
Abstract
Objectives:
To compare explicit and implicit stigmatizing attitudes towards mental illness among undergraduate students, medical school students, and psychiatrists, and to assess whether attitudes are associated with education level, exposure to, and personal experience with mental illness.
Methods:
Participants from McMaster University were recruited through email. Participants completed a web-based survey consisting of demographics; the Opening Minds Scale for Healthcare Providers (OMS-HC) 12-item survey, which measures explicit stigma; and an Implicit Association Test (IAT), measuring implicit bias toward physical illness (diabetes mellitus) or mental illness (schizophrenia).
Results:
A total of 538 people participated: undergraduate students (n = 382), medical school students (n = 118), and psychiatrists (n = 38). Psychiatrists had significantly lower explicit and implicit stigma than undergraduate students and medical school students. Having been diagnosed with mental illness or having had a relationship with someone experiencing one was significantly associated with lower explicit stigma. Mean scores on the OMS-HC “disclosure/help-seeking” subscale were higher compared with the “attitudes towards people with mental illness” subscale. There was no correlation between the OMS-HC and IAT.
Conclusions:
These findings support the theory that increased education and experience with mental illness are associated with reduced stigma. Attitudes regarding disclosure/help-seeking were more stigmatizing than attitudes towards people with mental illness. The groups identified in this study can potentially benefit from anti-stigma campaigns that focus on reducing specific components of explicit, implicit, public and self-stigma.
Introduction
The 2012 Canadian Community Health Survey-Mental Health (CCHS-MH) showed that approximately 33.1% of Canadians experience a mental or substance-use disorder in their lifetime. 1 Indirectly, mental illness affects all Canadians through their relationships with family, friends, and colleagues. 2 In addition to being a wide-spread phenomenon, individuals with mental illness and those experiencing mental health issues are often subject to stigma, which can result in a great deal of discrimination and negative outcomes. 3
Broadly, stigma refers to negative stereotypes and beliefs held towards a particular topic or group of people. 3 Researchers have studied multiple dimensions of stigma and have developed many theoretical models to explain the processes. 4 Public stigma is the most common form of stigma and involves stereotyping, prejudice, and discrimination against people with mental illness. 4 When individuals become aware of public stigma, agree with it and apply it to themselves, this results in a second form of stigma called self-stigma. 5 This can lead to further harm and be a barrier to accessing aid. 5,6 Researchers and practitioners agree that reducing stigma associated with mental illness is a top priority. 4,7 Another layer in studying stigma is differentiating between explicit and implicit attitudes. 4,8 Explicit attitudes refer to what individuals say to others about their beliefs towards a given topic. 8 Implicit attitudes are internal beliefs individuals hold regardless of what they say or think they believe (out-of-conscious control). 8 Explicit attitudes are generally easier to measure than implicit attitudes and thus have been studied more frequently. 9
Previous work indicates that healthcare providers (HCP) who treat individuals with mental illness may also hold stigmatizing attitudes towards mental illness, which can potentially affect their practice. 9 –11 For example, a study by Peris et al. (2008) examined implicit and explicit stigma among HCPs and showed that both were associated with negative patient prognoses and that implicit stigma in particular was associated with over-diagnosis. 8 Another study showed that HCPs with implicit stigma were associated with greater restrictive or controlling clinical interventions for patients with mental illness. 6 It is crucial to continue studying implicit and explicit attitudes held by different groups, such as HCPs, as it can drastically affect care.
Moreover, there is limited research on comparing stigmatizing attitudes between different groups with varying levels of knowledge and experience, and the need to further explore this has been noted. 7,9,12 In an effort to reduce stigma, the Mental Health Commission of Canada has identified several groups that are considered a top priority for intervention: undergraduate students, medical school students, and psychiatrists. 13 Studying these groups in regards to explicit and implicit attitudes, as well as components of public and self-stigma, may reveal differences that can further develop the conceptual framework of stigma and inform future anti-stigma programs.
The objective of this study was to explore stigma in terms of explicit and implicit attitudes as well as factors of public and self-stigma among undergraduate students, medical school students, and psychiatrists. It was hypothesized that psychiatrists and individuals with more education, exposure, and experience with mental illness would have less stigmatizing attitudes.
Methods
Ethical Considerations
The study was approved by the Hamilton Integrated Research Ethics Board (Project ID: 1786). Participant consent was obtained before completing the study.
Study Population
Three groups were studied: undergraduate students, medical school students, and psychiatrists (including psychiatric residents) associated with McMaster University. Undergraduate students were recruited from the School of Business, and the Faculties of Engineering, Health Sciences, Science, and Social Sciences. Medical school students were recruited from the Michael G. DeGroote School of Medicine. Psychiatrists with a full or part-time academic appointment and psychiatric residents were recruited from the Department of Psychiatry and Behavioural Neurosciences.
Sample Size Calculation
There were an estimated 26,780 undergraduate students, 609 medical school students, and 142 psychiatrists and psychiatric residents. 14 SurveyMonkey’s sample size calculator was used to estimate required sample sizes, based on previously published methods. 15,16 Using a 95% confidence level and 5% margin of error, we estimated 379, 236, and 104 desired participants for each respective group to achieve a representative sample.
Recruitment
Multiple email invitations (∼3) were sent to all potential participants through departmental administrators over a 6-wk period. Participants followed a link to a webpage that described the study and were instructed to complete the study on a computer or laptop. Data collection occurred from January 23 to April 17, 2017. SurveyMonkey prevented the same computer IP address from accessing the survey more than once.
Survey
Our study comprised 3 sections: (1) demographics; (2) Opening Minds Scale for Healthcare providers (OMS-HC) shortened 12-item version; and (3) Implicit Association Test (IAT). The demographics questionnaire and OMS-HC were developed in SurveyMonkey and the IAT was created using the Millisecond Inquisit programme. 17 A 4-digit ID number connected participants between the 2 datasets. Following completion of the IAT, participants were directed to a SurveyMonkey webpage with links to websites containing information about mental health, mental illness, stigma, and the Opening Minds initiative. 13,18 –20 Participants who completed the study were also given an opportunity to enter their email address for a chance to win one of four $25 giftcards. These data were stored separately from the study information to ensure anonymity.
Demographics Questionnaire
The demographics questionnaire collected information regarding sex, self-reported mental illness, diagnosed mental illness, and close relationship with someone experiencing a mental illness.
Opening Mind Scale for Health Care Providers (OMS-HC)
The OMS-HC measures explicit stigmatizing attitudes of health care professionals regarding mental illness. 9,21,22 The shortened 12-item OMS-HC was used to offset response burden and increase feasibility of use by busy populations. 21 The OMS-HC has 2 subscales: (1) attitudes towards “disclosure/help-seeking” and (2) “attitudes toward people with mental illness”. Two items were slightly modified to increase relevance to undergraduate students. Item 3 was modified to include “university” (i.e. “I would be more inclined to seek help for a mental illness if my treating health care provider was not associated with my workplace/university”). Similarly, Item 9 was altered to include “peers” (“If I were under treatment for a mental illness I would not disclose this to any of my colleagues/peers”). This shortened scale has been validated to be as consistent as the full scale, with an acceptable internal consistency (Cronbach’s alpha = 0.78). 21 Each item requires a response on a 5-point Likert scale (strongly disagree = 1, strongly agree = 5). Item 12 was reverse scored, and all items were summed to give explicit attitudes scores for each participant. A higher score indicated greater stigma.
Implicit Association Test (IAT)
The IAT is a computer-based cognitive-behavioural association test that assesses the strength of implicit attitudes by comparing the amount of time it takes to categorize attributes. 23 There is support that the IAT can be used to measure associations and has predictive validity. 24,25 Our study used the Millisecond Inquisit programme (v5.0) to develop an IAT comparing the implicit biases between mental (schizophrenia) and physical (diabetes mellitus) illness. 17 This involved presenting attribute categories on either side of the computer screen (“Good” or “Bad”) paired with a target category (“Schizophrenia” or “Diabetes mellitus”). Participants were required to quickly categorize the attributes (e.g., “Love”, “Awful”) and targets (e.g. “Hallucinations”, “Insulin”) that appear in the middle of the screen into corresponding sides of the screen using their computer keyboard. The quicker participants did this, the stronger that association was in their memory. 23 The categories were presented in a randomized manner to decrease order and anticipation effects. 26 Upon completing the IAT, each participant was provided with a D-score and its interpretation. 27 A negative D-score indicated a bias towards the mental illness, or an absence of stigma, whereas a positive D-score indicated a bias towards the physical illness, or the presence of stigma. A large D-score indicated a stronger association. 27 The IAT structure and details can be found in Appendix A.
Data Analysis
Only data from participants who completed all 3 sections of the study were included and data were analyzed using IBM SPSS Statistics v25. Descriptive statistics and bivariate analyses were performed to determine associations among the demographic variables, OMS-HC, and IAT scores. A Shapiro-Wilk test and visual inspection of normal Q-Q plots determined if the data were normally distributed. Pearson’s r for parametric variables was used to determine bivariate relationships between predictors (demographics) and dependent variables (OMS-HC and IAT scores). Independent and paired samples t tests were used to compare groups as well as one-way ANOVA for groups. Cohen’s d effect size was calculated for t tests and eta squared (ω2) for one-way ANOVA. Multiple linear regression was used to determine an association for demographic variables with OMS-HC and IAT scores. The psychiatric resident sample (n = 16) and psychiatrists sample (n = 22) were combined to increase power and because they were similar in terms of the characteristics assessed. All P-values reported are 2-tailed, with significance level at 0.05.
Results
Demographics
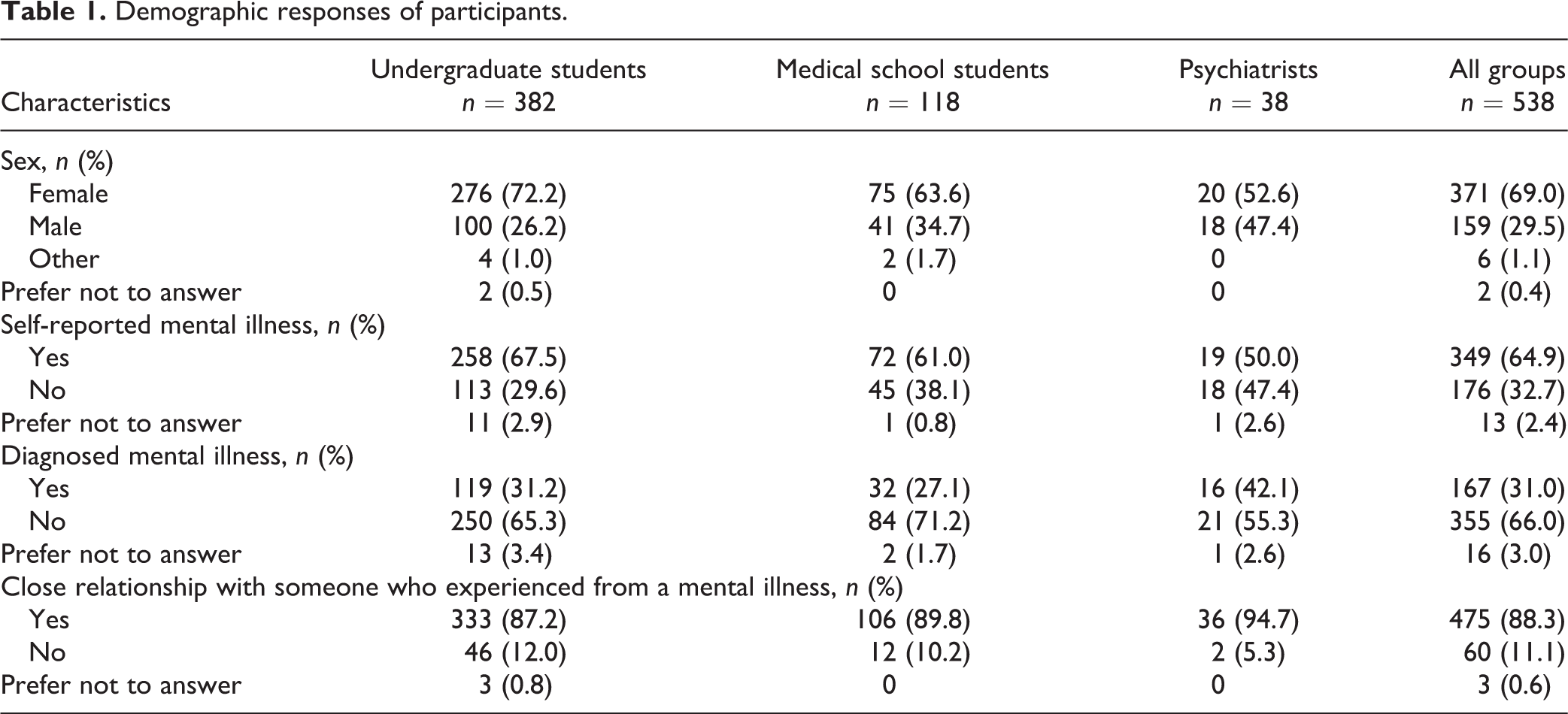
A total of 837 people viewed the survey webpage and 538 completed all 3 sections (completion rate of 64.3%). Demographic responses are summarized in Table 1. Most of the sample was female (69.0%), and 64.9% of participants self-reported having experienced a mental illness, whereas only 31% reported having been diagnosed with a mental illness by a HCP. Of the total sample, 88.3% had a close relationship with someone who experienced mental illness. The only significant correlation among demographic variables was between self-reported mental illness and having been diagnosed with a mental illness (r = 0.49, P < 0.001). All other correlations were non-significant or below r = 0.30 and are not reported. 28
Demographic responses of participants.
Explicit Attitudes
Normal Q-Q plots and Shapiro-Wilk tests showed that OMS-HC scores were normally distributed for undergraduate students (W = 0.99, P = 0.125), medical school students (W = 0.98, P = 0.083), and psychiatrists (W = 0.97, P = 0.324). The internal consistencies of the subscales were questionable (Cronbach’s alpha = 0.65 for “disclosure/help-seeking” and 0.66 for “attitudes towards people with mental illness”). Each subscale had an item (item 2 and 3, respectively) with low item-total correlation (r < 0.20). The internal consistencies were acceptable with these items removed (Cronbach’s alpha = 0.71 and 0.70, respectively).
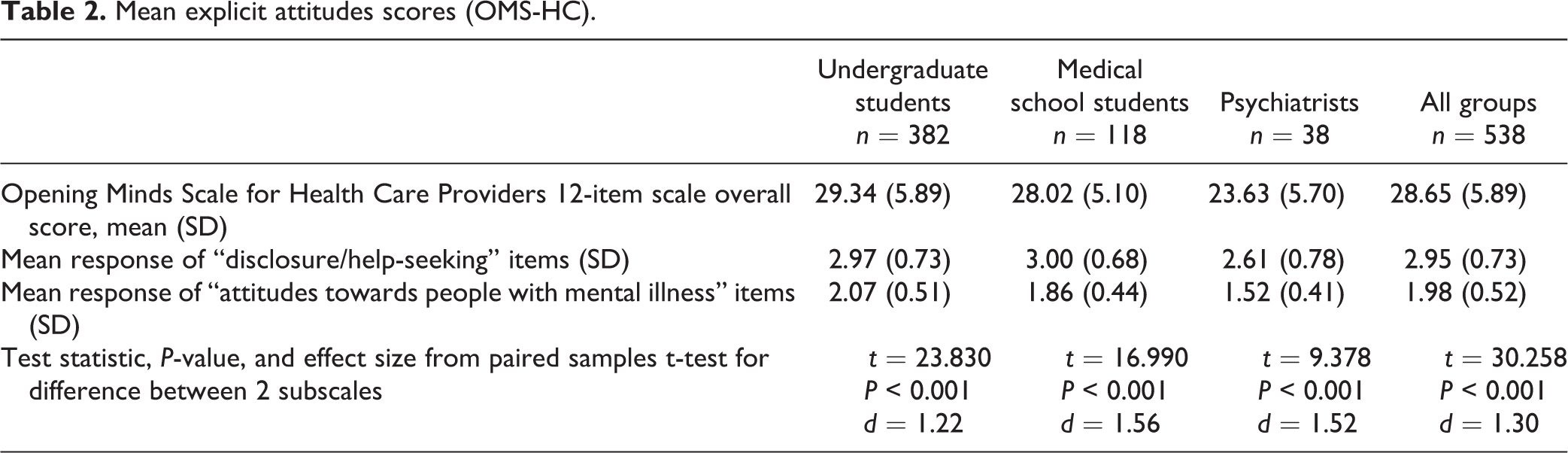
One-way ANOVA (F = 18.21, df = 2/535, P < 0.001, ω2 = 0.06) and post-hoc Tukey’s HSD showed that explicit stigma scores for psychiatrists (M = 23.63, SD = 5.70) were significantly lower than that for undergraduate students (M = 29.34, SD = 5.89, P < 0.001) and medical school students (M = 28.02, SD = 5.10, P < 0.001); the undergraduate and medical school students did not differ (P = 0.071).
The mean “disclosure/help-seeking” response (M = 2.95, SD = 0.73) was significantly higher than the mean “attitudes towards people with mental illness” response (M = 1.98, SD = 0.52) for all groups (P < 0.001, d = 1.30, see Table 2). One-way ANOVA and post-hoc Tukey’s HSD showed that, for the “disclosure/help-seeking” subscale (F = 4.78, df = 2/535, P = 0.009, ω2 = 0.02), psychiatrists had a significantly lower mean score than undergraduate students (P = 0.008) and medical school students (P = 0.010) and the latter 2 groups did not differ (P = 0.932). For the “attitudes towards people with mental illness” subscale (F = 26.62, df = 2/535, P < 0.001, ω2 = 0.09), psychiatrists again had a significantly lower mean score than undergraduate students (P <0.001) and medical school students (P = 0.001); however, medical school students also had a lower mean score than undergraduate students (P < 0.001).
Mean explicit attitudes scores (OMS-HC).
An independent samples t-test showed that the mean OMS-HC score was significantly lower (P < 0.001, d = 0.34) for those who had been diagnosed with a mental illness (M = 27.33, SD = 5.96) compared with those who were not (M = 29.30, SD = 5.78). The mean OMS-HC score was also significantly lower (P < 0.001, d = 0.55) for those who had a close relationship with someone experiencing from a mental illness (M = 28.25, SD = 5.83) v. those who did not (M = 31.35, SD = 5.39). There were no significant differences in explicit scores between sexes and those who did or did not self-reported having experienced mental illness.
Implicit Attitudes
Normal Q-Q plots and Shapiro-Wilk tests revealed that IAT scores were normally distributed for undergraduate students (W = 1.00, P = 0.564) and psychiatrists (W = 0.97, P = 0.333) but not for medical school students (W = 0.97, P = 0.006). The medical school students group had one outlying data point which was removed and the Shapiro-Wilk test was performed again (W = 0.99, P = 0.864). Because the rest of the data were normal, analyses were completed including this data point. Mean IAT scores were 0.27 (SD = 0.47) for undergraduate students, 0.33 (0.43) for medical school students, and 0.06 (0.43) for psychiatrists. A one-way ANOVA was significant (F = 5.02, df = 2/535, P = 0.007, ω2 = 0.02) and post-hoc Tukey’s HSD test showed that psychiatrists had a lower IAT score than that for undergraduate students (P = 0.017) and medical school students (P = 0.005); the latter 2 groups did not differ (P = 0.482). There were no significant differences in IAT scores among other demographic variables.
Prediction and Correlation of Explicit and Implicit Scores
Multiple regression analysis showed that group (P < 0.001), diagnosed mental illness (P = 0.002), and close relationship with someone experiencing a mental illness (P = 0.002) were significant predictors of OMS-HC scores (r = 0.31, P < 0.001) (Table 3). No variables or models were significant in predicting IAT scores. There was negligible correlation of r = 0.11 (P = 0.013) for all groups between OMS-HC and IAT scores. Correlation between the “disclosure/help-seeking” subscale and IAT (r = 0.04, P = 0.312), and “attitudes towards people with mental illness” subscale and IAT (r = 0.13, P = 0.002) were also negligible. The 2 OMS-HC subscales were weakly correlated (r = 0.33, P < 0.001).
Regression output for OMS-HC scores (r = 0.31, P < 0.001).

Discussion
Psychiatrists were expected to have significantly lower scores of explicit stigma than the other groups, similar to previous findings among Canadian HCPs. 9,21 It is surprising, however, that there were only minor differences between the medical school and undergraduate students. Furthermore, on the explicit stigma scale, scores were significantly lower for diagnosed mental illness or those who had a close relationship with someone experiencing a mental illness. This can be explained by the theory that people who have more personal experience have less stigmatizing explicit attitudes than those who do not. 22
Previous research has shown that receiving a diagnosis of a mental illness may increase stigma through labelling of an individual. 29,30 However, this study showed that having been diagnosed with a mental illness was significantly associated with decreased explicit stigma whereas self-reported mental illness was not. The relationship between being diagnosed with mental illness and lower explicit stigmatizing attitudes is unclear and difficult to explain in this cross-sectional study design. It is possible that individuals with existing lower explicit stigmatizing attitudes were more likely to seek treatment and receive a diagnosis. Stigma may have been a barrier to treatment-seeking and diagnosis for those who self-reported but were not diagnosed. Overall, our findings suggest that structured contact-based education interventions aiming to increase an individual’s exposure mental illness may effectively reduce stigmatizing attitudes in these populations. This approach has been widely endorsed by researchers and has been shown to be effective. 31 –36 It is important to note, however, that implicit attitudes are much harder to change and may not be affected by simple contact-based interventions. 37 –40
We found that “disclosure/help-seeking” scores were significantly higher than mean “attitudes toward people with mental illness” scores, similar to previous findings by Kassam et al. 21 Negative attitudes towards disclosure and help-seeking can lead to negative consequences and if an individual applies these attitudes to themselves and their behaviour, it could lead to self-stigma. 2 Previous studies have shown that self-stigma was significantly associated with help-seeking behaviour but public stigma was not. 41,42 Although the medical school students and undergraduates did not differ on the “disclosure/help-seeking” subscale, medical school students had significantly lower stigma on the “attitudes towards people with mental illness” subscale. It is possible that medical school assists in changing attitudes and that public stigma may be easier to change than self-stigma.
IAT scores were lowest for psychiatrists and did not differ between undergraduate students and medical students, consistent with explicit stigma. This absence of IAT and OMS-HC correlation is consistent with previous findings. 8,9,37,43 –45 The lack of standardization of setting (e.g., home, hospital, university) and equipment (e.g., computer, laptop) for completing the IAT may have contributed to the variability of the results. The absence of a correlation could also be due to the IAT and OMS-HC measuring different concepts. 45 The OMS-HC assessed general explicit stigmatizing attitudes whereas the IAT focuses on an individual’s preference of categorizing diabetes mellitus or schizophrenia as good or bad. It is also possible that participants blamed those with diabetes (particularly type 2) and schizophrenia as self-inflicted, further distinguishing the IAT from the OMS-HC.
The percentage of participants who reported having experienced a mental illness was 64.9%; yet, only 31.0% of participants had a history of diagnosis by a HCP. The 2012 CCHS-MH lifetime prevalence of a mental or substance-use disorder is 33.1%. 1 Other sources have estimated the lifetime prevalence of mental illness to be 50.0%. 46,47 Although there is no consensus for mental illness prevalence, the percent of participants that self-reported experiencing a mental illness was higher than expected. This may be due to the overly broad definition of mental illness in this study: “health conditions that are characterized by alterations in thinking, mood, or behaviour associated with significant distress and/or impaired functioning”. 48 The growing openness and discussion about mental illness, especially in a university setting, may also explain this high rate; however, this does not explain why substantially less participants reported having been diagnosed by a HCP. To our best understanding, there are no published studies comparing the rate of diagnosis to self-reported mental illness. Determining the reason for this difference and what role stigma plays might be a potential area for future research.
Limitations
Although sample size for undergraduate students (n = 382) was adequate, the medical school students (n = 118), psychiatric residents (n = 16) and psychiatrists (n = 22) samples were small. The latter 2 groups were combined post hoc (n = 38) to increase power. Subjects in this new group were likely to be similar in terms of experience, training, and exposure, as shown before. 9 Still, since 2 of the 3 samples were low, the study was underpowered and the results should be interpreted with caution. We did not collect information on the type of settings in which the psychiatrists practiced or the mental illnesses they treated, and it is possible that these differences may have affected the results of the OMS-HC and IAT.
Undergraduate student recruitment may have been biased because some departments were more interested in assisting with recruitment than others. The recruitment email invited participants to take part in a “Mental Health Attitudes” study. The word “stigma” was avoided with the intent of reducing sampling bias because individuals may have been more likely to participate if they had a pre-existing interest in stigma.
After accessing the survey, only 64.3% of participants went on to fully complete all 3 sections. It is possible that transitioning to the Millisecond website was a barrier. The variability in the IAT scores could be attributed to the intensive, time-pressed nature of the test, which may not be conducive to people who were trying to complete the test in a busy environment or in a situation where they could not fully focus. Furthermore, the IAT only measured attitudes towards schizophrenia and diabetes mellitus. These disorders are not representative of all mental and physical illnesses but were rather an example of each. As with any self-reported measure, there is always the possibility for self-reporting bias. We emphasized the anonymity of the survey and allowed participants to complete the survey on their own time and using private computers to address this bias.
Conclusion
Psychiatrists have significantly lower explicit and implicit stigma than undergraduate and medical school students. Factors associated with lower explicit stigma included history of mental illness diagnosis or close relationship with someone who experienced a mental illness. Attitudes towards disclosure and help-seeking were more stigmatizing than attitudes towards people with mental illness. Medical school students had better explicit attitudes towards people with mental illness than undergraduate students but the same attitudes towards disclosure/help-seeking, highlighting a potential area for stigma reduction. Although psychiatrists scored well on the concepts of stigma studied, it is possible that their attitudes may differ for other factors related to stigma, such as social distance, discrimination, among others, and therefore a multi-component stigma reduction strategy is still recommended. The proportion of participants who self-reported having experienced a mental illness was much higher than those who reported being diagnosed, and this opens a new area for further research especially in determining how stigma may explain this difference. If this difference is true for the general public then greater effort must be taken to ensure that those who feel like they are experiencing a mental illness are able to get the help they need.
Footnotes
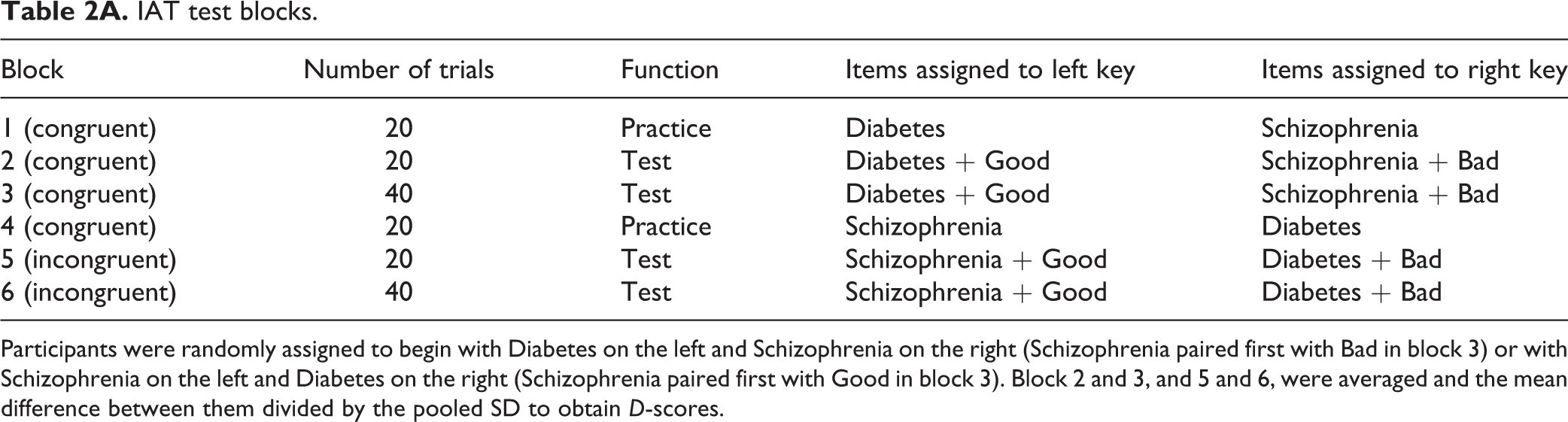
Appendix A. Structure of Implicit Association Test (IAT). Derived from Dabby et al. (2015). 9
IAT test blocks.
| Block | Number of trials | Function | Items assigned to left key | Items assigned to right key |
|---|---|---|---|---|
| 1 (congruent) | 20 | Practice | Diabetes | Schizophrenia |
| 2 (congruent) | 20 | Test | Diabetes + Good | Schizophrenia + Bad |
| 3 (congruent) | 40 | Test | Diabetes + Good | Schizophrenia + Bad |
| 4 (congruent) | 20 | Practice | Schizophrenia | Diabetes |
| 5 (incongruent) | 20 | Test | Schizophrenia + Good | Diabetes + Bad |
| 6 (incongruent) | 40 | Test | Schizophrenia + Good | Diabetes + Bad |
Participants were randomly assigned to begin with Diabetes on the left and Schizophrenia on the right (Schizophrenia paired first with Bad in block 3) or with Schizophrenia on the left and Diabetes on the right (Schizophrenia paired first with Good in block 3). Block 2 and 3, and 5 and 6, were averaged and the mean difference between them divided by the pooled SD to obtain D-scores.
Acknowledgements
The authors would like to thank all of the participating departments in assisting with the recruitment of participants.
Data Access
All data used in this research are stored and maintained by the corresponding author. Those interested in accessing the data can contact the corresponding author for further details.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant from the Department of Psychiatry and Behavioral Neurosciences, McMaster University.