
Abstract
Objectives:
To report the outcomes of young people (aged 14-30 years) treated for major mental disorders in a lay health worker (LHW) intervention model in a rural district of conflict-ridden Kashmir, India.
Methods:
Over a 12-month follow-up, LHWs collected data on symptoms, functioning, quality of life and disability, and patients’ and families’ service engagement and satisfaction.
Results:
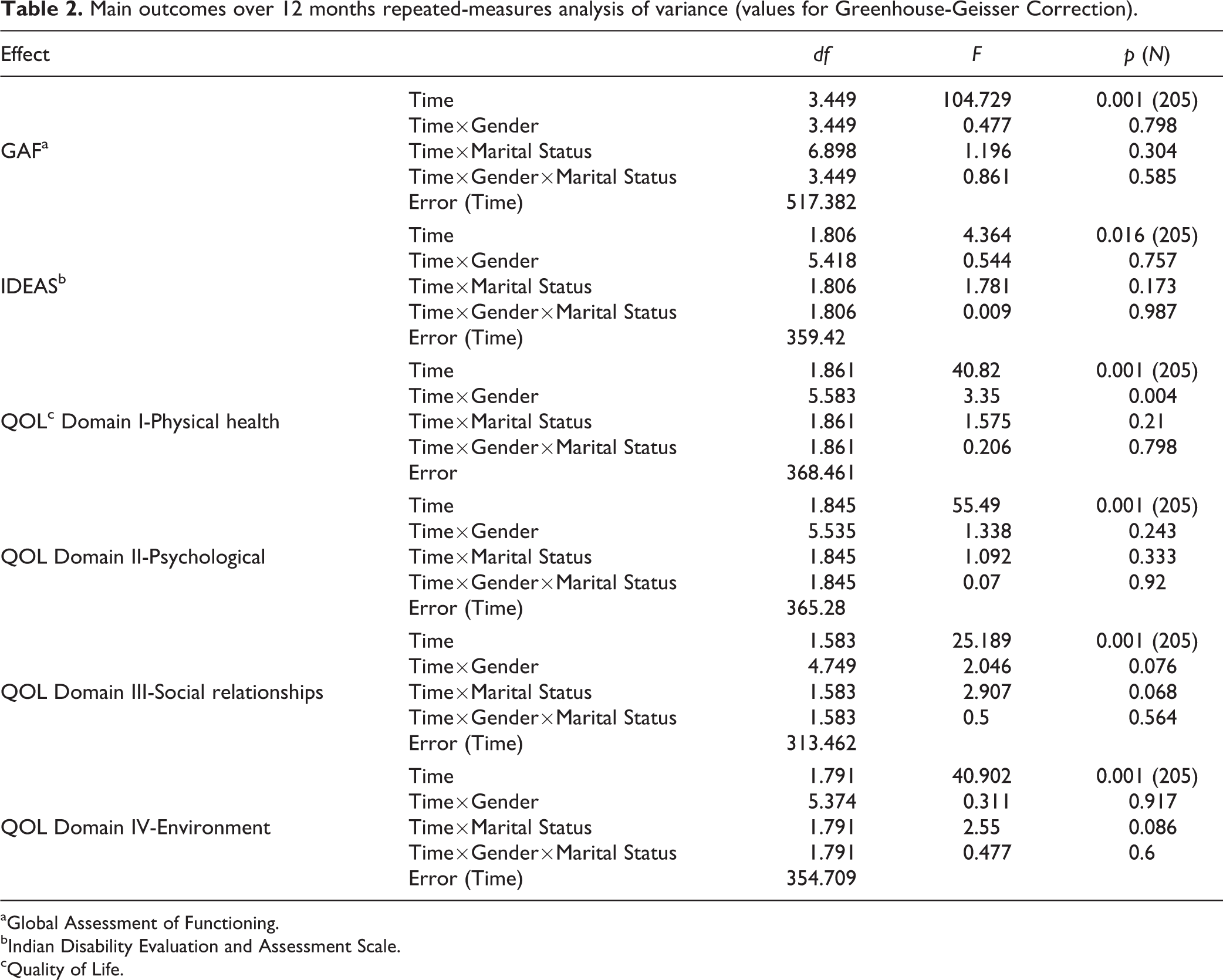
Forty trained LHWs (18 males and 22 females) identified 262 individuals who met the criteria for a diagnosis of a major mental disorder, connected them with specialists for treatment initiation (within 14 days), and provided follow-up and support to patients and families. Significantly more patients (14-30 years) were identified during the 14 months of the project than those in all age groups in the preceding 2 years. At 12 months, 205 patients (78%) remained engaged with the service and perceived it as very helpful. Repeated measures ANOVA showed significant improvements in scores on the global assessment of functioning (GAF) scale (F[df, 3.449] = 104.729, p < 0.001) and all 4 domains of the World Health Organization quality of life (WHOQOL) brief version (WHOQOL-BREF) of the survey—Physical F(df, 1.861) = 40.82; Psychological F(df, 1.845) = 55.490; Social F(df, 1.583) = 25.189; Environment F(df, 1.791) = 40.902, all ps < 0.001—and a decrease in disability (F[df, 1.806] = 4.364, p = 0.016). An interaction effect between time and sex was observed for the physical health domain of the WHOQOL-BREF.
Discussion and Conclusions:
Our results show that an LHW-based service model, implemented in a rural setting of a low-to-middle income region plagued by long-term conflict, benefits young people with major mental disorders. We discuss the implications of our findings in the context of similar environments and the challenges encountered.
In our previous report (Part I 1 ), we described the adaptation and implementation of a model of mental healthcare for young people (aged 14-30 years) of a rural district in India’s Kashmir valley. The latter has had an environment of prolonged armed conflict with limited access to treatment for major mental disorders. We trained 40 lay health workers (LHWs) to provide basic mental health services, supported by low-cost technology and specialists (a psychiatrist, a social worker, and a psychologist) for consultation and supervision. In our previous report (Part I 1 ), we outlined the geographic, political, and epidemiological background to the nature and magnitude of the problem; the status of services, or lack thereof, when the project was initiated; the nature, process and content of the adaptations made to the LHW model implemented elsewhere in India; the project’s objectives; and the implementation of the project.
Here, we report the methods and results of the evaluation of symptoms, quality of life, and functioning after one year.
Methods for Measuring Outcomes
This project was approved by McGill University in Montréal, as well as the local institutional ethics committee of the Sher-i-Kashmir Institute of Medical Sciences, Srinagar, Kashmir, and the Indian Council of Medical Research. Following initial assessments, all patients were invited to sign an informed consent (in Kashmiri or Urdu), approved by the local ethics committee, to participate in periodic evaluations of outcomes on symptoms, quality of life, and functioning.
Assessments and Instruments
Symptoms and personal functioning were evaluated with the Global Assessment of Functioning (GAF) scale, 2 which rates functioning and symptoms using 10 categories, with a total range of scores from 0 to 100. For each category, there is a description of the anchors, and the evaluator chooses a category first before assigning a score within the 10-point range of that category. GAF was rated at entry (baseline) and then every month thereafter.
The Indian Disability Evaluation and Assessment Scale (IDEAS) was used to assess the level of disability and functioning. 2 IDEAS is designed to evaluate disability in 4 domains: self-care, interpersonal activities, communication and understanding, and work. 3 This scale was developed in India and, therefore, considered relevant to the patient population of this study. It has a high level of internal consistency (reliability), convergent validity with measures of psychopathology and discriminant validity with the World Health Organization Quality of Life Survey (WHOQOL-100), a measure of quality of life 3 . IDEAS was administered at baseline, 6 months, and 12 months.
Quality of life was assessed with the abbreviated WHOQOL assessment, WHOQOL-BREF. This self-administered instrument has 26 items and covers 4 domains: physical health, psychological health, social relations, and environment. It has been tested globally at 24 sites on 11,830 subjects and shown to possess a high level of reliability and construct, as well as discriminant validity. 4 The WHOQOL-BREF was used at baseline, 6 months, and 12 months to assess the 4 QOL domains.
Each patient and one family member were asked to provide information separately on how satisfied they were with the service they received using 4 options ranging from not satisfied to very satisfied.
All instruments were translated into Kashmiri and Urdu, the 2 languages spoken in the region and written in a variation of Arabic script, and then translated back to English. The translations and back-translations were reviewed by the site principal investigator (MM) as well as the project principal investigator (AM) for accuracy; Kashmiri is the mother tongue for both investigators, and both speak Urdu. Patient consent forms were provided in Kashmiri and Urdu. When patients were unable to read and write, LHWs carefully read out the questions of the WHOQOL-BREF and recorded their responses verbatim. This procedure was followed in the original validity and reliability study of the WHOQOL-BREF. 4 Initially, all assessments were conducted on paper and the data entered into an SPSS file; later in the project, the data were entered through a web-based platform (see Part I 1 ). Data were verified with the local project coordinator in Kashmir by the research coordinator at the centre in Montréal.
Data analysis
One-way repeated measures analyses of variance (ANOVA) tests were conducted to evaluate change in patients’ symptoms and personal functioning (GAF), disability (IDEAS) and quality of life (WHOQOL-BREF) using scores for each measure at baseline, 6 months and 12 months. Married status and female sex have been associated with favourable clinical outcomes and adverse social outcomes (e.g., abandonment by families) in India. 5,6 Therefore, a subsequent multivariate analysis of variance (MANOVA) was conducted using sex and marital status as covariates.
A Greenhouse-Geisser estimate was used to correct the degrees of freedom in all repeated measures ANOVAs because the assumption of sphericity had been violated for the measures of the 3 main outcomes. Analyses reported here are based on patients for whom complete data were available, as missing data were minimal.
Results
Over a 14-month period (April 2015 to June 2016), 279 cases were identified as experiencing presentations consistent with mental disorders. During consultations, a psychiatrist diagnosed 262 of these (see Table 1 for demographics and diagnostic breakdown) as meeting the criteria for a major mental disorder. Of the remaining 17 not included, 5 presented primarily with family adjustment problems; 9 had unmanaged co-morbid medical disorders (diabetes, metabolic syndrome and suspected thyrotoxicosis) requiring hospital care; and 3 had suspected dissociative disorders that could not be confirmed.
Patient socio-demographic information and diagnosis.
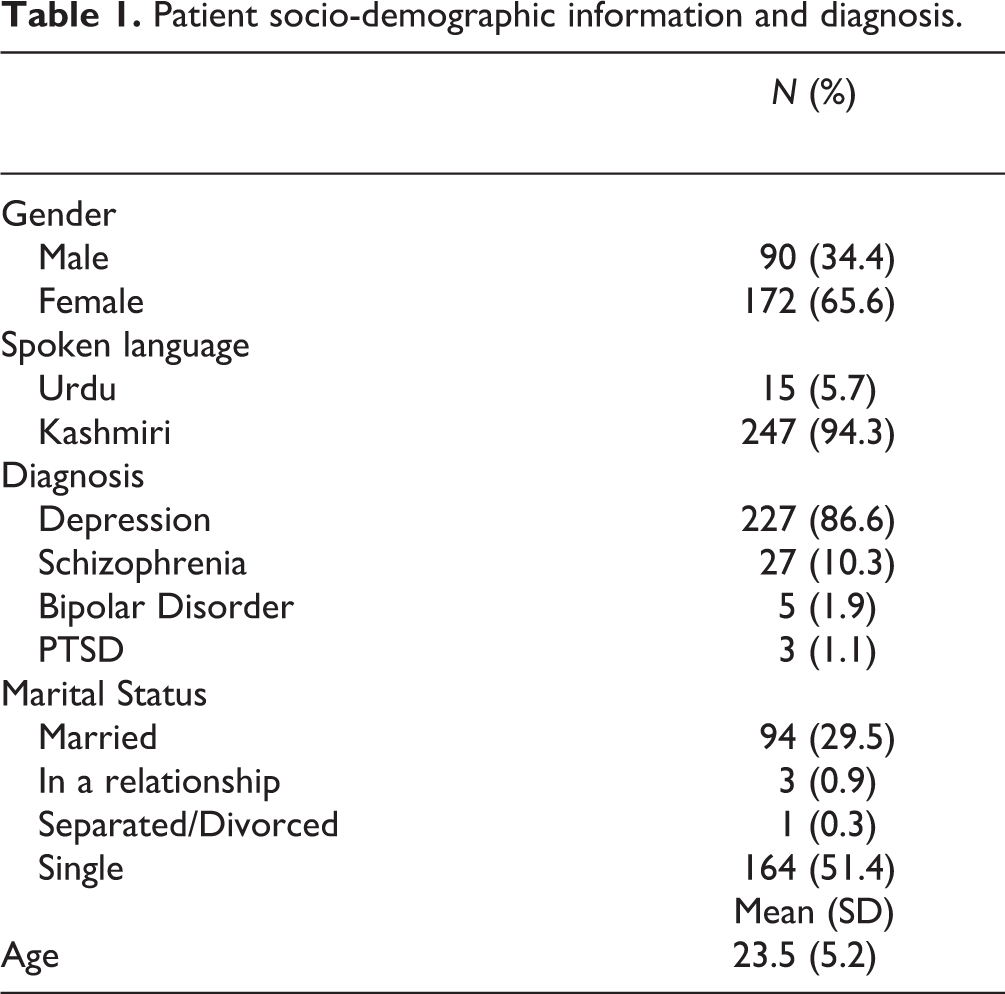
Following initial contact with LHWs, the mean time to receiving a consultation with a psychiatrist was 14 days (range, 0-90 days). Most (87%) patients had a diagnosis of major depressive disorder at baseline (n = 227) (Table 1).
Twenty-three patients (9%) dropped out of care (21 immediately following the initial assessment and 2 during the follow-up). The LHWs’ assessment of patient and family engagement revealed that at 6 months, 239 (91%) patients and 236 (90%) family members remained involved. At 12 months, 205 (78%) patients and 204 (78%) family members were still involved.
Clinical, Functional and Quality of Life Outcomes (see Table 2 and Figures 1 –3)
The results of the repeated measures ANOVA indicated significant improvement over time in the GAF scale (F[3.449, 517.382] = 104.729, p = 0.001). Subsequent analysis using MANOVA with sex and marital status as fixed factors revealed no effect of either sex or marital status. Complete data on GAF were available for 238 patients at 6 months and for 205 patients at 12 months. At 6 months, 159/238 (66%) patients showed an improvement in one and 62/238 (26%) patients in 2 categories. At 12 months, 114/205 (55%) patients showed an improvement across 3 categories and 72/205 (35.1%) patients across 2 categories.
Main outcomes over 12 months repeated-measures analysis of variance (values for Greenhouse-Geisser Correction).
aGlobal Assessment of Functioning.
bIndian Disability Evaluation and Assessment Scale.
cQuality of Life.
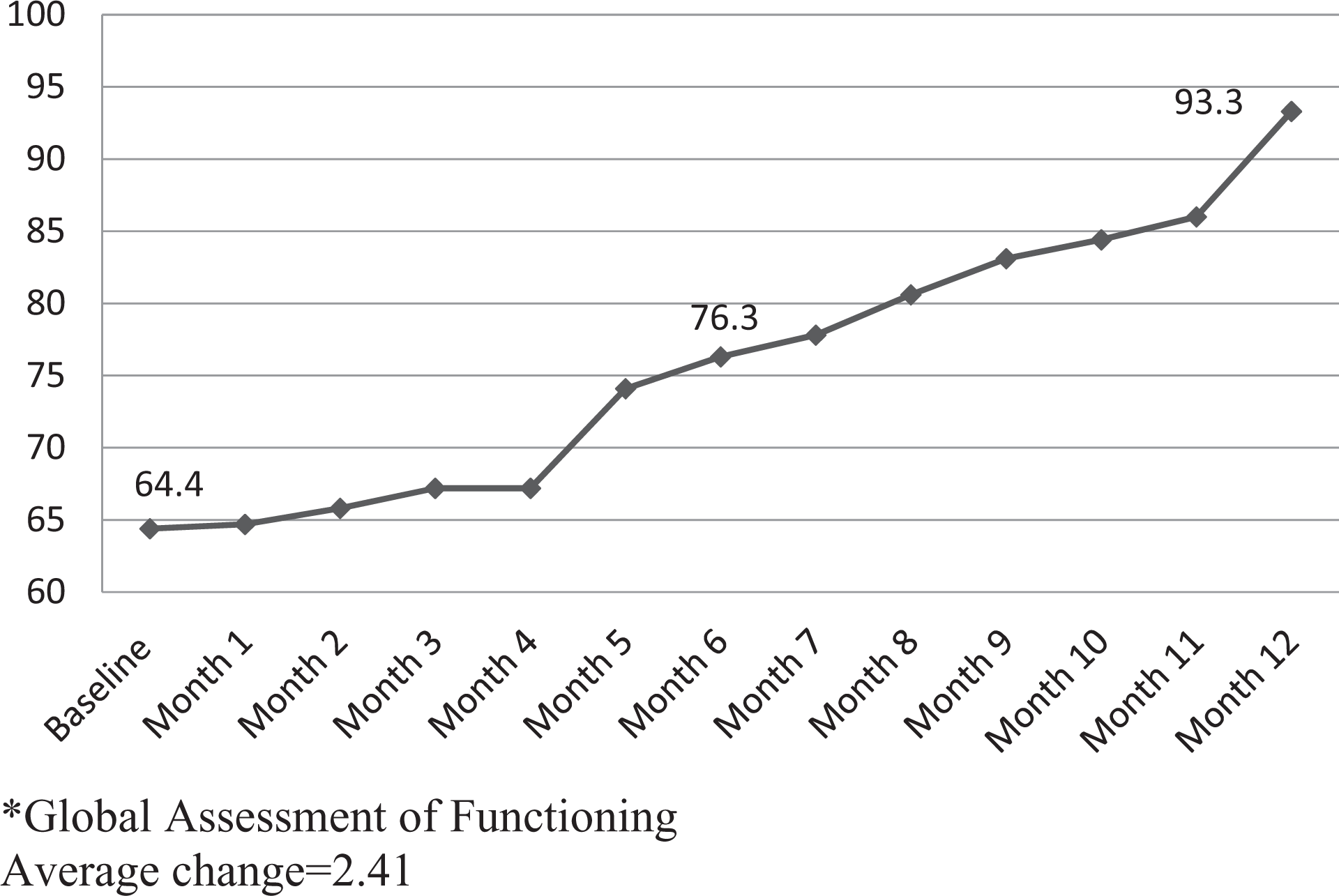
Average global assessment of functioning
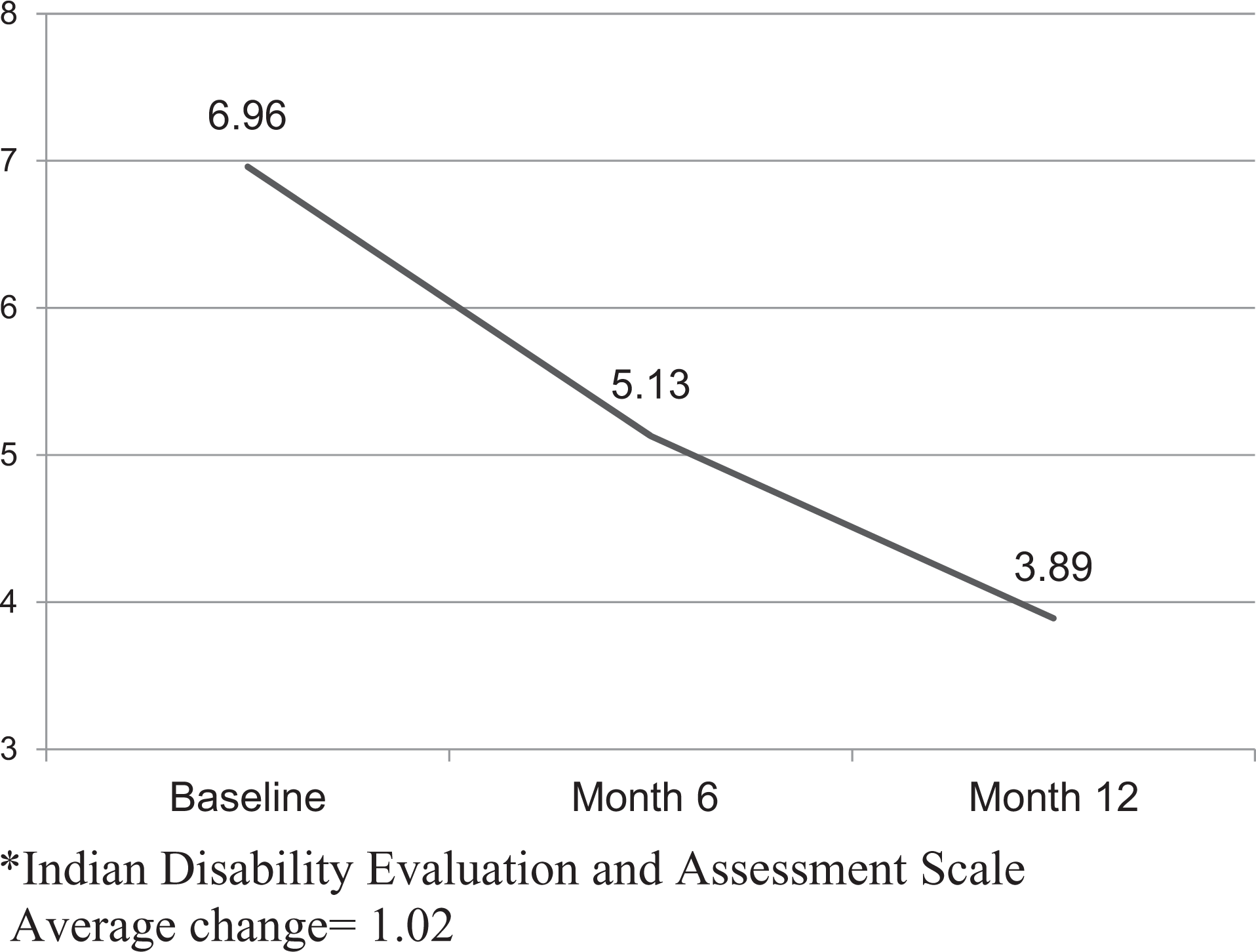
Average Indian Disability Evaluation and Assessment Scale (IDEAS) score over time.
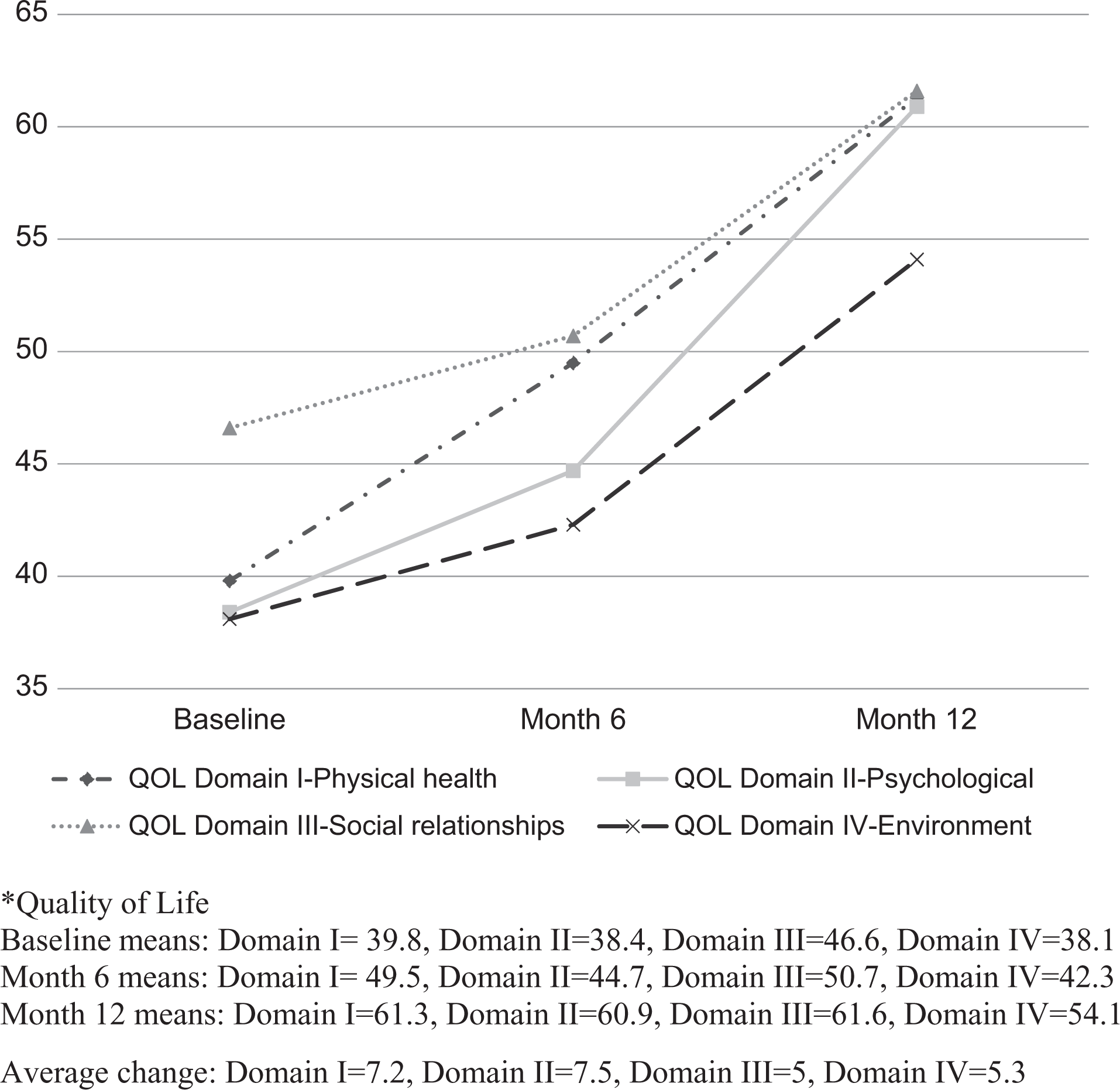
Average quality of life (QOL) score over time.
We also found significant improvement in functioning (i.e., a decrease in IDEAS disability score) over time (F[1.806, 359.429] = 4.364, p = 0.016). Again, subsequent MANOVA analysis revealed no effect of sex or marital status.
The repeated measures ANOVA indicated a highly significant improvement over time for all WHOQOL-BREF domains: physical health (F[1.861, 368.461] = 40.820, p = 0.001]); psychological health (F[1.845, 365.280] = 55.490, p = 0.001); social relationships (F[1.583, 313.462] = 25.189, p = 0.001) and environment (F[1.791, 354.709] = 40.902, p = 0.001). Only improvement in the physical health domain was influenced by sex, with females improving more than males (F[1.861, 368.461] = 3.350, p = 0.004).
All 205 patients and 204 families who answered the satisfaction and helpfulness questions at 12 months reported being satisfied with the services received. They particularly liked receiving free medication and other treatments; doorstep service by the LHWs; and the chance to provide feedback on the change that the intervention had made in their lives.
Discussion
While the LHW model is a feasible and scalable means of delivering mental health care in low- and middle-income environments generally, 7 –9 we have described (Part-11) how this can also be adapted to an environment where an entire population has suffered from the combined detriments of prolonged armed conflict in addition to poverty, low employment, geographic isolation, and poor access to services. This was done through an existing voluntary organization (SAWAB) that had been providing rudimentary psychiatric services with very limited resources.
The partnership with SAWAB, with its well-established local roots and status in the community, facilitated multiple stakeholder engagement, which was seen as an essential ingredient to the success of our project through our Theory of Change exercise. Engaging various stakeholders, including traditional healers (Pirs), religious leaders (imams), village elders, teachers, and the police was a crucial part of the project implementation. At least in the context of our study, stigma about mental illnesses did not appear to impede the involvement of village elders, teachers, and others. This may be related to a sense of shared vulnerability in the context of exposure to traumatic experiences related to the armed conflict.
Other ingredients for the successful implementation of our model included LHW training and support from professional services. The availability of highly subsidised post-secondary education concomitant with the high unemployment rate may explain why our project attracted and retained personnel with a higher level of education than required. A major disruption to the training process occurred just one week into training, when the Kashmir valley was hit by one of the worst floods in its recent history and the training had to be moved to a temporary location on higher ground. The support from professional services was facilitated by an existing relationship between SAWAB and psychiatric services in the city (Srinagar). This allowed the LHWs to obtain relatively rapid consultations for diagnosis and treatment as well as supervision of their day-to-day work.
We had assumed that technology would play a major role in service delivery. Although it did provide additional assistance to the LHWs in staying connected to their patients and their families and in monitoring their treatment adherence, the LHWs reported that patients seemed to prefer direct contact. Previous reports on the region have indicated widespread exposure to traumatic events, such as shootings, bombings, and other types of violence. Indeed, the youth on whom we focussed (aged 14-30 years) had grown up entirely in an era of ongoing conflict, as indeed had the LHWs. The latter hailed from the very communities they served, and shared similar experiences of conflict and suffering. Such shared experiences likely helped the LHWs in engaging patients and their families and winning the trust of stakeholders. The use of technology did, however, play a major role in the ability of LHWs to access training material at any time and in collecting data, especially in the latter part of the project.
In addition to improving access, our model yielded strongly positive outcomes with respect to global functioning, symptoms, disability, and quality of life. It also satisfied, engaged and retained most of the patients and their families. Our dropout rates are even lower than the relatively low rates reported in one-year treatment studies in low- and middle-income countries like India. 9 –11 These significant improvements in access, engagement, and outcomes are attributable to several interrelated factors.
Key Factors Facilitating Positive Outcomes
The broad social acceptance of the project and, thereby, the high levels of public engagement, are likely explicable by our early and sustained involvement of multiple stakeholders, especially traditional healers, religious leaders, and school teachers. This social alliance was further strengthened by the key role of LHWs, who had sound knowledge of local conditions and were often known to the patients. The high levels of family involvement that have been reported in low- and middle-income countries, 12 –14 further boosted by our LHWs’ engagement efforts, may also have contributed to the low treatment dropout rates and better treatment adherence. 15 –19 The project’s social success owed much to the standing that our local partner, SAWAB, enjoyed in the community. SAWAB is a known and trusted provider of emergency mental health help after disasters, like the 2006 Kashmir earthquake (see Part I1 for more information).
Part of the reason for our strongly positive outcomes may be the generally high response rates among young, treatment-naïve patients. 20 –23 In our case, there was the added psychological effect of a long-suffering people, with limited previous access to mental healthcare, viewing rapid and easy access to treatment with much hope. Their positive outlook toward their treatment, the sustained involvement of their families, and the provision of free medication and supportive therapy likely contributed to the improved outcomes. Also significant were the timeliness and quality of care, which were ensured by effective outreach and early identification; the diligence of well-trained LHWs; the supervision and services of mental health professionals (psychologists and psychiatrists); and the grounding of the model and its delivery in sound, local cultural knowledge.
That a project of this scale was relatively quickly rolled out in a conflict-plagued region and continued despite a natural disaster is a testament to community resilience and the rapid development of trust through the existing voluntary sector (SAWAB), phenomena that bear further systematic investigation.
Methodological Considerations
Patients showed a highly significant improvement in GAF scores and most patients improved across at least 2 categories, implying a meaningful change. Their relatively high baseline ratings despite clear diagnoses of major mental disorders and exceptionally high 12-month ratings could reflect an inflation of scores by the LHWs at all time-points. Some of this inflation could be because of minimal post-training monitoring of assessments. Time constraints and the disruption of the training by floods precluded inter-rater reliability training. While it is possible that the scores are inflated, this is unlikely to have occurred selectively at any time-point. The higher GAF scores may also reflect that some LHWs may have identified with the patients’ suffering. Indeed, there were instances where some LHWs described their own conflict-related experiences of anxiety, nightmares, and other experiences in their encounters with patients and families.
The self-administered measures that also showed significant improvement are unlikely to have been influenced by rater bias. The instrument we used to assess disability and functioning was chosen primarily because it had been developed in India. It emphasizes a reduction in disability over time and not an improvement in functioning. Relatively few patients were rated as seriously disabled. This could reflect the young age of the patients and, possibly, the relative recent onset of their illness. Moreover, some LHWs may have been hesitant to see patients as very disabled. The economic disruption caused by the conflict has resulted in extremely low employment rates. This may have coloured raters’ perceptions, making it difficult for them to distinguish “normal” levels of economic inactivity from levels indicative of or related to mental illness.
Most (87%) of the patients treated had a diagnosis of a major depressive disorder. The substantially higher proportion of women (67%) in our sample is consistent with women having higher rates of depressive disorders. 24 Nonetheless, there may be a need for targeted outreach to increase the identification of mental health and addiction problems among men. It had been reported anecdotally that a new problem of substance abuse had become prevalent among young men in the Kashmir valley, which, before the conflict, was almost non-existent in this predominantly Muslim population. Such reports arose from group discussions held with stakeholders by the project investigators and LHWs, and were based on observations made by teachers as well as clinicians involved through SAWAB in their respective practices. It is likely that young men are reluctant to report and seek help for problems of substance abuse because of cultural and religious taboos on substance use.
Given the region’s history of conflict and previous findings of the high prevalence of post-traumatic stress disorder (PTSD), 25 the number of PTSD cases in our sample was low. There is often a high rate of comorbid depression in cases of PTSD, 26 –28 with depressive symptoms requiring more urgent attention. Clinicians may have favoured diagnoses like major depressive disorder that allowed them to prescribe more specific treatments. Because trauma is an entrenched, longstanding and “accepted” aspect of people’s daily lives in this region, they may have not seen the need to explicitly disclose traumatic experiences or may have feared repercussions from authority. Similarly low rates of PTSD diagnosis have been reported in other jurisdictions where exposure to traumatic events is prevalent. 29 Future research should examine the extent to which this reflects true under-prevalence vs. clinician bias/preference for alternative diagnostic formulations.
We acknowledge that there was no control group. Conducting a controlled study in a community with high levels of suffering and little mental healthcare access would have been difficult, if not unethical. Our study sought to demonstrate the workability of a low-cost, LHW-based model in a setting like Ganderbal, to the longer-term end of arguing for its scale-up to other rural parts of Jammu and Kashmir and, potentially, to other similar remote, rural, resource-poor, and conflict-affected parts of the world.
Conclusions
The success of this model is predicated on the integration of various components previously identified as valuable in global mental healthcare innovations. These include the availability of suitable LHWs and their proper training; support from professional service providers; the engagement of multiple stakeholders; and the involvement, especially in case identification, of key community figures (e.g., religious leaders) and institutions (e.g., schools).
Relatively novel to our study is the specificity of our context as a conflict-ridden zone and the involvement of an existing voluntary medical sector. The former required the engagement of not only those who may be generally involved in the pathway to care for young people needing care but also of district administration including the armed forces and the police to ensure feasibility and security. In such regions, it may be particularly important to recruit LHWs from the same communities as patients. Their shared lived experiences of trauma and conflict may promote the engagement of patients and families and their retention as service providers. Similar to our method of access to specialists through SAWAB, there are instances of specialists from Non-Governmental Organizations supervising LHWs in low- and middle-income contexts. 30,31
In addition to the model we deployed, there are reports of using other models of care in conflict-ridden areas. For example, in the tribal area of North Waziristan, Pakistan, which has a large, internally displaced population as a consequence of armed conflict, Humayun et al. (2017) conducted mental health camps to identify cases and provide psychosocial support and treatment. 32 They used volunteer professionals from Islamabad, the capital of Pakistan, to bolster the scant local services, and used Mental Health Gap Action Programme (mhGAP) guidelines to train local health workers. Notably, unlike us, Humayun et al. relied on an existing corps of health workers and not LHWs; did not conduct a long-term follow-up; and did not report outcomes. It may therefore be worthwhile to investigate a combination of their model and ours in areas of highly variable resource availability.
Scaling our model up to the entire region of Kashmir would require the involvement of individuals (opinion leaders, politicians and figures of traditional authority) and institutions (health, development and finance departments) that hold the key to public culture, policy, and funding. Further innovation of mixing this with improved primary health care or other models should also be explored.
Mental healthcare models like ours, and the one used by Humayun et al., offer hope not only in low- and middle-income contexts but parallel environments elsewhere. For instance, Canada’s remote northern communities, too, have high needs, poor resources and geographical isolation and could benefit from such innovative, low-cost, high-impact interventions.
Supplemental Material
Supplemental Material, LHW_Post-training_Quiz - Testing the Effectiveness of Implementing a Model of Mental Healthcare Involving Trained Lay Health Workers in Treating Major Mental Disorders Among Youth in a Conflict-Ridden, Low-Middle Income Environment: Part II Results
Supplemental Material, LHW_Post-training_Quiz for Testing the Effectiveness of Implementing a Model of Mental Healthcare Involving Trained Lay Health Workers in Treating Major Mental Disorders Among Youth in a Conflict-Ridden, Low-Middle Income Environment: Part II Results by Ashok Malla, Mushtaq Margoob, Srividya Iyer, Abdul Majid, Shalini Lal, Ridha Joober and Bilal Issaoui Mansouri in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
We acknowledge the generous support of Drs. Rashid (general practitioner) and Majid (Community Medicine) for their contribution to training and supervision of LHWs and for their constant support as members of the community in the region where the project was carried out. We also want to thank Mr. Hashim Makhdoom for his collaboration on data collection and verification. Last, but not least, we want to thank the young people of the Ganderbal district and their families or agreeing to participate in the evaluation of the care they received and the 22 young women and 18 men (LHWs) who provided care with compassion and personal interest under difficult circumstances.
Data Access
The senior author and all other authors had full access to the data. The data are saved as per regular research protocol and can be made available with mutual agreement depending on the purpose for such demand, through approach to the senior and corresponding author (A.M.).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: None of the authors had any conflict of interest in relation to the funding sources or conduct of this study. Other aspects of COI are provided separately as per guidelines.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded primarily through a grant from Grand Challenges Canada with additional smaller contributions from the Graham Boeckh Foundation, Douglas Mental Health University Institute and Myelin & Associates. The funding sources had no role in data collection, analysis interpretation or in the writing of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.