
Abstract
Objective:
This study examined the physical and mental health of Cree adults, as well as the personal, clinical, and environmental factors associated with the presence of lifetime anxiety and mood disorders.
Methods:
Mental health was assessed using the computerised version of the Diagnostic Interview Schedule (CDIS-IV), and standardised instruments were used to assess physical health, addiction severity, and psychological distress in 506 randomly selected participants from 4 Northern Cree communities in Quebec.
Results:
Overall, 46.1% of participants reported chronic medical problems, 42.1% were current smokers and 34.5% met the DSM-IV criteria for an anxiety or mood disorder. Individuals with an anxiety or mood disorder were younger, predominantly female, and with higher educational levels, and a large proportion (47.7%) met the lifetime criteria for substance dependence. Hierarchical regression determined that anxiety or mood disorders were associated with serious problems getting along with parents, a history of physical and sexual abuse, and a lifetime diagnosis of substance dependence. Overall, 29.7% of Cree adults reported sexual abuse, 47.1% physical abuse, and 52.9% emotional abuse.
Conclusions:
This study highlights the high rates of physical and mental health problems in Cree communities and the association among parental history of psychological problems, history of abuse, and psychological distress. Participants expressed a desire for additional medical and psychological treatments to address the patterns of abuse, trauma, and mental disorders that are burdening the Cree communities in Northern Quebec.
The Aboriginal population in Canada exceeded 1.6 million people in 2016, growing by 43% between the years 2006 and 2016—more than 4 times the growth rate of the non-Aboriginal population. 1 Many studies have demonstrated that Aboriginal individuals have higher rates of physical health problems than the non-Aboriginal population, including adult and childhood obesity and diabetes, 2 –4 infant mortality, 5 and an increased risk of death from homicide, suicide, and pneumonia. 6 Overall, Canadian Aboriginal peoples have poorer quality of life and the lowest life expectancy compared with the general population. 7,8
Although several reports describe the high rates of chronic medical illnesses among some Canadian First Nations, there have been few epidemiological studies related to the rates of mental illness. 9 A 1997 survey in Ontario found that 16% of adults in First Nations communities met the criteria for major depression, as compared with 8% of other Canadians. 10 Based on results from the 2002 Canadian Community Health Survey – Mental Health and Well-being, 29% of off-reserve Aboriginal Canadians experienced high psychological distress, a rate significantly higher than that for Caucasians (20%). Aboriginal individuals were between 2- and 5-times more likely to experience any of the selected mental disorders (major depression, mania, panic disorder, social phobia, agoraphobia) or show substance dependence as compared with other ethnic subgroups. 11
Suicide and self-injury are the leading causes of death among Aboriginal peoples up to 44 years old. 12 The rates of suicide among Canadian Aboriginal populations are reportedly 2- to 10-times higher than the national rate. 13 –16 Factors such as being female, history of sexual abuse, domestic or family problems, violence, and substance abuse are associated with the risk of suicide in Canadian Aboriginal communities. 6,14,17,18 Among on-reserve Manitoba First Nations adults, who did not attend a residential school, those with a lifetime history of physical, sexual, or emotional abuse were 5.86-times more likely to have a suicide attempt history after adjusting for demographic factors and having a parent or grandparent who attended a residential school. 17 Additionally, the experience of abuse or fear increased the likelihood of suicide attempt by a factor of 9 among on-reserve Manitoba First Nations adolescents. 18
Many authors have stated that the lack of research is a limitation to understanding the impact of physical and mental illness among Aboriginal communities. 19 –21 Due to the paucity of accurate information on the wellbeing of Aboriginal peoples, there is an underdevelopment of local services and low rates of service utilisation. 9,22 A recent review identifying trends in Canadian Aboriginal health-risk research stressed a greater need for mental health treatment in First Nations communities. 23
The present study aimed to measure physical health, lifetime rates of anxiety and mood disorders, and substance dependence among a random sample from 4 of the 9 Cree communities in Northern Quebec. The secondary objective was to estimate the extent to which physical and psychosocial factors were associated with the diagnoses of anxiety and mood disorders. Standardised instruments and structured interviews were used to collect quantitative data on physical and mental health. Multiple variables potentially related to wellbeing were measured including socio-demographics, medical, employment, substance use, social, and psychological problems and distress, and history of abuse.
Methods
Ethical Considerations
The study protocol and consent form were approved by the Research Ethics Board (REB) of McGill University. The Research Committee of the Cree Board of Health and Social Services of James Bay (CBHSSJB) conducted further ethical review through the process outlined in the Cree Board of Health’s research procedures manual. 24 The community partners for this project were the Cree Nation local governments, represented by their Public Health Officers or Wellness Coordinators. Partial financing for the project was obtained from the Fonds Québécois de la Recherche sur la Société et la Culture (FQRSC), with additional funds provided by the Public Health Department of the CBHSSJB. ‘Letters of Understanding’ were signed between each Cree Nation government and the CBHSSJB to spell out mutual obligations and responsibilities involved with the partnership. A Steering Committee was formed consisting of one of the authors (J.T.), who represented the CBHSSJB Research Committee; a CBHSSJB representative for health and social services; and local government representatives. In addition, Research Advisory Committees (RACs) were formed in each of the participating Cree Communities.
Language
English to Cree translation (and back translation) of all instruments was completed before initiating the study. There were significant issues related to literacy and language, both in terms of the spoken Cree language (northern v. southern dialects of the Cree language), and the written language (the use of syllabics v. roman phonetics). The southern (inland) and northern (coastal) versions of Cree are different and the posters, radio messages, research instruments, and letters to participants were produced in both versions of Cree. To produce a Cree Lexicon to be used in the research, several workshops were held with one of the authors (K.G.) as well as elders, psychologists, social workers, translators, and members of the community with expertise in Cree. This led to the formation of a consensus document of terminology related to addiction and mental health. The consent form and all instruments, including the CDIS-IV, were available in both English and Cree (syllabics and phonetic versions). Self-report questionnaires were audio-taped in Cree, and participants with poor reading skills were able to listen to the questionnaire items on a laptop computer carried by each interviewer. Cree-speaking interviewers were available to clarify items on self-reports.
Sampling and Data Collection Procedures
Of 510 participants sampled, 4 individuals were excluded due to refusal at consent or cognitive problems. Therefore, a total of 506 randomly selected individuals from 4 of the 9 Cree communities from Northern Quebec were included in this study. In each participating community, local RAC members informed community members about the study via posters, pamphlets, newsletters, and local radio before the arrival of the interview team. A random sample was generated using housing lists, stratified by age and gender. Letters of invitation to participate were hand-delivered to randomly selected householders by members of the interview team or the RAC. The letters informed potential participants that a member of the interview team would return to their home to obtain consent and to conduct the interviews. It also gave them an option of setting up a specific time or an alternate venue if they did not want to be interviewed in their homes.
Randomly selected participants completed the informed consent procedures (prepared in English, Cree-simplified roman script, and Cree syllabics) followed by 2 interviews of 1.5-h duration. The interviewers collected information on socio-demographics, legal status, family/social functioning, psychological distress, mental disorders, as well as the severity and consequences of mental health and substance abuse problems. Participants ranged in age from 18 to 85 y, and had a mean (SEM) age of 44 y ± 0.7 y. For further information on the sampling procedure and a full description of the sociodemographic information, please refer to Gill et al. (2016). 25
Primary Survey Instruments
Standardised instructions were read to all participants in their language of choice. The CDIS-IV is a computerised version of the structured Diagnostic Interview Schedule that was used to assess major psychiatric disorders (DSM-IV diagnostic criteria). 26 Because of the fully structured nature of the DIS, non-clinicians were capable of administering this interview with adequate training, ensuring reliability and validity. 26
The Addiction Severity Index (ASI) is a structured interview that assesses general problems in 7 domains including health, drug use, alcohol use, family and social functioning, employment, legal problems and psychological distress. Within each domain, a quantitative composite severity index is produced based on the number, duration, frequency, and intensity of symptoms experienced over the previous 30 d. Each composite score ranges from 0.00 to 1.00, with 1.00 being the most severe. The psychometric properties of the ASI have been found to be excellent, with inter-rater reliability ranging from 0.86 to 0.96, and a test–retest reliability of 0.92. 27,28
Statistical Analysis
All statistical analyses were conducted using SPSS version 22 (IBM Corp). Analyses were carried out to compare basic socio-demographics and selected physical and mental health variables stratified by gender and the presence of an anxiety or mood disorder. Independent samples t-tests or ANOVA were used for continuous variables and Chi-squared test for categorical variables. The alpha levels were corrected for multiple comparisons using Bonferroni and statements of significance were based on these adjusted values. Chi-squared post-hoc tests compared cells with a z-test with Bonferroni correction and used adjusted standardised residuals, where residuals > |2| indicated statistical significance. Means and standard deviations are presented where appropriate. Effect sizes for significant results are reported as the phi (Φ) coefficient for Chi-squared tests, and Cohen’s d for independent samples t-tests.
Multivariate hierarchical logistic regression analyses were performed to identify the most significant variables associated with lifetime mood or anxiety disorder. Variables entered into the model included socio-demographics, lifetime psychosocial factors, and substance use. The model fit was assessed by the Hosmer and Lemeshow Goodness-of-fit test.
Results
Gender Comparisons of Physical Health
Females had higher rates of unemployment (χ2 [1, N = 501] = 10.32, P = 0.001, Φ = 0.14), worked fewer days (t[475.14] = 3.28, P = 0.001, d = 0.29), and had lower mean monthly income from employment (t[495] = 4.25, P = 0.0001, d = 0.38). Table 1 shows the full sample of 506 participants stratified by gender for measures of physical and mental health. Overall, 42.1% of participants were current smokers and 46.1% had a chronic medical problem that interfered with their functioning. Women had a significantly higher number of days of medical problems in the past month (t[502.58] = 3.42, P = 0.001, d = 0.30). There were no differences between men and women with regards to their use of prescribed medications or their number of lifetime hospitalisations. Approximately 38.5% of individuals were troubled or bothered by medical problems in the past month and 32.7% rated the need for additional medical treatment as important.
Physical and Mental Health Stratified by Gender
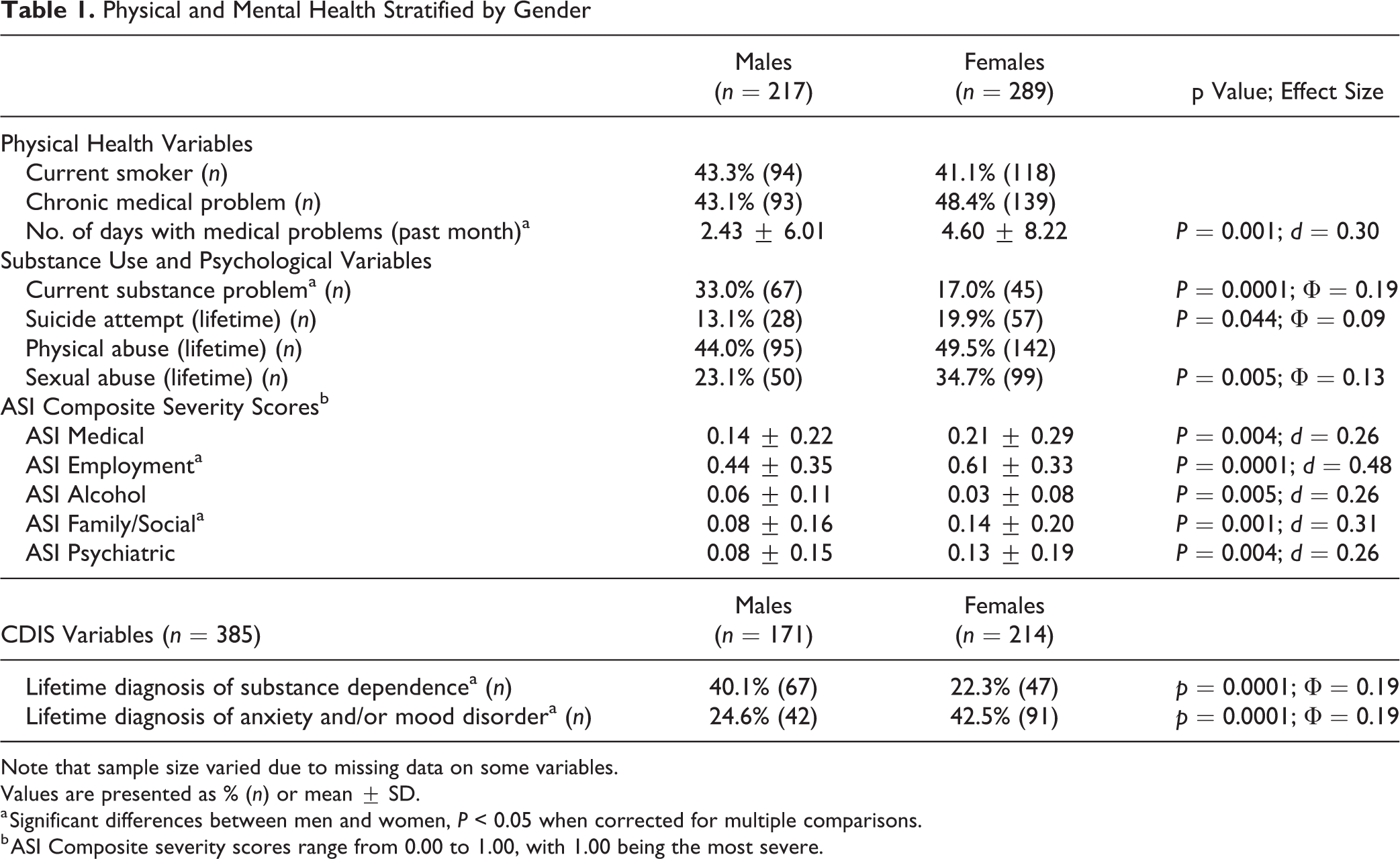
Note that sample size varied due to missing data on some variables.
Values are presented as % (n) or mean ± SD.
a Significant differences between men and women, P < 0.05 when corrected for multiple comparisons.
b ASI Composite severity scores range from 0.00 to 1.00, with 1.00 being the most severe.
Gender Comparisons of Mental Health
As reported on the ASI, women were more likely to have experienced depression in the past 30 d compared with men (26.7% v. 13.0%, respectively; χ2 [1, N = 500] = 13.85, P = 0.0001, Φ = 0.17). Overall, 33.1% of the participants were bothered by psychological problems in the past month and 25.4% rated the need for additional psychological treatment as important. Females also had a greater severity of family/social problems, as calculated by the ASI composite score (t [492.88] = 3.48, P = 0.001, d = 0.31). When corrected for multiple comparisons, Cree men and women were equally likely to have experienced emotional, physical, and sexual abuse in their lifetime (52.9%, 47.1%, and 29.7%, respectively). A history of suicide attempts was prevalent among 17% of the full sample.
Women experienced higher rates of mood (χ2 [1, N = 384] = 9.95, P = 0.002, Φ = 0.16), and anxiety (χ2 [1, N = 383] = 8.23, P = 0.004, Φ = 0.15) disorders in their lifetime, whereas men were more likely to have met the criteria for substance dependence (χ2 [1, N = 378] = 14.09, P = 0.0001, Φ = 0.19), and to have a history of substance abuse treatment (χ2 [1, N = 498] = 13.15, P = 0.0001, Φ = 0.16). Current substance problems were also a significant issue among men as compared with women (χ2 [1, N = 467]= 16.03, P = 0.0001, Φ = 0.19). Overall, 24% of individuals had a current substance problem.
Anxiety or Mood Disorders
From the total sample of 506 participants, 385 (76%) completed the CDIS-IV. Attrition analysis found no significant differences between completers and non-completers across socio-demographics, ASI variables, or other measures of psychological distress. Overall, 20.9% of the sample met the criteria for an anxiety disorder and 26.8% had a mood disorder in their lifetime. The most commonly diagnosed anxiety disorders were post-traumatic stress disorder (8.9%), specific phobia (6.2%), and generalised anxiety disorder (4.7%), and the most common mood disorder was major depression (25%). About 12% of the sample met the criteria for both anxiety and mood disorders in their lifetime, whereas 22% had only one diagnosis. The only significant difference between the groups was that individuals with both an anxiety and mood disorder were more likely to be prescribed psychiatric medication in their lifetime compared with those with either an anxiety or mood disorder (χ2 [1, N = 131] = 17.52, P = 0.0001, Φ = 0.37). Therefore, the 2 groups were collapsed and compared with individuals without an anxiety/mood disorder in terms of physical and psychological functioning.
As shown in Table 2, individuals with an anxiety/mood disorder were significantly younger (t [383] = 4.84, P = 0.0001, d = 0.54), predominantly female (χ2 [1, N = 385] = 13.56, P = 0.0001, Φ = 0.19), and with higher levels of education as compared with those without a disorder (χ2 [2, N = 354] = 20.61, P = 0.0001, Φ = 0.24).
Selected Demographics, Physical and Mental Health Stratified by Anxiety or Mood Disorder.
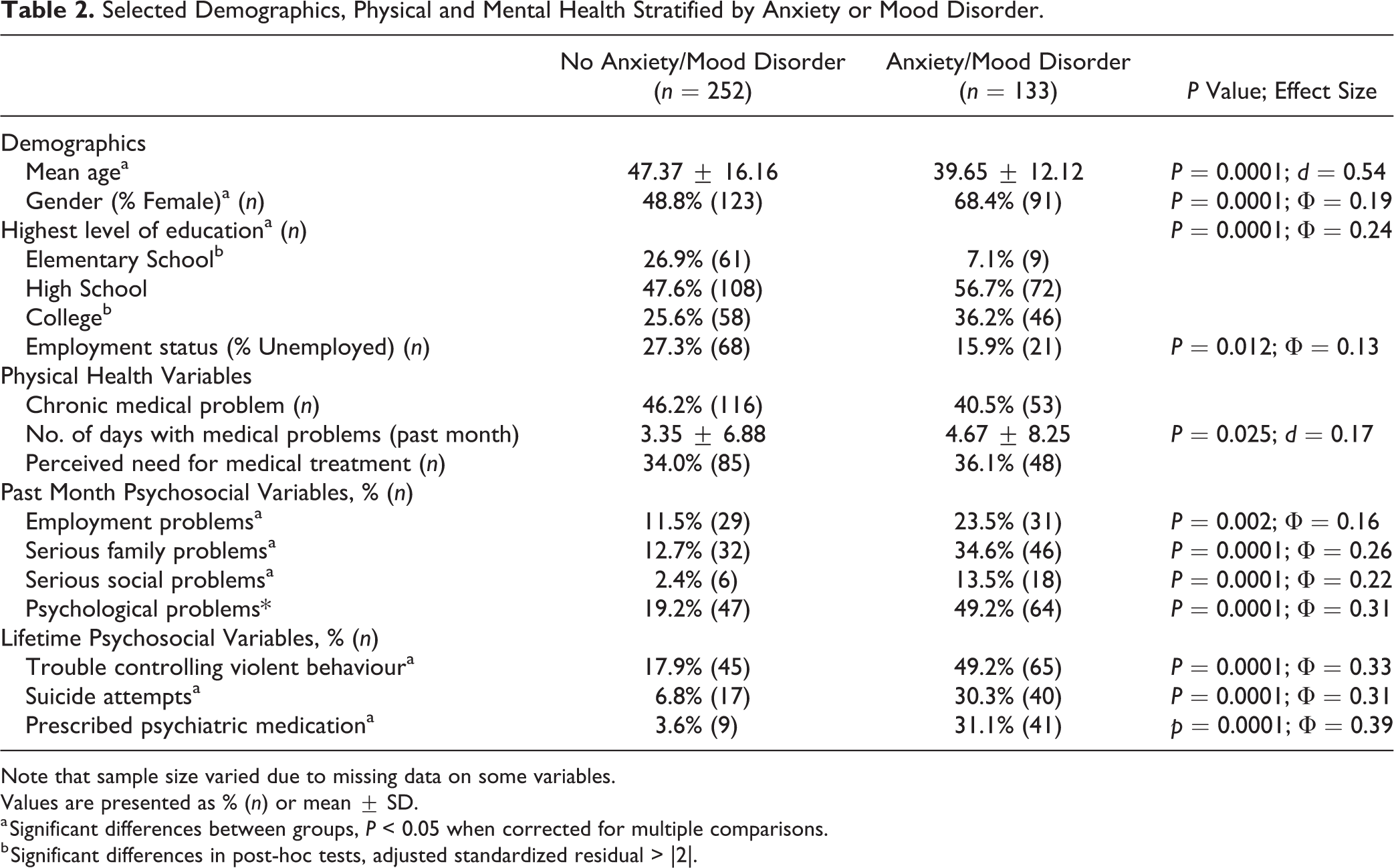
Note that sample size varied due to missing data on some variables.
Values are presented as % (n) or mean ± SD.
a Significant differences between groups, P < 0.05 when corrected for multiple comparisons.
b Significant differences in post-hoc tests, adjusted standardized residual > |2|.
Physical and Mental Health Stratified by Anxiety/Mood Disorder
Physical and psychosocial problems for those with and without an anxiety/mood disorder are presented in Table 2. There were no significant differences between the groups on any measure of physical health. No correlation was found between the presence of anxiety or mood disorders and chronic medical conditions (P > 0.05). A multivariate analysis found a significant interaction effect of age between chronic medical conditions and anxiety/mood disorder, such that individuals with chronic medical problems and no anxiety/mood disorder were significantly older than those with an anxiety/mood disorder but no chronic medical problems (56.44 ± 14.32 v. 36.14 ± 10.27, respectively; F[1,378] = 7.92, P = 0.005).
The prevalence rates of emotional, physical, and sexual abuse were significantly greater among individuals with an anxiety/mood disorder (smallest χ2 [1, N = 385] = 38.94, P = 0.0001, Φ = 0.32). Those with an anxiety/mood disorder were more likely to experience hallucinations (14.5% v. 4.4%); have trouble concentrating, remembering, and understanding (46.2% v. 13.5%); or have suicidal thoughts (53.8% v. 15.5%) and suicide attempts in their lifetime (smallest χ2 [1, N = 383] = 12.27, p = 0.0001, Φ = 0.18) as compared with no disorder. An anxiety/mood disorder was also associated with a greater prevalence of family, social, and psychological problems in the past month (smallest χ2 [1, N = 382] = 18.22, P = 0.0001, Φ = 0.22), and greater severity of ASI composite scores in these domains (smallest t [186.17] = 4.73, P = 0.0001, d = 0.54; Table 3). Among individuals with any lifetime anxiety/mood disorder, 50% were currently bothered by psychological problems and 40.5% reported the need for additional psychological treatment as important.
Substance Problems and Addiction Severity Index Composite Severity Scores Stratified by Anxiety and/or Mood Disorder
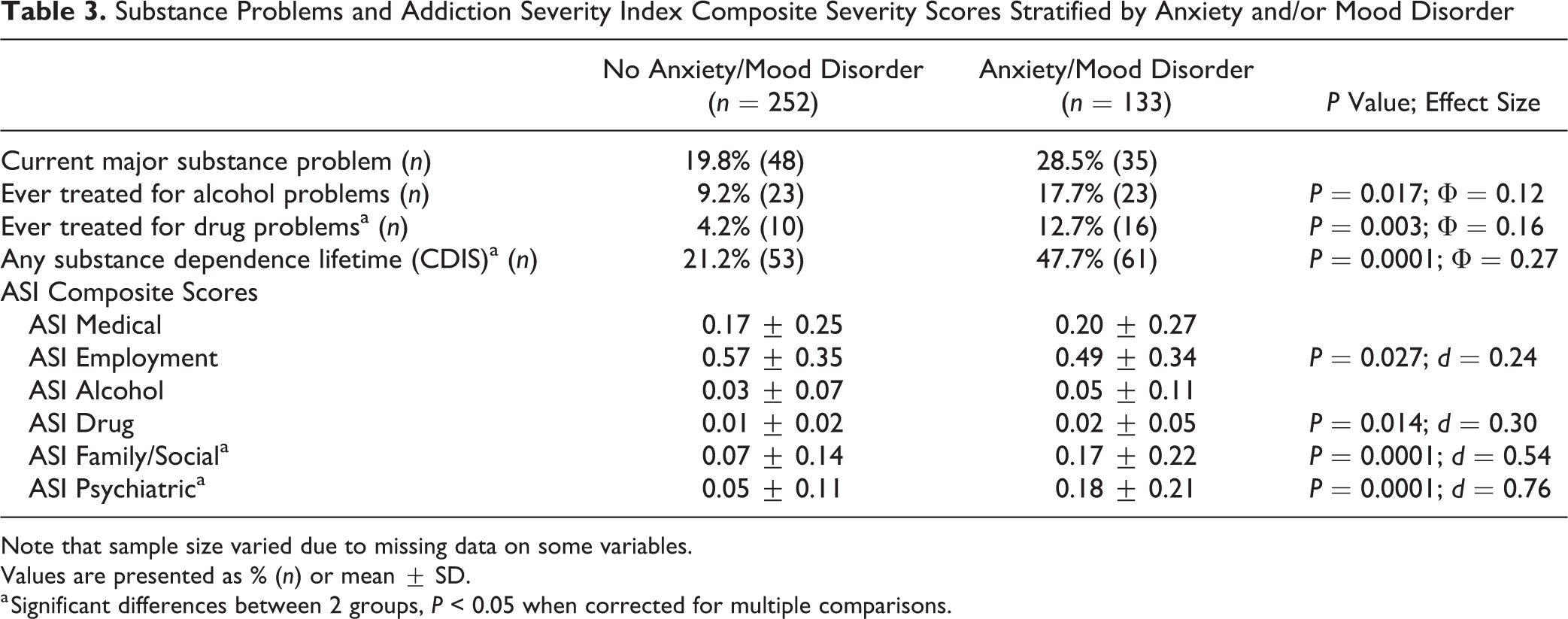
Note that sample size varied due to missing data on some variables.
Values are presented as % (n) or mean ± SD.
a Significant differences between 2 groups, P < 0.05 when corrected for multiple comparisons.
Table 3 describes substance use variables and ASI composite scores stratified by lifetime anxiety/mood disorder. The presence of a disorder was significantly associated with comorbid lifetime substance dependence (χ2 [1, N = 378] = 28.13, P = 0.0001, Φ = 0.27). The anxiety/mood disorder group was also more likely to have experienced drug problems in the past month (χ2 [1, N = 381] = 8.45, P = 0.004, Φ = 0.15), to have a history of drug abuse treatment (χ2 [1, N = 366] = 9.11, P = 0.003, Φ = 0.16), and a family history of substance problems (χ2 [1, N = 300] = 19.16, P = 0.0001, Φ = 0.25).
Figure 1 presents variables of familial stress and abuse among individuals with neither, one, or both an anxiety and mood disorder. Post-hoc tests found significant differences between no versus both anxiety and mood disorder groups for every variable of familial stress or abuse (adjusted standardized residual > |2|).
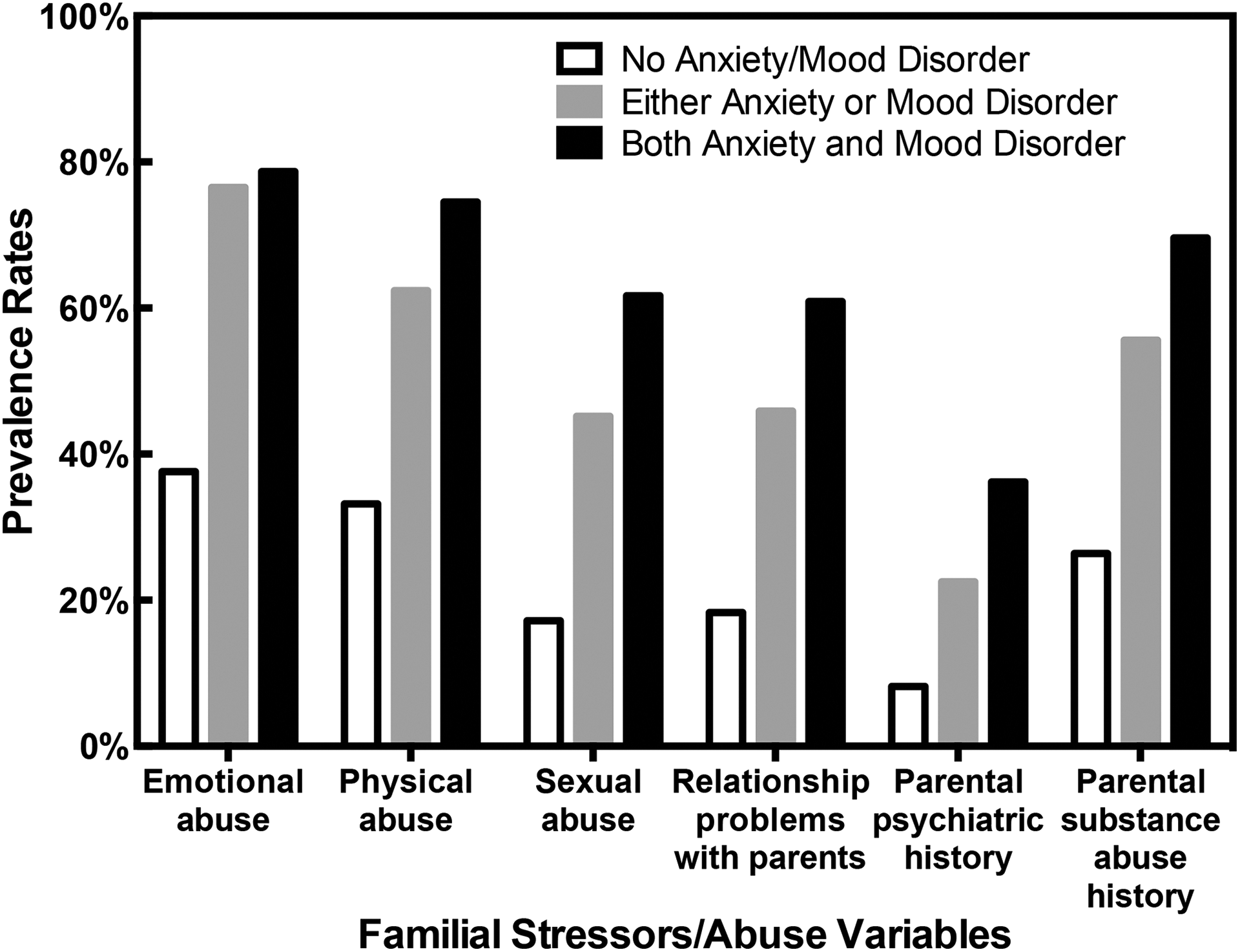
History of family stress and trauma among individuals with anxiety or mood disorders.
Regression Model
Table 4 demonstrates the overall hierarchical logistic regression analysis of lifetime indicators of an anxiety and/or mood disorder. Step 1 includes socio-demographic variables, such as gender, age, and number of years of education; Step 2 includes lifetime problems getting along with parents, trauma, and abuse variables; and Step 3 includes substance use variables. The final model accounts for 40.3% of the variance in lifetime anxiety and mood disorders (Model χ2 = 118.07; df = 11; P = 0.0001) and has a good Hosmer and Lemeshow Goodness of fit (P = 0.78). Predictors that were significant in the overall model included being female, having a history of physical or sexual abuse, problems getting along with parents, and meeting the DSM-IV criteria for lifetime substance dependence.
Multi-Construct Logistic Regression Analyses of Factors Associated with the Presence of Lifetime Anxiety and/or Mood Disorder (n = 342).
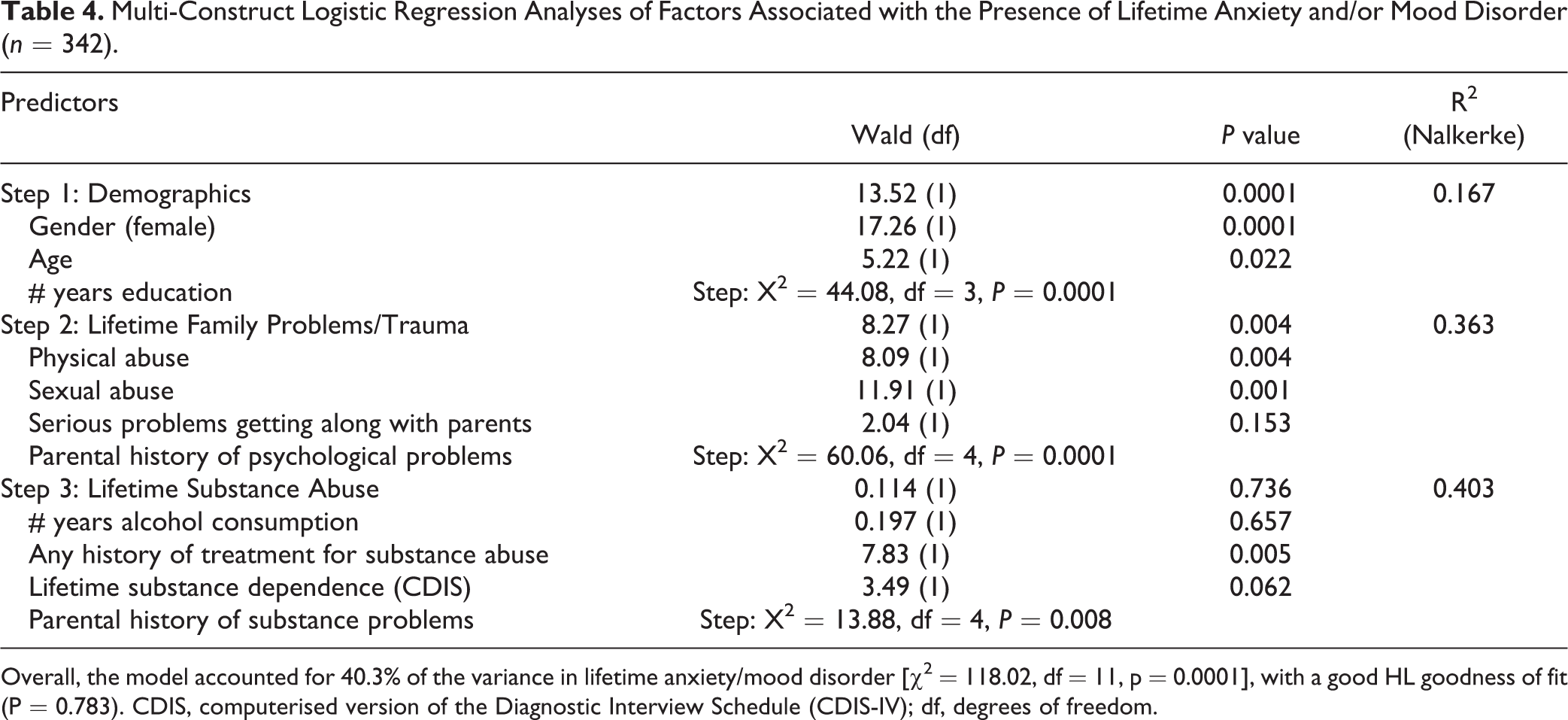
Overall, the model accounted for 40.3% of the variance in lifetime anxiety/mood disorder [χ2 = 118.02, df = 11, p = 0.0001], with a good HL goodness of fit (P = 0.783). CDIS, computerised version of the Diagnostic Interview Schedule (CDIS-IV); df, degrees of freedom.
Discussion
The perceived importance of additional medical treatment among a large proportion (32.7%) of the sample suggests a need for more health services in Cree communities. In an analysis of merged Canadian Community Health Survey data of the Canadian territories from 2007 to 2014, the proportion of Aboriginal peoples who had contact with a medical doctor or nurse in the past 12 mo was significantly lower than that for non-Aboriginal peoples. 29 A review by Smylie et al. (2006) concluded that the deficiency of appropriate planning and support of local health services might be contributing to the underdevelopment of community-level healthcare systems. 30 No correlation was found between the presence of anxiety or mood disorders and chronic medical conditions, suggesting that chronic health problems and psychological distress manifest independently of each other.
High rates of mental health problems are a persistent and troubling occurrence among Canadian Aboriginal communities. 9,31,32 A 2012 Statistics Canada study found that the lifetime prevalence of any mood disorder was 12.6% among the general population. 33 In the current study, 27% of Cree participants met the criteria for this diagnosis. A recent study determined that the prevalence of anxiety disorders among Canadian First Nations adults living off-reserve was 14.5%, 34 in contrast to the rate of 20.1% in the present study.
Individuals in the anxiety/mood disorder group were significantly younger, predominantly female, with a higher degree of education than those without anxiety or mood disorders, findings that were replicated in another study of Cree individuals with psychological distress. 9 A higher level of education is often associated with more stressful occupations and work situations, which may explain these associations among the anxiety/mood disorder group. 9 Men were more likely to have a current major substance problem and to have met the DSM-IV criteria for substance dependence in their lifetime, but the low perceived need for drug abuse treatment in the sample may be due to a general unwillingness to reveal distress among men. 9 The higher prevalence of mood or anxiety disorders among women and substance problems among men replicates well-known findings in the literature. 35
In the present study, 30% of individuals with anxiety/mood disorders and 17% of the full sample reported suicide attempts, similar to a report that 15% of Aboriginal peoples in Manitoba reserve communities (n = 2,728) had a history of suicide attempts. 17 Individuals with lifetime anxiety/mood disorders also had higher rates of lifetime substance dependence, history of treatment for drug abuse, and family history of substance problems. Lifetime drug use and family history of alcoholism have been shown to increase the prevalence of suicide attempts by 5.31- and 3.17-times, respectively, among on-reserve First Nations adolescents in Manitoba. 18 Substance problems were also associated with problem gambling among the same population of Cree peoples in Northern Quebec. 25 It is notable that risk factors for problem gambling similarly included traumatic life events (physical and emotional abuse) as well as anxiety and depression.
Overall, compared with the Canadian general population, Cree adults in this study experienced higher rates of physical (26.1% v. 47.1%) and sexual (10.1% v. 29.7%) abuse. 36 Being female, history of physical or sexual abuse, problems with family, and substance abuse were significant predictors of the presence of anxiety and mood disorders in the hierarchical regression model. The relationship among experiences of physical and sexual abuse, substance use problems, depression, anxiety, and suicide ideation and attempts has been demonstrated along with the presence of intergenerational transmission of violence and substance abuse among an urban Aboriginal population. 37 Aboriginal women are also more likely to live in environments in which substance abuse and domestic violence are widespread. 38,39
It is important to consider both the individual effects and the broader historical context within which intergenerational trauma has been experienced by Aboriginal peoples. Health disparities are directly and indirectly related to many factors, including social, economic, cultural, and political inequities. 40 Aboriginal communities have consistently attributed the disproportionate rates of psychological distress to their historical experiences of colonialism, including community dislocation and placement of children into residential schools. 41 –43 With the current legislation governing child welfare, it is estimated that there are 3 times as many Aboriginal children being removed from their families than at the height of the residential school system. 44 Reviews by health care organizations, professional collectives, and the Auditor General of Canada have criticized the government response to inequitable service disparities that are faced by First Nations children and families. 45 –47 In addition to adequate government funding, collaboration with Aboriginal service providers and healers is integral to increase the availability of culturally safe service provisions in these communities. 48 –50 The current study did not examine the context in which experiences of physical and sexual abuse occurred. However, childhood abuse or neglect is a prevalent issue in some Aboriginal communities. Among 234 American Indian women seeking primary care treatment at a community-based Indian Health Service Hospital in New Mexico, 77% reported experiences of childhood abuse or neglect. Among the sample in New Mexico, severe child maltreatment was significantly associated with lifetime posttraumatic stress disorder, substance use disorders, and mood disorders. 51 The Canadian Incidence Study of Reported Child Abuse and Neglect, 2008, showed that, although only 6% of children in Canada are Aboriginal, they comprise 22% of the substantiated reports of child maltreatment. 52 In the 2012 Canadian Community Health Survey, history of any child abuse increased the odds of anxiety, mood, substance use disorders, and suicide attempts by at least a factor of 2, controlling for sociodemographics. 36 Therefore, it is likely that a portion of individuals in the current sample who reported a history of abuse experienced maltreatment in childhood.
The Pathway to Hope program was developed by Alaska Natives to address child sexual abuse from a historical perspective: ‘that the higher rates of sexual abuse among certain Tribes, regions and communities is linked in part to years of victimization, but may also be perpetuated by internalized oppression and lateral violence among Tribal members’. 53 The program is focused on training community leaders to facilitate discussions of childhood sexual abuse and provide guidance in the development of culturally specific healing strategies. 53
The current study did not assess factors of intergenerational or historical trauma, or experiences of community dislocation. The large body of literature that implicates historical trauma in the experience of psychological distress by Aboriginal peoples suggests that these factors are important to address in interventions for healing; yet, this claim has not been rigorously evaluated. 42 The First Nations Mental Wellness Continuum Framework (2015) emphasizes the inclusion of trauma-informed, holistic interventions that incorporate cultural language, practices, ceremonies, knowledge, land and values. 54
More needs to be done to work with Aboriginal communities to address the disparities in health care services and interventions for psychological distress faced by Aboriginal peoples. 55 In a review of mental health service use between American Indian and Alaska Natives in the Northern and Southwestern Plains of the United States, the use of services differed by location: the Southwestern population was more likely to consult traditional healers than mental health professionals for mental health problems, whereas the opposite was true for Aboriginal peoples in the Northern Plains. 56 In another study, with adults from 8 Midwestern reservations and reserves, formal medical services were more likely to be endorsed as effective for emotional or substance abuse problems than traditional informal services. 57 These findings highlight the importance of incorporating community preferences into service development. Research must be continued in collaboration with Aboriginal communities to aid in the development of informed, relevant interventions to address the disparities in physical and mental health among Aboriginal peoples.
Conclusion
This study examined anxiety and mood disorders in a random sample of Cree adults, using validated diagnostic and research measures. There were strong relationships among family problems, parental history of psychological problems, physical/sexual abuse, substance abuse and psychiatric disorders for the Cree. Collaborations with Aboriginal communities are needed to develop strategies to reduce the high rates of abuse and mental health problems experienced by Aboriginal peoples in Canada.
Footnotes
Authors’ Note
L.M.H is now at the Department of Psychological Clinical Science, University of Toronto Scarborough, Toronto, Ontario, Canada.
Data Access
Final data ownership resides with the Cree Nation, and data access cannot be granted due to ethical considerations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research study was funded by the Cree Board of Health and Social Services of James Bay (CBHSSJB), the Fonds de Recherche du Québec – Société et Culture and the Ministère de la Santé et des Services Sociaux, Québec.