
Abstract
Objective:
Young people who are at clinical high risk (CHR) of developing psychosis are often help seeking and have significant distress and dysfunction. There are limited guidelines for the assessment and treatment for this population. The aim of this guideline was to develop treatment recommendations for this at-risk group.
Method:
A systematic search was conducted for published guidelines for CHR. All current guidelines for schizophrenia were reviewed for treatment guidelines on individuals at CHR. The recommendations adopted were primarily drawn from the European Psychiatric Association (EPA) guidance on the early intervention in clinical high-risk states of psychoses and the 2014 National Institute for Health and Care Excellence (NICE) guidelines on the treatment and management of those at CHR for psychosis.
Results:
After the guideline development process described, 9 recommendations were developed based on the quality of evidence, appropriateness for the Canadian health care system, and clinical expert consensus.
Conclusions:
Assessment by an expert in the field was the first recommendation. It was recommended that treatment follow a staged approach with psychological treatments being the first-line treatment and pharmacotherapy reserved for adults, those who did not respond to psychological interventions, and those who had more severe symptoms.
Detection and intervention very early in the course of psychotic illness was a major research goal for realising substantive improvements in the outcome of schizophrenia spectrum disorders. This focus has led to more than 2 decades of work studying young people who may be at risk of developing a psychotic illness and exploring the possibility of intervention before the onset of the full disorder, in the hope that preemptive efforts may produce improved outcomes. The research has focused on 3 areas: identifying criteria for defining those at clinical high risk, strategies for identifying those at clinical high risk, and interventions for those at clinical high risk.
The prepsychotic or ‘prodromal’ stage of illness is defined as the period marked by changes from a person’s premorbid mental state and level of functioning up to the appearance of psychotic features. 1 Our conceptual understanding of the clinical high-risk state has arisen first from the long-established observation that 80% to 90% of individuals with schizophrenia retrospectively report a prodromal period characterised by increasing problems in thinking, feeling, and behaving. Second, it has arisen from the epidemiological evidence of a continuum of psychotic symptoms in the general population. 2 However, it is less clear how many individuals who display ‘prodromal symptoms’ will subsequently develop a psychotic illness. Thus, a precondition for early intervention is the accurate detection of prodromal states (i.e., knowing who may be at true risk of developing a psychotic illness). Over the past decade, there have been major advances in research in Australia, North America, and Europe to develop and test operational criteria for prospectively assessing psychosis liability over time. These efforts suggest that it is possible to reliably identify an ‘at-risk mental state’ in which individuals have an elevated risk (e.g., 25%-35%) of developing a diagnosable psychotic illness over several years. 3 Several reviews and meta-analyses have been published focusing on the development of the field, 4 clinical studies, 5 treatment outcome, 6 and conversion to psychosis. 3
Clear criteria have been established for identifying those at risk for developing a psychosis. 7,8 These criteria identify 3 syndromal subgroups. The first is the attenuated positive symptom syndrome (APSS), which includes the emergence or worsening of non-psychotic-level disturbances in thought content, thought processes, or perceptual abnormalities in the past year. This is by far the most common syndrome observed. 9 The second is the brief intermittent psychotic symptom syndrome (BIPS), which requires the presence of any 1 or more threshold positive psychotic symptoms (unusual thought content, suspiciousness, grandiosity, perceptual abnormalities, and disorganised communication) that are too brief to meet diagnostic criteria for psychosis. Finally, the third criterion is genetic risk and deterioration (GRD), which requires having a combination of both functional decline and genetic risk (i.e., either schizotypal personality disorder or a first-degree relative with a schizophrenia spectrum disorder). 7 Since prodromal is a retrospective concept—that is, an individual needs to develop an illness to have experienced a prodromal period—and since the criteria are clinically based, these individuals are considered to be at clinical high risk (CHR) for psychosis.
The 2 most widely used measures to determine the CHR criteria are the Comprehensive Assessment of At-Risk Mental States (CAARMS) 8 and the Structured Interview of Prodromal Syndromes (SIPS), 7 which is the most commonly used measure in North America. The goal of the SIPS interview, as well as the associated Criteria of Prodromal Syndromes (COPS), is to identify operationally the presence of an at-risk state for psychosis, to measure symptom severity over time, and to evaluate conversion to actual psychosis.
Young people who meet these CHR criteria are generally help-seeking adolescents or young adults, 13 to 30 years old. Since much of the current knowledge on individuals at CHR is a result of research, these young people are considered help seeking because they or their families have made some effort to seek help for their concerns. This contrasts with studies where screening methods for meeting CHR criteria are conducted in large population samples. These young people often present with a multitude of concerns in addition to complaints of attenuated positive psychotic symptoms. Many have comorbid diagnoses, in particular anxiety and depression that can be clinically debilitating. 10,11 High levels of negative symptoms, significant impairments in academic performance and occupational functioning, and difficulties with interpersonal relationships are often observed. 12,13 It is often the case that these problems have been present for some time but recently worsened, triggering concern in family members or friends who have recommended professional evaluation. There is also evidence of cognitive impairment, the severity of which lies between that of those with a first episode of psychosis and healthy controls. 14,15 It should be noted that youth who are help seeking or referred from other clinicians are more likely to be at risk of developing psychosis than those who may have been identified through screening. 16
Methods
The methods for the Canadian Schizophrenia Guidelines are described in brief here; please see the Introduction and Methodology manuscript for an in-depth description. 17 The guidelines were developed using the ADAPTE process. 18 Recognising that the development of guidelines requires substantial resources, the ADAPTE process was created to take advantage of existing guidelines and reduce duplication of effort.
The first phase of the ADAPTE process, the setup phase, involved preparing for the ADAPTE process. We assembled a national multidisciplinary panel from across Canada, including stakeholders with expertise in schizophrenia and mental health, health policy, patient advocacy, and lived experience with schizophrenia. Endorsement bodies for the guidelines include the Canadian Psychiatric Association and the Schizophrenia Society of Canada, who were also heavily involved in the dissemination and implementation strategy.
The second phase of the ADAPTE process, the adaptation phase, involves the process of identifying specific health questions; searching for and retrieving guidelines; assessing guideline quality, currency, content, consistency, and applicability; decision making around adaptation; and preparing the draft adapted guideline. We searched for guidelines on schizophrenia in guideline clearinghouses and on the websites of well-established guideline developers for mental health disorders, including the National Institute for Health and Care Excellence (NICE), the Scottish Intercollegiate Guidelines Network (SIGN), the American Psychiatric Association, the American Academy of Child and Adolescent Psychiatry, and the European Psychiatric Association. A MEDLINE search was also performed using the term guideline as the publication type and schizophrenia as the title or clinical topic. Inclusion criteria were that the guideline needed to be published after 2010, be written in English, and that recommendations had to be developed using a defined and systematic process. We identified 8 current guidelines that were potentially suitable for adaptation. These guidelines were reviewed and evaluated in duplicate using the AGREE II tool, 19 an instrument to evaluate the methodological rigor and transparency in which a guideline is developed. Based on this evaluation, we determined that 2 guidelines were of suitable quality and content for adaptation (see Table 1).
Clinical Practice Guidelines Used for the Canadian Schizophrenia Guidelines.
Recommendations from each guideline were extracted and divided based on content and reviewed by the relevant working group. Following the ADAPTE process, working groups selected between guidelines and recommendations to create an adapted guideline. Each working group carefully examined each recommendation, the evidence from which the recommendation was derived, and the acceptability and applicability of the recommendation to the Canadian context. After reviewing the recommendations from the guidelines, the working groups decided which recommendations to accept and which to reject, as well as which recommendations were acceptable but needed to be modified. Care was taken when modifying existing recommendations not to change the recommendations to such an extent that they were no longer in keeping with the evidence upon which they were based. Please see the Appendix for how and why the first recommendation in this article was modified from its original form.
Each working group developed a final list of recommendations from the included guidelines that were presented to the entire guideline panel at an in-person consensus meeting. Working group leaders presented each recommendation and its rationale to the panel. Anonymous voting by the entire panel using clicker technology was performed for each recommendation. Recommendations required agreement by 80% of the group to be included in the Canadian guidelines. If a recommendation did not receive 80% agreement, the group discussed the recommendation and if minor modifications to the recommendation would alter the likelihood that the recommendation would pass. In these situations, recommendations were modified (as described above), and the group revoted at a later date using an online anonymous survey. Whenever modifications in wording were made to original recommendations, the text ‘modified recommendation from’ appears in the Canadian Schizophrenia Guidelines, and the source of each recommendation is written beside the recommendation statement.
The strength or grade of the recommendation is provided in brackets if applicable, using the system from which the recommendation came. The grades of recommendation for each reference guideline and their meaning are explained in brief in Table 2 (see Introduction and Methodology manuscript for a more detailed description). 17 Once the voting and consensus process was completed, each working group created a separate manuscript that contains all the recommendations adapted from the included guidelines, with accompanying text explaining the rationale for each recommendation.
Grade/strength of recommendation classification systems for included guidelines.a
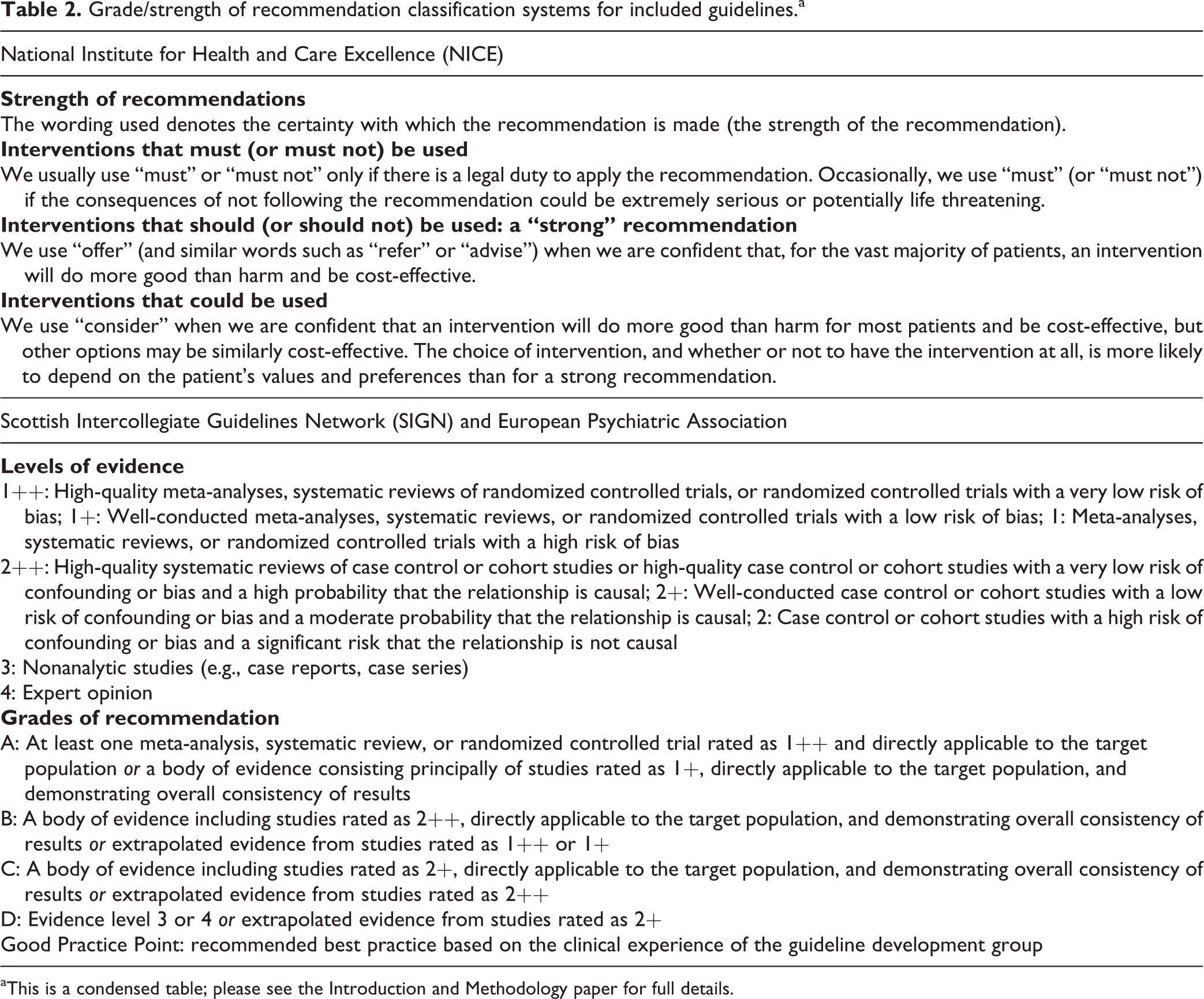
aThis is a condensed table; please see the Introduction and Methodology paper for full details.
During the finalisation phase, the Canadian Schizophrenia Guidelines were externally reviewed by those who will be affected by its uptake: practitioners, policy makers, health administrators, patients, and their families. The external review asked questions about whether the users approve of the draft guideline, strengths and weaknesses, and suggested modifications. The process was facilitated through the Canadian Journal of Psychiatry and the Schizophrenia Society of Canada. The Canadian Psychiatric Association Clinical Practice Guidelines Committee reviewed and approved the guideline methodology process.
Recommendations
In developing our recommendations, the working group has primarily drawn upon the European Psychiatric Association (EPA) guidance on the early intervention in clinical high-risk states of psychoses 20 and the 2014 NICE guidelines on the treatment and management of those at clinical high risk for psychosis. 21
Clinical high-risk criteria (i.e., the APSS criterion, the BIPS criterion, or the genetic risk and functional decline syndrome) can be assessed with either the SIPS 7 or the CAARMS. 8
With reference to each of the recommendations, where relevant, we provide a brief synopsis of the state of the current evidence for effectiveness.
Recommendation 1
If a person is distressed and may have a decline in social functioning and has
transient or attenuated psychotic symptoms or other experiences or behaviour suggestive of possible psychosis or schizophrenia or a first-degree relative with psychosis or schizophrenia or schizotypy
refer him or her for a comprehensive assessment without delay to a specialist mental health service or an early intervention in psychosis service because this person may be at risk of developing psychosis.
[Modified from NICE (Strong)]
Recommendation 2
A consultant psychiatrist or trained specialist with experience in at-risk mental states should carry out the assessment.
[NICE (Strong)]
In practice, it would be reasonable for the specialist assessment to include both an assessment of the clinical high-risk state using a measure such as the CAARMS 8 or the SIPS 7 and to identify the comorbid problems that may need to be treated. About 73% of those identified as showing a clinical high-risk state also had a comorbid axis I diagnosis. Depression was the most common. 10 There is now an individualised risk calculator that can improve prediction in the situation that the individuals at clinical high risk are help seeking and have been diagnosed using the Structured Clinical Interview for Prodromal State. 22
Recommendation 3
Offer individual cognitive-behavioural therapy (CBT) with or without family intervention.
[NICE (Strong, grade low to moderate)]
EPA guidance 20 reviewed psychological interventions with CHR participants. Of the 9 studies published to date, the majority used CBT. Only 1 family randomised controlled trial (RCT) has been published to date. 23
Recommendation 4
Offer interventions recommended in NICE guidelines for the presenting problem, that is, current individual needs (anxiety, depression, emerging personality problems, or substance misuse).
[NICE (Strong)]
Comorbid disorders, including depression at 40%, anxiety, and substance use, are common in those at CHR. 10,24 These conditions should be treated with the standard treatments for those disorders. The presence of a comorbid condition, including substance use disorder, does not appear to increase the risk of transition to psychosis, 25 but treatment can relieve distress and improve functioning.
Recommendation 5
Offer interventions to prevent the development or persistence of functional deficits (social, educational, or vocational).
[EPA (Grade D)]
Functional impairments, defined by the presence of a decline in functioning and/or the presence of cognitive impairment, have been observed to be present before and often worsen until the onset of psychosis. There is also evidence that functional deficits predict conversion to psychosis. 12 These findings support the careful assessment of functioning and the use of psychosocial interventions such as social skills training that address the specific problems of the individual.
Recommendation 6
Psychological interventions, in particular CBT, as well as pharmacological interventions are able to prevent or at least postpone a first psychotic episode in adult CHR patients.
[EPA (Grade A)]
The EPA guidance combined the results of 7 RCTs that investigated psychological and/or pharmacological interventions and included 916 participants. Results were that at 6 months, the experimental conditions significantly reduced the risk for conversion of first-episode psychosis by 64% compared to the control condition. At 12-month follow-up, the experimental condition reduced the risk of conversion by 56%. 26
Recommendation 7
These treatments should be monitored by a psychiatrist, a clinical psychologist, or an equivalent mental health professional.
[EPA (Grade D)]
The research studies that demonstrate effectiveness of interventions for the clinical high-risk state have used evidence-based treatments delivered with high fidelity.
Recommendation 8
In adult CHR patients, a staged intervention model should be applied with the least restrictive treatment approach (i.e., CBT) being offered as a first choice. Where psychological interventions have proved ineffective, and there are severe and progressive attenuated psychotic symptoms, they should be complemented by low-dose second-generation antipsychotics in adult CHR patients. Here the primary aim is to achieve a degree of symptomatic stabilisation. Any long-term antipsychotic treatment with a primarily preventive purpose is not recommended.
[EPA (Grade D)]
Staged intervention models have been advocated for interventions in the earlier and milder forms of specific mental disorders. 27,28 Staging involves selecting treatments that may be simpler or less intrusive for the earlier stages of the disorder. For example, in those at clinical high risk who do not yet meet criteria for a psychotic illness, psychological interventions should be considered as first-line treatments and pharmacological interventions reserved for those who symptoms do not respond or are escalating.
Recommendation 9
If, after treatment, the person continues to have symptoms, impaired functioning, or is distressed but a clear diagnosis of psychosis cannot be made, monitor the person regularly for changes in symptoms and functioning for up to 3 years using structured and validated assessment tools. Determine the frequency and duration of monitoring by 1) the severity and frequency of symptoms, 2) the level of impairment and/or distress, and 3) the degree of family disruptions or concern.
If a person asks to be discharged from the service, offer follow-up appointments and the option to self-refer in the future. Ask the person’s family physician to continue monitoring changes in his or her mental state.
[NICE (Strong)]
Some patients may not agree to any treatments, particularly when symptoms are mild, not distressing, or when there is a lack of insight. A 2.5-year longitudinal follow-up study found that (71%) participants had not made the transition to psychosis. For that group, there was significant improvement in ratings for attenuated positive and negative symptoms over the first year, but at least 1 attenuated positive symptom was still present for 43% of the sample at 1 year and for 41% at 2 years. At the follow-up time points, social and role functioning were significantly poorer in the clinical sample relative to nonpsychiatric comparison subjects. 29
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.