
Abstract
Clozapine is the most effective antipsychotic for the 25% to 33% of people with schizophrenia who are treatment resistant, but not all people achieve response. Using data from a previously published clozapine systematic review and meta-analysis, we explored the proportion of people who achieved response and examined the absolute and percentage change in Positive and Negative Syndrome Scale (PANSS) scores. Overall, 40.1% (95% confidence interval [CI], 36.8%-43.4%) responded, with a mean reduction in PANSS of 22.0 points (95% CI, 20.9-23.1), a reduction of 25.8% (95% CI, 24.7%-26.9%) from baseline. These reductions are clinically meaningful. A 40% response rate to clozapine suggests that 12% to 20% of people with schizophrenia will be ultra-resistant.
Treatment-resistant schizophrenia (TRS) is defined as ongoing symptoms and functional impairment despite 2 adequate trials of different antipsychotics with appropriate adherence monitoring. 1 Approximately 20% to 33% of people with schizophrenia have TRS. 2,3
Among people with TRS, clozapine is the most effective medication for positive symptoms. 4 However, there is a lack of clarity about both response rates and the degree of improvement that may be expected. We therefore measured response rates to clozapine, as well as the absolute and percentage improvement in psychotic symptoms among people with TRS using data from a recently published systematic review and meta-analysis. 4
Methods
We used data from a published meta-analysis by our group. 4 Search strategies were outlined previously. Briefly, we searched PubMed, Embase, and the Cochrane Trials Register for randomised controlled trials of clozapine compared to other antipsychotics for TRS.
Data from studies were divided into all time points (with the last end point used), short term (last end point less than 3 months from baseline), and long-term (last end point greater than 3 months from baseline). Our outcomes were the proportion achieving response, as well as absolute and percentage changes in psychotic symptoms measured by the Positive and Negative Syndrome Scale (PANSS) or the Brief Psychiatric Rating Scale (BPRS). Equipercentile linkage tables were used to convert BPRS to PANSS for absolute change and percentage change scores 5 to allow comparison between studies.
For the analysis of response rates, we used an arcsine (inverse sine) transformation for binomial variables to give a weighted estimate of mean response rate and standard deviations (SDs). 6
For the analyses of absolute and percentage changes in score, weighting was calculated using the inverse of the square of standard errors. 7 Although means were available for all time points, standard deviations of absolute differences were missing in 8 studies, as were standard deviations of the baseline measure in 2 studies and of the end-point value in 7 instances. We therefore imputed missing standard deviations based on the relationship between baseline (Vb) and end-point variances (Ve) and the variance of the absolute change (Vc). We used the following equation: Vc = Vb + Ve – 2ρSbSe, where ρ is the correlation between baseline and end-point values, and Sb is the baseline standard deviation and Se the end-point standard deviation.
In 7 instances, all 3 standard deviations were available, which allowed the calculation of ρ. Apart from 2 instances, all values were between 0.73 and 0.83, with a median of 0.75. In all studies, at least 2 standard deviations were available. All missing standard deviations were imputed assigning a common value to ρ. For the main analysis, the observed median value of 0.75 was used, but sensitivity analyses with values of 0.7 and 0.8 were also performed.
In terms of the percentage change, no standard deviations were available, although in 2 instances, 8,9 the raw data were provided, thereby enabling direct calculation. In other instances, percentage change could be computed using the following asymptotic formula for the variance of the ratio of 2 random end-point and baseline variables, x and y, respectively: V[(y – x)/y)] = V(x/y) = (x/y) 2 × (Vx/x 2 + Vy/y 2 – 2ρSxSy/xy). 10 No additional imputation was needed, as all quantities in this formula were already available from the analysis of absolute change.
A sensitivity analysis was conducted based on whether studies had strict TRS criteria rather than treatment intolerance as an inclusion criterion. We also examined the effect of differences in response criteria on outcome.
Results
We used data from a published meta-analysis by our group 4 (PROSPERO registration number: CRD42014013134). PROSPERO was amended prior to this analysis. Details on the study selection and PRISMA checklist have been published previously. 4 Briefly, 2589 studies were identified in the initial database search, with 2402 excluded at title and abstract, a further 167 excluded at full text, and 1 additional study included from a hand search of key articles. Characteristics of the 21 studies included in this subanalysis are provided in Table 1. Six studies used the Kane et al. 11 TRS inclusion criteria of 2 or more adequate trials of previous antipsychotics with ongoing psychotic symptoms, but none met the recently published TRS criteria, which also include monitoring adherence of previous antipsychotic trials and ongoing functional impairment. 1 For the purpose of this analysis, we have used the Kane et al. 11 TRS criteria.
Included Studies.a
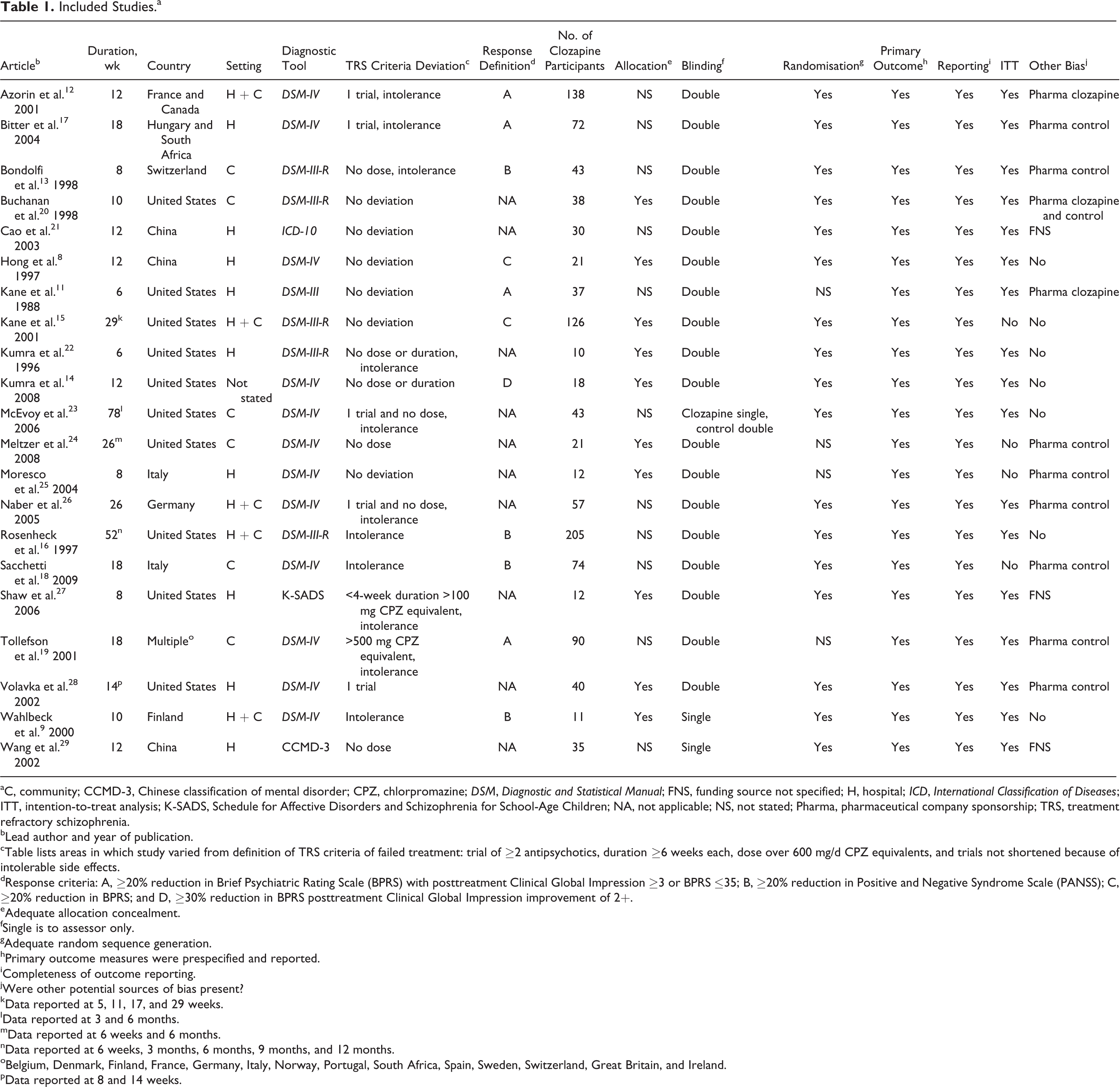
aC, community; CCMD-3, Chinese classification of mental disorder; CPZ, chlorpromazine; DSM, Diagnostic and Statistical Manual; FNS, funding source not specified; H, hospital; ICD, International Classification of Diseases; ITT, intention-to-treat analysis; K-SADS, Schedule for Affective Disorders and Schizophrenia for School-Age Children; NA, not applicable; NS, not stated; Pharma, pharmaceutical company sponsorship; TRS, treatment refractory schizophrenia.
bLead author and year of publication.
cTable lists areas in which study varied from definition of TRS criteria of failed treatment: trial of ≥2 antipsychotics, duration ≥6 weeks each, dose over 600 mg/d CPZ equivalents, and trials not shortened because of intolerable side effects.
dResponse criteria: A, ≥20% reduction in Brief Psychiatric Rating Scale (BPRS) with posttreatment Clinical Global Impression ≥3 or BPRS ≤35; B, ≥20% reduction in Positive and Negative Syndrome Scale (PANSS); C, ≥20% reduction in BPRS; and D, ≥30% reduction in BPRS posttreatment Clinical Global Impression improvement of 2+.
eAdequate allocation concealment.
fSingle is to assessor only.
gAdequate random sequence generation.
hPrimary outcome measures were prespecified and reported.
iCompleteness of outcome reporting.
jWere other potential sources of bias present?
kData reported at 5, 11, 17, and 29 weeks.
lData reported at 3 and 6 months.
mData reported at 6 weeks and 6 months.
nData reported at 6 weeks, 3 months, 6 months, 9 months, and 12 months.
oBelgium, Denmark, Finland, France, Germany, Italy, Norway, Portugal, South Africa, Spain, Sweden, Switzerland, Great Britain, and Ireland.
pData reported at 8 and 14 weeks.
Eleven studies provided data on response rates, 8 short term, 8,9,11 –16 and 5 long term 15 –19 (2 had data for both time points 15,16 ). Twenty studies had usable data on change in total psychotic symptoms, 8,9,11 –15,17 –29 with 16 providing short-term data 8,9,11 –15,20 –25,27 –29 and 8 with long-term data 15,17 –19,23,24,26,28 (4 had data for both time points 15,23,24,28 ).
The mean response rate in the short term was 32.8% (95% confidence interval [CI], 29.1%-36.6%; homogeneity χ2 = 15.4; df = 7; P < 0.001; I2 = 54.7%), and in the long term it was 38.6% (95% CI, 34.3%-43.0%; homogeneity χ2 = 11.51; df = 4; P = 0.02; I2 = 65.3%). When all time points were combined using the last data point in each study, the mean response rate was 40.1% (95% CI, 36.8%-43.4%; homogeneity χ2 = 17.52; df = 10; P > 0.05; I2 = 42.9%) (Table 2). Three studies reported strict TRS criteria, with a mean response rate of 35.2% (95% CI, 28.5%-42.3%; homogeneity χ2 = 2.17; df = 2; P > 0.05; I2 = 7.7%). For studies using Kane et al. 11 response criteria (or stricter), the mean response rate was 41.6% (95% CI, 37.0%-46.2%; homogeneity χ2 = 6.33; df = 4; P > 0.05; I2 = 36.9%).
Response Rate and Change in PANSS.a
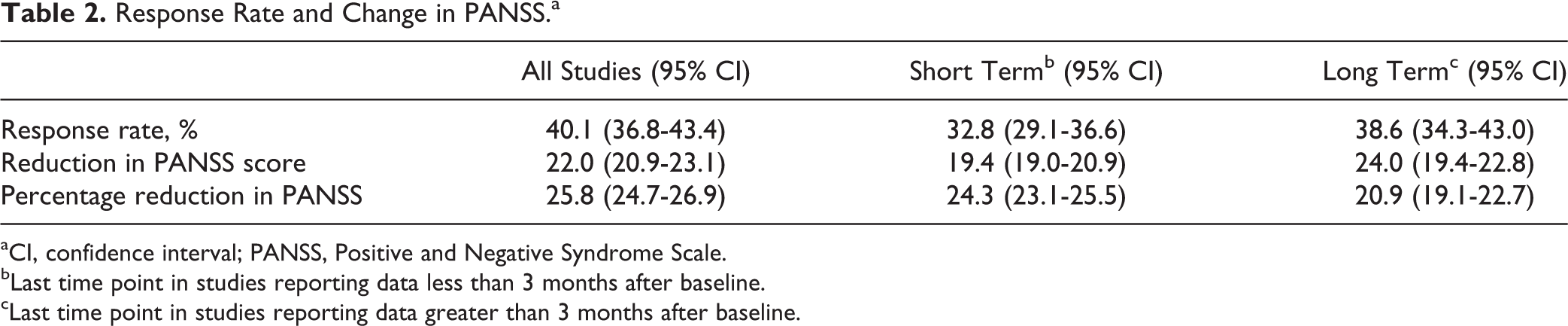
aCI, confidence interval; PANSS, Positive and Negative Syndrome Scale.
bLast time point in studies reporting data less than 3 months after baseline.
cLast time point in studies reporting data greater than 3 months after baseline.
Twenty studies provided data for absolute and percentage change in psychotic symptoms, 8,9,11 –15,17 –29 16 short term 8,9,11 –15,20 –25,27 –29 and 8 long term 15,17 –19,23,24,26,28 (4 had data for both time points 15,23,24,28 ). For short-term studies, the mean reduction in PANSS was 19.4 points (95% CI, 19.0-20.9) with a reduction of 24.3% (95% CI, 23.1%-25.5%) from baseline. Among long-term studies, the mean reduction in PANSS was –24.0 points (95% CI, 19.4-22.8) with a reduction of 20.9% (95% CI, 19.1%-22.7%) from baseline. When all time points were combined using the last data point in each study, the mean reduction in PANSS was 22.0 points (95% CI, 20.9-23.1) with a reduction of 25.8% (95% CI, 24.7%-26.9%) from baseline. When ρ was set at 0.7, the mean reduction in PANSS was 22.1 points, a reduction 25.6% from baseline, and when ρ was set at 0.8, the mean reduction in PANSS was 22.9 points, a reduction 26.0% from baseline. Unconverted BPRS percentage improvement was 3% to 5% greater than when converted to PANSS.
We could only undertake sensitivity analysis for the effect of differences in TRS criteria on 6 short-term studies. The mean reduction in PANSS for short-term strict TRS studies was 20.1 points (95% CI, 18.4-21.8) with a reduction of 27.7% (95% CI, 26.0%-29.4%) from baseline.
Discussion
Response rates for clozapine ranged from 32% in the short term to 39% in the long term. The absolute reduction in overall PANSS was clinically significant, being greater than the commonly used cutoff of 15.3 points. 30 The percentage change in PANSS was within, or greater than, the 16% to 24% range of a minimum clinically important difference. 30
One limitation of this analysis was that definitions of response varied between the studies. However, a sensitivity analysis on variations in criteria did not appreciably alter response rates. Similarly, a sensitivity analysis of the use of strict TRS criteria made only a small difference to response rates, although these studies had low heterogeneity. We had to impute standard deviations of absolute and percentage change in PANSS; however, varying ρ from 0.7 to 0.8 made little difference to the result. It has been noted in other studies that PANSS percentage improvement is lower than BPRS improvement by 4% to 5%, 5 which corresponds to our findings, and as such, our percentage improvement may be conservative. Our results showed heterogeneity and, as such, should be treated with caution.
Overall, these results suggest that patients, clinicians, and carers can hope for clinically meaningful improvement in psychotic symptoms with a trial of clozapine. Despite this finding, clozapine remains underutilised. 31 Only a third of people with TRS in an Australian jurisdiction had been given a trial of clozapine. 32 There is an urgent need to increase the access to clozapine for people with TRS globally. 31
However, this study also shows that 40% of people with TRS will fail to respond to clozapine, suggesting that 12% to 20% of all people with schizophrenia will be ultra-resistant, defined as failure to respond to adequate trials of 2 antipsychotics and clozapine. 1 Given the limited prospects of novel, more effective antipsychotics in the short to medium term, 33 there is a need to explore the use of existing agents that can augment the effects of clozapine and other antipsychotics, as well as greater access to evidence-based psychological therapies for people with schizophrenia. Further research into the biology of TRS may inform future treatment options.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DS is supported in part by NHMRC ECF AP1111136.