
Abstract
Objective:
Stigma resistance (SR) has recently emerged as a prominent aspect of research on recovery from schizophrenia, partly because studies have suggested that the development of stigma-resisting beliefs may help individuals lead a fulfilling life and recover from their mental illness. The present study assessed the relationship between personal SR ability and prediction variables such as self-stigma, self-esteem, self-reflection, coping styles, and psychotic symptomatology.
Method:
We performed an exploratory cross-sectional study of 170 community-dwelling patients with schizophrenia. Self-stigma, self-esteem, self-reflection, coping skills, and SR were assessed through self-report. Psychotic symptom severity was rated by the interviewers. Factors showing significant association in univariate analyses were included in a stepwise backward regression model.
Results:
Stepwise regressions revealed that acceptance of stereotypes of mental illness, self-esteem, self-reflection, and only 2 adaptive coping strategies (positive reinterpretation and religious coping) were significant predictors of SR. The prediction model accounted for 27.1% of the variance in the SR subscale score in our sample.
Conclusions:
Greater reflective capacity, greater self-esteem, greater preferences for positive reinterpretation and religious coping, and fewer endorsements of the stereotypes of mental illness may be key factors that relate to higher levels of SR. These factors are potentially modifiable in tailored interventions, and such modification may produce considerable improvements in the SR of the investigated population. This study has implications for psychosocial rehabilitation and emerging views of recovery from mental illness.
Self-stigmatisation is highly prevalent among individuals with schizophrenia. 1,2 It occurs when people with mental illnesses agree with and internalise negative stereotypes and is typically associated with the shame and distress people feel at having a mental illness. 3 –5 The clinical interest in this construct stems from its relationship with inadequate adherence to medication and psychological treatment, which often results in inferior treatment outcomes, high relapse rates, increased symptom severity, and impaired psychosocial functioning. 6,7 As an initial step in investigating these psychological processes, Ritsher and colleagues 8 developed the Internalized Stigma of Mental Illness (ISMI) Scale, which is a self-report measure with 2 dimensions: self-stigma and stigma resistance (SR). Research has determined that SR is a separate construct, theoretically 7 –10 and psychometrically 11,12 distinct from self-stigma.
In more recent years, substantial evidence of the favourable effects of SR has been produced. For example, higher SR is associated with higher levels of self-esteem, empowerment, metacognitive capacity, and quality of social connections but also with lower levels of self-stigma and severities of depressive, positive, and negative symptoms. 9 –12 Furthermore, evidence exists that high SR may lead to individuals from stigmatised groups experiencing greater self-esteem and empowerment as well as a higher quality of life. 13,14 Research has suggested that exploring certain possible relationships of SR with sociodemographic and other clinical characteristics may explain why some patients develop SR, whereas others do not. 9 –15 An inconsistent link between SR and psychotic symptoms has been identified; several studies have reported that higher SR is related to lower positive or negative symptom levels, whereas other studies have identified no relationship. 10 To date, research on the relationship between SR and sociodemographic variables has been limited and has suggested that no relationship exists between SR and sociodemographic variables (e.g., age and education). 9,11
Reduced self-esteem has been proposed as a main consequence of mental illness or mental illness stigma. 6 Lower self-esteem may also contribute to greater social alienation. 16 This vicious cycle relegates many people with severe mental illness to a lifetime of social segregation and isolation. Studies have reported that elevated self-esteem can reduce self-stigma as well as its harmful effects. 17,18 Furthermore, self-esteem is reportedly closely connected to SR. 9 –12
Self-reflection, considered a metacognitive process, 19 refers to the processes through which people focus on their feelings, emotions, thoughts, and experiences to gain insight, learn from their mistakes, and improve themselves. 20,21 Individuals with schizophrenia generally have compromised capacity for self-reflection, 22,23 which has been linked to symptoms, 24 impaired insight, 20,23 high self-stigma, 25 maladaptive coping, 26,27 learning difficulties, 28,29 and inferior psychosocial functioning. 30,31 Although greater reflective processing capacity has been reported to be related to greater insight into illness, it can also imply a greater chance of adapting stigmatising labels and internalising stigmas. 25 For these reasons, studies on self-reflection in people with schizophrenia have attracted increasing attention. However, at present, the relationship between self-reflection and SR in patients with schizophrenia is still unclear.
Being diagnosed with a severe mental illness is typically a stressful and unsettling experience. Coping with the broader implications of a mental illness is a difficult and often lifelong process. 32,33 Individuals with schizophrenia often report and demonstrate significant difficulty coping with life stresses. 34 –36 People with schizophrenia, compared with people without a mental illness, often employ a more limited range of coping strategies, which are characterised by a preference for avoidance and passive coping rather than help-seeking or active problem-solving approaches. 34,37,38 Because of the need to identify the conditions and patient coping strategies that intensify the SR process, how coping strategies relate to SR among patients experiencing internalising stigma should be characterised. Coping preferences may be another individual difference that distinguishes high levels of SR from lower levels of SR in patients with schizophrenia. Nevertheless, this relationship remains to be empirically investigated.
After reviewing the aforementioned studies, we aspired to ascertain the relative importance of these multiple associations, because how these factors are associated with SR remains unclear. Furthermore, most studies have been limited to Western populations. Thus, we conducted exploratory research to investigate the effects of sociodemographic and clinical variables on SR among Chinese individuals diagnosed as having schizophrenia. We hypothesised that self-stigma, self-esteem, self-reflection, and coping strategies significantly predict SR. Specifically, we expected that individuals with lower self-stigma levels, higher self-esteem levels, greater reflective capacity, and more favourable coping preferences would more effectively resist stigma. We used multivariate regression analysis with backward-stepwise elimination, which is a set of approaches for evaluating the order of importance of variables and for selecting useful subsets of variables; the approaches are therefore suited to managing exploratory data. 39,40 Finally, this article outlines the practical implications of SR interventions.
Participants
Power analysis for multiple regression using 25 observed variables, a medium effect size of 0.2, and a probability of 0.05 yielded a recommended minimum sample size of 134 and a power of 0.8. 41,42 A convenience sample of 190 participants was recruited to ensure an adequate sample size. All outpatients diagnosed as having schizophrenia or schizoaffective disorder according to the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR), 43 were recruited consecutively in 2013 and 2014 from 2 hospitals’ outpatient psychiatric clinics. Participants were receiving ongoing outpatient treatment and were in a stable clinical condition, which was defined as no hospitalisations or changes in medication within the preceding 6 months. Participants were excluded if they 1) were younger than 18 years or older than 65 years, 2) had a history of brain trauma or neurological disease, 3) presented with symptoms of alcohol or substance abuse and dependence in the 12 months prior to participation, or 4) could not provide informed consent. Ethical approval was obtained from the Institutional Review Board of the Tri-service General Hospital, National Defense Medical Center, Taiwan (ID: SS100-05). After comprehensively explaining the study methodology and procedures for protecting confidentiality, the participants were asked to provide written informed consent. We initially invited 190 individuals to participate in this study; 5 respondents refused to participate, and 15 did not meet the study’s eligibility criteria. Ultimately, 170 respondents (response rate: 89%) accepted our invitation. Data on sociodemographic characteristics (e.g., age, sex, and education) and self-reported illness duration were documented.
Measures
Self-Stigma and SR
The ISMI scale is a 29-item self-administered questionnaire for measuring the self-stigma and SR associated with mental illness. 8 Each scale item was rated on a 4-point Likert scale, and high scores indicated high self-stigma or SR levels. The ISMI scale contains 5 subscales: alienation, stereotype endorsement, discrimination experience, social withdrawal, and SR. The Chinese version of the ISMI scale has favourable internal consistency, favourable test-retest reliability, and adequate convergent and construct validity. 12 In the present study, satisfactory internal consistency was identified (0.70-0.88).
Self-Reflection
To evaluate the subjects’ self-reflection, we used the self-reflectiveness subscale of the Beck Cognitive Insight Scale (BCIS). 44 The BCIS is a 15-item self-report scale, with items rated from do not agree at all (scored 1) to agree completely (scored 4). Kao et al. 45 validated a Chinese version of the BCIS and reported that it has adequate psychometric properties. The self-reflection subscale (9 items) assesses willingness to accept fallibility and external feedback as well as recognising dysfunctional reasoning style, for which a higher score indicates higher levels of self-reflection. In the present study, the Cronbach’s α for this subscale was 0.78.
Self-Esteem
The unidimensional self-report Rosenberg Self-esteem Scale (RSES) comprises 10 items that are coded using a 4-point Likert scale identical to that used in the ISMI scale. 46 Higher scores on the RSES indicate higher self-esteem levels. In a previous study, the Chinese version of the RSES exhibited high internal consistency and adequate convergent validity. 47 The scale also exhibited high internal consistency in this study (Cronbach’s α = 0.92).
Coping Styles
The COPE is a multidimensional coping inventory that assesses how an individual manages difficult situations. 48 The COPE scale comprises 53 items measuring 14 strategies, split into overarching domains of adaptive and maladaptive strategies. The adaptive domain averages the following subscales: 1) positive reinterpretation, 2) venting of emotions, 3) use of instrumental social support, 4) active coping, 5) religious coping, 6) restraint, 7) use of emotional social support, 8) acceptance, 9) suppression of competing activities, and 10) planning. The maladaptive domain averages the following subscales: 1) mental disengagement, 2) denial, 3) behavioural disengagement, and 4) substance use. The Chinese version of the self-report scale was reported to exhibit favourable reliability. 49 Each item in the COPE is scored using a 5-point Likert scale from not at all to very much, indicating how much people engage in each type of activity when they encounter a difficult, upsetting, or stressful situation. In our sample, all subscales demonstrated acceptable internal consistency (0.70-0.82). The adaptive and maladaptive domains were recalculated accordingly and demonstrated excellent reliability in our sample (Cronbach’s α = 0.88 and 0.84, respectively).
Psychotic Symptomatology
Psychotic symptom severity was assessed using the Positive and Negative Syndrome Scale (PANSS), 50 Chinese version. 51 The PANSS is a 30-item semistructured interview scale and was developed to comprehensively assess the symptoms of schizophrenia. 50 For the purposes of this study, 2 of 3 analytically derived components were used: positive and negative symptoms. 51 They contain 7 items each with possible overall scores ranging from 7 to 49, in which a higher score indicates a higher severity of psychotic symptoms.
Statistical Analysis
The data were analysed using Statistical Product and Service Solutions, version 15.0 (SPSS, Inc., an IBM Company, Chicago, IL). Descriptive analysis included calculation of means, standard deviations (SDs), skewness, and the kurtosis of the indicator variables. Compared with the normal distribution, all variables remained under the critical value of 7 for kurtosis and 2 for skewness. 52 Independent t tests were used to assess between-sex differences in the main variables. In each case, the ISMI-SR score was entered as the dependent variable, and all sociodemographic and clinical variables were entered as independent variables.
Selection of variables in the stepwise multiple regression model was based on the exploratory univariate linear regressions conducted in the present study between SR and prediction variables with assumed clinical importance. All variables that were significantly associated with SR in the univariate analyses at a P < 0.05 level were included as independent variables and subsequently subjected to stepwise multiple regression to search for their contribution to SR. The fit of the model was tested after elimination of each variable to ensure that the model still adequately fit the data. When no more variables could be eliminated from the model, the analysis was complete. 38
Results
Of the 170 participants, 93 (55%) were men and 147 (86%) were unmarried or single. Most participants were unemployed (n = 125, 73.5%). The average age of the patients was 44.4 years (SD = 10.1; range, 19-65), and their mean duration of formal education was 12.3 years (SD = 2.69; range, 6-18). The mean age of illness onset was 26.4 years (SD = 7.26; range, 14-50). The mean illness duration was 17.9 years (SD = 10.0; range, 2-45). The descriptive statistics for the measures are presented in Table 1. The results revealed no difference between the main variables between the sexes except for in 2 adaptive subscales: venting of emotion and acceptance (t = −3.34 and −2.68, respectively; both P < 0.01).
Descriptive Statistics of All Indices Related to Stigma Resistance, Self-Stigma, Self-Reflectiveness, Self-Esteem, Coping Styles, and Psychotic Symptoms (n = 170).
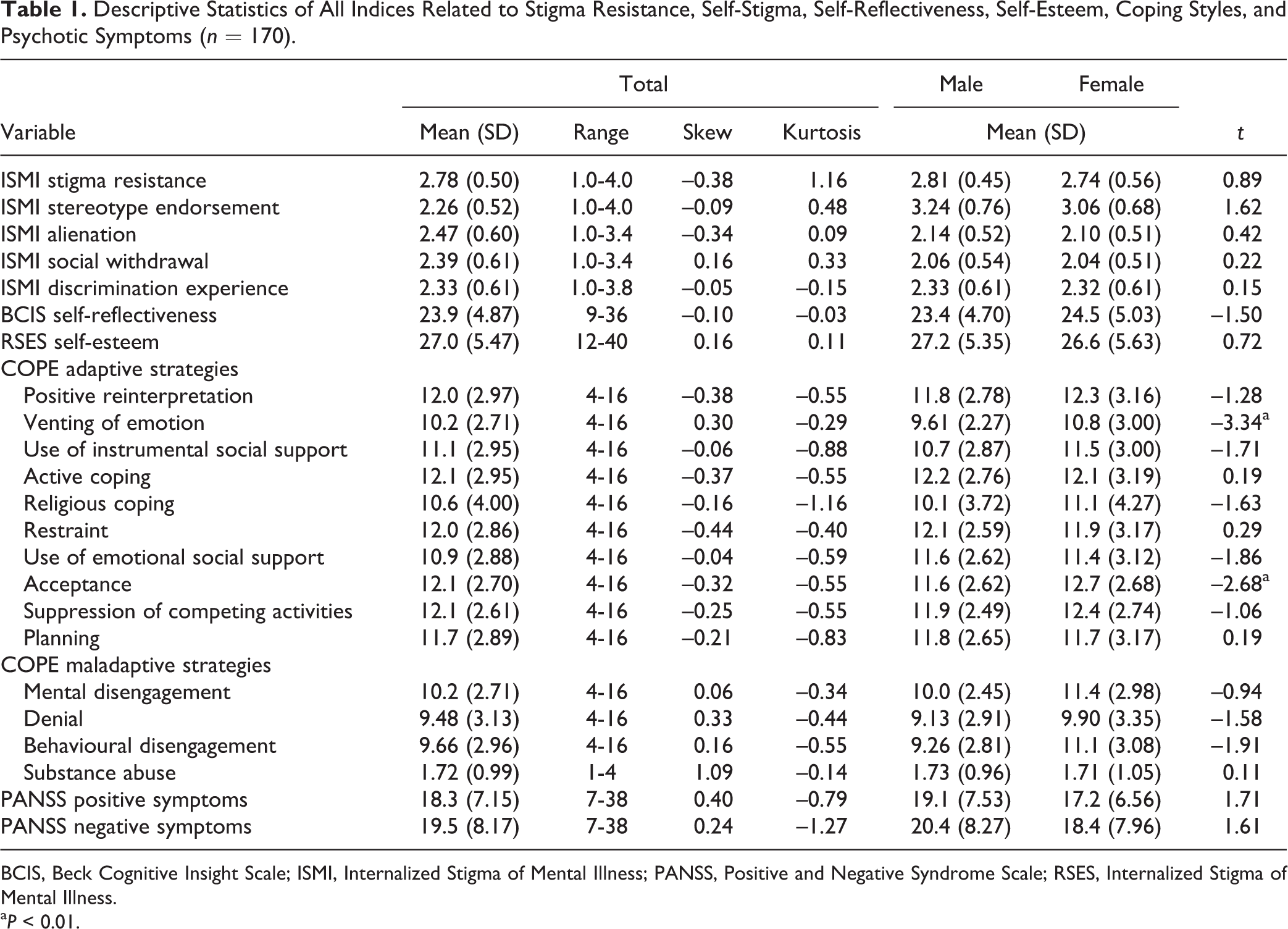
BCIS, Beck Cognitive Insight Scale; ISMI, Internalized Stigma of Mental Illness; PANSS, Positive and Negative Syndrome Scale; RSES, Internalized Stigma of Mental Illness.
a P < 0.01.
We performed univariate regressions for ISMI-SR scores with any of the sociodemographic and clinical variables assessed. These analyses provided a preliminary screening of appropriate candidate variables for entry into a stepwise multiple regression model, as described hereinafter. On the basis of these preliminary univariate associations, P < 0.05 was adopted for inclusion in the regression model. The following variables were selected for the ISMI-SR model: ISMI stereotype endorsement (β = −0.31, P < 0.001), ISMI alienation (β = −0.28, P < 0.001), ISMI social withdrawal (β = −0.18, P = 0.02), ISMI discrimination experience (β = −0.19, P = 0.01), BCIS self-reflection (β = 0.18, P = 0.02), RSES self-esteem (β = 0.37, P < 0.001), and all COPE adaptive strategies (β = 0.20-0.38, all P < 0.05). Some sociodemographic (i.e., age and education) and clinical (i.e., illness duration, psychotic symptom severities, and all maladaptive coping strategies) variables were nonsignificantly related to the dependent variable in the univariate analysis (Table 2). Hence, we did not include these variables in the subsequent analyses.
Exploratory Univariate Regression between Stigma Resistance and Sociodemographic and Clinical Characteristics.
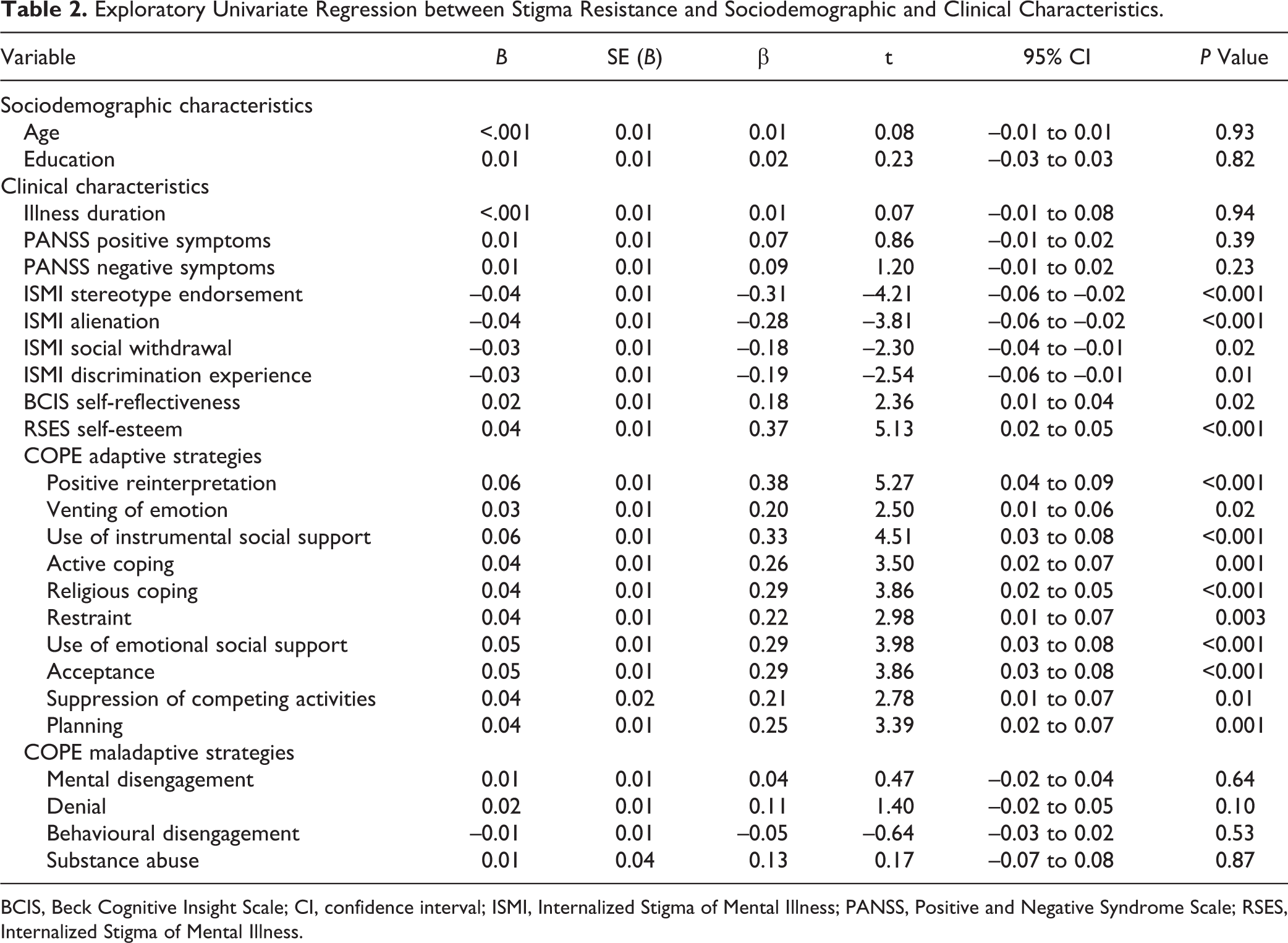
BCIS, Beck Cognitive Insight Scale; CI, confidence interval; ISMI, Internalized Stigma of Mental Illness; PANSS, Positive and Negative Syndrome Scale; RSES, Internalized Stigma of Mental Illness.
To identify the most significant variables connected to SR, backward-stepwise multiple-regression analysis was performed using the ISMI-SR score as the dependent variable and various psychological measures showing a significant correlation in the univariate linear regression analyses as independent variables. We also performed stepwise regression to determine which adaptive coping strategies were significantly associated with SR. After backward selection of variables, the combination of 5 predictor variables provided the best-fit ISMI-SR model to the data. This regression model was significant (F = 12.2; df = 5, 164; P < 0.001), accounting for 27.1% of the variance in SR. Only 2 adaptive coping strategies, positive reinterpretation (β = 0.15, P = 0.04) and religious coping (β = 0.17, P = 0.03), were significantly associated with SR. Furthermore, acceptance of the stereotypes of mental illness (β = −0.23, P = 0.004), self-reflection (β = 0.16, P = 0.04), and self-esteem (β = 0.20, P = 0.02) accounted for a significant amount of variance in SR among the patients with schizophrenia. No other variables were significant (Table 3).
Multiple Regression with a Backward Stepwise Procedure for Specific Adaptive Coping Strategies: Contributors to Stigma Resistance.
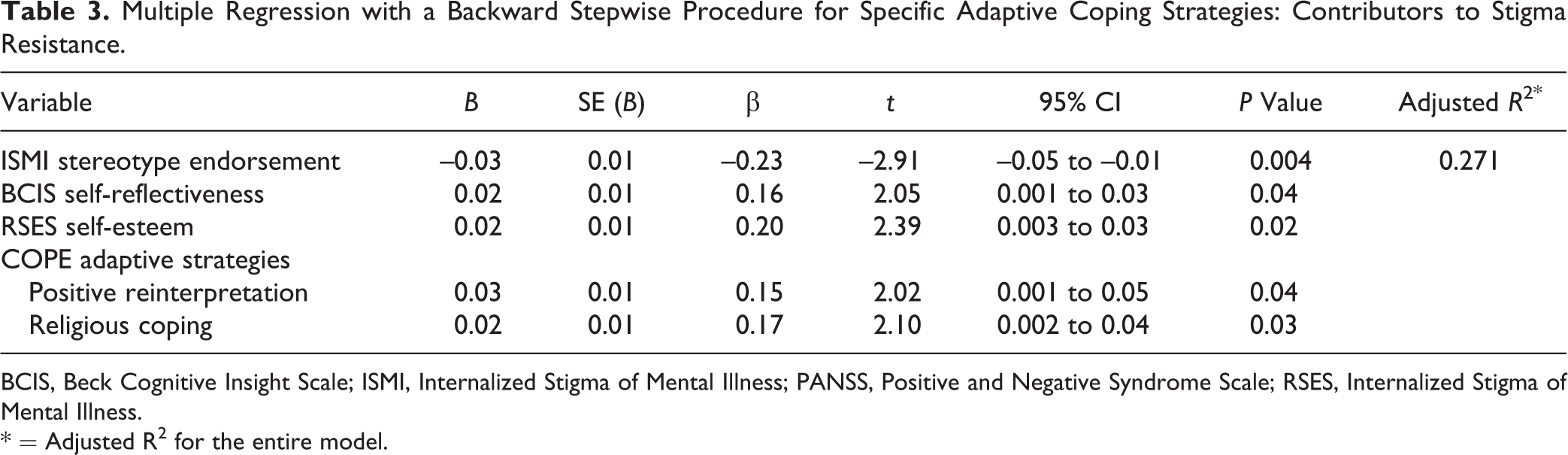
BCIS, Beck Cognitive Insight Scale; ISMI, Internalized Stigma of Mental Illness; PANSS, Positive and Negative Syndrome Scale; RSES, Internalized Stigma of Mental Illness.
* = Adjusted R2 for the entire model.
Discussion
This is the first study, to our knowledge, to systematically analyse the role of self-stigma, self-esteem, self-reflection, and 2 different coping strategies (adaptive and maladaptive) in SR among patients with schizophrenia. Our exploratory clinical study revealed 5 main findings. First, consistent with our hypothesis and previous studies, 9,11,12 we determined that self-stigma was inversely related to SR. Second, also consistent with our hypothesis and the literature, 9 –12 self-esteem was positively associated with SR. Third, as expected, our results confirmed that self-reflection correlated positively with SR. Fourth, the results revealed that adaptive coping strategies, but not maladaptive coping strategies, were positively related to SR. We noted that the stepwise regression results showed that greater SR was linked with less self-stigma but greater self-reflection and self-esteem. The results further showed that greater SR was related to a more adaptive coping style and, specifically, that greater use of the adaptive strategies of positive reinterpretation and religious coping was significantly associated with higher SR. Finally, in line with previous findings, 9,11,15 the present study discovered no significant differences in the relationship of the ISMI-SR subscale score with sociodemographic and clinical variables (e.g., age, education, and positive and negative symptoms).
The findings of this study indicate that self-esteem is both a product of socially constructed experiences 53 and a factor that shapes an individual’s indices of distress. 54 Self-esteem may also contribute to higher success motivation. 55 In addition, it may increase the ability to achieve goals, manage emotions, and cope with problems, whereas low self-esteem may lead to avoidance. 56,57 For example, higher self-esteem may increase motivation to engage in self-care behaviours that ultimately reduce symptoms, and it may improve coping skills, thereby reducing stigma and increasing a person’s capacity to counteract the stigma of mental illness.
The past decade has seen an increase in research on the correlates and consequences of inadequate self-reflective capacity. In particular, self-reflective processing is essential for evaluating personal behaviour 58 and developing emotional intelligence. 59 Performing reflective practice with a professional helps people avoid excessive negative emotions, such as defensiveness or regret. 60 Thus, our findings relate to the relationship of SR with emotion regulation and are consistent with those of a recent study. 61 Rajj et al. 61 demonstrated a relationship between the brain circuitry for emotional regulation and resistance toward the stigma of schizophrenia in the rostral-ventral medial prefrontal cortex and suggested that enhanced emotion regulation directly contributes to SR in addition to an individual’s ability to interact socially and benefit from social support. Because current data suggest that evidence-based psychoeducational and cognitive remediation programs improve aspects of self-reflection, 62,63 this study’s findings indicate that clinicians and researchers working with people with schizophrenia must develop tailored adjunctive interventions that can be administrated alongside these evidence-based programs, attending to the recovery of patients. However, studies have suggested that an unexpected effect of intervention benefits is that more self-reflection leads to higher stigma levels. 24,25,62,64,65 These findings suggest that self-reflection is a double-edged sword for people with schizophrenia and complicates researchers’ understanding of the impact of self-reflection on clinical outcomes. Increased reflection allows individuals to be not only cognisant of the stigmatising beliefs that are caused by their illness but also the need to combat these stigmatising beliefs. Nevertheless, future studies must clarify which other factors play key roles in influencing self-reflection related to self-stigma and SR.
Identifying the coping strategies most central to SR may help highlight the most relevant cognitive techniques for stigmatised individuals. The results of this study suggested that a greater preference for using 2 adaptive coping strategies—namely, positive reinterpretation and religious coping—were independent correlates of SR in schizophrenia. Carver et al. 48 suggested that the value of positive reinterpretation is that it not only reduces distress but also can be used to reappraise a stressful situation and see it more positively. According to Cooke et al., 66 finding meaning in this coping is a vital strategy that helps patients reframe their unusual mental experiences by attributing to them a spiritual meaning. Thus, employing a positive coping strategy such as reinterpretation, rather than a denial coping strategy, may substantially reduce distress. 66 The neuropsychological model supports that the median prefrontal cortex is partly comparable with the brain regions key to positive reappraisal and optimism, 67,68 and this fits with the view of SR as encompassing different but related elements such as enhancing emotion regulation or eliciting positive emotions. Another adaptive coping strategy, religious coping, was also determined to be positively related to SR in schizophrenia. The role of religion in coping strategies for responding to stressful events has been empirically studied in patients with schizophrenia. 69 –72 Our findings suggested that religion is relevant when treating individuals with schizophrenia because it helps reduce symptom severity, enhances adaptive coping, and fosters recovery. 69 –72 Religious coping enhances patients’ personal resilience and self-efficacy, which are vital for coping with illness experiences such as residual symptoms and stigma. 11,72,73
Increasingly, researchers have reported that cultural factors influence a range of phenomena in schizophrenia. 37,74 Culture shapes various aspects of the self, including feelings of self-esteem, 75,76 self-stigma, 77 and coping styles. 78 In China, traditional cultural values include collectivistic and sociocentric cultural components in which people from birth onward are integrated into cohesive groups, long-term relationships, and extended family structures, which may provide buffering mechanisms against the occurrence of distress by improving self-esteem in people with severe mental illness 37,75 or may devalue individual instincts by tending to lower self-esteem. 76 In addition, Chinese culture may lead to intensified stigma. 77,79
Several limitations may have affected this study. First, generalisation of our findings is limited by the sample origin and illness stage of the participants. Second, the present study was cross-sectional in nature, so clear causal associations between SR and predictors could not be determined and should be elucidated by longitudinal studies. Third, although validated for use in studies on schizophrenia, 7,8,12 the validity of the construct of the SR subscale should be discussed, considering its relatively low internal reliability compared with the other 4 subscales of the ISMI scale. Finally, the self-reflectiveness subscale of the BCIS that was used in this study was originally developed for assessing cognitive insight. This subscale includes different elements from the other measures of self-reflection that have been widely used. Thus, more finely tuned or widely accepted measures of self-reflection such as the Metacognitive Assessment Scale, 80 Metacognitive Assessment Scale–Abbreviated, 81 Meta-Cognitions Questionnaire, 82 or self-reflectiveness task 23,83 are necessary to replicate and confirm the importance of our findings.
Conclusions
Although our findings may be tentative, this study substantially extended the insight into the underlying mechanisms of SR development among people with schizophrenia. To date, several interventions have been developed to directly address self-stigma, and many are in the early stages of development with limited effectiveness information available. 84 By advancing the understanding of stigmatisation’s multifaceted pathways and the components and factors that affect these pathways, we hope that the contributions in this article assist readers in precipitating the dismantling of self-stigma. With replication across broader samples and using longitudinal designs, our findings may have crucial clinical implications for designing psychoeducational programs to fight stigma.
Footnotes
Acknowledgements
We thank Prof. Ritsher, the original ISMI scale designer, for permission to administer the ISMI scale in our study. We also thank all participants who kindly volunteered to take part in this study
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Science Council, Taiwan (NSC 101-2314-B-003-002, 102-2410-H-003-016). This article was subsidised by the National Taiwan Normal University (NTNU), Taiwan, ROC.