
Abstract
Objective:
The objective of this article is to identify best practices in the diagnosis and assessment of patients with schizophrenia spectrum and other psychotic disorders. The diagnosis and assessment may occur in a range of situations from the emergency room to the outpatient clinic and at different stages of the disorder. The focus may be on acute exacerbations of illness, residual symptoms, levels of function, or changes in the response to treatment.
Methods:
A systematic search was conducted for guidelines published in the last 5 years for schizophrenia and schizophrenia spectrum disorders. The guidelines were rated by at least 2 raters, and recommendations adopted on the diagnosis and assessment were primarily drawn from the American Psychiatric Association practice guidelines for the psychiatric evaluation of adults and the National Institute for Health and Care Excellence guideline on psychosis and schizophrenia in adults. A number of de novo recommendations were also developed.
Results:
Eleven recommendations were identified that cover a range of assessment situations from diagnosis to the involvement of families in assessments.
Conclusions:
An accurate assessment establishes the baseline for treatment planning based on clinical decision making for both pharmacotherapy and psychosocial treatments.
Keywords
The assessment of individuals with schizophrenia follows the same general principles as any other psychiatric assessment. An assessment is the process of obtaining information about a patient through a variety of methods, including face-to-face interviews, reviews of medical records, physical examinations, diagnostic testing, and history taking from other sources. 1 This article focuses on assessments for diagnosis and ongoing treatment. Some aspects of the assessment of physical health are addressed in more detail in the article on physical health, and there is more detail on the assessment of comorbid substance use in the article on comorbid substance use. Assessments to support decision making on pharmacotherapy such as an assessment of treatment resistance are addressed in the article on pharmacotherapy.
Diagnosis of Schizophrenia
Like all mental disorders, schizophrenia spectrum and other psychotic disorders are diagnosed based on clinical features. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition 2 (DSM-5) uses a categorical approach to classifying mental disorders but also recognizes that symptom domains such as psychosis involve multiple diagnostic categories. Schizophrenia is not the only diagnosis that has psychotic symptoms included in its diagnostic criteria. Psychotic symptoms may occur in both bipolar disorder and major depressive disorder, where they are described as mood-congruent or mood-incongruent psychotic symptoms. Psychotic symptoms also occur in substance-related and addictive disorders. 2 The schizophrenia spectrum and other psychotic disorders section of the DSM-5 includes schizophrenia, other psychotic disorders, and schizotypal personality disorder.
There are 5 key features that define schizophrenia spectrum and other psychotic disorders. These include delusions, hallucinations, disorganized thinking (inferred from speech), grossly disorganized or abnormal motor behaviour, and negative symptoms. 2 For schizophrenia specifically, the presence or absence of specific psychotic symptoms identified as first-rank symptoms (auditory hallucinations; thought withdrawal, insertion, or interruption; thought broadcasting; somatic hallucinations; delusional perception; feelings or actions controlled by external agents) may be particularly helpful for making the diagnosis. 3 Negative symptoms, although less prominent during the acute phase, reflect reductions in previous levels of behaviour or drive. These include affective flattening (diminished emotional expression), avolition (reduction in self-initiated purposeful activity), alogia (poverty of thought or poverty of thought content), and anhedonia (decreased ability to experience pleasure from positive stimuli). Diminished emotional expression and reduced motivation appear to be the core negative symptoms. 4
In the DSM-5, the schizophrenia spectrum and other psychotic disorders chapter organizes disorders along a gradient of psychopathology from conditions that do not reach full criteria for a psychotic disorder such as schizotypal personality disorder or are limited to one domain of psychotic symptoms such as delusional disorder or catatonia. Next are more time-limited conditions such as brief psychotic disorder, which lasts more than a day and remits by 1 month. In schizophrenia, the disorder must persist for at least 6 months and include at least 1 month of active-phase symptoms. Schizophrenia is further distinguished by the requirement to demonstrate a markedly impaired level of function.
Accurate early identification and assessments are central to early intervention services. Although the unspecified schizophrenia spectrum diagnosis is often used at the initial assessment, following 1 year of engagement with early intervention services, the diagnoses become more specific, and a higher proportion will meet the criteria for schizophrenia. 5 Not surprisingly, the diagnosis of substance-induced psychotic disorder made in the emergency department is notoriously unreliable due to the lack of comprehensive information to support the exclusion of a psychotic disorder that is not substance induced. Even in research studies, there is weak agreement between initial clinical assessments and initial research assessments, and many such diagnoses are revised later. 6 The attenuated psychosis syndrome is mentioned without specific criteria in section II of the DSM-5, referring to other specified schizophrenia spectrum and other psychotic disorder. The attenuated psychosis syndrome is noted in section III of the DSM-5 as a condition for further study, including proposed criteria. The proposed criteria in section III were set by expert consensus with an intention of providing a common language for researchers and clinicians who are interested in studying these disorders, but the criteria are not intended for clinical use.
The range and nature of symptoms of schizophrenia and the need to assess levels of function make it essential for the clinician to obtain information from as many sources as possible when making a diagnosis. The most reliable way of making a diagnosis combines structured clinical interviews and information from multiple informants as well as a review of previous medical records. Structured diagnostic interviews prove to be more reliable than unstructured interviews, 7 and diagnoses are more reliable when the best-estimate lifetime psychiatric diagnostic method is used. 8 The structured clinical interview for the DSM achieves good reliability 9 and has been updated for the DSM-5. 10 Several semistructured diagnostic interviews are also available for adolescents. 11 The most widely used has been the Schedule for Affective Disorders and Schizophrenia for School-Age Children. 12 Reliable diagnoses can be made at the time of the first episode of psychosis, with the understanding that the specific diagnosis may change after a year.
The assessment recommendations in this article came primarily from the American Psychiatric Association (APA) practice guidelines for the psychiatric evaluation of adults, 13 the National Institute for Health and Care Excellence (NICE) guideline on psychosis and schizophrenia in adults: treatment and management, 14 and the practice parameter for the assessment and treatment of children and adolescents with schizophrenia. 15 The recommendations on genetic testing are based on the genetic testing statement of the International Society of Psychiatric Genetics (ISPG). 16 The assessment guideline includes more de novo recommendations than the other guidelines because some of the APA guidelines were combined or the wording changed to fit the Canadian context. These changes went beyond the minor word changes that would allow them to be described as modified. The guideline on genetic testing was not addressed in other clinical practice guidelines and was considered a significant omission from those guidelines, given the strength of evidence in the statement.
Methods
The methods for the Canadian Schizophrenia Guidelines are described in brief here; please see the Introduction and Methodology paper for an in-depth description. The guidelines were developed using the ADAPTE process. 17 Recognizing that the development of guidelines requires substantial resources, the ADAPTE process was created to take advantage of existing guidelines and reduce the duplication of effort.
The first phase of the ADAPTE process, the setup phase, involved preparing for the ADAPTE process. We assembled a national multidisciplinary panel from across Canada, including stakeholders with expertise in schizophrenia and mental health, health policy, patient advocacy, and lived experience with schizophrenia. Endorsement bodies for the guidelines include the Canadian Psychiatric Association (CPA) and the Schizophrenia Society of Canada, who were also heavily involved in the dissemination and implementation strategy.
The second phase of the ADAPTE process, the adaptation phase, involved identifying specific health questions; searching for and retrieving guidelines; assessing guideline quality, currency, content, consistency, and applicability; decision making around adaptation; and preparing the draft-adapted guideline. We searched for guidelines on schizophrenia in guideline clearinghouses and on the websites of well-established guideline developers for mental health disorders including the NICE, Scottish Intercollegiate Guidelines Network, APA, American Academy of Child and Adolescent Psychiatry, and European Psychiatric Association. A MEDLINE search was also performed using the terms “guideline” as the publication type and “schizophrenia” as the title or clinical topic. Inclusion criteria were that the guideline needed to be published after 2010, the guideline be written in English, and recommendations be developed using a defined and systematic process. We identified 8 current guidelines that were potentially suitable for adaptation. 1,18 –22 These guidelines were reviewed and evaluated in duplicate using the AGREE II tool, 23 an instrument to evaluate the methodological rigour and transparency with which a guideline is developed. Based on this evaluation, we determined that 6 guidelines were of suitable quality and content for adaptation, of which 3 guidelines provided references appropriate for assessments (Table 1). Recommendations from each guideline were extracted and divided based on content and reviewed by the relevant working group. The community treatment group also identified 2 recommendations from the Institute of Health Economics. 24 The Consensus Development Conference has a unique format based on a jury trial, which provides an independent and critical review of issues by an unbiased panel. The conference is a survey of the best available evidence, which informs a consensus statement that is relevant for policy and practice. The conference involves 20 to 25 experts who deliver scientific evidence addressing 5 to 8 questions in a given field over 2 days of hearings, which are attended by a jury or panel of about 12 members and an audience of delegates.
Clinical practice guidelines used for the Canadian Schizophrenia Guidelines.
Following the ADAPTE process, working groups selected guidelines and recommendations to create an adapted guideline. Each working group carefully examined each recommendation, the evidence from which the recommendation was derived, and the acceptability and applicability of the recommendation to the Canadian context. After reviewing the recommendations from the guidelines, the working groups decided which recommendations to accept and which to reject and which recommendations were acceptable but needed to be modified. Care was taken when modifying existing recommendations not to change the recommendations to such an extent that they were no longer in keeping with the evidence upon which they were based.
Each working group developed a final list of recommendations from the included guidelines that were presented to the entire guideline panel at an in-person consensus meeting. Working group leaders presented each recommendation and its rationale to the panel. Anonymous voting by the entire panel using clicker technology was performed for each recommendation. Recommendations required agreement by 80% of the group to be included in the Canadian guidelines. If a recommendation did not receive 80% agreement, the group discussed the recommendation and whether minor modifications to the recommendation would alter the likelihood that the recommendation would pass. In these situations, recommendations were modified (as described above), and the group revoted later using an online anonymous survey. Whenever modifications in wording were made to original recommendations, the text “modified recommendation from” appears in the Canadian Schizophrenia Guidelines, and the source of each recommendation is written beside the recommendation statement. The strength or grade of the recommendation is provided in brackets, if applicable, using the system that the recommendation came from. The grades of recommendation for each reference guideline and their meaning are explained in brief in Table 2 (see the Introduction and Methodology paper for a more detailed description). Once the voting and consensus process was completed, each working group created a separate paper that contained all the recommendations adapted from the included guidelines, with accompanying text explaining the rationale for each recommendation.
Grade/strength of recommendation classification systems for included guidelines.a
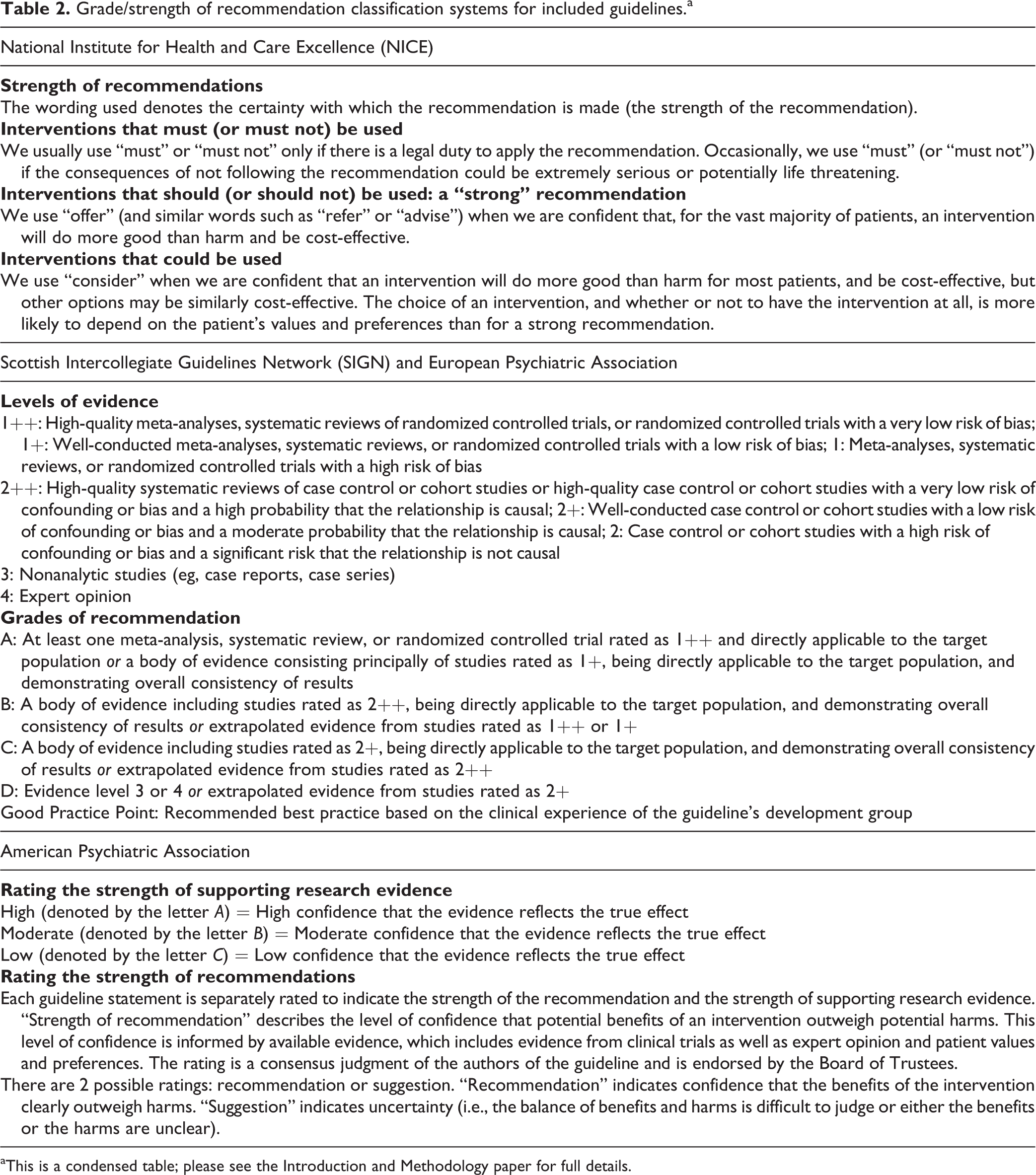
aThis is a condensed table; please see the Introduction and Methodology paper for full details.
During the finalization phase, the Canadian Schizophrenia Guidelines were externally reviewed by those who will be affected by their uptake: practitioners, policy makers, health administrators, patients, and their families. The external review asked questions about whether the users approve of the draft guideline, strengths and weaknesses, and suggested modifications. The process was facilitated through the Canadian Journal of Psychiatry and the Schizophrenia Society of Canada. The CPA Clinical Practice Guidelines Committee reviewed and approved the guideline methodology process.
Results
Recommendation 1: Assessment and Care Planning
An initial comprehensive multidisciplinary assessment (including an evaluation by a psychiatrist) comprised the following:
A full mental status examination with particular attention to symptoms of psychosis, negative symptoms, general psychopathology, insight, and competence. Risk of suicide and aggression. A psychiatric history including prior diagnoses and treatments, prior hospitalizations, and emergency room treatments. For patients with previous episodes of illness, review and document the treatments provided (types, duration, and doses), adherence, and responses to treatment. In the absence of quantitative measures, note the outcomes of previous treatments and whether positive symptoms were nonresponsive, symptoms were ameliorated but still present, or no symptoms of psychosis were observed. A history of substance use including tobacco, alcohol, marijuana, hallucinogens, stimulants, opioids, and other drugs. A history of psychosocial development and neurodevelopmental problems. Current occupational or educational functioning, social network size and satisfaction, sexual functioning, housing, and financial status. A history of health problems and an assessment of current health status including access to primary care (see the section on physical health). Where possible, include information from family or partners and health records. [APA practice guidelines for the psychiatric evaluation of adults (level of evidence: C)]
Assessments are undertaken for several reasons, and the focus of the assessment varies accordingly. Recommendation 1 is focused on the initial assessment when making a diagnosis is an objective or on the periodic comprehensive review when treatment plans are reviewed. The assessment offers the opportunity to engage the patient and caregivers by attending to their concerns, providing information, and reviewing options. When the focus is on examining risk during the initial assessment, factors such as past depression, suicide attempts, and harm to others need to be included. In an emergency, an assessment of risk for suicide and aggression is more often the focus of attention. Finally, an assessment of physical health is an essential part of the initial and periodic assessment; it is covered in the section on the assessment of physical health.
Recommendation 2: Assessment of the First Episode of Psychosis
Accessibility and timelines are important aspects of the assessment of the first episode of psychosis. See new patients within 2 weeks of referral.
An assessment for the first episode of psychosis includes recommendation 1 (assessment and care planning) as well as a family history of psychiatric disorders.
Pay particular attention to the longitudinal assessment of the onset of changes in behaviour and in the timing and course of the onset of the first symptoms of psychosis.
The relationship of substance use to the onset of psychotic symptoms, specifically the duration, quantity, and timing of substance use.
The developmental history, including social and academic functioning in childhood and adolescence, may help indicate the onset of decline in function and can be of prognostic value for the degree of symptomatic and functional recovery.
The duration of untreated psychosis, which represents the time from the onset of psychotic symptoms to the time of the first effective treatment, has prognostic value.
Include family members or other carers as part of the initial assessment whenever possible, with the consent of the competent patient. [De novo recommendation (Good Practice Point)]
Easy and timely access to appropriate assessments and care are important in the first episode of psychosis to reduce the duration of untreated psychosis and minimize the complications of the first episode of psychosis. The duration of untreated psychosis is a significant predictor of outcomes. 25,26 It is reduced when there is timely access to treatment services for the first episode of psychosis. 27 In Canada, the CPA has set 2 weeks as an appropriate standard wait time for a scheduled nonurgent first-episode psychosis referral. 28 The same time period has been adopted in the UK as a national quality standard. 29
While the information gathered during the initial assessment is essential for making a diagnosis and recommending a treatment plan, it is an important opportunity to engage the patient, the family, or other carers and establish a collaborative relationship and shared decision making.
Recommendation 3: Neuropsychological Assessment
Neuropsychological testing is suggested in patients with a first episode of psychosis and in those with poor responses to treatment. It may be important for documenting cognitive deficits and for treatment and academic planning. [De novo recommendation (Good Practice Point)]
Neurocognitive testing is a robust predictor of overall levels of functioning and may be a target for interventions. 30 It is mentioned in the text of the practice parameter for the assessment and treatment of children and adolescents with schizophrenia as part of a broad recommendation to evaluate other pertinent clinical conditions, although not as a formal recommendation of its own, with levels of evidence. 15 The MATRICS consensus cognitive battery is a standardized set of cognitive measures that is approved by the US Food and Drug Administration and National Institute of Mental Health. 31 It can be undertaken by any appropriately trained mental health professional. The interpretation of neurocognitive test results is optimally carried out by a neuropsychologist.
Recommendation 4: Brain Imaging
Order neuroimaging with computed tomography or magnetic resonance imaging based on specific aspects of the history, neurological examination, or neuropsychological testing results. Consider on a case-by-case basis at the time of the first episode of psychosis. [De novo recommendation (Good Practice Point)]
This recommendation is a modification of some earlier clinical practice guideline recommendations that brain imaging be considered as part of a routine investigation of all patients with a first episode of psychosis. Multiple studies and systematic reviews have found that routine neuroimaging in the first episode of psychosis cannot be justified because findings do not alter clinical management in a meaningful way. 32 The risks of radiation exposure and delay in treatment also argue against routine neuroimaging. Imaging is indicated in the presence of signs and symptoms suggestive of intracranial pathology including headaches, nausea and vomiting, seizure-like activity, and later age at the onset of symptoms. Clinical features in patients with psychiatric symptoms suggestive of autoimmune encephalitis are an indication for magnetic resonance imaging and a more extensive evaluation and include rapid progression of working memory deficits over less than 3 months, new focal central nervous system findings, or seizures not explained by a previously known seizure disorder. 33
Recommendation 5: Genetic Testing
Consider genetic testing based on the history and physical examination of the patient, especially at the time of the first episode of psychosis. Although they lack diagnostic specificity, certain copy number variations (CNVs; especially chromosome 22q11) are more prevalent in individuals with schizophrenia. The identification of these CNVs in patients with schizophrenia may help diagnose rare conditions that have important medical and psychiatric implications for individuals and may inform psychiatric genetic counseling. The identification of de novo CNVs may also have a place in counseling. [De novo recommendation (Good Practice Point)]
Individuals with schizophrenia have an increased genome-wide burden of CNVs. 34 This recommendation is based on a work published by the ISPG in 2014. 16 The best-known example is the 22q11.2 deletion, which is a CNV on the long arm of chromosome 22. It is responsible for a physical phenotype that affects multiple organ systems and commonly cognitive development. A high proportion, up to 25%, of adults with the deletion have schizophrenia. 35 A review of the 22q11.2 deletion in schizophrenia estimated a prevalence of 1% to 2%. 36 The clinical features of schizophrenia in patients with the 22q11.2 deletion resemble those in patients without the deletion. 37,38 The syndrome can be recognized by clinical features including hypernasal speech; characteristic facial features such as a long and narrow face, narrow palpebral fissures, flat cheeks, a prominent nose, small ears, a small mouth, and retruded chin; learning difficulties; and heart defects. 39
Recommendation 6: Ongoing Assessment of Positive and Negative Symptoms
Assess positive and negative symptoms at least every 3 months in the stable patient.
Note the presence or absence of positive symptoms. When present, rate the severity of key positive symptoms (hallucinations, conceptual disorganization, delusions and/or unusual thought content, and suspiciousness) using a quantitative measure.
Following a change in treatment, reassess the severity of key positive symptoms for the amount of change at regular intervals. An assessment of the level of positive symptoms and treatment responses is especially important for selecting and monitoring patients for the second-line antipsychotic clozapine.
Note the presence or absence of negative symptoms. When present, rate the severity of key negative symptoms (blunted affect, emotional withdrawal, poor rapport, passive social withdrawal, and lack of spontaneity) using a quantitative measure.
When making a differential diagnosis, distinguish negative symptoms that are intrinsic to schizophrenia from negative symptoms related to depression, drug side effects or interactions, substance use, anxiety, cognitive impairment, or neurological disorders. [De novo recommendation (Good Practice Point)]
This recommendation combines elements from more general recommendations in the APA practice guidelines for the psychiatric evaluation of adults 13 with more specific recommendations in the schizophrenia literature. Although there is a developing research literature on the benefit of measurement-based care in the treatment of depression, 4 there is little specific evidence for schizophrenia care. 40,41 The DSM-5 provides several assessment measures and emphasizes the need for clinician-rated assessments of the dimensions of psychosis severity. It provides an 8-item scale, which includes positive, negative, and depressive symptoms. This measure has been shown to have good interrater reliability. 42 Several scales designed to assess these symptoms have psychometric properties and have been widely used in research. These include the Positive and Negative Syndrome Scale 43 and the Brief Psychiatric Rating Scale. 44 Depressive symptoms occur at all stages of schizophrenia, but their assessment can be challenging due to the overlap with negative symptoms. The Calgary Depression Scale for Schizophrenia is a reliable and valid measure, which has been developed to assess depression in schizophrenia independent of negative symptoms. 45 The presence of negative symptoms has been recognized since the earliest descriptions of schizophrenia, and the variety of ways of classifying negative symptoms has been reviewed. 4 A challenge in the use of rating scales in schizophrenia is the requirement for training to utilize scales reliably. 46,47
Recommendation 7: Ongoing Assessment of Suicide Risk
An assessment of suicide risk is an essential part of the initial assessment, and active reassessments should be performed for those known to be at risk or those who respond to routine periodic screening questions about depression and suicidal thinking. The assessment includes the following:
Current suicidal ideas, suicide plans, and suicide intent, including active or passive thoughts of suicide or death. Delusions and hallucinations with content related to suicide or with a risk of harm if acted upon. Hopelessness. Impulsivity. Access to suicide methods, including firearms. Reasons for living (e.g., sense of responsibility to family, children, or others; religious beliefs). [De novo recommendation (Good Practice Point)]
The lifetime risk for suicide among people with schizophrenia is about 5%. 48 A systematic review found that robust risk factors for suicide in schizophrenia included previous depressive disorders, previous suicide attempts, drug misuse, agitation or motor restlessness, fear of mental disintegration, poor adherence to treatment, and recent loss. 49 Although the review found no association with hallucinations in general, attention to the specifics of psychotic experiences, particularly the content of delusions and hallucinations, is reinforced by a study that found that command hallucinations carried a higher risk of suicide. 50 The Suicide Risk Assessment Guide provides a thorough and practical introduction to a general assessment of suicide risk. 51 The Columbia Suicide Severity Rating Scale is a reliable and valid assessment tool that has been used in research and clinical settings. 52 There is a website that offers online training in the use of the scale (http://cssrs.columbia.edu/training_cssrs.html).
Recommendation 8: Ongoing Assessment of Risk of Aggression
An assessment of the risk of aggression is an important part of the initial assessment, especially in those known to be at risk or those who respond to routine periodic screening questions about aggression. A more detailed assessment includes the following:
Current aggressive or psychotic ideas, including thoughts of physical or sexual aggression or homicide. Impulsivity, including anger management issues. Access to firearms or other weapons. Specific individuals or groups toward whom homicidal or aggressive ideas or behaviours have been directed in the past or at present. [De novo recommendation (Good Practice Point)]
This recommendation combines 2 statements from the APA practice guidelines (guideline IV, statements 2 and 3). 1 There are increased rates of violent crime, suicide, and premature mortality over the life span associated with schizophrenia. 53 A systematic review and meta-analysis concluded that although schizophrenia and other psychoses are associated with violence and violent offending, particularly homicide, most of the excessive risk appears to be associated with substance abuse comorbidity. 54 Antipsychotic drug treatment substantially decreases the risk of violence and crime in patients with schizophrenia. 55 Rates of violence at onset appear to be more common in less developed countries. 56 Clinical features associated with violence include psychotic symptoms, such as persecutory ideation. 57 In the first episode of people with schizophrenia, violence in the week following presentation was associated with drug misuse and high psychopathology scores. Overall, despite a high rate of verbal aggression, physical violence toward other people is uncommon in individuals presenting with a first episode of psychosis. 58
Recommendation 9: Ongoing Assessment of Substance Use
A regular assessment of substance use (including, but not limited to, tobacco and alcohol) includes the following:
Particular substance(s) used. Quantity, frequency, and pattern of use. Duration of current level of use. Impact on medication adherence. Route of administration. Level of dependence. Readiness to change. Urine toxicology need not be carried out routinely but can be used in acute situations where clinically indicated and otherwise where agreed upon with the patient as part of treatment planning. [NICE (Strong)]
An assessment of substance use in schizophrenia is important because the prevalence of substance use disorders is high and its impact is significant. 59,60 The Canadian Schizophrenia Guidelines recommend in the section on service organization that the treatment of psychosis and substance use disorders be integrated and recommend specific interventions for the treatment of substance use disorders. The section on physical health highlights the importance of cigarette smoking on health. When all patients are routinely screened for substance use, the results can be incorporated into a treatment plan. Several screening tools that also quantify use and lead to interventions are available. The DSM-5 recommends the use of the NIDA-Modified ASSIST. 61 Biological screening can supplement interview screening and can be used to confirm the substances used and support treatment planning.
Recommendation 10: Involvement of the Patient in Treatment Decision Making
During the initial psychiatric evaluation of a patient, include an explanation to the patient of the following: the differential diagnosis and a discussion of the risks of untreated illness, treatment options, and benefits and risks of treatment.
Shared decision making requires that both parties are actively involved in the decision-making process and includes asking the patient about treatment-related preferences.
During ongoing treatment, include a discussion of the risks of untreated illness, treatment options, benefits and risks of treatment, and relapse prevention. [De novo recommendation (Good Practice Point)]
This recommendation to involve the patient in treatment decision making as part of the assessment process embeds shared decision making into the treatment process from the start. An early definition of shared decision making suggested that at least 2 participants need to be involved, both parties need to share information, both parties need to build a consensus about the preferred treatment, and agreement needs to be reached. 62 A more recent review has developed an integrative model based on a systematic review. The authors identified 20 categories that included patient values/preferences and the patient’s ability/self-efficacy to follow through on the recommendations. 63 There has been little research on the outcome of shared decision-making interventions for people with mental disorders, so no conclusions about outcomes can be drawn. 64 However, shared decision making supports a recovery approach. 65
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.