
Abstract
Background:
Major depression is prevalent, impactful, and treatable in military populations, but not all depressed personnel seek professional care in a given year. Care-seeking patterns (including the use of primary vs. specialty care) and factors associated with the likelihood of mental health service utilization in depressed military personnel are poorly understood.
Methods:
Our sample included 520 Regular Force respondents to the 2013 Canadian Forces Mental Health Survey. All study participants had past-year major depression. Subjects reported whether they had spoken about their mental health with at least one health professional in the past 12 months. We used multivariate Poisson regression to explore factors associated with past-year mental health service use.
Results:
Three-quarters of Canadian military personnel with past-year depression had sought mental health care in the previous 12 months. Among care-seeking personnel, 70% had seen a psychologist or psychiatrist, while 5% had exclusively received care from a primary care physician. Belief in the effectiveness of mental health care was the factor most strongly associated with care seeking. Female gender, functional impairments, and psychiatric comorbidities were also associated with care seeking. Surprisingly, stigma perceptions had no independent association with care seeking.
Conclusions:
The proportion of depressed Canadian Armed Forces personnel who seek professional care and who access specialty mental health care is higher than in most other populations. However, an important minority of patients are not accessing health services. Efforts to further increase mental health service utilization in the Canadian military should continue to target beliefs about the effectiveness of mental health care.
Major depression is the most common mental disorder in the Canadian Armed Forces 1 ; annually, 8% of their personnel suffer from a major depressive episode, compared to 4% of carefully matched Canadian civilians. 2 A disproportionate risk of major depression has also been reported in military personnel from Australia, the United Kingdom, and the United States. 3 –5 In the Canadian Armed Forces, major depression is identified as the primary cause of medical release from military service in 150 individuals per year. 6
There are numerous effective treatment options for major depression. 7,8 Unfortunately, many adults with major depression never seek professional care and therefore cannot benefit from effective treatment. 9 In 2002, a telephone survey of 304 community-dwelling Canadian adults with probable major depression estimated that only 56% had sought mental health care in the past year. 9 Similarly, a 2002 survey of 8441 Canadian military personnel estimated that only 37% of those with a lifetime history of major depression had sought mental health care within 12 months of depressive symptoms onset. 10 Furthermore, a longitudinal study of over 22,000 US infantrymen found that, from 2003 to 2011, the annual prevalence of past-year mental health service utilization among depressed soldiers only ranged from 20% to 42%. 11
Most military personnel with untreated mental disorders do not recognize the need for professional help. 12 Among depressed patients who recognize the need for help, the failure to receive timely care could be explained by any combination of factors from 3 broad treatment barrier categories: availability barriers (e.g., services not available locally), accessibility barriers (e.g., services too expensive), and acceptability barriers (e.g., stigma). 10,13 Since the early 2000s, the Canadian Armed Forces have made substantial investments to renew their mental health system, by establishing novel treatment centres and prevention programs, doubling the number of their mental health clinicians, and intensifying screening efforts for common mental disorders. 14 As a result, availability and accessibility barriers should now have little impact on members of the Regular Forces, who are entitled to free and unlimited mental health care through the Canadian Forces Health Services, as well as transportation to and from treatment centres as required. 15 Nevertheless, acceptability barriers remain a concerning issue; a recent study found higher mental health stigma in the Canadian military than in a comparable civilian population. 16
Previous research has identified several factors associated with increased likelihood of care seeking in patients with mental health disorders, including female sex, 17 older age, 17 marital status, 17 high education status, 18 comorbid disorders, 17 severity of psychiatric symptoms, 18 and awareness of treatment history in family members and friends. 19 In military populations, high levels of social support, 20 previous military deployment, 21 overcoming perceived stigma, 20 and positive attitude toward mental health treatment 22 have also been associated with increased likelihood of mental health service utilization. However, the association between each of these factors and the health service utilization of depressed patients, in the context of recent Canadian Armed Forces mental health initiatives, 14 remains unclear.
In civilian populations, depressed patients who seek care are often treated exclusively in primary care settings. 23 Previous studies have shown that, in general, depressed patients receive more adequate care when they are treated by mental health specialists than by primary care physicians alone. 24,25 High-quality measurement-based care can, however, be provided to depressed patients by primary care physicians, and when treatment adheres to best-practice guidelines, patient outcomes are identical between primary care and specialty mental health settings. 26 Unfortunately, primary care physicians often lack the time and resources required to provide guideline-concordant treatments to their depressed patients. 25,27 Indeed, major depression is often missed or misdiagnosed in primary care settings. 28 Furthermore, primary care physicians tend to treat their depressed patients with pharmacotherapy alone, rather than a combination of pharmacotherapy and psychotherapy, even when there are mental health specialists on site. 29
The objectives of this study were to 1) estimate the prevalence of past-year mental health service use in Canadian Armed Forces personnel who had had a major depressive episode over the same time period, 2) estimate the proportion of care-seeking personnel who were treated by mental health specialists, and 3) identify correlates of care-seeking behaviour.
Methods
Data Source
We used data from the Canadian Forces Mental Health Survey, conducted by Statistics Canada in 2013. 14 Briefly, a random sample was selected from a sampling frame of over 72,000 Canadian Armed Forces personnel. Trained Statistics Canada interviewers then conducted face-to-face, computer-assisted interviews with 6996 Regular Force members (80% response rate) and 1469 reservists (79% response rate).
Study Sample
Regular Force personnel are full-time service members and receive complete medical coverage from the Canadian Forces Health Services. On the other hand, Reservists are mostly part-time personnel and are usually only eligible to receive care through the Canadian Forces Health Services for medical issues directly related to their military service. We therefore only included Regular Force personnel in our sample, because availability and accessibility should not vary within this subpopulation.
We further restricted our sample to personnel with past-year depression (8% of all Regular Force members 1 ), as identified using the World Health Organization (WHO) CIDI 3.0 structured interview. This fully structured diagnostic interview can be administered by lay personnel and is based on International Classification of Diseases, Tenth Revision (ICD-10) and fourth edition of the Diagnostic and Statistical Manual of Medical Disorders (DSM-IV) diagnostic criteria. 30 It is a valid tool for measuring past-year mood disorders. 31
Our study sample therefore consisted of 520 survey participants, weighted to represent 5120 Regular Force personnel with past-year depression.
Past-Year Mental Health Care Seeking
Using a single item from the WHO CIDI 3.0 module on health services use, all participants were asked if they had talked about their “emotions, mental health, or use of alcohol or drugs” to a psychiatrist, family doctor, general practitioner, psychologist, nurse, social worker, and/or counsellor in the past 12 months. Participants who responded positively to this item were classified as having sought mental health care in the past year. We further categorized care seekers as having sought care from a primary care physician (family doctor or general practitioner), mental health specialist (psychiatrist or psychologist), and/or other care provider (nurse, social worker, or counsellor).
Perceived Need for Mental Health Care
Using a single item from the WHO CIDI 3.0 module on health services use, all participants were asked if there was ever a time in the past 12 months when they felt they needed help for their “emotions, mental health, or use of alcohol or drugs” but did not receive it. Non–care seekers who responded positively to this item were considered to have perceived the need for mental health care.
Demographic Information
The survey collected information on the sex, age group (i.e., 18-29 years, 30-39 years, or 40-60 years), marital status (i.e., married/common-law, widowed/separated/divorced, or single), and service element (i.e., Navy, Army, or Air Force) of each participant. Participants were also asked if they had ever deployed in support of Canada’s combat mission to Afghanistan.
Comorbid Psychiatric Conditions
The WHO CIDI 3.0 structured interview, 30 described above, was also used to measure past-year posttraumatic stress disorder (PTSD), general anxiety disorder, panic disorder, and alcohol use disorder. Our analyses adjusted for past-year PTSD—a disorder that disproportionately affects military personnel, especially those who have deployed in support of a combat mission 32 —and any other past-year mental health disorder as 2 dichotomous variables.
Functional Impairment Level
The Sheehan Disability Scale 33 was used to measure the functional impairment of depressive symptoms across 5 domains. Using a 10-point scale, participants reported how much their feelings of depression had interfered with their ability to 1) assume family responsibilities, 2) attend school, 3) work, 4) form and maintain close relationships, and 5) engage in social activities over the past 12 months. As recommended by previous authors, 33 scores were categorized as no impairment (score = 0), mild impairment (score = 1-3), moderate impairment (score = 4-6), marked impairment (score = 7-9), or severe impairment (score = 10) for each of the 5 domains. The highest impairment level reported by each participant was retained for our analysis.
We also computed the mean impairment score across all applicable life domains for each individual. Mean scores ranged from 0 to 10 and were categorized into 1 of 5 impairment levels, as described above. Sensitivity analyses using mean impairment scores yielded highly concordant results to those of primary analyses using maximum impairment scores; for brevity, results of these sensitivity analyses are not presented herein.
Social Support
Social support was measured using a modified version of the Social Provision Scale. 34 Using a 4-point scale, participants were asked to rate their endorsement of 10 items such as “there are people I can depend on to help me if I really need it” and “I feel a strong emotional bond with at least one other person.” Ratings were summed into a total score ranging from 10 to 40. For the purposes of our study, we categorized scores into quartiles.
Awareness of Treatment History in Family and Friends
Participants who reported that a close family member or a close friend had “ever been treated for an emotional or mental health problem” were considered aware of mental health treatment history in family or friends.
Mental Health Treatment Barriers
All participants were asked if they felt that 1) their military unit leaders would encourage them to use mental health services, if ever they needed care; 2) they would be seen as weak if ever they sought mental health care; 3) they could get time off work if ever they needed mental health treatment; 4) seeking mental health care would harm their military career; and 5) treatments would be effective if ever they experienced a mental health problem. Response options included “strongly agree,” “agree,” “neither agree nor disagree,” “disagree,” and “strongly disagree.” Each of the 5 treatment barriers listed above was operationalized as a dichotomous variable, with “strongly agree” and “agree” responses considered as positive endorsement of the survey item.
Analyses
We estimated the proportion of Regular Force personnel with past-year depression who had sought mental health care in the past 12 months. Using purposeful selection methods, 35 we fitted 15 bivariate Poisson regression models to describe the association between past-year mental health care seeking and each of the 15 independent variables described above and listed in Table 1. Significant variables at the α = 0.25 level were added to a multivariate Poisson model. Variables were then iteratively removed from this model if they were nonsignificant at the α = 0.1 level and if their removal did not cause remaining parameters to change from more than 10% of their original value. It should be noted that robust Poisson regression is a valid modelling approach for common binomial outcomes in cross-sectional studies when calculating risk ratios. 36
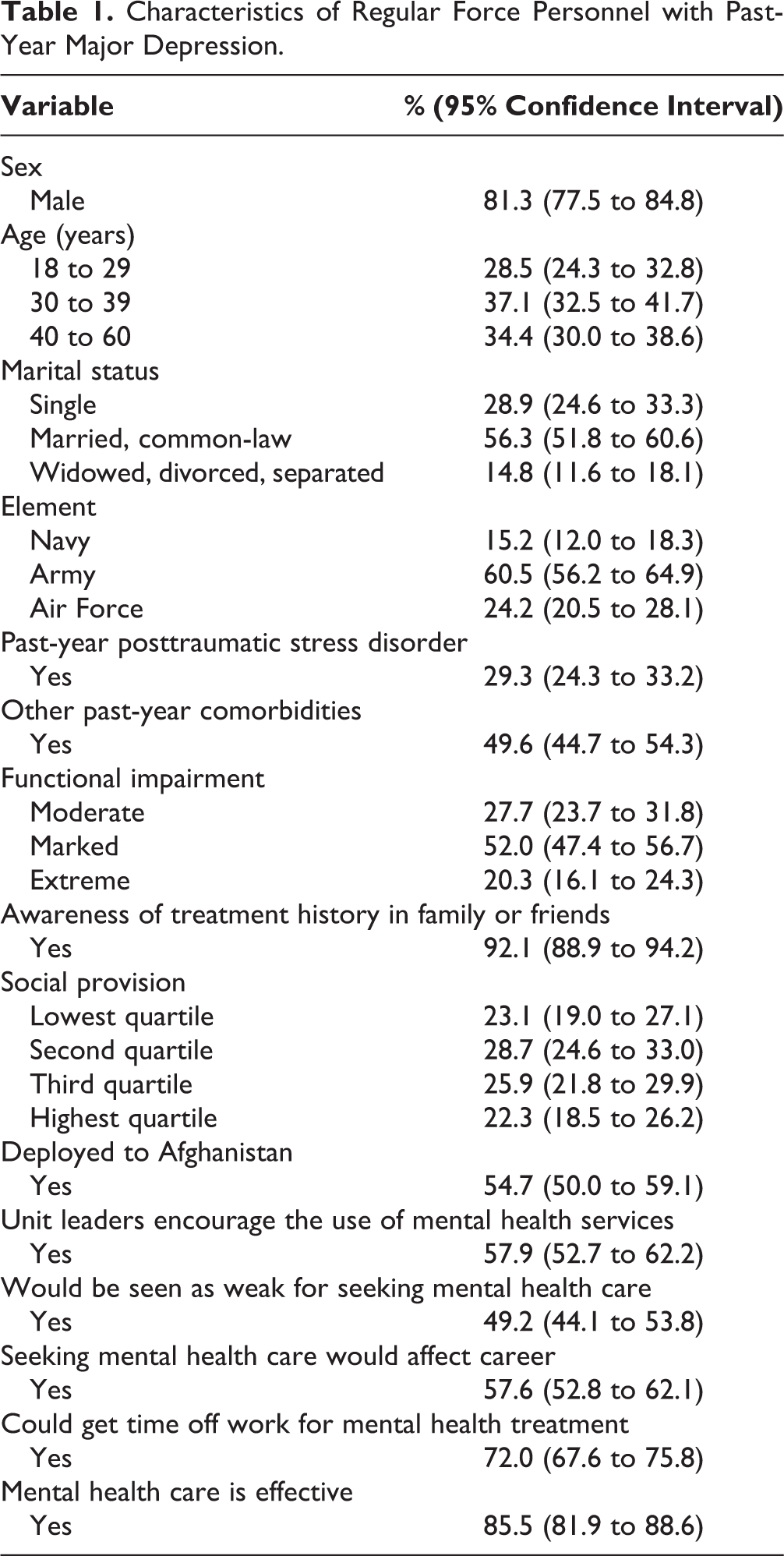
Characteristics of Regular Force Personnel with Past-Year Major Depression.
Sampling weights were used to obtain estimates representative of the source population while accounting for the survey’s stratified sampling design. Confidence intervals were obtained through 500 bootstrap replicate samples. All analyses were conducted using Stata, version 14. 37
Ethical Considerations
This study was approved by the University of Ottawa’s Research Ethics Board and by relevant bodies within Statistics Canada. Survey participation was strictly voluntary, and participants provided written consent. To protect the confidentiality of military personnel, Statistics Canada requires that all raw cell counts be rounded to the nearest 20 and that weighted population counts be rounded to the nearest 20 before being converted to proportions.
Results
Most Regular Force personnel with past-year depression were male, younger than 40 years, and serving with the Army (Table 1), which broadly reflects the demographic profile of the Canadian Armed Forces population. Most personnel with past-year depression said that their unit leaders encourage the use of mental health services, but 49% reported that they would be seen as weak for seeking mental health care, and 58% reported that seeking mental health care would affect their career. Nevertheless, 86% reported that mental health care is effective (Table 1).
In the previous 12 months, 75% (95% confidence interval [CI], 70% to 79%) of personnel with past-year depression had sought professional mental health care, while another 7% (95% CI, 5% to 10%) had perceived the need for care but had not received treatment.
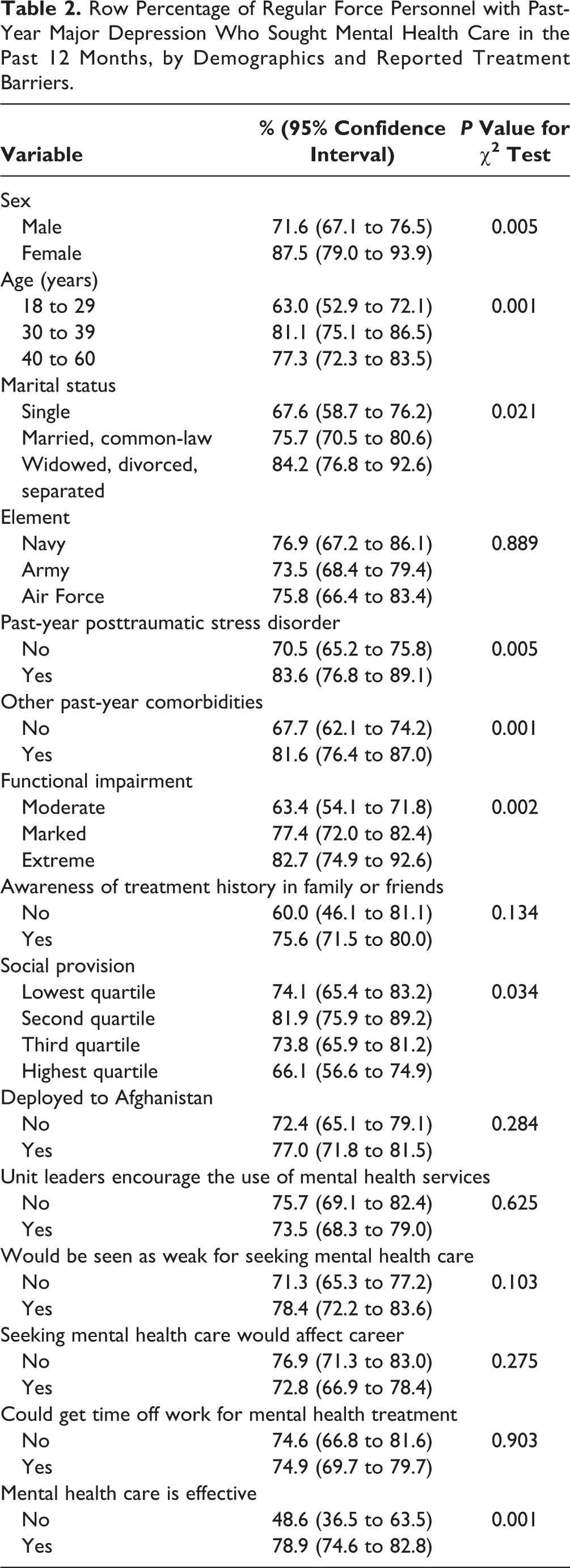
The prevalence of past-year care seeking differed significantly across levels of sex, age category, marital status, past-year psychiatric comorbidities, depression-related impairment level, and social support quartiles (Table 2). Endorsing the effectiveness of professional mental health care was associated with a higher proportion of past-year care seeking (Table 2). However, the prevalence of past-year care seeking was similar between depressed personnel who did and did not report other treatment barriers, including stigma concerns (Table 2).
Row Percentage of Regular Force Personnel with Past-Year Major Depression Who Sought Mental Health Care in the Past 12 Months, by Demographics and Reported Treatment Barriers.
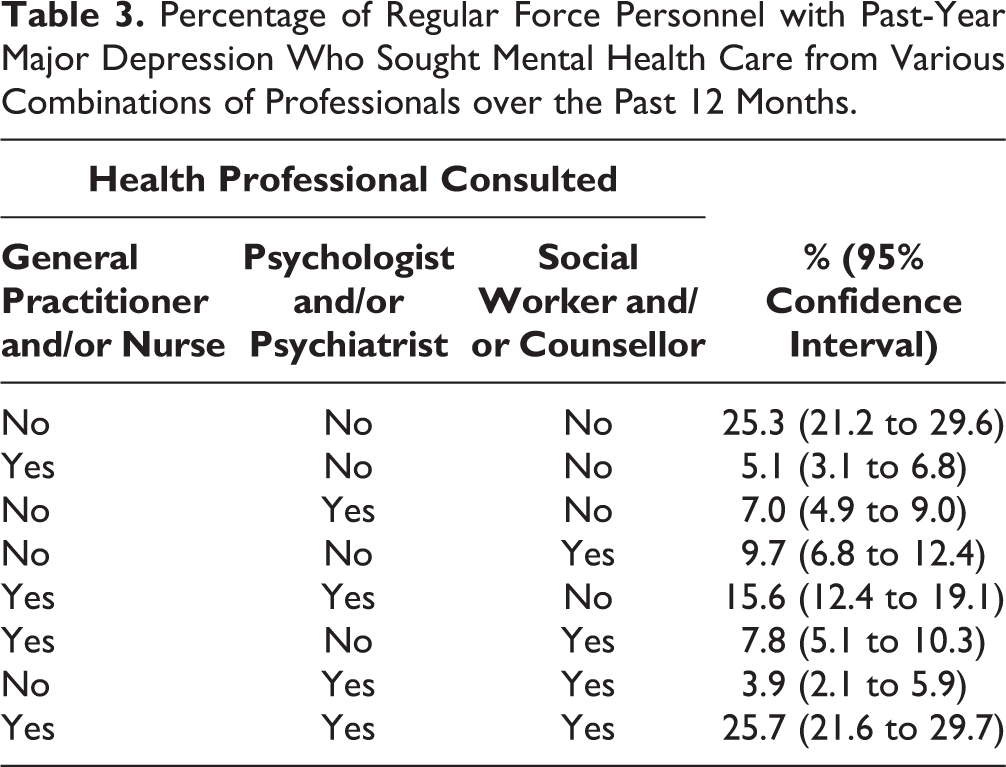
In the previous 12 months, depressed personnel who sought mental health care did so from a variety of health professionals. Among care seekers, 70% had talked to a psychologist or psychiatrist, and only 5% had been treated exclusively in primary care (Table 3). Depression-related impairment was associated with the type of mental health care sought; 75% of personnel extremely impaired by their depressive symptoms had consulted a psychiatrist or psychologist in the past 12 months, compared to 54% of personnel markedly impaired and 32% of personnel moderately impaired (P < 0.001).
Percentage of Regular Force Personnel with Past-Year Major Depression Who Sought Mental Health Care from Various Combinations of Professionals over the Past 12 Months.
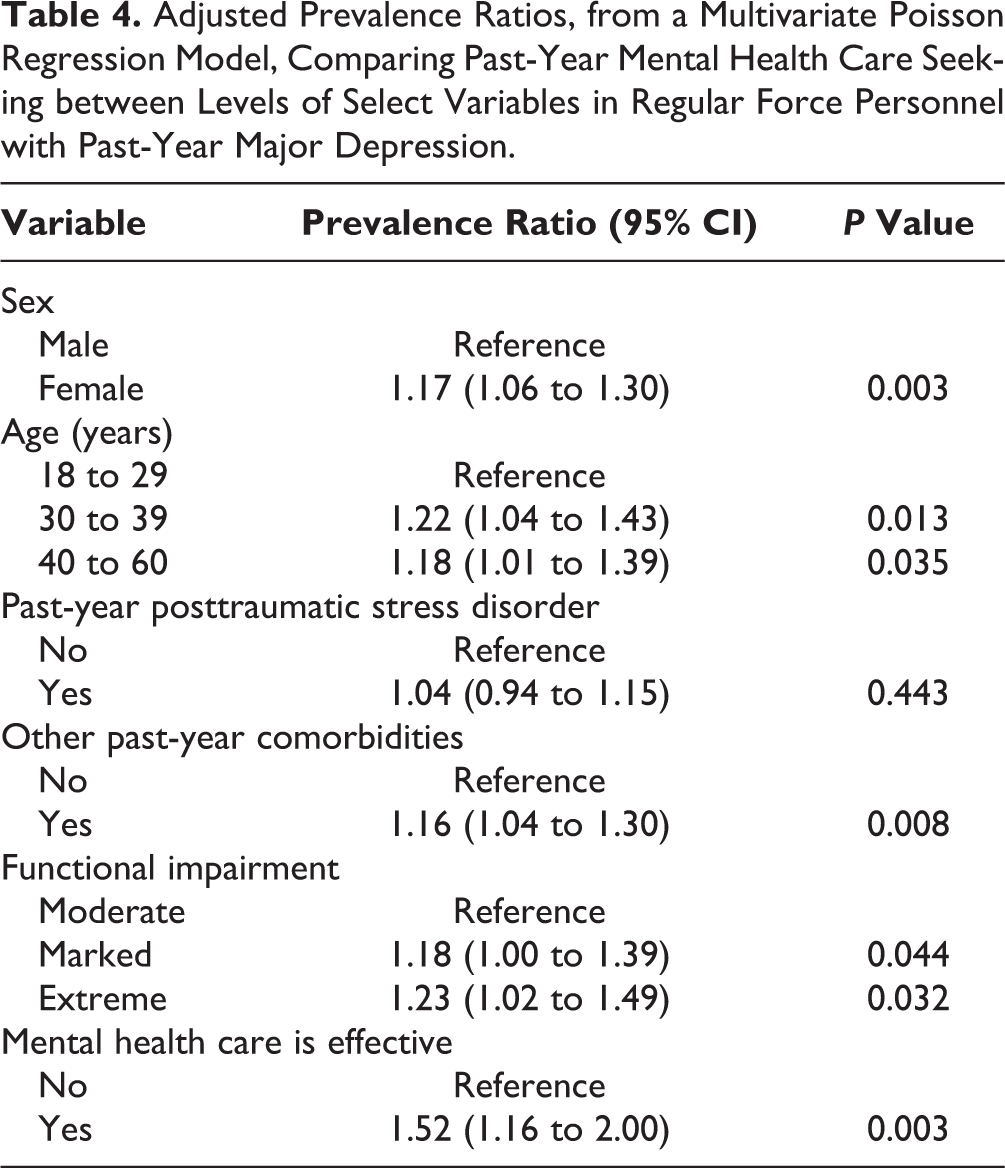
Our final multivariate Poisson regression model included sex, age, impairment level, past-year PTSD and other psychiatric comorbidities, and belief in the effectiveness of mental health treatments as significant determinants of past-year care seeking. After adjusting for covariates retained in the final model, belief in the effectiveness of mental health care was the strongest predictor of past-year care seeking in Regular Force personnel with past-year depression, associated with a 52% increase in the past-year prevalence of health service utilization for mental health issues (Table 4).
Adjusted Prevalence Ratios, from a Multivariate Poisson Regression Model, Comparing Past-Year Mental Health Care Seeking between Levels of Select Variables in Regular Force Personnel with Past-Year Major Depression.
Discussion
Results from this large population-based study have shown that three-quarters of Canadian military personnel with past-year depression sought professional mental health care in the past 12 months, and only a small proportion sought care exclusively from primary care physicians. Belief in the effectiveness of mental health care was the factor most strongly associated with care seeking. Stigma concerns were not associated with care seeking.
The care-seeking rate reported herein is substantially higher than what has been observed elsewhere. 9,11 Depressed Canadian military personnel therefore seem to access mental health care in greater numbers than depressed patients in other populations. This finding could be partly explained by unique aspects of the Canadian Armed Forces mental health system, including 1) access to unlimited mental health care, free of charge; 2) frequent mental health literacy training, to teach personnel how to recognize the progression of mental health symptoms and where to turn to for help; and 3) routine screening for mental disorders during mandatory periodic health assessments and upon return from overseas deployments. The latter two of these health system components were renewed and enhanced over the decade preceding data collection for this study, 14 which could partly explain why the care-seeking rate reported herein is substantially higher than what has been observed in previous Canadian military studies. 10 Nevertheless, the remarkably high care-seeking rate reported in our study is not entirely without precedent; in some civilian communities, as many as 84% of depressed individuals have been found to seek care. 38 Among UK veterans receiving war pensions for PTSD or physical disabilities, 72% of individuals who had major depression at some point during their military careers had sought mental health care before retiring from military service. 39
Most care-seeking personnel with past-year depression had received care from a psychologist or psychiatrist. This finding contrasts with care-seeking patterns observed in civilian populations, where depressed patients are often treated exclusively in primary care settings. 23 The relatively high use of specialty mental health services among care seekers may be due to the Canadian Armed Forces’ integrated health care system, where primary care and mental health clinics are part of single care delivery units. This finding is also encouraging, because guideline-concordant care is more likely to be administered to depressed patients in specialty mental health clinics than in primary care settings. 25 Future research may be needed to ensure that all care-seeking depressed Canadian Armed Forces personnel are receiving adequate treatment, particularly patients who are severely affected by their symptoms and who do not access specialist care.
Belief in the effectiveness of mental health treatment was the strongest predictor of past-year mental health services utilization among depressed personnel. This finding is consistent with results of the WHO World Mental Health Surveys, where desire to handle mental health problems on one’s own and perceived ineffectiveness of mental health care were the most commonly cited barriers to initiating and maintaining treatment in individuals with past-year psychiatric disorders. 40 Indeed, population-based studies from multiple different countries have consistently reported a significant association between mental health literacy and care-seeking attitudes. 41 The present study has found a relatively high level of mental health literacy in the Canadian Armed Forces, with 86% of depressed personnel recognizing the potential effectiveness of mental health treatment. Nevertheless, continuing mental health education efforts along those lines may further reduce the major depression treatment gap. Although results were not significant at the 95% confidence level, this study found a higher prevalence of past-year mental health service utilization in personnel who were aware of mental health treatment history among family or friends, mirroring findings among the Canadian general population. 19
As expected, severity of functional impairment caused by depressive symptoms was another strong predictor of past-year care seeking in personnel who had had depression in the past 12 months. Depressive symptoms range in severity among individuals who meet the clinical definition of major depression, 42 and patients most affected by their symptoms are the most likely to seek care. 18 It should be noted that interference with daily activities is one of the diagnostic criteria used by the WHO CIDI 3.0 to define past-year depression. 30 As a result, depressive symptoms must have caused at least moderate impairment to all participants included in our sample.
Somewhat surprisingly, stigma concerns and other perceived barriers to mental health care were not associated with past-year care seeking in depressed personnel. This finding is consistent with a growing body of literature documenting the absence of an association between perceived stigma and mental health services use in military populations. 15,22 A recent study reported that, despite experiencing a greater burden of mental health stigma than their civilian counterparts, Canadian Armed Forces personnel were more likely to seek mental health care than members of the general Canadian population; the study’s authors concluded that factors specific to the military, such as enhanced mental health literacy programs, may have counterbalanced the negative effects of stigma on care seeking. 16 However, these and other authors have highlighted the pitfalls of using cross-sectional data to study the relationship between perceived stigma and care seeking. 43 Indeed, stigma may become more noticeable after patients enter treatment, such that care seeking could be a predictor, rather than an outcome, of perceived stigma. 16,43
Limitations
Our cross-sectional design did not permit us to study temporal relationships between variables of interest. Therefore, it is unclear if the major depressive episodes experienced by participants over the past 12 months truly preceded their decision to seek mental health care and if factors found to be associated with care seeking were already present before participants received treatment, so we cannot be certain that these factors influence care seeking. For example, depressed patients may have only learned that treatments are effective after seeking care. In fact, a previously published longitudinal study found no association between the perceived usefulness of particular treatments and subsequent care-seeking actions in depressed individuals. 44 Furthermore, all care seekers were grouped into a single category, regardless of their level of adherence to treatment, or the time elapsed between the onset of their depressive symptoms and their decision to seek care.
Limitations notwithstanding, our results are based on a large, representative sample of Regular Force members of the Canadian Armed Forces. Our results have important implications for health promotion and policy. First, the high proportion of mental health service use—particularly from mental health specialists—reported herein may speak to opportunities to reinforce other mental health systems. Second, we have found that, despite a high care-seeking rate, a quarter of all depressed personnel do not seek care in a given year; while very few depressed patients were treated exclusively by primary care physicians, primary care clinics may provide opportunities to identify depressed personnel who must undergo periodic health examinations but would not otherwise seek care and redirect them toward primary or secondary treatment. Finally, even if the associations we reported in our final multivariate model are not causal, they could be used to identify population subgroups at higher risk of undiagnosed major depression and inform efforts to further facilitate care seeking in depressed personnel.
Conclusion
Three-quarters of all Canadian Armed Forces personnel with major depression seek professional mental health care within a given year. This mental health service utilization rate is remarkably higher than what has been reported in several other depressed patient populations and highlights opportunities to improve civilian mental health care systems. Nevertheless, a significant minority of depressed personnel remain untreated. Of all the care-seeking determinants examined in our study, belief in the effectiveness of mental health care was the strongest determinant of health service utilization among depressed military personnel. Additional mental health literacy campaigns may therefore help to further reduce the remaining major depression treatment gap.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded, in part, by financial support from the Canada Research Chairs program for Ian Colman.