
Abstract
Objective:
To explore the effect of exercise on cognition in depression as well as the impact of potential moderators and intervention type.
Method:
Controlled and uncontrolled interventional studies that described an exercise intervention and cognitive outcomes in participants with major depressive disorder (MDD) were included following a search of Pubmed, Ovid Medline, PsycInfo and Embase from inception to January 2017. Meta-analyses were conducted to calculate Hedges’ g using a random-effects model. Meta-regression explored the relationships among age, baseline cognition, frequency and duration of exercise, and cognitive outcomes. Subgroup analyses were also conducted according to type and intensity of exercise interventions.
Results:
Of 12 controlled studies and 3 uncontrolled studies that met inclusion criteria, 9 (642 patients) were included in the meta-analysis. No significant effect of exercise was found on global cognition (Hedges’ g = 0.08, P = 0.33, I2 = 0%) or on individual cognitive domains. Meta-regression analyses failed to find significant relationships among participant age, baseline cognition, number of exercise sessions per wk, duration of exercise per wk, total duration of exercise during the intervention, or improvement in global cognition. Interventions combining physical with cognitive activity significantly improved global cognition (P = 0.048), whereas low-intensity interventions were also positive (P = 0.048).
Conclusions:
No impact of physical exercise was found on cognition in MDD overall. However, we found that interventions combining physical and cognitive activities had a positive impact, and that lower-intensity interventions, where adherence was improved, also impacted positively. There remains a lack of high-quality data in this population.
Depression is typically a relapsing, remitting condition, with a chronic course in many older and younger adults. 1 It is frequently complicated by cognitive impairment and, although cognitive performance may improve marginally with treatments for depression, cognitive dysfunction usually persists and is associated with increased risk of persistent depression. 2,3 Cognitive dysfunction is more closely associated with long-term functional outcomes than resolution of depressive symptoms, and is also associated with resistance to antidepressant treatment. 4,5 Depression in later life is associated with an approximate two-fold increased risk of dementia. 6 In certain instances, depression may occur as one of the earliest symptoms of an underlying cognitive disorder but depression with first onset in early life, decades before the onset of dementia, has also been associated with increased risk. 7 Increased number and severity of depressive symptoms throughout life are associated with dementia risk in a dose-dependent manner, suggesting that depression may be a true risk factor for cognitive decline. 8 For these reasons, it is now recognized that cognitive dysfunction is an important therapeutic target in depression. Interventions that improve underlying cognitive dysfunction could potentially modify the longitudinal course of depression with improved functional outcomes and potentially reduced resistance to treatment.
Exercise has been used to treat depression 9 and is known to have cognitive benefits in the general population, with one early pivotal study showing that adults who walk on a daily basis have reduced risk of cognitive decline. 10 In a recent longitudinal analysis of community dwelling adults aged 50 y and over, we found that depressive symptoms predicted accelerated cognitive decline and that physical inactivity was an important variable mediating this association. 11 It is not known, however, whether exercise improves cognitive dysfunction in the context of depression. One recent systematic review of interventional studies that focused on the impact of exercise on cognitive symptoms in depression failed to find a significant benefit. 12 That review included randomized controlled trials in which depression was diagnosed by diagnostic interview only. In view of the dearth of randomized controlled data in this area, we undertook a broader systematic review of the literature, including both controlled and uncontrolled studies using either diagnostic interviews or other validated measures of depression to determine whether exercise may be considered a therapeutic intervention for cognitive dysfunction in depression. We also wished to explore in greater detail several possible moderators of treatment outcome. Specifically, we assessed whether participant characteristics, such as age and baseline cognition moderated treatment outcome in addition to intervention characteristics, such as duration and dose of exercise. There is also an emerging literature to suggest that interventions combining cognitive with physical activities may be superior to those using exercise alone. 13 –16 We wish to determine whether such combined interventions have a positive impact on cognitive symptoms in depression.
Methods
The review protocol was registered with PROSPERO (International database of prospectively registered systematic reviews in health and social care): CRD42017069756.
Search Strategy
We conducted a systematic review of the literature regarding the impact of exercise intervention on cognition in individuals with major depressive disorder (MDD). We searched the following databases: Pubmed, Ovid Medline (1946 to present), PsycInfo (1806 to January wk 4 2017) and Embase (1947 to 26 January 2017) from inception to January 2017 using the search terms exercise, physical activity, cognition, cognitive function, depressive disorder, and depression. We searched using the search terms [(exercise OR physical activity) AND (cognition OR cognitive function) AND (depressive disorder OR depression)]. The search was limited to papers published in the English language. Reference sections from review papers were manually searched to ensure that all relevant interventional studies were included. Detailed search strategies and results for each database are reported in the supplementary materials.
Eligibility Criteria
We included interventional studies (controlled or uncontrolled) for individuals with MDD of all ages where an exercise intervention was clearly described and its impact on cognitive function measured. Our search included all studies using a validated diagnostic tool, where depression was defined either by diagnostic interview or by using a cut-off on a validated depression scale. Exercise was defined according to the American College of Sports Medicine 17 as “a type of physical activity consisting of planned, structured, and repetitive bodily movement done to improve and/or maintain one or more components of physical fitness.”
Study Selection and Data Extraction
One researcher screened all titles and abstracts and obtained full texts of potentially relevant papers. Two researchers worked independently on these full texts to determine whether they met the inclusion criteria. Disagreements between the 2 reviewers were resolved by consensus. Initial agreement between the reviewers was high (k = 0.91). The 2 researchers also extracted the data separately, and all disagreements were resolved by consensus. Information was extracted regarding: 1) the trial’s inclusion and exclusion criteria; (2) the participant characteristics; (3) the type of intervention; and (4) the cognitive outcomes. The risk of bias was assessed using the Cochrane risk of bias tool. We assessed the publication bias by evaluating a funnel plot of the standard mean differences (SMD) for asymmetry, as well as Egger’s test.
Cognitive Outcomes
The primary outcome was global cognition: Global cognition was defined as the average change in all clinically validated measures of cognitive function following the exercise intervention (or control condition). 18 A “mean change score” was calculated for each cognitive domain, and the average of the changes in all cognitive domains was used for global change. When multiple tasks were presented for each cognitive domain, we calculated an average score, as previously described. 19 We then determined the impact on individual cognitive domains, including: processing speed, attention/vigilance, working memory, verbal learning and memory, visual learning and memory, reasoning, and problem solving, according to the structure of the MATRICS Consensus Cognitive Battery (MCCB). 20 When a task reported in studies was not part of the MCCB, we categorized the task into its respective domain according to instructions in the original study (see supplementary material).
Analyses
We conducted further analyses in studies eligible for meta-analysis. In studies with multiple treatment groups, we deleted intervention groups without physical exercise included 21,22 (such as cognitive behavior treatment and antidepressants), or combined groups where different types of exercise were treated as the physical exercise group, 23 according to the recommendation of the Cochrane Handbook. We used a pre–post correlation coefficient of 0.7 to calculate standard deviation (SD) of the mean change scores with the formula [SQRT(SD2 baseline+SD2 final-(2*0.7*SDbaseline*SDfinal))] when no related information was reported in the original study. 24,25 SMD was calculated as effect size for each study using the mean change scores and the SDs of both exercise and control groups. A random-effects model was applied throughout the study to account for the expected heterogeneity between studies. Heterogeneity between studies was determined using Cochrane’s Q and I2 values. The above analyses were performed in Review Manager 5.3. We then conducted meta-regression analyses to determine the relationship between continuous moderators (age, baseline cognition, number of exercise sessions per wk, exercise duration per wk, and total duration of the whole intervention) and effect-size estimates. Influence plot analysis was performed by removing each study. Subgroup analyses were conducted according to the intensity of the exercise intervention and whether the interventions consisted of combined cognitive and physical activities or physical activity alone. Different exercise intensities were defined according to American College of Sports Medicine. 17 These analyses were performed by STATA 12.
Results
Search Results
A total of 2,202 articles were identified, of which 15 were eligible for inclusion in a qualitative review. Of these 15 studies, 9 randomized controlled trials were suitable for inclusion in a quantitative meta-analysis. The full details of the search results are reported in Figure 1, and a list of the included and excluded studies is provided in Supplemental Table S1. The main characteristics of the included studies are shown in Table 1. The 9 studies in the meta-analysis included 642 study participants with depression, of whom 374 were randomized to an exercise intervention. The mean age was 46.8 y (SD, 13.8 y), and 68.2% were female (n = 438). Exercise interventions were 9.8 wk on average, with 2.1 sessions per wk (range, 1 to 3 sessions) and 131.67 min (range, 90 to 180 min) in duration per wk.
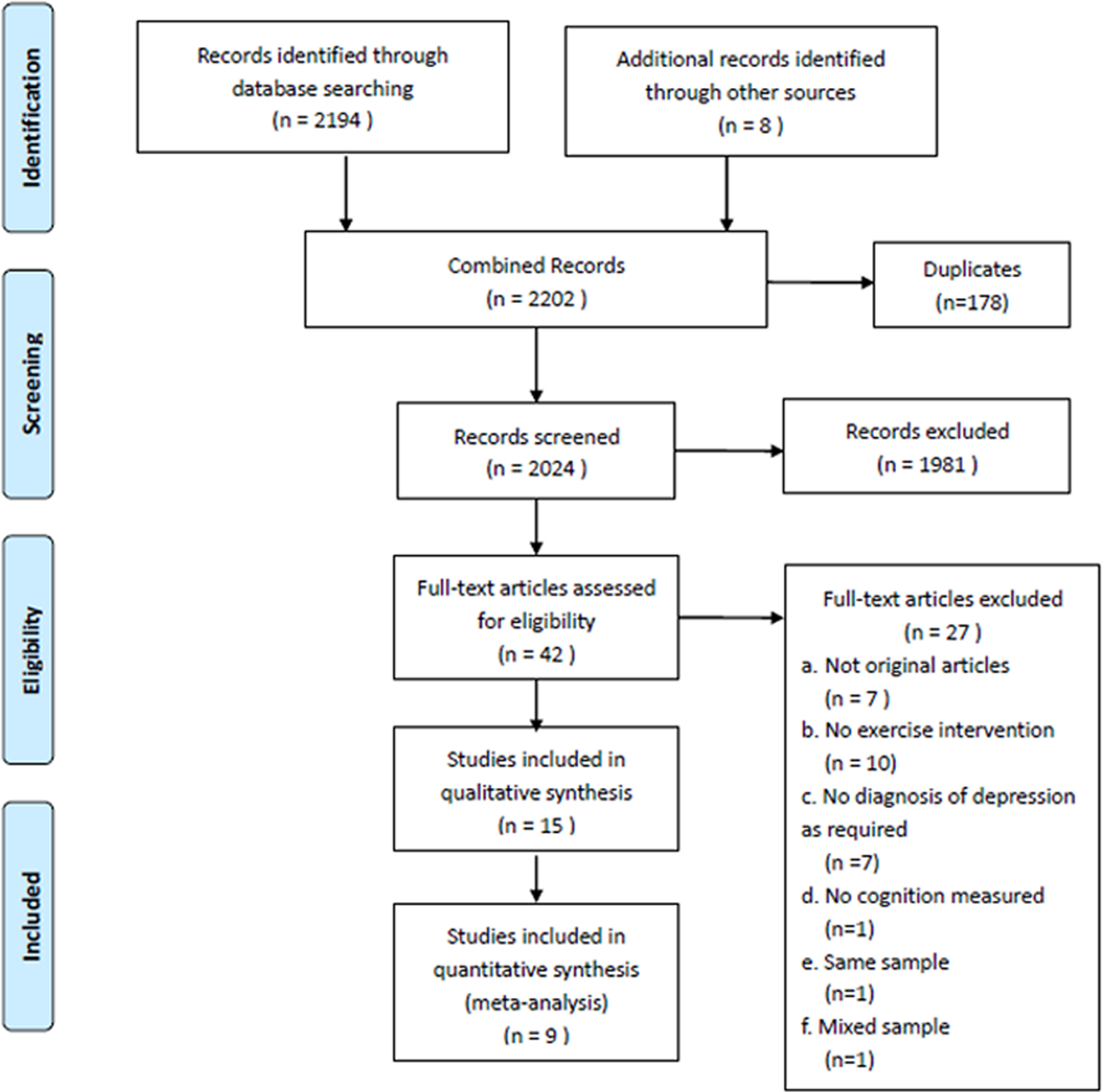
PRISMA flow diagram of the selection procedure.
Summary of Findings.
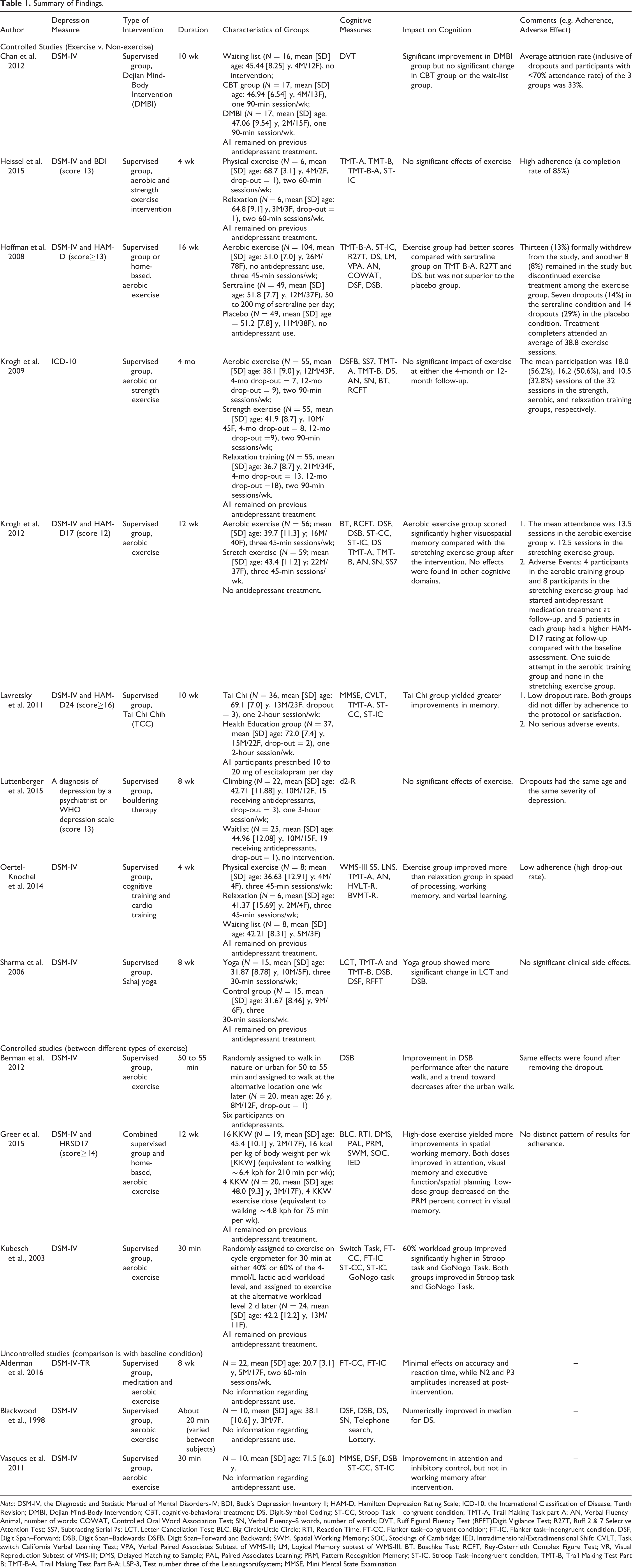
Note: DSM-IV, the Diagnostic and Statistic Manual of Mental Disorders-IV; BDI, Beck’s Depression Inventory II; HAM-D, Hamilton Depression Rating Scale; ICD-10, the International Classification of Disease, Tenth Revision; DMBI, Dejian Mind-Body Intervention; CBT, cognitive-behavioral treatment; DS, Digit-Symbol Coding; ST-CC, Stroop Task – congruent condition; TMT-A, Trail Making Task part A; AN, Verbal Fluency–Animal, number of words; COWAT, Controlled Oral Word Association Test; SN, Verbal Fluency–S words, number of words; DVT, Ruff Figural Fluency Test (RFFT)Digit Vigilance Test; R27T, Ruff 2 & 7 Selective Attention Test; SS7, Subtracting Serial 7s; LCT, Letter Cancellation Test; BLC, Big Circle/Little Circle; RTI, Reaction Time; FT-CC, Flanker task–congruent condition; FT-IC, Flanker task–incongruent condition; DSF, Digit Span–Forward; DSB, Digit Span–Backwards; DSFB, Digit Span–Forward and Backward; SWM, Spatial Working Memory; SOC, Stockings of Cambridge; IED, Intradimensional/Extradimensional Shift; CVLT, Task switch California Verbal Learning Test; VPA, Verbal Paired Associates Subtest of WMS-III; LM, Logical Memory subtest of WMS-III; BT, Buschke Test; RCFT, Rey-Osterrieth Complex Figure Test; VR, Visual Reproduction Subtest of VMS-III; DMS, Delayed Matching to Sample; PAL, Paired Associates Learning; PRM, Pattern Recognition Memory; ST-IC, Stroop Task–incongruent condition; TMT-B, Trail Making Test Part B; TMT-B-A, Trail Making Test Part B-A; LSP-3, Test number three of the Leistungsprüfsystem; MMSE, Mini Mental State Examination.
Among the 3 studies comparing different exercise environments, different exercise dosages and different levels of intensity, respectively, 83 patients with depression were included. The mean age was 40.4 y (12.5 y), and 68.7% were female (n = 57). Two studies used a randomized cross-over design, and one session intervention. 26,27
In the 3 uncontrolled studies, 42 patients with depression were included, and mean age was 36.9 y (SD, 21.7 y). In the 2 studies that reported the gender ratio, 75% were female. 13,28 In all of the above studies, 13 studies used DSM-IV for diagnosis, whereas one study used a cut-off on a validated depression scale and the other used ICD-10.
Risk of Bias in Included Studies
Bias assessments of individual studies are reported in Supplemental Figure S1. Of these, 11 studies had adequate random sequence generation, 21 –23,26,29 –34 whereas one did not provide sufficient information, 35 and there was no adequate random sequence generation in the 3 uncontrolled studies. Only 5 studies had adequate allocation concealment, 21 –23,29,30 and no study could achieve the blinding of participants and personnel because of the intervention type. Blinding of outcome assessment was reported in 6 studies. 21 –23,29 –31 Seven studies were at risk of bias from incomplete outcome data with no intention-to-treat (ITT) analyses, 13,21,26,28,31,32,34 whereas selective reporting was detected in 3 studies. 22,28,30 According to the Cochrane Collaboration’s tool, all of these studies should be considered as having a “high risk of bias”.
Meta-analysis & Meta-regression & Subgroup Analysis
The results of meta-analysis are shown in Figure 2. No significant effect of physical exercise was found on global cognition for the study participants with depression. There was no significant effect of physical exercise in terms of speed of processing, attention/vigilance, working memory, verbal learning and memory, visual learning and memory, or reasoning and problem solving. No significant evidence of heterogeneity was observed in global cognition and among all of the individual domains, except in the visual learning and memory domain (I2 = 68%; P = 0.04).
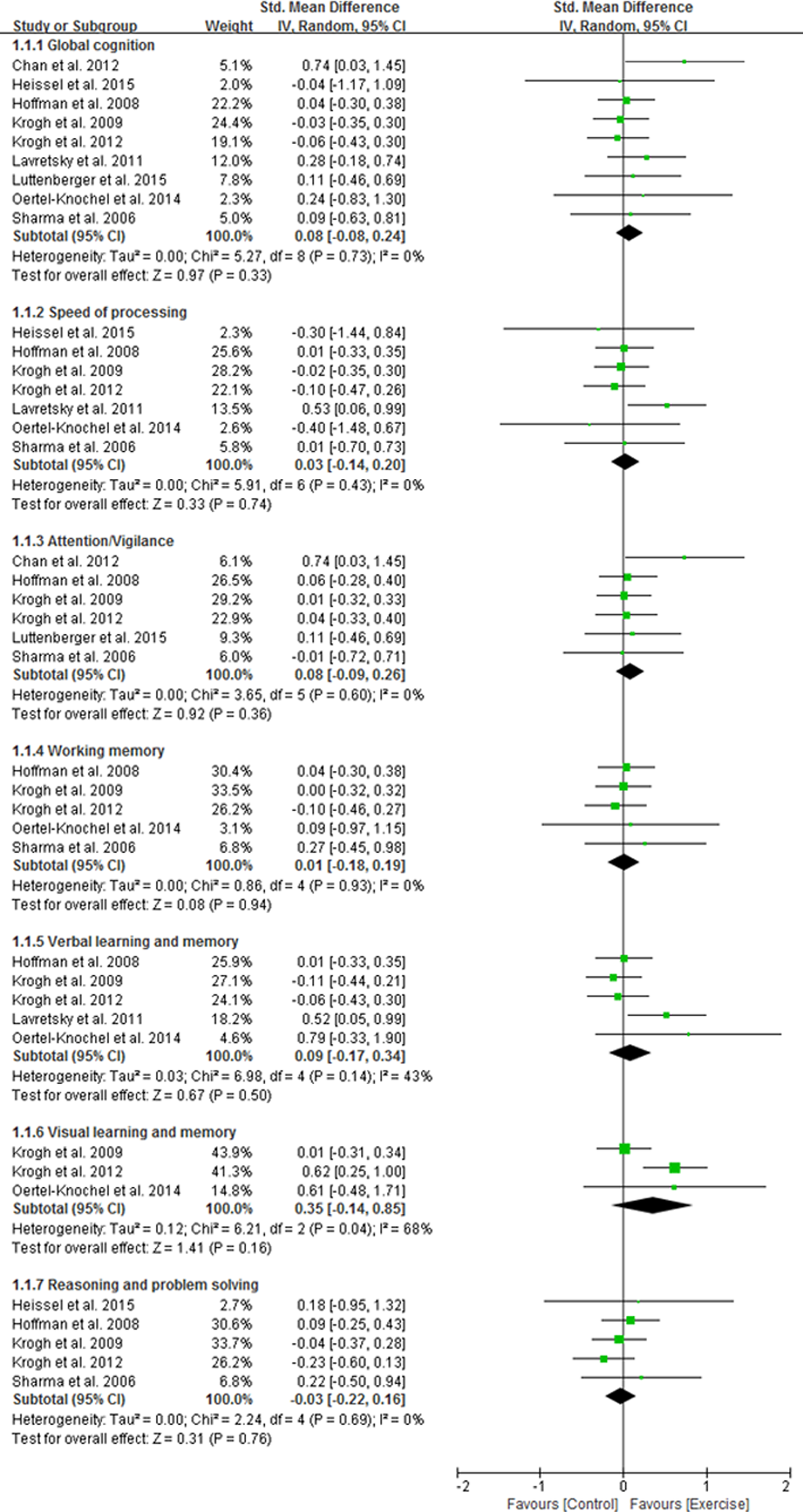
Forest plot of the effect of physical activity on cognition in depression.
Neither the funnel plot (Supplemental Figure S2) nor the Egger’s test (P = 0.188) suggested a publication bias. Removing each study from the overall effect size had no significant difference on our results (Supplemental Figure S3).
The meta-regression analyses also failed to detect a significant relationship between participant age (B = 0.0068, SE = 0.0077, t = 0.89, P = 0.401), baseline cognition (B = 0.0021, SE = 0.0012, t = 1.81, P = 0.121), sessions per wk (B = −0.1368, SE = 0.0991, t = −1.38, P = 0.210), exercise duration per wk (B = −0.0035, SE = 0.0028, t = −1.25, P = 0.253), total duration of exercise during the intervention (B = −0.0225, SE = 0.0231, t = −0.97, P = 0.364) and improvement in global cognition.
Adherence was determined according to the mean number of completed sessions for all participants, which was reported in 4 studies. Low-intensity exercise interventions had a high rate of adherence (≥70%, N = 1) and significantly improved global cognition (N = 3, n = 136, P = 0.048), whereas moderate- to high-intensity interventions generally had a lower rate of adherence (mean, 55.17%; range, 37.5% to 74.61%, N = 3) and did not impact significantly on global cognition (N = 6, n = 506, P = 0.969). No significant difference in cognition was detected between the 2 groups (P = 0.084; Figure 3).
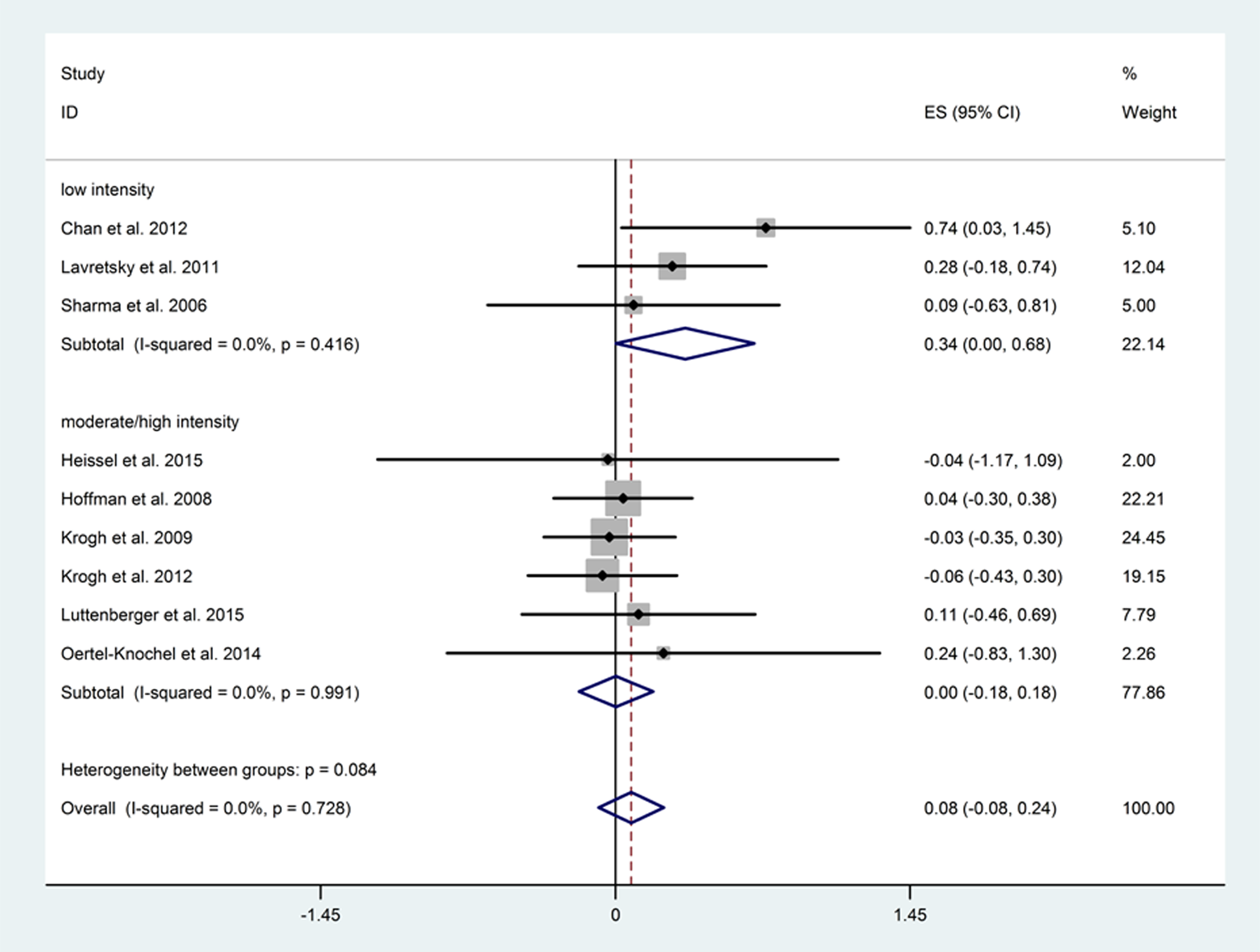
Subgroup analysis between different exercise intensity groups.
Exercise interventions that combined physical exercise with cognitive activity (including Dejian Mind-Body Intervention, Tai-chi, cognitive training and cardio training, and Sahaj yoga) significantly improved global cognition (N = 4, n = 150, P = 0.048), whereas those with physical exercise alone did not (N = 5, n = 492, P = 0.971); although the differences between the subgroups did not reach significance (P = 0.077; Figure 4).
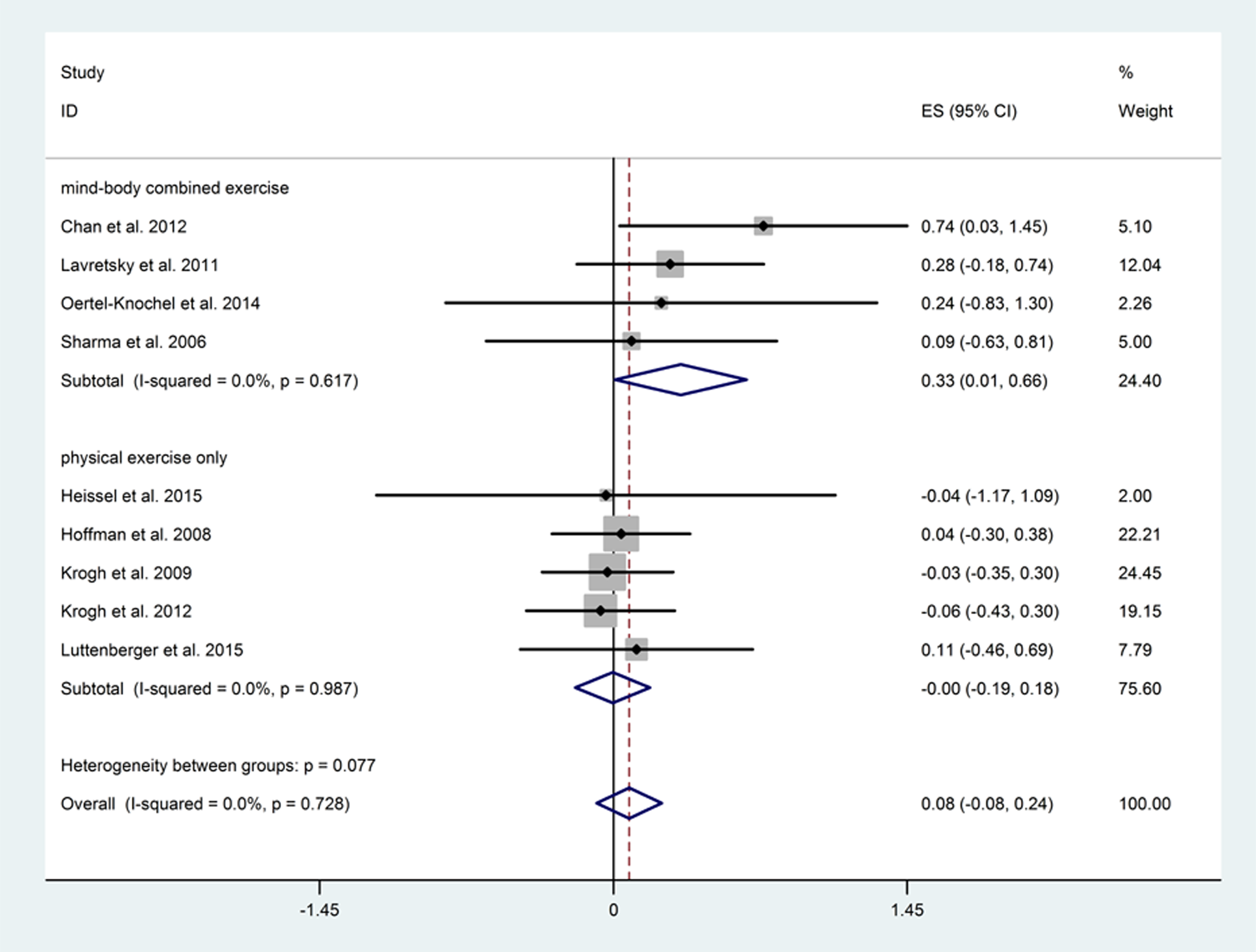
Subgroup analysis between different exercise types.
Discussion
In this meta-analysis, we failed to find a significant effect of physical exercise either on global cognition or on individual cognitive domains in study participants with depression. The impact was not influenced by the age of participants, baseline cognition, or the time spent exercising. However, interventions that combined physical exercise with cognitive activity significantly improved global cognition, and we also report positive findings for low-intensity interventions.
The lack of an overall positive impact of physical exercise on cognition in this meta-analysis is consistent with previously reported findings in this population. 12 However, this contrasts with findings in other populations, including those with dementia, 36 mild cognitive impairment, 37 and schizophrenia. 18 In some studies of healthy adults, positive findings have also been reported. 38 This may reflect the overall low dosage of physical exercise in the studies included (mean duration of 131 min), which is lower than the 150 min of moderate intensity per wk recommended by the World Health Organization. 39 Another variable, which may explain the generally negative findings in this meta-analysis, may be the lack of cognitive impairment at baseline in the samples included. Cognitive improvement may be greater in patients with more cognitive impairment at baseline. 38 None of the studies included in this meta-analysis required the presence of cognitive impairment at baseline, which may have resulted in an underestimation of the impact of physical exercise on cognition, particularly among those with cognitive impairment. An overall high risk of bias was noted among the included studies, which may have also impacted on the findings. All 3 uncontrolled studies found a positive effect for physical exercise on either speed of processing 28 or attention. 13,40 However, it is not possible to determine whether this represents a true effect of the intervention or simply reflects practice effects given the lack of a control group.
In the meta-regression analyses, we found that the impact of exercise on cognition was not influenced by the characteristics of participants, such as age and cognitive function at baseline. However, the under-representation of older participants and those with cognitive impairment at baseline could have resulted in reduced power to detect the impact of these factors. Some studies have suggested that physical exercise may have a greater impact on cognition in older persons and in those with cognitive impairment at baseline. 37,41 One study, published following the completion of this meta-analysis, reported a significant positive impact of progressive aerobic exercise on the cognition of older adults with depression, whereas those randomised to the non-progressive exercise group did not achieve significant cognitive benefits. 42 It is noteworthy that in that study, exercise was combined with antidepressant treatment, whereas, in many of the other studies, exercise was simply added to the existing treatment plan, which may or may not have included antidepressant medication. It is not possible, therefore, to determine whether the added use of antidepressant medication significantly moderated the effect of exercise on cognition in these subjects with depression.
The impact of exercise was not associated with time spent on physical exercise per wk or with the frequency or total duration of the exercise over the whole intervention, which is consistent with the only other meta-analysis published on this topic. 12 This may reflect the overall low dose of exercise in the included studies. We note that one study comparing different doses of exercise found a greater impact on cognition with higher doses of exercise, suggesting a positive relationship between dose and impact of exercise. 32
Significant improvement was found in the low-intensity group, whereas no effect was found in the moderate- to high-intensity groups. This contrasts with previous findings in the general population, 43 and may be explained by the reduced motivation and energy in depressed patients as well as the higher rate of attrition in studies with a longer duration of follow-up and higher intensity of exercise. We note that studies with a moderate- or high-intensity intervention generally had a lower rate of completion (mean of 55%), whereas lower-intensity interventions reported more favourable adherence (70%). One study, comparing the effects of different levels of exercise in depression, revealed greater cognitive benefits with higher levels of exercise. 27 However, both workload levels in this meta-analysis could be considered low intensity according to their defined lactic acid workload. 39
In subgroup analyses, we found that interventions combining physical exercise with cognitive activity—so called, mind-body interventions—significantly improved cognition. This finding is supported by a recent meta-analysis in healthy adults that found a significant benefit for interventions combining exercise with cognitive activity over exercise alone. 44 However, a recent randomized, controlled trial 45 in older adults with cognitive complaints failed to find significant differences between the combined effects of physical plus mental activity compared with that of physical or mental activity alone. The factorial design in that study may have resulted in reduced power to detect the combined impact on cognitive function. In this meta-analysis, yoga, tai chi, a Chan-based, mind-body intervention, and cognitive training combined with aerobic exercise were included in the combined group. The positive effects for yoga, tai chi, and cognitive training have been reported in previous studies 15,16,46,47 but their impact on cognition in depressed patients remains relatively underexplored. Both cognitive training and physical exercise are known to have positive effects on several mechanisms underlying neural plasticity and cognitive functioning. 48 –51 The interventions may have independent or additive effects on cognition and further investigation of the underlying mechanisms and predictors of response is required. 52 One study reported a greater benefit for walking in a natural compared to an urban environment. 26 Previous studies have reported that environmental enrichment may have beneficial effects upon cognition; although, it was not possible to definitively address this question here. 53
This systematic review has several strengths and limitations. The main limitation is lack of rigorous studies in this field, meaning that the findings reported here should be interpreted with caution. Another limitation is that different cognitive outcomes were used. This may have led to variability in estimates of the cognitive effects of exercise. However, we did not find significant evidence of heterogeneity for global cognition among the included studies. Individual cognitive domains were measured in only a small number of studies, and most studies assessed cognition as a secondary outcome or were part of larger trials. Most studies used an aerobic exercise intervention, which made it difficult to compare the relative impact of aerobic exercise v. resistance training. We conducted a series of meta-regression and subgroup analyses but note that some of these analyses may have been underpowered because of the limited number of studies. Finally, as all of these studies were conducted over a relatively short duration (range from 4 to 16 wk), it is not possible to determine the effects of exercise over a longer duration.
Conclusion
In conclusion, our meta-analysis failed to find a significant overall beneficial effect of exercise on cognitive symptoms in MDD. However, there is a relative lack of high-quality data in this population and negative findings may be attributable to methodological limitations among the included studies. In subgroup analyses, we found that interventions combining physical with cognitive activity had a positive impact upon cognition, whereas lower-intensity interventions, where adherence was improved, also had a positive impact. Future studies should determine how cognitive outcomes in depression vary according to the type of exercise intervention and the baseline characteristics of the study participants.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Authors declared that there is no conflict of interest in this systematic review. For included studies: Krogh et al (2012) reported two funders were conmmercial funders, and one co-author was an editor at PLOS ONE in their study; Authors had received grants and honoraria from several pharmaceutical companies in studies of Geer et al (2015) and Hoffman et al (2008); No declaration of conflicting interests were made in the study of Sharma et al (2006); All the other included studies declared no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.