
Abstract
Objective:
Poor adherence to antipsychotic medications is strongly associated with psychotic relapses and hospitalizations. This may hinder patients’ ability to function, particularly in a first episode of psychosis (FEP). Poor adherence to treatment may be due to poor insight that can alter the capacity to consent to care, including pharmacotherapy. When patients are judged legally lacking the capacity to consent to care, treatment can be mandated through community treatment orders (CTOs). This naturalistic study examines the effects of CTOs in FEP patients.
Method:
This study examines 38 FEP patients legally deemed unable to consent to care during their follow-up. Using a naturalistic mirror-image approach, we compare clinical (Scale for the Assessment of Positive Symptoms [SAPS], Scale for the Assessment of Negative Symptoms [SANS]), functional (Global Assessment of Functioning Scale [GAF], Social and Occupational Functioning Assessment Scale [SOFAS]), and service use (number of emergency room visits, length of hospitalizations) indicators before and after CTO.
Results:
After the CTO, 37 of 38 patients complied with treatment. Statistically significant improvements in clinical (▵SAPS = –6.3; 95% CI, 4.5 to 8.1 and ▵SANS = –2.2; 95% CI, 0.9 to 3.4, P < 0.01) and functional (▵GAF = +15.0; 95% CI, 8.4 to 21.6, ▵SOFAS = +18.6; 95% CI, 12.8 to 24.4, P < 0.01) outcomes were observed. Significant reduction in emergency room visits (P = 0.016) and days of hospitalization per month in acute care units (P < 0.05) were identified with no difference in hospital days per month in short-stay units. Moreover, encounters with case managers (P = 0.008) and attendance of cognitive therapy sessions (P = 0.031) were significantly higher. However, patients’ weight significantly increased after CTO (▵weight = +8.0 kg, P < 0.01).
Conclusions:
In FEP patients, CTOs improve compliance to treatment, which contributes to reducing positive and negative symptoms, shortening hospital stays, and improving functioning.
Background
Nonadherence to antipsychotic medication in patients with psychotic disorders has been strongly associated with multiple relapses and hospitalizations. 1 Patients with a first episode of psychosis (FEP) receiving care in early intervention services tend to have greater compliance to treatment and better outcomes. 2 However, despite the specialized early intervention approaches adopted in these programs, disengagement from care and poor adherence to pharmacotherapy remain relatively high and can hamper symptomatic remission and functional recovery. 3 –5
Poor insight, often present in patients with psychotic disorders, encompasses several dimensions, including the capacity of patients to recognize the nature of their disorder and the need for treatment. 6 Under these circumstances, the capacity of patients to consent to care, including treatment with antipsychotic medication, may be questioned, and care providers have the possibility to request a substituted consent to care through legal procedures.
For a patient to be deemed lacking the capacity to consent to care, legal procedures are initiated by a physician and submitted to judicial authorities who may or may not grant a community treatment order (CTO) to mandate specific care modalities to patients without their consent. In the province of Quebec, 5 criteria to assess the “capacity to consent to care” are based on Nova Scotia’s Hospitals Act. 7,8 These criteria consist of determining if a “person understands and appreciates a) the condition for which the specific treatment is proposed; b) the nature and purpose of the specific treatment; c) the risks and benefits involved in undergoing the specific treatment; d) the risks and benefits involved in not undergoing the specific treatment.” Last, it is recommended that “in determining a patient’s capacity to make a treatment decision, the psychiatrist shall also consider whether the patient’s mental disorder affects the patient’s ability to appreciate the consequences of making the treatment decision.” 8 Although the definition of “capacity to consent to care” varies from one jurisdiction to another, it usually comprises the inability of patients to understand their illness and that the illness limits their capacity to understand the beneficial and side effects of the treatments offered to them. However, admissibility criteria and application modalities of CTOs vary from jurisdiction to jurisdiction.
While the goal of CTOs is to ensure that patients comply with treatment to increase the likelihood of remission and recovery, evidence on the effectiveness of CTOs remains equivocal and may depend, among other things, on the legal provisions adopted by various jurisdictions. 9 In this article, effectiveness of CTOs is conceived as their effect on the disorder outcomes mainly through a better compliance to treatment, which is the primary purpose of CTOs. However, it is possible that downstream effects of compliance, such as changes in insight, and working relation with care providers may also contribute to this effectiveness.
The Oxford Community Treatment Order Evaluation Trial (OCTET), a randomized controlled trial (RCT) examining the effect of CTOs in England and Wales, did not identify differences in the rate of hospital readmission over a period of 12 months between patients receiving care under either CTO or “section 17 leave” (a treatment modality with “equivalent levels of clinical contact but different lengths of compulsory supervision”). 10 However, the authors of this study stated that in England and Wales, “CTOs require patients to accept clinical monitoring and allow rapid recall for assessment but do not authorize forcible treatment outside hospital.” 10 Hence, it is possible that the CTO modalities examined by the OCTET study are limited, to a certain extent, in improving the compliance to pharmacotherapy outside hospitals without the patient’s consent. These CTOs seem to be only weakly enforceable in practice because they do not authorize the administration of medication. Rather, patients must be rehospitalized to be treated. These jurisdiction-specific legal provisions therefore limit the generalizability of the OCTET findings. A Cochrane review 11 examined the OCTET study and 2 other RCTs conducted in the United States, both comparing standard care to care under CTOs. 12,13 This review did not report differences between the 2 treatment conditions on several outcome variables, including service use, clinical and functional outcomes, and perceived coercion. The only advantage reported was a reduction in the risk of being a victim of violent or nonviolent crimes. 11 In contrast to these negative studies, 3 non-RCT studies in Canada found positive results such as a decrease in hospital stays, number of admissions, and increase in service use in case management. 14 –16 These conflicting results may arise not only from differences in study methodologies and patient characteristics but also from the wide variations of jurisdiction-dependent legal provisions.
Few studies have examined the effects of CTOs in patients with FEP treated in an early intervention program. A recent Australian study compared patients with FEP who were under CTO at least once during their treatment (19.2%) to those who were never under CTO, with regard to several pretreatment characteristics. 5 It was reported that the former had greater severity of symptoms, lower functioning, and lower levels of insight and were more likely to be hospitalized. The authors concluded that FEP patients under CTOs may represent a group of patients with severe mental illness and called for more studies to examine the effects of these compulsory modalities of treatment in FEP. This is particularly important given the purported beneficial effects of shortening the duration of untreated psychosis (DUP) 17,18 for treating psychotic symptoms but also the potential effects of this modality on patient compliance to treatment and therapeutic alliance. Indeed, given the coercive nature of CTOs, it is important to investigate their effects not only on illness-related outcomes but also on the well-being of patients and their sense of autonomy.
In Canada, provisions of care under CTOs vary significantly from one province to the other, and these variations include specific directive with regard to the history of treatment and service use. For example, in the province of Ontario, CTOs are restricted to patients who have had more than 2 hospitalizations, or at least 30 days of hospitalization during the 3 years preceding the filing of a CTO. Under such provisions, patients with FEP may be less likely to be placed on CTOs compared to patients in more advanced phases of illness. This is not the case in Quebec, where no specific criteria with regard to prior hospitalizations are required for a CTO to be filed.
The purpose of this naturalistic study is to examine the effectiveness of CTOs in patients with FEP with regard to several clinical and functional outcomes and health care utilization using a naturalistic mirror-image approach.
Materials and Methods
Settings
This study took place at the Prevention and Early Intervention Program for Psychoses (PEPP), at the Douglas Mental Health University Institute, Montreal, Canada. PEPP-Montreal provides specialized early intervention for patients presenting with affective and nonaffective psychotic disorders living in a defined catchment area of 300,000 residents in the area of southwest Montreal. It has no competing private or public service, making the sample of patients close to a treated incidence sample. 19,20 Patients can be admitted to the program as outpatients or through an inpatient unit. All patients are followed for a period of 2 years by psychiatrists and case managers and are offered a variety of pharmacological and psychosocial interventions as per their individual needs. 19
Participants
The present sample is derived from a larger sample of patients with a DSM-IV diagnosis of a first episode of affective or nonaffective psychotic disorder. To be admitted to the program, patients must have less than 30 days of exposure to antipsychotics. We admitted 665 patients to PEPP between January 2003 and July 2015. Of those, 548 consented to the PEPP research protocol, where patients consent to have periodic symptomatic and functional evaluations over the 2-year period while they are treated at PEPP. Thirty-eight (7%) of the 548 patients were under a CTO at some point and constitute the subsample analyzed in this study. All patients were followed for a period of 2 years by psychiatrists and case managers independently of when the CTO was obtained. In the months between the patient’s entry into the PEPP program and the date that patients were placed under a CTO, patients could refuse treatment while still being engaged in the PEPP program. CTOs do not provide patients with any more or any less services in our program. All patients in the PEPP program are offered the same services such as modified assertive case management, assisted housing, cognitive-behavioural therapy (CBT), and multifamily group therapy.
When CTOs were obtained for hospitalized patients, a nurse explained the legal obligation to comply with treatment. If the patient refused to comply, 4 (or more) hospital staff approached the patient and together reasserted the patient’s legal obligations to comply with treatment. The patient was then accompanied to the treatment room, where typically a long-acting antipsychotic (LAA) medication was given in compliance with the specific judgment.
In outpatient settings, patients who are on a CTO and who failed to attend a scheduled treatment appointment are brought to the hospital according to specific legal procedures. First, the hospital’s legal department is contacted and informed about the situation. The legal department then contacts the police and describes the patient’s breach of legal obligations to comply with treatment. Subsequently, the police locate and bring the patient to the emergency room, where nursing staff typically reminds the patient about his or her legal obligation and administers treatment, typically an LAA. The patient is then discharged, if in stable condition.
Participants were 14 to 35 years of age, with an IQ greater than 70 and no neurological disorders/head injuries or substance-induced psychosis but could have a comorbid substance abuse disorder. Demographic, clinical, service use, and medication data were collected throughout a 2-year follow-up period. All patients provided written informed consent to the research procedures. A parent or guardian provided the consent for patients younger than 18 who provided assent. The Douglas Mental Health University Institute Research Ethics Board approved the research protocol.
Measures
Diagnosis was determined by Structured Clinical Interview for DSM-IV (SCID), 21 which was performed at entry and repeated at month 12. Symptoms were measured using the Scale for the Assessment of Positive Symptoms (SAPS) 22 and the Scale for the Assessment of Negative Symptoms (SANS) 23 at baseline (usually within 1 month of admission) and months 3, 6, 12, 18, and 24. At each evaluation time point, trained research assistants conducted all symptom assessments for the preceding month and achieved interrater reliability ranging between 0.75 and 0.92. The SAPS total global score was calculated as the sum of the global scores of the 4 subscales: hallucinations, delusions, bizarre behaviour, and formal thought disorder. The SANS total global score was calculated as the sum of the global scores of the 4 subscales: affective flattening/blunting, alogia, apathy, and asociality with the exclusion of the global rating of attention. To measure the level of functioning, the Global Assessment of Functioning Scale (GAF) 24 was administered at the same time points as symptom assessments while the Social and Occupational Functioning Assessment Scale (SOFAS) 25 was conducted at baseline, month 12, and month 24. DUP was calculated as the period between the time of onset of psychotic symptoms to the time of adequate antipsychotic treatment, defined as taking antipsychotics for 1 month.
Body weight was measured in kilograms at baseline and months 1, 2, 3, 6, 9, 12, 15, 18, 21, and 24. The existence of a CTO, medications, hospital visits and/or stays, outpatient visits, and interventions were all obtained from patients’ clinical records. This is a naturalistic outcome study with a flexible protocol for antipsychotic treatment guided by the treating clinician within a broader set of guidelines.
Statistical Analysis
Means, standard deviations, and frequencies were calculated for all study variables. To compare outcome variables before and after CTO, paired samples t tests were used. We conducted a Pearson product-moment correlation to determine whether there is an association between the time it takes to obtain a CTO and changes in positive symptoms (measured by changes in SAPS scores). All statistical tests were considered significant if P < 0.05. Analyses were performed using SPSS, version 23 (SPSS, Inc., an IBM Company, Chicago, IL).
Results
The study sample comprised 38 FEP patients, mostly Caucasians (67%), single people (97%), and males (76%), with a mean age of 22.6 years (Table 1). Of the 38 patients studied, 30 were admitted to the FEP program as inpatients while the remaining 8 entered the program as outpatients. Although CTOs in Quebec do not require a previous or concurrent hospitalization, 35 of the 38 patients examined had either previous hospitalizations (n = 8) and/or concurrent hospitalizations (n = 27). Most of the patients lived with their families (76%), were unemployed (89%), and had a level of education that did not exceed high school (68%). The mean DUP was 60 weeks, which is comparable to the mean DUP of FEP patients in our program (DUP = 57; SD: 116.7 weeks). Patients predominantly had nonaffective psychosis (79%), with half of the sample having a comorbid substance use disorder. The average time to obtaining a CTO was 6.5 months (SD = 6.2) from PEPP entry. After a CTO was granted, compliance to treatment was very high (97%; 37 of 38 patients).
Demographics.
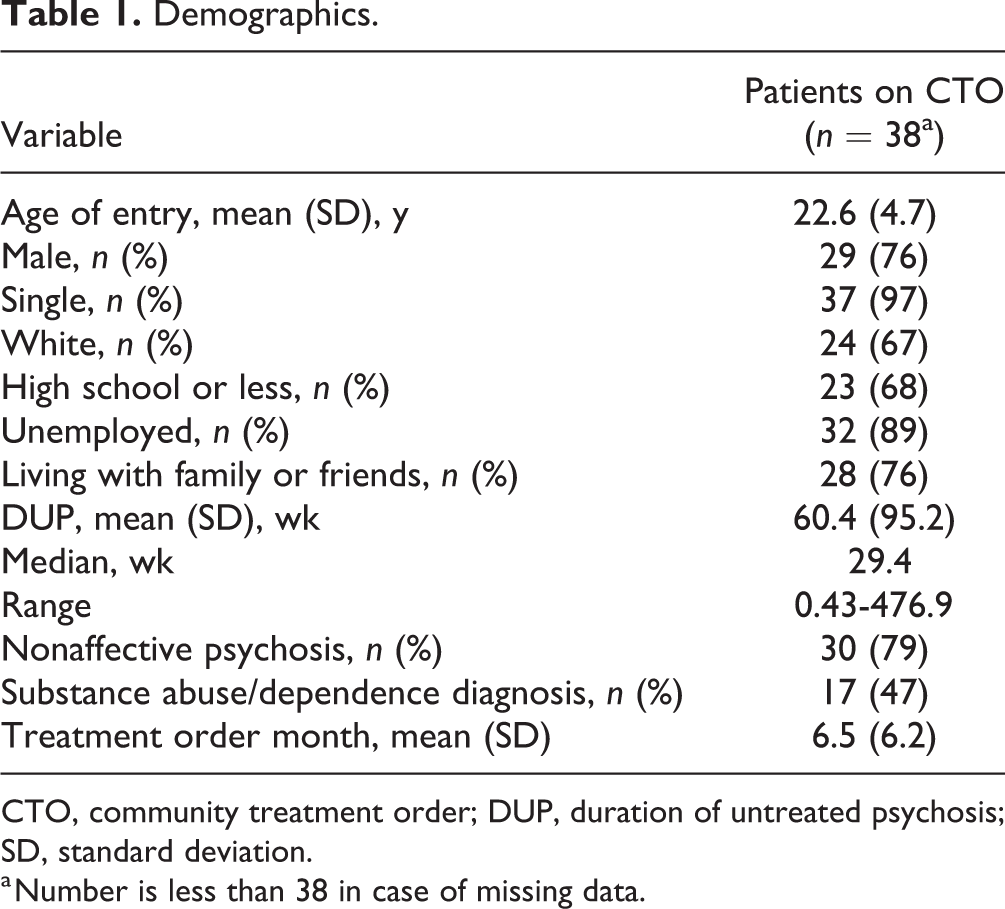
CTO, community treatment order; DUP, duration of untreated psychosis; SD, standard deviation.
a Number is less than 38 in case of missing data.
Most patients (95%, n = 36) received an LAA after the CTO was granted. Of these 36 patients, long-acting paliperidone was given to 40.5% (n = 15), risperidone to 37.5% (n = 14), aripiprazole extended release to 13.5% (n = 5), and zuclopenthixol to 5.4% (n = 2).
Patients were assessed at many time points during their 2-year follow-up. For each patient, we calculated the mean score on each scale (SAPS, SANS, GAF, and SOFAS) before the CTO and compared it to their mean score after the CTO. After obtaining a CTO, patients showed a significant decrease (P < 0.01) in positive symptoms (▵SAPS = –6.3; 95% confidence interval [CI], 4.5 to 8.1) and negative symptoms (▵SANS = –2.2; 95% CI, 0.9 to 3.4) compared to the period before CTO. There was also a significant increase (P < 0.01) in the level of functioning as measured by the GAF (average increase = 15.0 points; 95% CI, 8.4 to 21.6) and the SOFAS (average increase = 18.6 points; 95% CI, 12.8 to 24.4). However, patients on CTOs had a statistically significant increase (P < 0.01) in weight after CTO (average increase of 8.0 kg) (Table 2).
Clinical Outcomes before and after Application of CTO.
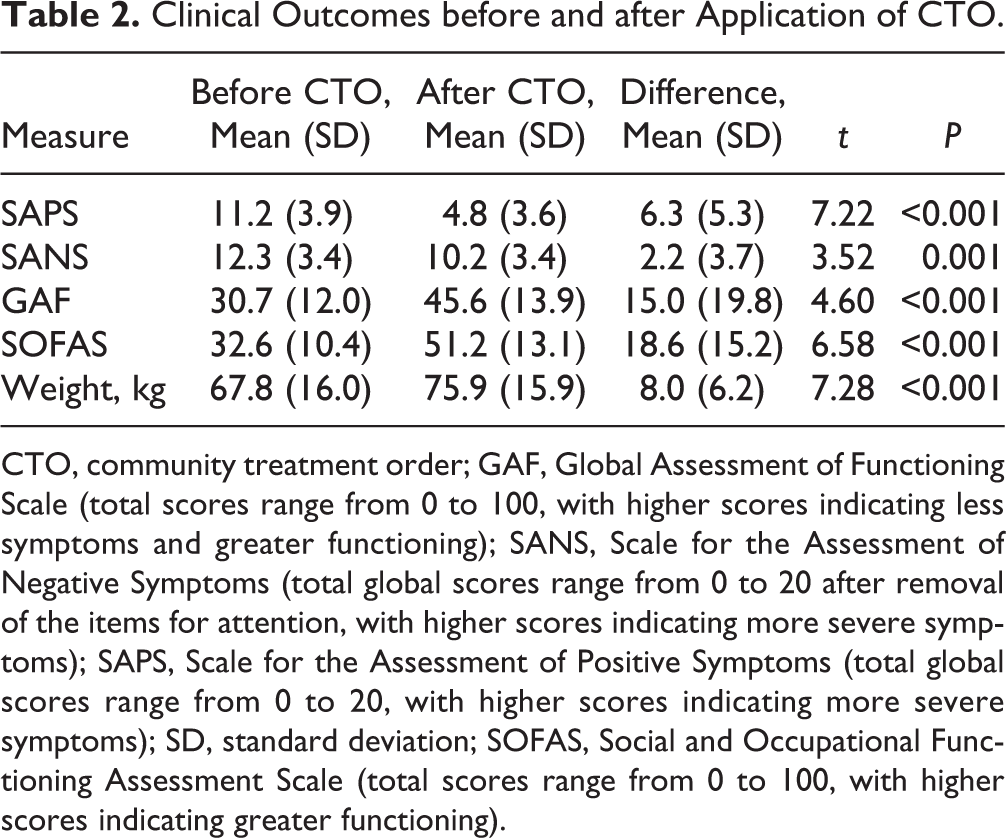
CTO, community treatment order; GAF, Global Assessment of Functioning Scale (total scores range from 0 to 100, with higher scores indicating less symptoms and greater functioning); SANS, Scale for the Assessment of Negative Symptoms (total global scores range from 0 to 20 after removal of the items for attention, with higher scores indicating more severe symptoms); SAPS, Scale for the Assessment of Positive Symptoms (total global scores range from 0 to 20, with higher scores indicating more severe symptoms); SD, standard deviation; SOFAS, Social and Occupational Functioning Assessment Scale (total scores range from 0 to 100, with higher scores indicating greater functioning).
Given that CTOs were granted at different times during the 2 years of follow-up, the time spent before CTOs was not equal to the time spent after the CTO. Hence, we compared the rate of hospitalization and emergency room (ER) visits (in days per month) before and after the CTO was obtained. In terms of service use, we found a statistically significant reduction after CTOs in the rate of ER visits and hospital days in acute care units, in both adults and adolescents (Table 3). No significant difference was found in the length of stay on short-stay units. Notably, FEP patients on CTOs continued to use other resources with significant increases in CBT session attendance and regular follow-up with case managers (Table 4).
Service Use before and after Application of CTO.
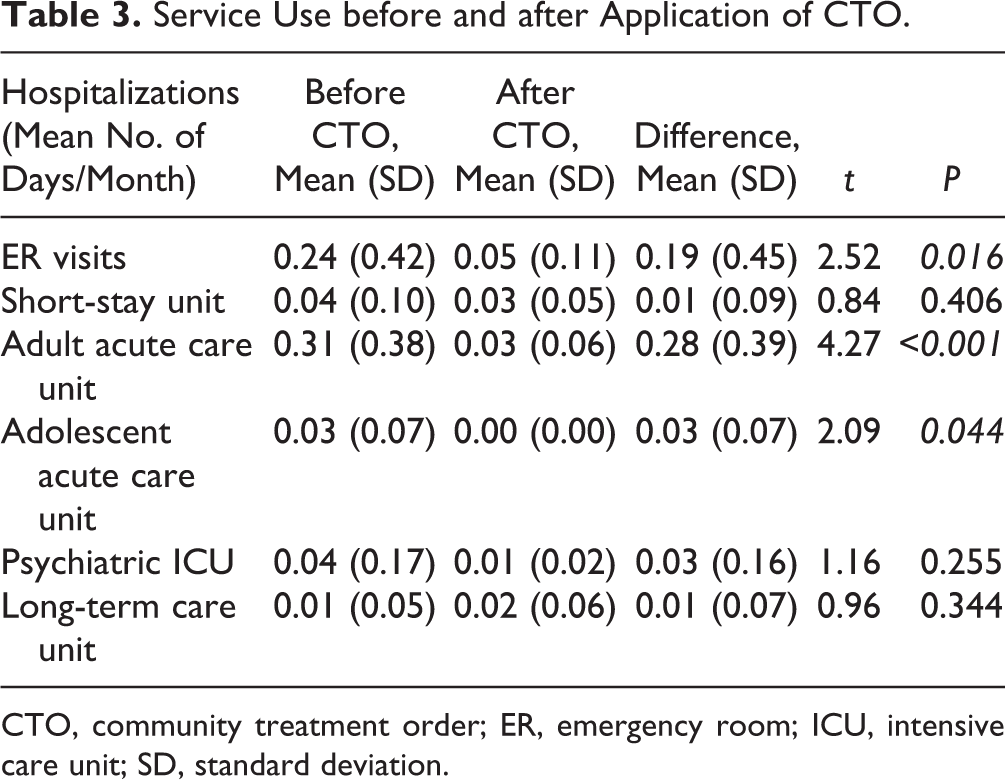
CTO, community treatment order; ER, emergency room; ICU, intensive care unit; SD, standard deviation.
Service Use (CBT and Case Management Visits) before and after CTO.
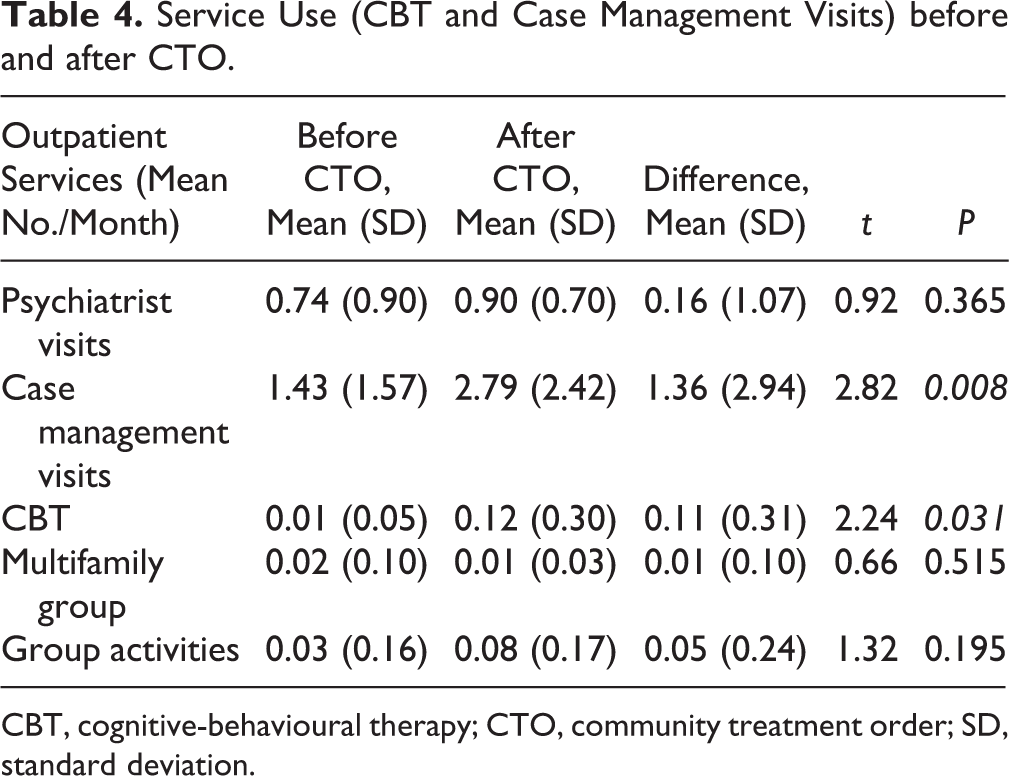
CBT, cognitive-behavioural therapy; CTO, community treatment order; SD, standard deviation.
Figure 1 shows that reductions in mean SAPS scores are negatively correlated (r = –0.488, P = 0.02) with the time elapsed between admission to the program and the time the CTO was obtained. This delay in obtaining a CTO and starting treatment accounts for 23.8% of the variance in the change of SAPS scores; the earlier the CTOs are obtained, the greater the decrease in SAPS scores.

Greatest changes in SAPS are observed when CTOs are obtained early in the course of illness. Increases in SAPS are only seen when CTOs are obtained after 10 months from baseline. CTO, community treatment order; SAPS, Scale for the Assessment of Positive Symptoms.
Figure 1 also shows that CTOs obtained after 10 months from entry to the program are associated with small changes in SAPS scores and even occasional increases. No increases in positive symptoms were observed when CTOs were obtained before 10 months. Given that patients committed to CTOs late in their follow-up in the program may have been treated for a shorter period of time compared to patients who were committed earlier to CTO, we carried out a regression analysis to examine the change in SAPS scores while adjusting for patients’ stay in the program after being under CTO. We found that the effect of time to CTO on the SAPS score was no longer significant (P = 0.1).
Discussion
Shared decision making and cooperation between care providers and patients are important values in early intervention programs for psychotic disorders. However, in a substantial proportion of patients, the capacity to consent to care can be severely impaired because of the nature of psychotic disorders. In such cases, care providers can opt for legal procedures to compel patients to comply with treatment, including pharmacotherapy.
To our knowledge, the effects of these complex interventions have not been studied in the context of patients with FEP. Previous studies examined more advanced phases of the illness and reported conflicting results with respect to the efficacy of CTOs. 7 –13 Some discrepancies may be due to methodological considerations. Others can be explained by the wide variability in modalities and eligibility criteria for obtaining CTOs, not only across countries but even between jurisdictions within the same country.
It has been reported that the reduction of DUP is associated with improved outcomes in FEP patients. 17,18 It is therefore possible that patients who do not consent to care may experience longer periods of untreated psychosis, which in turn can reduce their chance of remission and recovery. Furthermore, some studies indicate that patients with FEP who do not consent to care are more likely to present with severe forms of psychotic illness. 5 Consequently, it is important to conduct studies investigating the effects of CTOs in patients with FEP, which are, to our knowledge, lacking in Canada and worldwide.
In many jurisdictions, CTOs require previous hospitalizations. This reduces the likelihood of obtaining CTOs in the early stages of psychosis. However, in the province of Quebec, no specific restriction in relation to the history of hospitalization (number and duration) or the setting where treatment is provided (inpatient or outpatient) is required to seek and obtain CTOs. This facilitates the investigation of the effects of CTOs in patients with FEP.
This mirror-image study comparing 38 patients with FEP before and after a CTO generated several findings. First, the proportion of patients under CTOs in our sample is approximately 7%. This proportion appears to be lower than the one reported in the only study reporting the proportion of patients with FEP under CTOs originating from Australia (19.2%). However, this comparison should be regarded with caution given the potential differences between the 2 legal systems where these studies were conducted. Second, we found that 97% of patients who received a CTO were compliant with treatment in our program, thus demonstrating the intended goal of CTOs is achieved. Third, while under a CTO, patients with FEP showed statistically significant clinical outcomes, including reductions in positive and negative symptoms and increased social and occupational functioning compared to the period preceding the CTO. Improvement of both negative and positive symptoms is associated with better prognosis and functional outcomes. 26 Our data suggest that by mandating treatment, including pharmacotherapy, CTOs may help in reducing symptoms and in promoting better social and vocational outcomes, as reflected by a statistically significant and clinically meaningful improvement of the SOFAS scores after CTOs. Furthermore, patients had significantly less ER visits and less hospitalization days in acute care units after CTOs. Moreover, patients also had a significant increase in outpatient services use such as CBT and regular follow-up with case managers. This observation is interesting and somewhat counterintuitive. Indeed, although in most cases, CTOs compel patients to comply with LAA, they cannot compel patients to comply with psychotherapy and be more adherent to encounters with case managers. These observations suggest that CTOs may help the patient and care providers to move beyond the contentious question of pharmacotherapy and focus more on other needs of the patient, thus aligning with more optimal treatment plans.
Several limitations should be kept in mind while interpreting our results. First, this study was conducted in the province of Quebec, where a CTO can be sought without a history of hospitalization and can be obtained in inpatient or outpatient settings. Thus, our results may not apply to jurisdictions with different legal requirements. Second, this study was not an RCT but a naturalistic mirror-image study where patients were their own controls and the order of the treatment was fixed and not randomized (a variable period of treatment before CTO followed by a complementary period of treatment under CTO). Typical limitations of mirror-image studies include the conflation of results with an expected regression to the mean. Indeed, what happens after an intervention in a mirror-image study may be the result of the natural progression of the illness with patients returning to their baseline. This effect may be particularly important if the initial severity of illness is high, such as observed in this sample. In the present study, patients were placed on CTOs at different points in time from the index episode. Hence, this naturalistic design allowed us to test if the length of time to obtain a CTO is associated with reduction in symptoms and whether the effect observed is compatible with a regression to the mean. We find that symptom improvement is significantly greater when the CTO is obtained earlier with time to CTO accounting for a significant (P = 0.02) and sizable (23.8%) amount of the variance in change of positive symptoms. This observation is compatible with the regression to the mean hypothesis, and this is strengthened by the fact that the significance of this relationship fell to a nonsignificant level when we adjust for the length of time from CTO to last assessment. This suggests that the duration of treatment under CTO (longer in those who were committed earlier to treatment) may be the main source of the observed correlation. Notwithstanding these methodological limitations, the optimal time to seek a CTO remains complex. Reducing DUP, a variable associated with better remission of positive symptoms in FEP, 17,18 may guide this decision. Other important factors that need to be carefully considered include the functional consequences of untreated psychoses, the potential danger and victimization, the side effects of pharmacotherapy, and the consequences of coercive measures on the patient. Third, it is important to note that this is a short-term study. The effects of CTOs need to be reevaluated according to the legal conditions (duration of CTOs being specified in each judgment) but also according to the clinical needs of the patient and the evolution of mental condition and insight. While patients are under CTOs, it is important to discuss what modalities of treatment should be established after the CTO. Advanced treatment plans may help to avoid another episode of coercive treatment.
Finally, given the retrospective nature of this study, the effects of the coercive nature of CTOs on the psychological well-being of patients were not explored. Future studies combining both quantitative and qualitative approaches are needed to explore these effects.
Conclusion
In patients lacking the capacity to consent to care, CTOs may be used to provide treatment, including medication administration, and may be beneficial for patients. However, it should always be kept in mind that CTOs represent difficult experiences for patients given their coercive nature. Working very closely with patients to avoid such an intrusive procedure should be the priority of care providers, particularly in the early phases of illness. The low proportion of CTOs in our program indicates that in most cases, CTOs can be avoided. However, in the minority of cases where CTOs were sought and applied in FEP patients, our data suggest that there are several beneficial effects to this procedure, including a positive impact on how patients comply with their treatment. Indeed, 97% of patients who received a CTO complied with treatment in our FEP program. Furthermore, although CTOs compel patients to comply with LAA medications, they cannot compel patients to comply with psychotherapy and be more adherent to case management visits. Yet, FEP patients had significant increases in outpatient services (e.g., CBT) and regular follow-up with case managers. Given that the legal criteria used to grant CTOs vary significantly from one jurisdiction to the next, adopting legal provisions similar to those of the province of Quebec may help to better care for some patients with FEP who lack the capacity to consent to care in Canada and worldwide. Longer-term and qualitative studies are needed to better understand the full range of consequences of this procedure.
Footnotes
Data Access
As clinical researchers, we deeply value and appreciate the sharing of data. However, we are unfortunately unable to share our data because of Research Ethics Board (REB) constraints. Specifically, REBs emit research certificates on the condition that no patients be identifiable. It is of course possible for us to share anonymized data. However, relatively few patients (38) participated in our study. The shared data would include age, sex, and date that the CTO was attributed by the Douglas Institute. We fear that given the relatively small sample size of our study, this information may be sufficient to identify a patient and hence contravene the REB’s conditions.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Levy reports to have received a grant from Janssen for the conduct of this study and to be a speaker for Janssen, Lundbeck, and Otsuka outside the submitted work. Dr. Joober reports to be a speaker and/or consulting committee member for Pfizer, Janssen, BMS, Sunovian, Myelin, Otsuka, Lundbeck, shire, and Perdue; to have received grants from Janssen, BMS, Otsuka, Lundbeck, Astra Zeneca, and HLS; and to have royalties from Henry Stewart talks, all outside the submitted work except for the abovementioned grant.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by Janssen, Inc. (budget 8400027).