
Abstract
Objective:
Estimates of mood and anxiety disorders are highly variable among migrant groups, as they are influenced by the socio-political context. Our objective was to conduct a systematic review and meta-analysis to synthesize available Canadian evidence on the prevalence and incidence of mood and anxiety disorders among migrant groups.
Methods:
Studies were identified from MEDLINE, EMBASE, and PsycINFO. They were included if they used population-based samples, presented data on the incidence or prevalence of diagnosed or self-reported mood or anxiety disorders for first-generation migrant groups in Canada, and used a Canadian-born or long-term resident reference group.
Results:
Nineteen studies met our inclusion criteria. Prevalence ratios ranged from 0.48 to 0.87, and nearly all estimates were obtained from population health surveys. Prevalence estimates among migrant groups were lower than the reference group, with the 90th percentile of estimates ranging from 1.5% to 8.2%. Risk factors for mood and anxiety disorders among migrants included being female, younger, unemployed, having lower income, and living in neighborhoods with a lower proportion of migrants.
Conclusions:
There remain many gaps in our current understanding of mood and anxiety disorders among migrant groups in Canada. Although evidence suggests the prevalence of mood and anxiety disorders are consistently lower among migrant groups, a lack of incidence estimates limits the strength of this conclusion. Future research should focus on comparisons of self-reported and diagnosed estimates, the use of a range of different primary or secondary data sources, and consideration of important risk factors.
Prospero Citation:
Jordan Edwards, Malini Hu, Amardeep Thind, Saverio Stranges, Maria Chiu, Kelly Anderson. The burden of mood and anxiety disorders among immigrant and refugee populations in Canada: a systematic review. PROSPERO 2018 CRD42018087869 Available from: http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018087869.
One in five Canadians are foreign born, which is the highest proportion among the seven nations with the largest economies in the world (G7). 1 The relationship between mental health and immigrant and refugee status is complex, and its reporting requires thorough contextualization. 2,3 Two of the most common classes of psychiatric disorders are mood and anxiety disorders, which have a profound impact on the overall burden of mental illness in Canada. 4 Mood and anxiety disorders comprise a broad spectrum of conditions with a wide range in severity, from states of anxiety and poor adjustment to more severe debilitating disorders such as obsessive-compulsive disorders, phobic disorders, depressive disorders, and bipolar disorder. Both classes of disorders can have a major impact on a person’s everyday life, and can range from short episodes to a more chronic course of illness. 5
Compared with native-born residents, the prevalence and incidence of mood and anxiety disorders are highly variable among migrant groups and are influenced by the socio-political context. 6 Experiences before, during, and after migration have been shown to influence the risk of mood and anxiety disorders. 7,8 Research from Canada and the United States (US) suggests that generation status (i.e., first- v. second-generation), age at migration, length of time in the new country of residence, and country of origin all influence the relationship between migrant status and mental disorders. 6,9,10,11,12
The prevalence and incidence of mood and anxiety disorders can impact health service planning and public health initiatives. 13 Variation in observed estimates may be due to factors such as cultural differences in access to mental health care and help seeking attempts in ethnic minority populations. 14 Furthermore, the availability and use of culturally sensitive measures of mood and anxiety disorders may also contribute to observed differences. For example, the Cultural Formulation Interview (CFI), which was designed to address cross-cultural issues with diagnoses made using the DSM-5, is readily available, even though previous research suggests it is used inconsistently across encounters. 15,16
Although the epidemiology of mood and anxiety disorders among migrant groups has been studied previously in Canadian settings, 17 –43 a comprehensive synthesis of the literature does not exist. Synthesizing available estimates and assessing the state and quality of currently available Canadian evidence will strengthen our understanding of the etiology of mood and anxiety disorders among Canadian migrant groups, and will help inform health service planning to meet the mental health needs of newcomers. It is also important for highlighting gaps in the current evidence base and priorities for future research directions.
Our objective was to conduct a systematic review of the literature on mood and anxiety disorders among migrant groups in Canada. We specifically sought to synthesize prevalence ratios and incidence rate ratios of mood and anxiety disorders among immigrants, refugees, and Canadian-born or long-term resident comparison groups. We further sought to explore whether these estimates varied by age, gender, length of time in Canada, age at migration, or country of origin.
Our systematic review followed the guiding principles of the Cochrane Collaboration, 44 and adhered to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guidelines 45 (Appendix S1). The review methodology was pre-registered with the PROSPERO international prospective register of systematic reviews (CRD42018087869).
Methods
Search Strategy
Following consultation with a librarian, we searched the electronic databases Medline, EMBASE, Sociological Abstracts, and PsycINFO in March 2018 using controlled vocabulary and keyword variations of the following concepts: mood, anxiety, immigrant, refugee, and Canada (search strategy Appendix S2). We searched for studies on any mood or anxiety disorder that included but was not limited to depression, generalized anxiety disorder, and bipolar disorders. We also conducted forward and backward citation searches of included studies. 18 –43
We searched the grey literature in April 2018 using the electronic databases Dissertations and Theses and Canadian Health Research Collection using identical controlled vocabulary as our previous electronic search. We further searched the grey literature guided by the Grey Matters’ checklist 46 by searching all websites listed in the checklist under the headings of “health statistics” and “Canada” (Appendix S2) using the terms “mood” or “anxiety”. We did not restrict searches by date or language. When abstracts or unpublished papers were retrieved in our search, we contacted the corresponding authors to establish whether the work had been subsequently published.
Selection Criteria
We included studies that used population-based samples and reported the incidence or prevalence (or numerator and denominator data that enables computation) of diagnosed or self-reported mood or anxiety disorders for at least one migrant group aged 16 and over from any country (first-generation immigrant or refugee) as compared with a reference group from Canada.
47
We did not impose limits on language or date. We included relevant review articles if they presented primary data on prevalence or incidence estimates that had not been reported elsewhere. Definitions for our inclusion criteria were as follows: Population: Our population of interest were all people over the age of 16, as this age range has been previously used to describe adult psychiatric populations.
13
Studies focusing on child and adolescent populations were excluded given that psychiatric presentations may differ in these age groups.
12
If a study was unclear regarding the included ages, we considered it to have an adequately “adult” population if there was a mean age of at least 30 y. Exposure: We included any person coming to Canada from any country as any class of immigrant or refugee (i.e., economic, family class, or refugee).
48
We restricted our search to first-generation migrant groups, as we were interested in exploring influences of the migration process on mood and anxiety disorders. Comparison: We included studies using Canadian-born or long-term resident comparison groups, defined by Chen et al., in 2009, which may or may not include second-generation migrant groups.
23
We excluded studies that specifically used a second-generation migrant reference group, as directly comparing first and second-generation migrant groups was outside of the scope of this review. Outcome: We included studies assessing any mood or anxiety disorder that used symptom-rating scales, self-reported diagnoses, or diagnoses obtained from medical records or health administrative data. Study Design: We included studies that provided estimates from any Canadian setting, whether national, provincial, or from a specific geographical region. We included studies using any well-defined population. The populations must have been defined by geographic boundaries (e.g., Ontario) or by other criteria such as a membership (e.g., Blue Cross Health Insurance Plan) or occupation (e.g., research using occupational cohorts). Included studies were also required to provide denominator data for their estimates of prevalence or incidence.
5
Study Selection and Data Extraction
The first author (JE) screened titles and abstracts from the electronic database search for studies meeting our inclusion criteria. The first author also screened the titles from the grey literature searches and conducted backward and forward citation searches. Full-text articles were obtained for potentially relevant studies or where relevance was unclear. Two authors (JE, MH) independently assessed the full-text articles to determine eligibility and to complete data extraction. In the case of disagreement, resolution was achieved by discussion with a third reviewer. A bibliographic list of excluded studies from the full-text assessment can be found in Appendix S3. We used a data extraction form developed a priori (see Appendix S4) to record information about the methods and results of each included study. This information was partitioned into 3 categories: Study characteristics: author, publication year, setting, study design, study duration, data source, study population, population ethnicity, country of birth, study exclusion criteria, sampling methodology, age range, diagnostic outcomes. Incidence and prevalence estimates: sample size of migrant groups and reference groups, prevalence estimates or incidence rates, prevalence type, adjustment (if any) for confounding factors. Risk factors: other data derived from the included studies to allow for further analyses of potential variation in prevalence and incidence estimates. We extracted data on all risk factors assessed.
Critical Appraisal
Two independent reviewers (JE, MH) assessed the risk of bias. In the case of disagreement, resolution was achieved by including a third reviewer. We used a risk of bias tool developed by Kirkbride and colleagues in 2012 49 to study characteristics, and outcome variables based on best practice in epidemiological studies. Study quality was rated on a 7-point scale from 0 to 6. Seven indicators of study quality were assessed: defined catchment area, accurate denominator data, population-based case finding, standardized research diagnosis, blinding to demographic variables, inclusion criteria clearly listed, and leakage study conducted. We modified this tool by removing the last item on leakage, which is used to identify potential missed cases from screening procedures; this was largely not applicable to this report, given that all but one study used a survey design, and therefore this item did not differentiate study quality. 49
Data Analysis
We have summarized information on the characteristics of the included studies, such as study location, data sources, sample, type of migrant group, mood or anxiety disorders measured, measurement type, and risk factors assessed. We used this information to perform a narrative synthesis of the results to summarize broad themes across the available literature. We also present unadjusted prevalence, incidence, and prevalence/incidence ratios for each of the included studies. Our forest plot was created using the metan package for STATA (version 13). 50 We made a post hoc decision to not conduct a meta-analysis due to the high degree of homogeneity of the estimates and the substantial overlap in secondary data sources used to compute these estimates; as such, pooled estimates would neither increase the precision nor resolve inconsistencies in the estimates of mood and anxiety disorders among migrant groups in Canada. Finally, publication bias was explored by creating funnel plots using the confunnel procedure and performing Egger’s test.
Results
Our search strategy identified 2,725 citations and we screened 101 full-text articles. Of these, 19 primary studies met the inclusion criteria (Figure 1). 18 –43
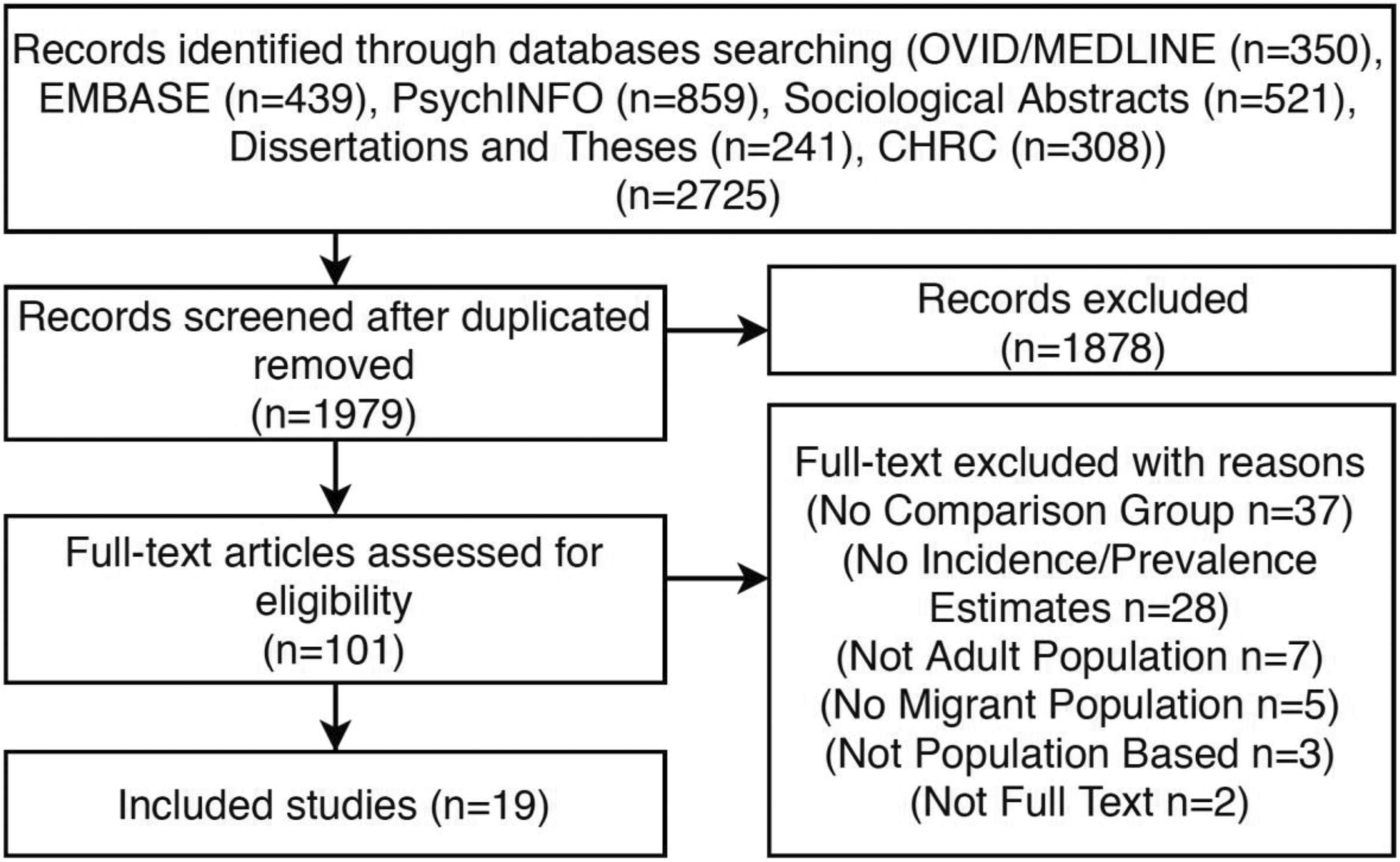
Flow chart of the search strategy and exclusion process of the systematic review evaluating mood and anxiety disorders among migrant groups in Canada.
Study Characteristics
The 19 included studies were conducted between 2002 and 2017 (Table 1). Nearly all studies (n = 15) used data from different waves of the Canadian Community Health Survey (CCHS), which provided national estimates. Of the remaining studies, one used data from Ontario, 3 concentrated on British Columbia, and one was conducted in Quebec. Two studies 23,42 used a longitudinal design, whereas the rest used a cross-sectional design. Seventeen studies collected data from any migrant group, whereas 2 studies focused on migrant groups of Chinese/South Asian decent. 24,39 Most studies considered migrants as a single group, with little consideration of ethnicity, country of origin, or migrant class. Four of the included studies provided age estimates for both migrant and Canadian-born/long-term resident groups. 26,39,42,43 Four of the included studies provided estimates for recent (less than 10 y in Canada) and long-term (more than 10 y in Canada) migrant groups. 18,34,37,38
Characteristics of Studies Included in the Systematic Review of Mood and Anxiety Disorders Among Migrant Groups in Canada (n = 19).
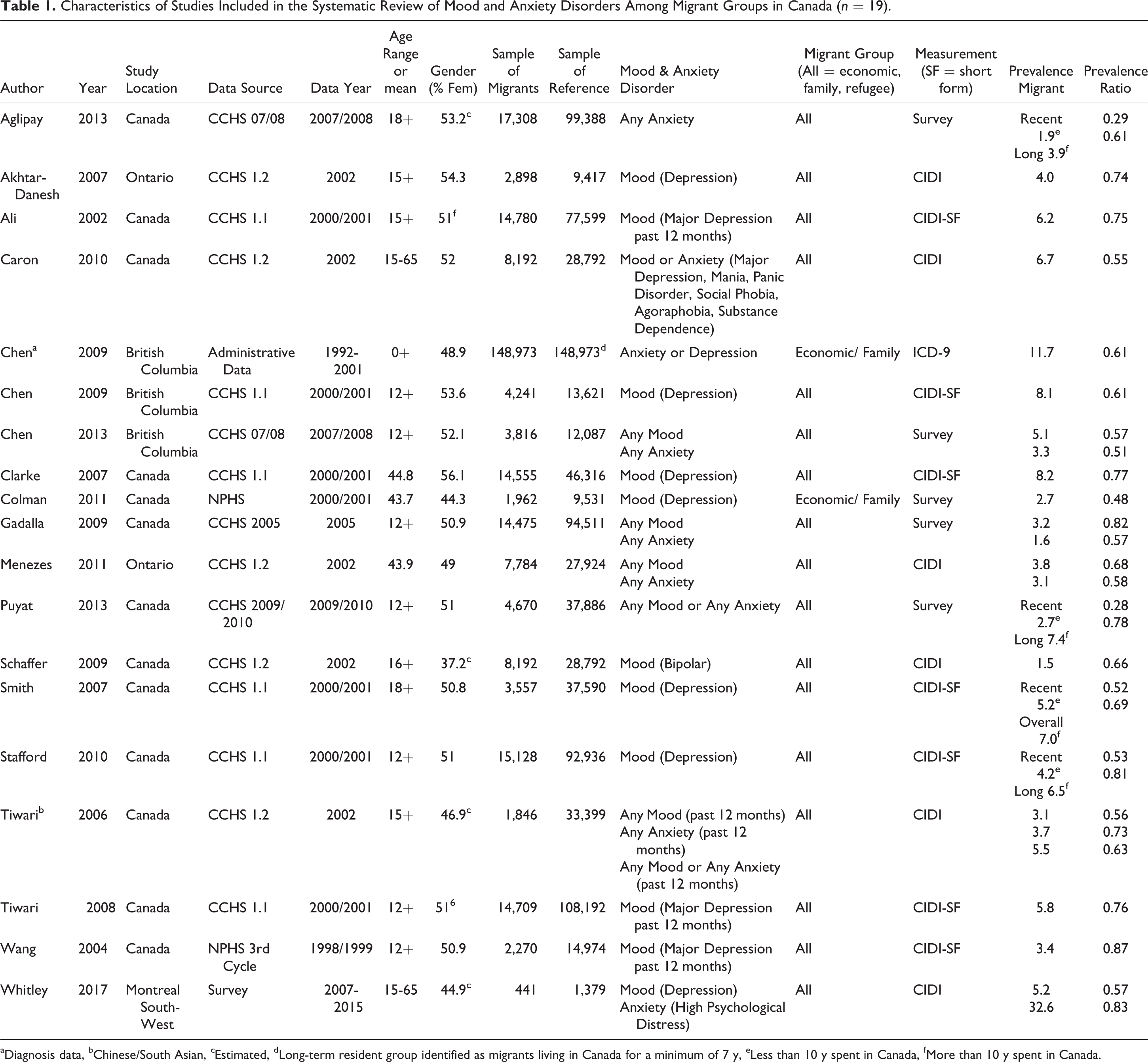
aDiagnosis data, bChinese/South Asian, cEstimated, dLong-term resident group identified as migrants living in Canada for a minimum of 7 y, eLess than 10 y spent in Canada, fMore than 10 y spent in Canada.
Mood and anxiety disorders were measured in 3 ways: 1) using symptom rating scales, specifically the Composite International Diagnostic Interview (CIDI n = 6; CIDI-Short Form n = 7); 2) using self-reported diagnosis (e.g., “Do you have a diagnosed anxiety disorder such as a phobia, obsessive-compulsive disorder, or panic disorder?”) (n = 5); 3) using clinical diagnoses based on ICD-9 codes from health administrative data (n = 1).
Most of the included studies had low risk of bias for all criterion assessed. Five of the included studies did not provide standardized diagnostic criteria, which led to a rating of high-risk of bias (Table 2).
Quality Assessment Ratings for Studies Included in the Systematic Review of Mood and Anxiety Disorders Among Migrant Groups in Canada, Developed by Kirkbride and Colleagues. 50
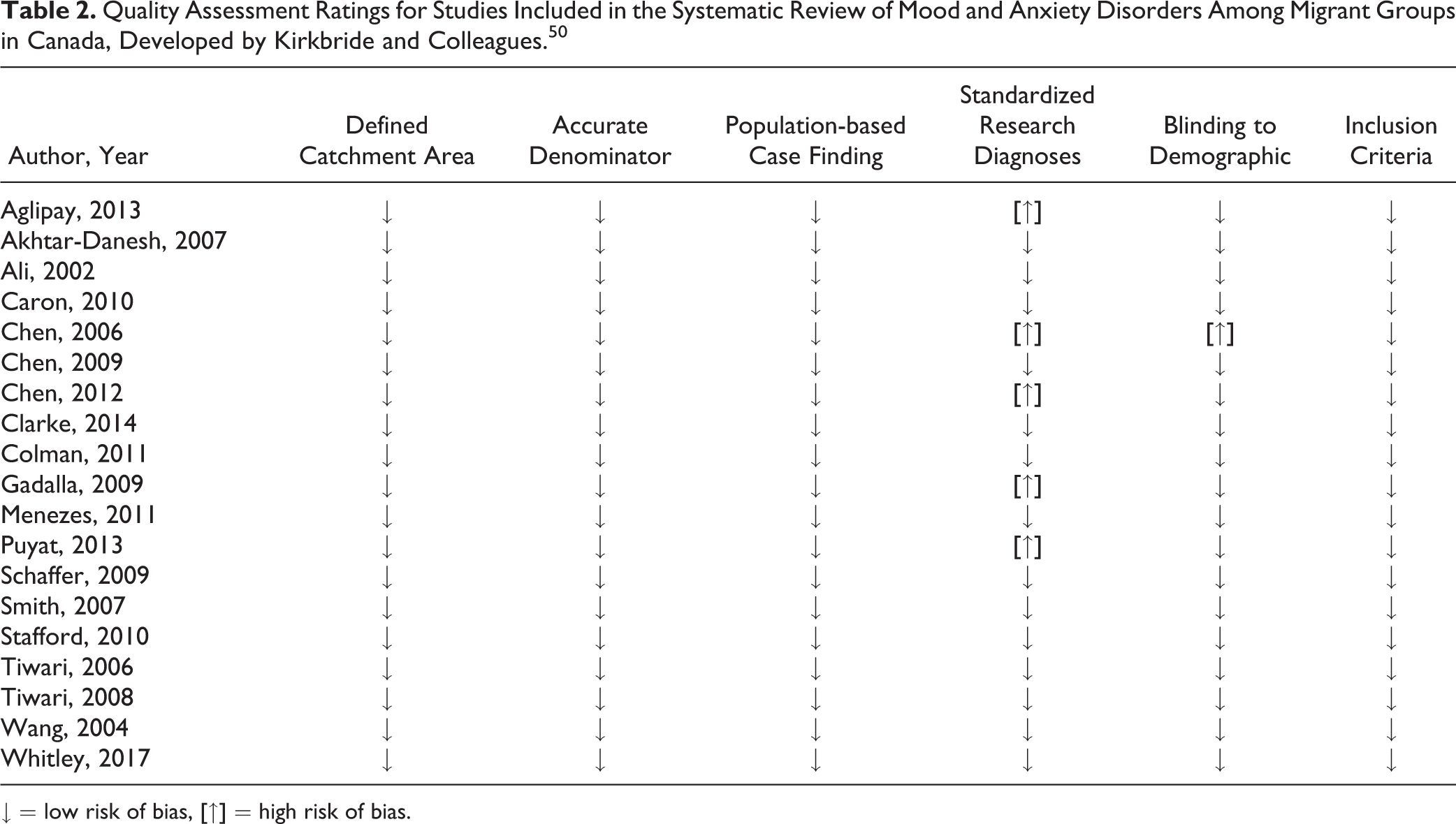
↓ = low risk of bias, [↑] = high risk of bias.
Overall Estimates of Mood and Anxiety Disorders
Reported prevalence estimates for mood and anxiety disorders among migrant populations ranged from 1.5% to 32.6%, with the 90th percentile of studies ranging from 1.5% to 8.2%. All of the included studies provided information to calculate prevalence ratios, and none of the included studies provided incidence data to calculate risk ratios. The prevalence ratios from the included studies ranged from 0.48 to 0.87 (Figure 2). Finally, the symmetrical appearance of the funnel plot suggested that there was no evidence of publication bias (Appendix S5). The results of the Egger’s test were non-significant (p = 0.295) indicating no statistical evidence of publication bias.
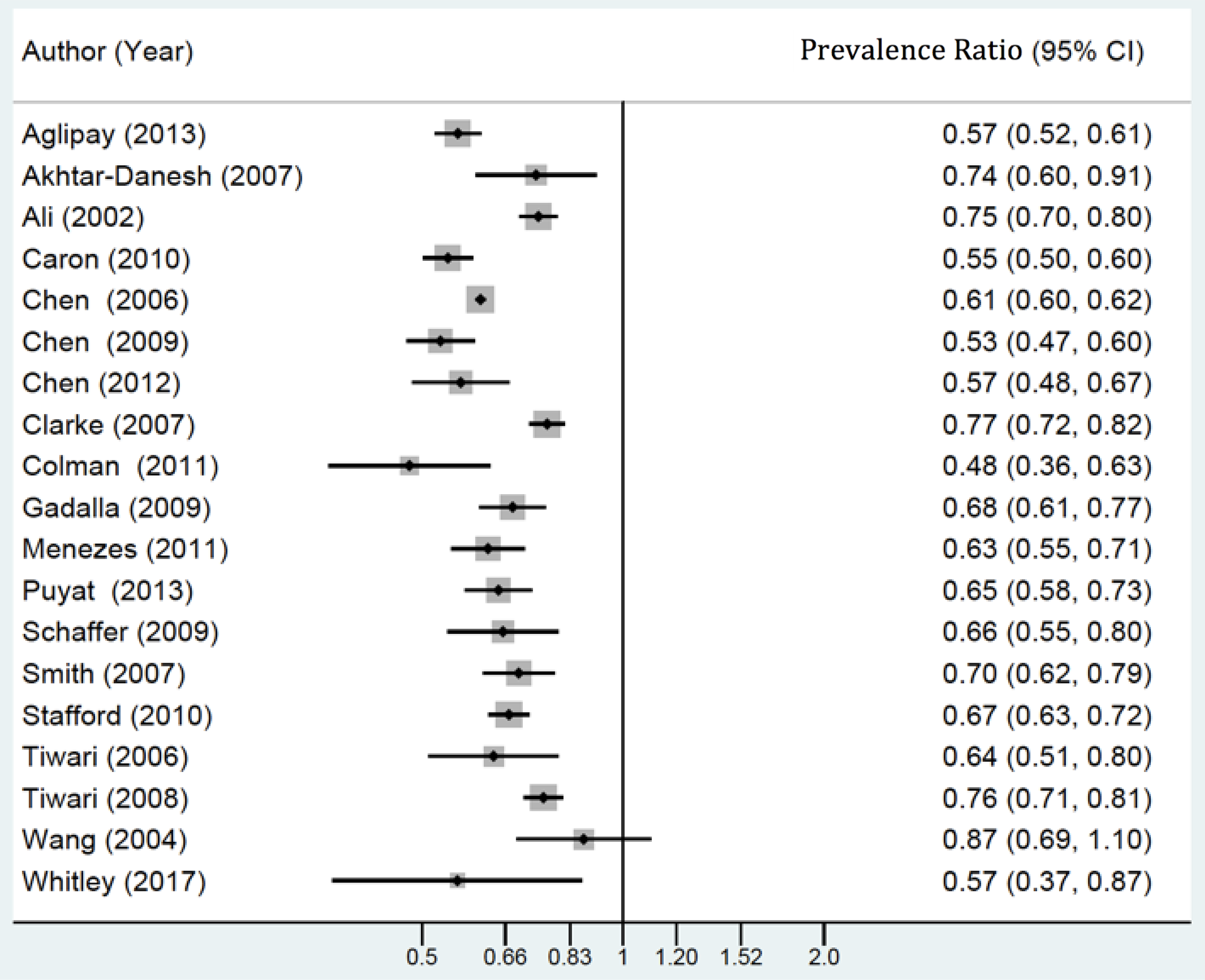
Prevalence ratios of mood and anxiety disorders among migrant groups, and Canadian-born/long-term resident comparison groups.
Risk Factors for Mood and Anxiety Disorders among Migrant Groups
Gender and Age: Three studies presented various adjusted and stratified prevalence ratios, taking into consideration gender and age.
19,40,43
Estimates were consistently higher for females and for younger migrants in both unadjusted and adjusted estimates. For example, the OR for women compared with men, after adjusting for other socio-demographic characteristics, was 1.47 (95% CI = 1.32 to 1.62) for mood disorders and 1.62 (95% CI = 1.45 to 1.80) for anxiety disorders.
43
Employment, Income, Education, Language, Marital Status: Three studies provided prevalence estimates among migrant groups considering risk factors of employment, income, education, and language.
21,40,43
Employment, higher income, understanding of English or French language, and being married were each shown to be protective against mood and anxiety disorders in 3 studies,
21,40,43
whereas one study did not find a protective effect for education.
40
Years in Canada, Neighbourhood Migrant Concentration, and Neighbourhood Disadvantage Factor: Five studies provided information on the relationship between length of time in Canada and mood and anxiety disorders among migrant groups.
18,34,37,38,43
Two studies provided information on the relationship between neighbourhood migrant concentration, and neighbourhood disadvantage factor and mood and anxiety disorders among migrant groups.
18,43
Recent migrant groups (less than 10 y in Canada) had consistently lower estimates of mood and anxiety disorders compared with long-term migrant groups (more than 10 y in Canada).
18,34,37,38
This is reinforced in the analysis by Menezes et al., which identified a higher odds of having a mood or anxiety disorder with increasing years in Canada among all age groups, except for people over the age of 60 y.
43
There was also evidence that an increase in neighbourhood migrant concentration had a protective effect against depression among migrants. A 10% increase in the proportion of migrant residents in a neighbourhood was associated with a 10% decrease in the odds of depression (95% CI = 0.84 to 0.95).
43
Finally, a neighbourhood disadvantage factor was developed by the study investigators and was based on: 1) percent below the low income cut-off, 2) percent rental accommodation, and 3) percent who moved in the last year. There was evidence that higher levels of neighbourhood disadvantage were associated with an increased odds of mood disorders (OR = 1.23; 95% CI = 1.17 to 1.29) and anxiety disorders (OR = 1.15; 95% CI = 1.09 to 1.21).
Discussion
This review provides the first comprehensive synthesis of the Canadian literature on the epidemiology of mood and anxiety disorders among migrant groups. Available evidence suggests that estimates of mood and anxiety disorders are consistently lower among migrant groups compared with Canadian-born/long-term resident comparison groups. Estimates of mood and anxiety disorders among migrants are less consistent across the globe. Similar to our findings, estimates from the US using a nationally representative survey found that first-generation migrants were significantly less likely than native-born Americans to be diagnosed with a mood or anxiety disorder. 6 However, other international estimates have conflicting results; for example the pooled estimate from an international meta-analysis (Sweden, Denmark, UK, Netherlands, Israel, Germany, Australia, and the USA) suggests higher estimates of mood and anxiety disorders among migrant groups, relative to native-born/long-term resident comparison groups. 51 The differences observed across nations may reflect differences in global migrant flows (i.e., migrants entering or leaving given countries), illegal migration, immigration policies, and the availability of post-migration support of new migrants in the host countries. 43,52 Furthermore, differences may reflect variation in the composition of migrant groups within each country, who may differ by socio-economic status and in their distribution of pre- and post-migration risk factors for mood and anxiety disorders. 53,54
Though Canadian estimates are currently limited, there are several reasons why self-reported estimates of mood and anxiety disorders could be lower among migrant groups compared with host-country comparison groups. The first is selective migration, specifically positive migrant selection, where migrants are selected based on skills and education. 55 Canadian immigration policies result in an influx of healthier migrants as compared with the general population. 56 This concept applies primarily to economic class migrants, which make up roughly 50% of new immigrants in Canada. 57 In the current review, we were unable to distinguish estimates of mood and anxiety disorders among migrant classes (economic, family reunification, or refugee). Previous evidence suggests that estimates of mood and anxiety disorders would be higher among refugee groups compared with immigrant groups. 2 Another explanation for the lower estimates of mood and anxiety disorders we observed between migrant and host country groups is cultural differences. Differences in cultural practices, symptomatology, stigma, and diagnostic practices of mood and anxiety disorders may influence whether people are diagnosed with a mood or anxiety disorder, as well as whether they are willing to self-report a mood or anxiety disorder. 53,58 As an example, in Japan, there is a culturally common fear of conducting innapropriate social behaviour called taijin kyofusho (TKS). While this fear may be characterized as an anxiety disorder in a Canadian setting, it may not be seen as unreasonable to the sufferer as it is aligned with cultural values. 58 Present evidence suggests that migrant groups are less likely to seek out or be referred to mental health services, which would result in an underestimation of the prevalence of these disorders. 2,14, Our current Canadian estimates rely heavily on self-reported survey data. Previous Canadian research comparing self-report and diagnosed mood and anxiety disorders found consistently lower self-reported estimates. 59 As these trends may differ by migrant group, further exploration of diagnosed estimates of mood and anxiety disorders among migrant groups in Canadian is warranted.
We found variation in the prevalence estimates of mood and anxiety disorders among migrant groups in Canada. While much of this variation may be due to the definitions of mood and anxiety disorders used to estimate prevalence, another potential source is time since migration. Our findings indicated that more recent migrant groups had lower estimates of mood and anxiety disorders. This trend aligns with the healthy immigrant effect, a phenomenon where migrant groups are shown to be healthier during the early years post-migration, and their health status subsequently worsens to more closely resemble that of the host country. 6 It is important to note that evidence suggests that the healthy immigrant effect does not hold true for refugee groups, who likely have elevated pre-migratory stressors that contribute to elevated mental distress and higher reported mental illness. 6 Most (n = 15) of the included studies did not present information on time spent in Canada or refugee status, and differences between samples may have contributed to the variation we observed.
A key finding of our review, which impacts our ability to both contextualize and translate our results, is that available Canadian data on mood and anxiety disorders among migrant groups are limited to prevalence estimates. Global evidence suggests that Canada is falling behind in its evaluation of the incidence of mood disorders among migrant groups. 51 By considering the temporality and directionality of associations, measures of incidence provide insight into the role of migratory and postmigration experiences on rates of mood and anxiety disorders among migrants in Canada. In contrast, the prevalence estimates currently available in the Canadian literature combine both factors associated with disorder onset and factors associated with its persistence. Of the limited Canadian research that has explored factors associated with mood and anxiety disorders among migrant groups, findings aligned with those of the general Canadian population. 32,43 Findings suggest that female gender, younger age, unemployment status, low education, and being unmarried are all associated with a higher risk of mood and anxiety disorders among migrant groups. 32 Evidence from the US found similar results among Asian Americans. 60 Other risk factors, such as neighbourhood migrant concentration and neighbourhood disadvantage, have not been widely studied among migrant groups. 43 Our results indicate a need to assess and solidify the relationships between key risk factors and mood and anxiety disorders among migrant groups in Canada.
The current body of evidence also highlights the need to broadly explore the factors that may impact the mental health of migrant groups, including factors related to pre-migration, migration, and post-migration, which may influence rates of mental illness. 8,61 This would provide a more nuanced and informative understanding of the relationship between mood and anxiety disorders and migrant groups. Furthermore, there are a number of potentially important correlates related to mood and anxiety disorders that have not been previously explored among Canadian migrant groups, including ethnicity, country of origin, migrant class, and acculturation. 43 More detailed analyses could be conducted by pooling the various waves of CCHS to perform an individual data meta-analysis, as well as linking the CCHS with other administrative databases. Finally, there is a need to enhance our etiological understanding of mood and anxiety disorders among migrant groups. One approach would be to evaluate whether certain mood and anxiety disorders are prone to genetic influence or stress-related factors, taking into consideration epigenetic contributions.
Limitations
We were limited in our ability to conduct subgroup analyses for specific risk factors (e.g., ethnicity, length of time in Canada, country of origin) due to a lack of data in the available literature. We were also limited in our ability to provide meaningful pooled estimates due to the high degree of homogeneity of the secondary data sources included in the review. Although the overall quality of the included studies was high, future research should use standardized diagnoses of mood and anxiety disorders to allow for greater comparability across studies.
There is currently a lack of prospective studies that present estimates of the incidence of mood and anxiety disorders in Canada. Future research should focus on estimating the incidence of these disorders to improve our understanding of mood and anxiety disorders among migrant groups.
Conclusions
We have demonstrated lower prevalence ratios of mood and anxiety disorders among first-generation migrant groups in Canada, relative to Canadian-born comparison groups. This review has identified key gaps in our current understanding of mood and anxiety disorders among migrants in Canada. We have identified a lack of incidence estimates, an over-reliance on cross-sectional and self-reported data, and a need to consider key risk factors, including migrant class, country of origin, neighbourhood migrant concentration, and neighbourhood disadvantage. As migration remains a key feature of the Canadian population and its growth, further research on migrant mental health is warranted.
Supplemental Material
Supplemental Material, Appendix_S1_-_MOOSE - Gaps in Understanding of the Epidemiology of Mood and Anxiety Disorders among Migrant Groups in Canada: A Systematic Review
Supplemental Material, Appendix_S1_-_MOOSE for Gaps in Understanding of the Epidemiology of Mood and Anxiety Disorders among Migrant Groups in Canada: A Systematic Review by Jordan Edwards, Malini Hu, Amardeep Thind, Saverio Stranges, Maria Chiu and Kelly K. Anderson in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, Appendix_S2_-_Search_Strategy_ - Gaps in Understanding of the Epidemiology of Mood and Anxiety Disorders among Migrant Groups in Canada: A Systematic Review
Supplemental Material, Appendix_S2_-_Search_Strategy_ for Gaps in Understanding of the Epidemiology of Mood and Anxiety Disorders among Migrant Groups in Canada: A Systematic Review by Jordan Edwards, Malini Hu, Amardeep Thind, Saverio Stranges, Maria Chiu and Kelly K. Anderson in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, Appendix_S3_-_Exclusion_List - Gaps in Understanding of the Epidemiology of Mood and Anxiety Disorders among Migrant Groups in Canada: A Systematic Review
Supplemental Material, Appendix_S3_-_Exclusion_List for Gaps in Understanding of the Epidemiology of Mood and Anxiety Disorders among Migrant Groups in Canada: A Systematic Review by Jordan Edwards, Malini Hu, Amardeep Thind, Saverio Stranges, Maria Chiu and Kelly K. Anderson in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, Appendix_S4_-_Data_Extraction_Form - Gaps in Understanding of the Epidemiology of Mood and Anxiety Disorders among Migrant Groups in Canada: A Systematic Review
Supplemental Material, Appendix_S4_-_Data_Extraction_Form for Gaps in Understanding of the Epidemiology of Mood and Anxiety Disorders among Migrant Groups in Canada: A Systematic Review by Jordan Edwards, Malini Hu, Amardeep Thind, Saverio Stranges, Maria Chiu and Kelly K. Anderson in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, Appendix_S5_-_Funnel_Plot - Gaps in Understanding of the Epidemiology of Mood and Anxiety Disorders among Migrant Groups in Canada: A Systematic Review
Supplemental Material, Appendix_S5_-_Funnel_Plot for Gaps in Understanding of the Epidemiology of Mood and Anxiety Disorders among Migrant Groups in Canada: A Systematic Review by Jordan Edwards, Malini Hu, Amardeep Thind, Saverio Stranges, Maria Chiu and Kelly K. Anderson in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
We gratefully acknowledge John Costella for his support in creating the search strategy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a New Investigator Fellowship from the Ontario Mental Health Foundation (KKA). This work was also funded by the Internal Research Fund of the Lawson Health Research Institute (KKA).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.