracted material on forms, consequences, facilitators, and barriers to impact; 2) refinement of the synthesis through discussion in a multidisciplinary research team; 3) refinement of the synthesis through consultation with a Lived Experience Advisory Panel; and 4) subgroup analysis. The goal of the synthesis process was to generate a framework describing broad forms of impact but that retained essential details of how impact occurred as presented in included articles.
The preliminary synthesis began by classifying knowledge about impact presented in the DAT as 1) transdiagnostic or 2) diagnostically specific. Example: “Feeling connected to the narrator” was classified as transdiagnostic, whilst “greater effort put into avoidance of ED behaviours” was classified as specific to an eating disorder diagnosis. Classifications were by S.R.E. and were reviewed by clinically qualified authors.
A preliminary synthesis was generated by S.R.E., who conducted an inductive thematic analysis on items classified as transdiagnostic. Items were grouped into named themes, which were selected 1) to describe a meaningful form of impact and 2) for orthogonality. Similar items grouped within a theme were combined. To raise quality, the preliminary synthesis was discussed in a team comprising analysts from multiprofessional backgrounds (mental health nursing, social psychiatry, clinical psychology, community development, design research) and including qualitative expertise. Closely related items were further combined, and names of themes and items were refined for clarity. “Moderators” were introduced to encompass facilitators and barriers.
The updated synthesis was presented to a Lived Experience Advisory Panel (LEAP), comprising 10 members with prior experience of mental health problems and of recovery. Three had published their own recovery narrative. A final version was produced based on their input. The principal change was identification of items to add existing themes to add depth. These items have been labelled as LEAP contributions to distinguish them from items sourced from included publications. During this consultation, LEAP members raised questions relevant to future research, and these are considered in the Discussion.
Items labelled as diagnostically specific to a clinical population were examined. To document forms of impact specific to that population, processes, outcomes, and moderators were tabulated.
Results
The PROSPERO flow diagram for this review is shown in Figure 1.
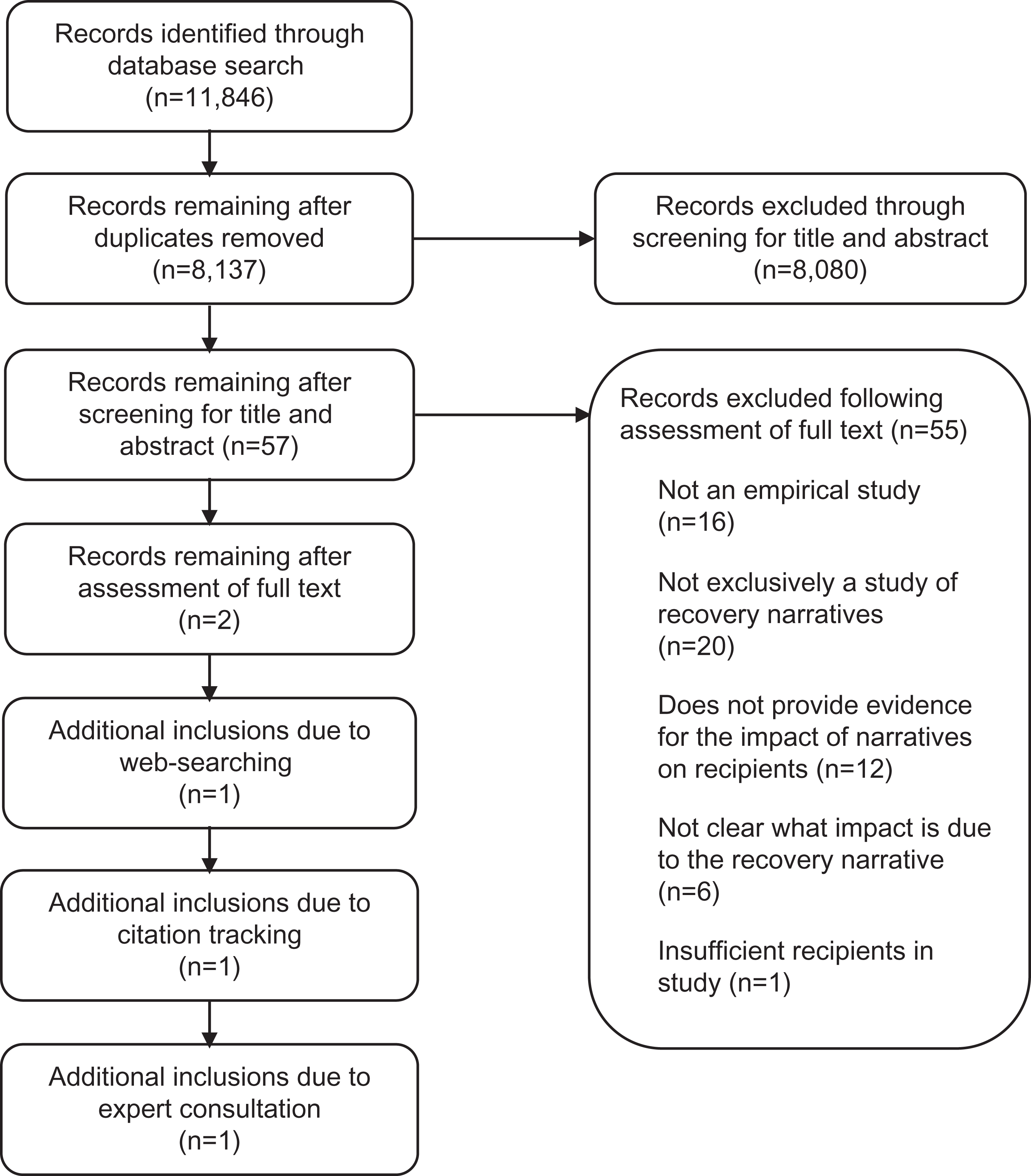
Flow diagram.
Five articles were included (studies 1-5). Featured narratives were characterized as “recovery stories” (studies 1 and 5), “memoirs” (studies 2 and 3), and “lived experience videos” (study 4). All narratives present in studies 2, 3, and 4 were inspected and found to meet the study definition of a recovery narrative.
Key characteristics of included studies are in Table 1. Further detail is provided in the DAT.
Summary of Included Publications (n = 5).
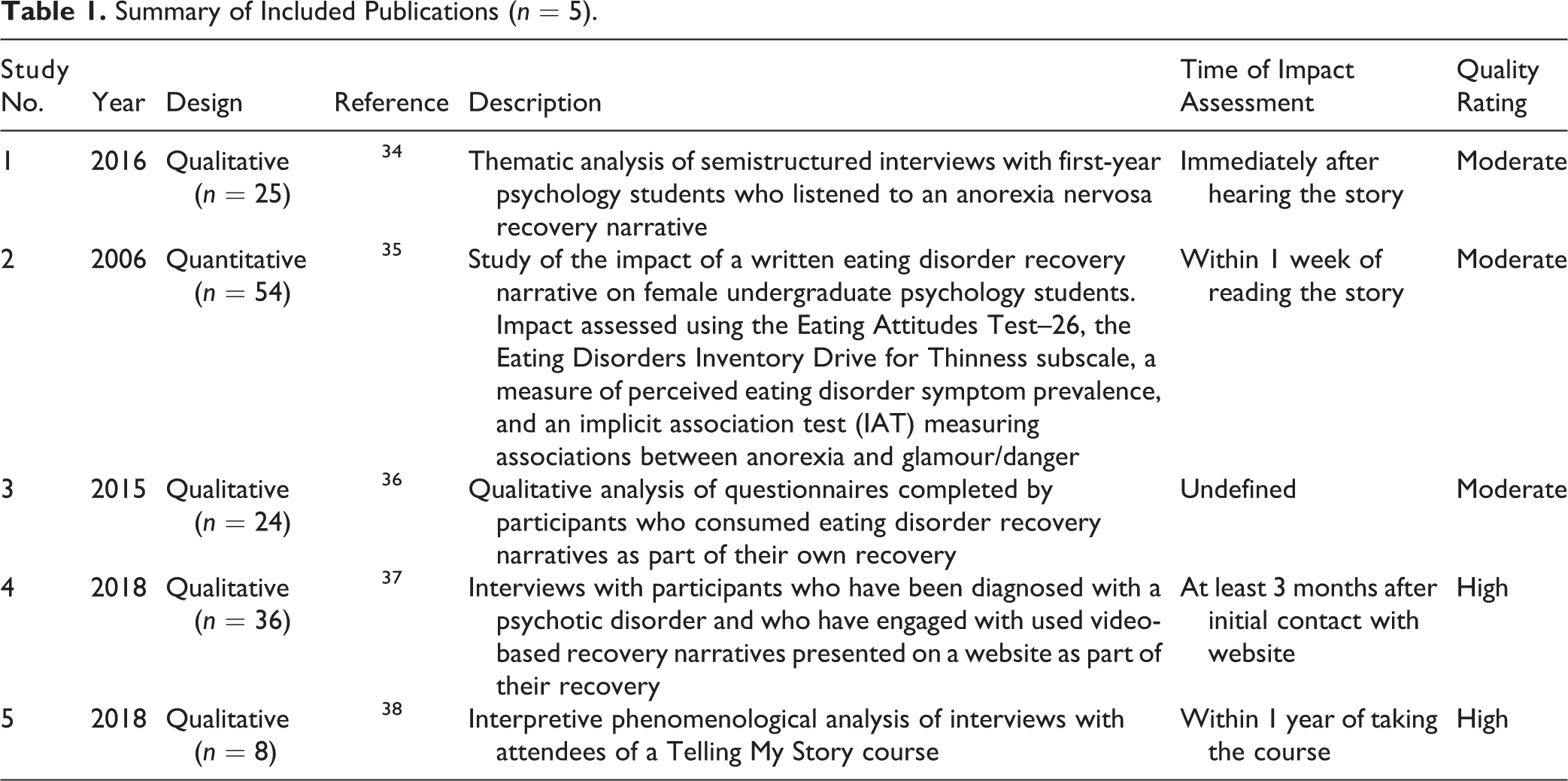
All included articles were studies of the impact of recorded recovery narratives and were of moderate or high quality. The single included quantitative study (study 2) failed to find evidence for impact of an eating disorder memoir on participants who were female undergraduates and not selected for membership of a clinical population. As this article provided no evidence for impact, facilitators, or barriers, it has not informed the narrative synthesis.
The 4 included qualitative studies (studies 1, 3, 4, and 5) were conducted recently. Collectively, these articles included 93 participants, 70 female and 23 male, and hence there is a clear gender bias across included qualitative research. Studies 1, 3, and 4 were conducted by research teams based in Australia but with no overlap in authorship. Studies 1, 3, and 4 note a lack of existing empirical evidence about the impact of recovery narratives on recipients.
Specific items were identified that provided insights into the impact of mental health recovery narratives on individuals experiencing eating disorders, and a subgroup analysis was conducted on these. Despite the inclusion of an article whose participants had been diagnosed with a psychotic condition, no knowledge about impact specific to psychosis was identified.
Framework for Transdiagnostic Impact
Table 2 presents a framework describing transdiagnostic impact, synthesized from forms and consequences identified in the DAT. This table includes the 6 themes identified through thematic analysis, which are our proposed forms of impact, and the items grouped within each theme, which provide more specific detail about how they occur.
Impact and Associated Processes of Recovery Narratives on Recipients.
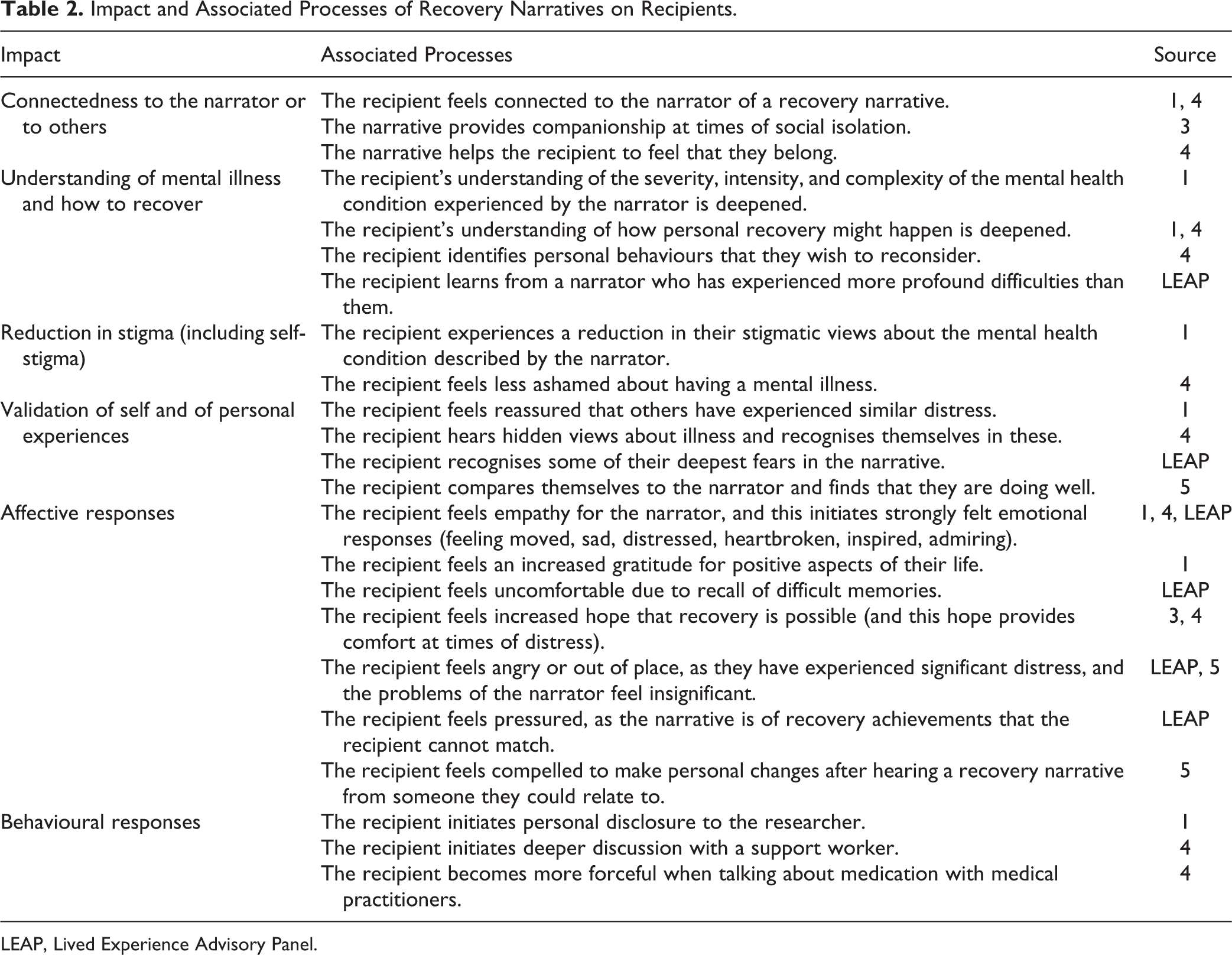
LEAP, Lived Experience Advisory Panel.
Impact described in this table has not been categorized as helpful or harmful due to the possible influence of contextual factors (e.g., “initiating personal disclosure to a researcher” might be helpful if the researcher has the required competence to engage but harmful if not). Connectedness, understanding, reduction in stigma, and validation might be thought of as more cognitive forms of impact, alongside the broad range of more affective responses listed in Table 2, and a limited range of behavioural responses.
Table 3 presents moderators identified through the synthesis, identified from facilitators and barriers listed in the DAT.
Moderators of Impact.
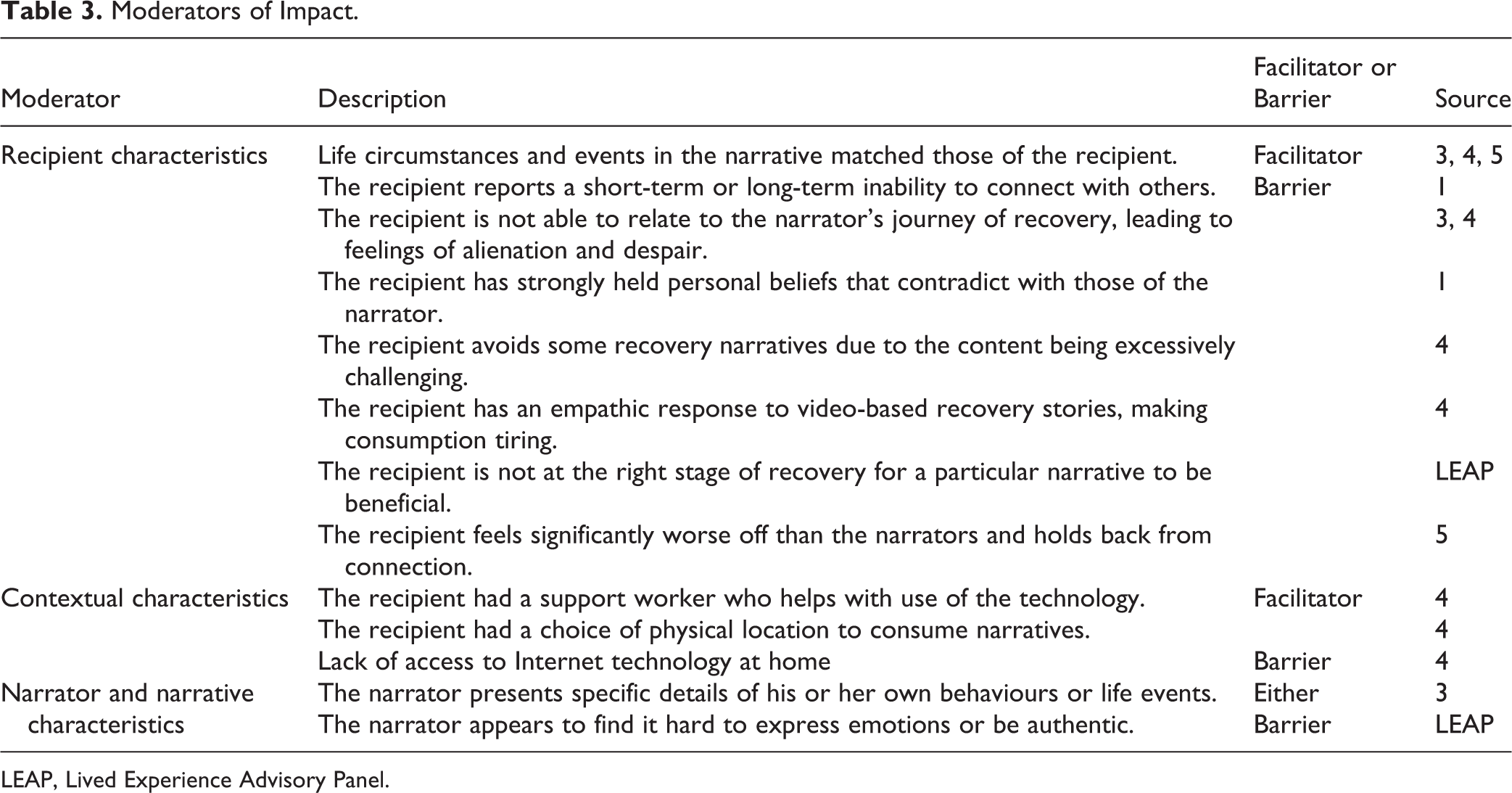
LEAP, Lived Experience Advisory Panel.
Items included in the categories of recipient and narrator/narrative characteristics appeared to facilitate or block a recipient in forming a connection with the narrator or narrative, suggesting an important role for connection forming in enabling impact to occur.
Forms of Impact Specific to Eating Disorders
Table 4 summarizes processes and impact identified as specific to eating disorders.
Processes and Impact Specific to Eating Disorders Narratives.
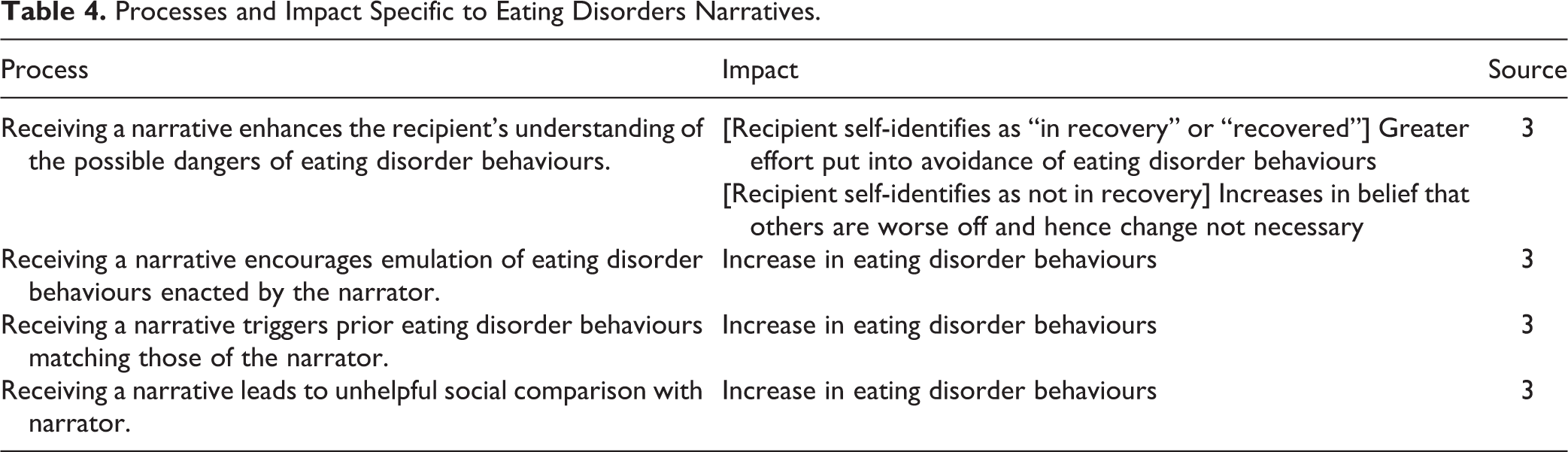
All identified processes can generate harmful behavioural responses, although for the first process, this only occurred if the recipient did not identify as being “in recovery” at the time of receiving the narrative; if the participant did identify as being “in recovery” or “recovered,” a helpful behavioural outcome was generated. These terms were participant-defined in the source article (e.g., there was no usage of a standardized measure to assess recovery stage).
Study 3 identifies a narrator/narrative characteristic that facilitates harmful behavioural outcomes—the inclusion of particular details of eating disorder behaviours engaged in by the narrator, such as dangerously low daily calorie counts or specific patterns of disordered eating.
Discussion
This review has presented a conceptual framework consisting of 9 superordinate themes, comprising 6 types of impact and 3 moderators of impact. A subgroup analysis identified types of impact specific to eating disorders. The inclusion of only 5 articles, despite widespread interest in the use of recovery narratives, suggests a knowledge gap that might be filled through further empirical work, and identification of this knowledge gap is a key contribution of this article. These findings will inform a future trial (ISRCTN11152837).
Relationship to Existing Frameworks
A prior review 25 has considered the impacts of sharing and receiving health material online and identified 4 domains in which positive and negative impact can occur for recipients: 1) finding information, 2) feeling supported, 3) experiencing health services, and 4) affecting behaviour. Feeling supported has similarities with validation of personal experiences, whilst finding information has similarities with understanding of mental illness and how to recover (with the latter being more specific to recovery narratives). Impact on behaviour occurs in both.
Our review has a stronger emphasis on factors that moderate impact, only briefly mentioned in the previous review. It also emphasizes forms of impact distinctive to recovery narratives, such as connection with and empathy for the narrator. Our review does not consider issues around unbalanced or misleading material, considered extensively in the previous review. Learning that an influential narrative might not be authentic can lead to anger in recipients, 39 and LEAP members wondered whether recipients could be harmed by deliberately misleading narratives.
Some online collections of recovery narratives are predicated on a belief that receiving narratives can encourage personal recovery. A systematic review has identified connectedness, hope, identity, meaning in life, and empowerment (CHIME) as processes that underpin personal recovery. 40 Elements of all 5 CHIME process are present in our conceptual framework. Connectedness appears in both frameworks. The CHIME notion of hope appears under affective responses, whilst the CHIME notion of identity incorporates “overcoming stigma,” present as an impact in our conceptual framework. This provides some validation that receiving recovery narratives can promote recovery. The inclusion of “reduction in stigma” as an outcome provides validation for the use of recovery narratives in antistigma campaigns.
Strengths and Limitations
A strength of the review is the identification, through scoping searches, of a broad range of terms that might be synonymous of recovery narrative, important as no included article used this term directly. Other strengths include the use of a wide range of publication databases and grey literature sources, double rating at each stage of sifting to maximize reliability, and the use of an established methodology for narrative synthesis. Limitations include a narrow focus on mental health recovery narratives, given that the impact of narratives produced by other clinical populations may also be relevant in mental health practice, the nonuse of some potential sources such as conference proceedings, and the restriction of the search strategy to English, meaning that some French-language publications could have been excluded.
Implications for Clinical Practice and Mental Health Interventions
Should recovery narratives be used as a resource in clinical practice and mental health interventions? The general clinical evidence is supportive for the former. A survey of 138 psychologists in the United States found a belief that mental health biographies can be helpful in therapy sessions, 41 and a review of case reports has demonstrated mechanisms for integrating autobiographies into psychotherapy sessions. 42 A range of publications have shown acceptability of bibliotherapy and self-help texts as a form of treatment across a range of conditions. 43,44 Biographical material used in these studies was typically in the form of recovery narratives.
The ready availability of mental health recovery narratives online may support usage with younger people, who are known to be heavy users of online health information. 45 This is important given recent arguments that youth mental health should be a priority area in Canada 46 and known challenges around extremely high suicide rates in Canadian Aboriginal youth. 47 Best practice guidelines on Canadian youth suicide reduction 48 include ensuring accessibility of services in rural and remote locations and enhancing engagement with marginalized individuals. Interventions drawing on online material are known to have particular relevance to areas with low population densities, 22 where access to both mental health care and to peers with experience of similar mental health problems may be difficult otherwise. 49 Although limited, Internet access in rural and remote areas of Canada is improving, 50 including through enhancements to cellular networks 51 and initiatives such as the Indigenous Connectivity Summit. 52
Our review highlights potential mental health uses and considerations that are relatively specific to recovery narratives. People experiencing high anticipated discrimination may benefit from stigma reduction by encountering role models through narratives who may not be available in everyday life. People experiencing high levels of social isolation, a known risk factor for youth suicide, 53 may experience enhanced connectedness and more validation of personal experiences. People who are early in their recovery journey may encounter relevant knowledge about how to recover. Knowledge presented in recovery narratives might enable people to cope more readily with the challenges of recovery, with coping being one source of resilience. 54
The review found that recovery narratives can engender strong affective responses, sometimes through empathy to the narrator, including emotions perceived as positive (hopefulness, gratitude for life) and others that are more distressing. LEAP members queried whether secondary traumatization might be one outcome of excessive exposure to distressing elements of recovery narratives, potentially through mechanisms similar to those known in relation to mental health care providers. 55 When available, clinicians should monitor and support processing of emotional responses by clients, given that empathy is known to be significant risk factor for secondary traumatisation. 56 Alternative approaches are needed when recovery narratives are used in online mental health interventions. These might include moderated discussion forums or online support groups, which can offer emotional and instrumental 11 support to members. 57
Our review found no material specific to psychosis, despite inclusion of an article with participants diagnosed with a psychotic condition, and hence does not provide any argument against the use of recovery narratives in the psychosis treatment—in the context of a debate around the appropriateness of using online material in the treatment of psychotic disorders. 58
A lack of connectedness to the narrator of the recovery narrative is identified as a significant barrier to impact in Table 3 and is also indicated as a potential cause of distress. This suggests a need for further research to identify factors that might disrupt connection, of broader importance given the perceived importance of personal connection in peer support work. It also highlights the need for clinicians to attend to a client’s capacity to connect as part of the decision-making process around whether to introduce recovery narratives and when making a selection.
In keeping with prior research into online material and eating disorders, this review supports an understanding of harms that can be caused by engaging with recovery narratives, through processes linked to the elements of the recovery narrative presenting adversity and struggle. LEAP members queried whether similar mechanisms might be seen in consumers with prior experience of self-harm, consistent with prior research that suggests that online material can in fact trigger instances of self-harm. 59 In keeping with Whitlock et al., 60 we would argue that regular assessment of narrative usage might enable the amelioration of harms. Alternative mechanisms are needed in the case of online interventions.
The findings of our review accord with prior work that suggests that the dissemination of specific details of harmful behaviours in online material is one mechanism of harm. 61 This might affect processes for selecting recovery narratives for use in mental health practice, through tactics such as avoiding recovery narratives that include specific details of harmful behaviours.
Conclusions
Mental health recovery narratives can have an impact on cognition, affect, and behaviour, and this impact is moderated by a range of factors. Mental health recovery narratives can promote recovery in recipients, but care might be needed for use with specific clinical populations.
Supplemental Material
Supplemental Material, 846108_digital_supplement_clear - Mental Health Recovery Narratives and Their Impact on Recipients: Systematic Review and Narrative Synthesis
Supplemental Material, 846108_digital_supplement_clear for Mental Health Recovery Narratives and Their Impact on Recipients: Systematic Review and Narrative Synthesis by Stefan Rennick-Egglestone, Kate Morgan, Joy Llewellyn-Beardsley, Amy Ramsay, Rose McGranahan, Steve Gillard, Ada Hui, Fiona Ng, Justine Schneider, Susie Booth, Vanessa Pinfold, Larry Davidson, Donna Franklin, Simon Bradstreet, Simone Arbour and Mike Slade in The Canadian Journal of Psychiatry
Footnotes
Data Access
The complete Data Abstraction Table for this work is included as an online supplement.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research Programme (Programme Grants for Applied Research, Personal Experience as a Recovery Resource in Psychosis: Narrative Experiences ONline (NEON) Programme, RP-PG-0615-20016). Mike Slade acknowledges the support of Center for Mental Health and Substance Abuse, University of South-Eastern Norway and the NIHR Nottingham Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.