
Abstract
Keywords
Trans Communities and Health
Transgender (trans) is a term used to describe people whose gender identity does not match the sex assigned to them at birth. 1 Gender expansive refers to a wide range of gender identities and expressions that expand and broaden definitions of gender-normative identities and are neither “male” nor “female,” including nonbinary, genderqueer, and gender fluid. 2 Population studies yielding prevalence data for transgender (trans) people have estimated that 0.5% to 1.3% of adults identify as trans and that there are approximately 25 million trans people worldwide. 3 However, decades of poor data collection and a lack of understanding and acknowledgment of the wide range of gender identities that exist along the gender spectrum have resulted in underestimates of the size of the trans population. Trans and gender expansive people frequently face discrimination, stigma, violence, and barriers accessing housing, employment, and education. 3 Trans and gender expansive people also experience major challenges accessing trans competent and affirming physical and mental health services, leading to a high prevalence of adverse health outcomes. 3 –5
The Trans PULSE study 6 investigated the health and well-being of trans people living in Ontario through surveys administered to 433 trans participants over the age of 16. Numerous significant and alarming findings were reported, including that 77% of trans people had seriously considered suicide and 43% had attempted suicide at some point in their lives and that 21% of trans people reported avoiding the emergency department when they needed it because of previous stigma and discrimination associated with their gender identity. 7,8
The Canadian Transgender Youth Health Survey 9 investigated the health of trans and gender expansive youth between 14 and 25 years across Canada. Nine hundred surveys were completed by young people in all provinces and territories except Nunavut and the Yukon. Key findings included that only 15% of youth with a family physician felt comfortable discussing their trans related health needs, 1 in 3 young people reported not having an adult in their family with whom they could talk about problems, 7 in 10 young people that felt their family did not understand them, and young people living in their felt gender all of the time were 50% more likely to report good or excellent mental health. Stigma associated with gender identity can be further intensified when individuals experience the intersection of trans identities and marginalizing conditions such as preexisting mental illness. 10
Trans Communities and Research
Although it is known that trans and gender expansive individuals experience negative health outcomes, including a high prevalence of mental health difficulties, suicide, depression, anxiety, and substance use, as well as HIV and other sexually transmitted infections, 3,11 trans health continues to be an understudied issue, and trans and gender expansive identities are rarely included in health research, surveys, intake forms, and point-in-time counts. Furthermore, very few studies have addressed the issue of validity and reliability in screening and assessment tools for use with trans and gender expansive individuals in physical and mental health settings. 12 While numerous screening tools are available, minimal information is available about the reliability and validity of these instruments with trans and gender expansive individuals. 12 Most surveys and instruments commonly confound sex and gender by asking survey respondents to check off either male or female for “gender.” For example, a commonly used measure for assessing mental health and functioning, the Achenbach System of Empirically Based Assessments, 13 includes the following forms: Adult Self-Report (ages 18+), Youth Self Report (ages 11-18), and Child Behaviour Checklist (ages 4-18). All of these forms ask participants to categorize their “gender” as either boy/male or girl/female; the instruments use cisnormative methods for scoring and do not permit any edits to the data collection forms to allow for more accurate and gender inclusive wording. Cisnormative is the assumption that all, or almost all, individuals are cisgender, unless otherwise specified. Cisgender refers to individuals whose gender identity matches with their sex assigned at birth. For example, a cisgender woman is someone who was assigned female at birth who goes through life identifying as a woman. Sex and gender are not the same; the sex a person is assigned at birth is not always congruent with the person’s lived gender identity. For example, a person assigned the female sex at birth may never identify as a woman but may rather go through life identifying as a man or as gender nonbinary.
Numerous studies have continuously placed trans people under the label sexual minority. While gender and sexual identity overlap, they are also not the same. Gender identity refers to how an individual identifies their gender (male, female, genderqueer, gender fluid, transgender, etc.) and sexual identity refers to how an individual identifies whom they are sexually and romantically attracted to (lesbian, gay, bisexual, heterosexual, etc.). 14 When surveys do not consider and acknowledge that people identify in more ways than “male” and “female,” these forms perpetuate data erasure toward trans and gender expansive individuals and make it extremely difficult to collect data that accurately reflect the population. If trans people are not included in the study of broader social and political issues, they will be excluded from consideration in the development of health policy, policy instruments, and programming. The perception that trans people are rare reinforces erasure of the trans population, 15 further exacerbating the increased risk of mental health issues, including suicidality, anxiety, and depression in trans individuals.
Drawing on the knowledge that gender and sexual identity-based stigma and discrimination negatively affect the mental health of lesbian, gay, bisexual, transgender, queer, questioning, and 2-spirit (LGBTQ2S) individuals, leading to high rates of mental health issues including depression, anxiety, and suicide, 16 –19 the Mental Health Strategy for Canada 20 has identified the need to prioritize and address the mental health needs of LGBTQ2S individuals. The strategy specifically recommends increased LGBTQ2S competency training for organizations and for professionals and the public to increase their level of understanding of the mental health needs of LGBTQ2S individuals. However, these mental health needs cannot be fully understood or addressed without research that captures and accurately represents trans and gender expansive individuals.
The following two recent clinical research experiences will help us illustrate our point. First, while preparing to conduct an evaluation of Canada’s first specialized transitional housing program for LGBTQ2S youth, we wanted to include an alcohol screener to help identify hazardous drinking in a set of surveys that each youth was being asked to complete during two separate intake and exit interviews. The Alcohol Use Disorders Identification Test (AUDIT-C) 21 was recommended as a reliable and valid screener. However, the interpretation of scores relies on classifying respondents as “women” or “men”; thus, the AUDIT-C could not be included, because categorizing participants in this manner forces people to conform to the gender binary and erases all identities that do not fit into those two categories. Second, while reviewing demographic data collected via a feasibility study for the Longitudinal Youth in Transition Study (LYiTS), 22 we noted that approximately 20% of the participants did not identify as male or female, many youth were unhappy with the options for identifying their gender, and we had inadvertently excluded certain gender identities. We also realized that some measures included a “gender” question with male and female options only (i.e., the Youth Self Report from the Achenbach system) and used cisnormative methods for scoring the data. Both of these recent experiences resulted in a great deal of discussion about how we are currently capturing gender and sex in mental health and psychiatric research and the effect that current clinical research practices may be having on our results and subsequent clinical and policy decisions.
This led us to a call to action for trans inclusive measures and practices in mental health and psychiatric research. To facilitate access to resources that would support clinicians and researchers in becoming more trans inclusive, we provide a short summary of key documents in the literature that may be used by mental health clinicians and researchers who want to prioritize more gender-affirming practices. This is not a comprehensive literature review; rather, our goal is simply to provide a starting point for our colleagues when discussing how to make their studies, instruments, and vocabulary more trans inclusive, affirming, and competent.
Guidelines and Documents to Support Clinicians and Researchers in Becoming More Trans Inclusive and Competent
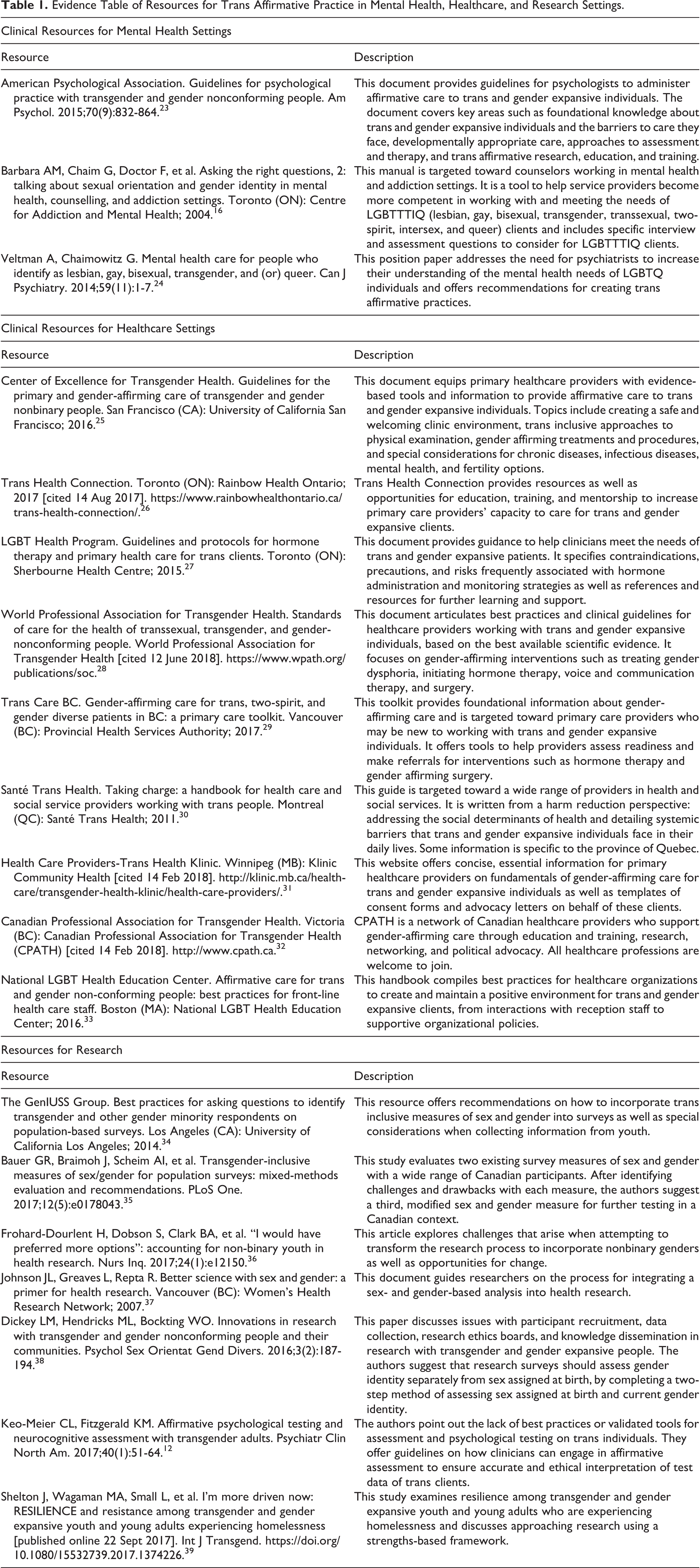
We searched the academic and grey literature using the CINAHL (EBSCO) database and Google Advanced Search using the keywords related to research measurement (e.g., assessment, norms, tool, validity, survey, etc.), gender identity (e.g., transgender, nonbinary, two-spirit, genderqueer, etc.), and area of practice (e.g., mental health, research, clinical) for articles over the past 15 years that offered guidelines, best practices, and concrete suggestions on trans inclusion in research and clinical practice. The citations of retrieved documents were also searched to further identify relevant resources. Experts in the field were then consulted to add any important resources that were missed in the search and finalize the list. Several clinical resources for healthcare settings were screened out because they highlighted programs that were limited to one province, and we wanted to ensure wider geographical representation from across Canada. The resources are organized into an evidence table (Table 1) with 3 sections: resources for mental health settings, for healthcare settings, and for research. The clinical resources for mental health settings outline essential knowledge and recommendations for trans inclusive best practices in assessment and mental health interventions. Resources for healthcare settings outline best practices for healthcare practitioners working with trans and gender expansive individuals. Resources for research offer suggestions for gender-inclusive research design, participant recruitment, data collection, and data analysis.
Evidence Table of Resources for Trans Affirmative Practice in Mental Health, Healthcare, and Research Settings.
We can no longer ignore gender identity in research, assessment tools, surveys, and intake interviews because trans and gender expansive people exist everywhere and are part of every population, regardless of whether your study or practice is LGBTQ2S specific. We call for a united effort to include trans and gender expansive individuals in research, surveys, questionnaires, and assessment tools. As clinicians, researchers, and community members, we have an ethical responsibility to ensure that all individuals are counted, regardless of their gender identity or expression.
Footnotes
Acknowledgements
Dana Gore is thanked for her support with the literature search.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kristin Cleverley was supported by the CAMH Chair in Mental Health Nursing Research while writing this article. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.