
Abstract
Objective:
Obsessive-compulsive symptoms (OCS) co-occur frequently with anxiety and depressive disorders, but the nature of their relationship and their impact on severity of anxiety and depressive disorders is poorly understood. In a large sample of patients with anxiety and depressive disorders, we assessed the frequency of OCS, defined as a Young Adult Self-Report Scale–obsessive-compulsive symptoms score >7. The associations between OCS and severity of anxiety and/or depressive disorders were examined, and it was investigated whether OCS predict onset, relapse, and persistence of anxiety and depressive disorders.
Methods:
Data were obtained from the third (at 2-year follow-up) and fourth wave (at 4-year follow-up) of data collection in the Netherlands Study of Anxiety and Depression cohort, including 469 healthy controls, 909 participants with a remitted disorder, and 747 participants with a current anxiety and/or depressive disorder.
Results:
OCS were present in 23.6% of the total sample, most notably in those with current combined anxiety and depressive disorders. In patients with a current disorder, OCS were associated with severity of this disorder. Moreover, OCS predicted (1) first onset of anxiety and/or depressive disorders in healthy controls (odds ratio [OR], 5.79; 95% confidence interval [CI], 1.15 to 29.14), (2) relapse in those with remitted anxiety and/or depressive disorders (OR, 2.31; 95% CI, 1.55 to 3.46), and (3) persistence in patients with the combination of current anxiety and depressive disorders (OR, 4.42; 95% CI, 2.54 to 7.70) within the 2-year follow-up period
Conclusions:
OCS are closely related to both the presence and severity of anxiety and depressive disorders and affect their course trajectories. Hence, OCS might be regarded as a course specifier signaling unfavorable outcomes. This specifier may be useful in clinical care to adapt and intensify treatment in individual patients.
Both anxiety and depressive disorders are clinically heterogeneous, and substantial differences in clinical presentation and course occur between individual patients. Clinical practice would benefit from specifiers that distinguish between mild disorders with favorable course trajectories and severe disorders with unfavorable course trajectories.
The presence and nature of comorbid disorders may signal unfavorable outcomes. For example, comorbidity between anxiety and depressive disorders is associated with higher illness severity, impaired functioning, unfavorable course, and poorer treatment outcome. 1 –6 Likewise, the combination of 2 anxiety disorders in an individual is associated with higher severity and chronicity compared with single anxiety disorders. 7,8 Further, in obsessive-compulsive disorder (OCD), comorbidity with anxiety and/or depressive disorders is associated with higher symptom severity, chronicity, and negative consequences in daily life. 9 –12 Even comorbid symptoms that by themselves do not reach a threshold to be considered a disorder may have an unfavorable impact on the course of the other disorders that they accompany. The most explicit example is panic attacks. Based on their negative impact on a variety of disorders, 13 –15 panic attacks are included as a specifier in the fifth edition of the Diagnostic Manual of Mental Disorders (DSM-5) 16 to alert clinicians to unfavorable outcomes.
Obsessive compulsive symptoms (OCS) occur in 30% to 40% of patients with an anxiety or depressive disorder. 4,17 Systematic studies of the impact of OCS on clinical outcome in anxiety disorders is—to the best of our knowledge—lacking, and studies on OCS and their impact on depressive disorders are scarce. In depressive disorders, one study has suggested that OCS are associated with poorer outcome. 18 Considering the suggestion from this study that OCS are associated with anxiety and depression symptom severity and have a negative impact on their course trajectories, this would mean that OCS might be a useful specifier signaling unfavorable outcomes.
Using longitudinal data from the Netherlands Study of Depression and Anxiety (NESDA), the present study was undertaken to examine the impact of OCS on anxiety and depressive disorders. We explored the impact of OCS on these disorders, above and over potential other confounders. We assessed the presence of OCS, examined the associations of OCS with severity of anxiety and/or depressive disorders, and investigated whether OCS predict onset, relapse, and persistence of anxiety and depressive disorders. We hypothesized that OCS are meaningful negative predictors of course in anxiety and depressive disorders.
Materials and Methods
Procedure
Data were obtained from NESDA. NESDA encompasses a longitudinal cohort study that has included 2981 adults (18-65 years of age) at baseline with anxiety disorders (panic disorder with/without agoraphobia, social phobia, and generalized anxiety disorder), with depressive disorders (major depressive disorder, dysthymic disorder), and healthy controls. A detailed description of the NESDA study design can be found elsewhere. 19 In short, the NESDA study aims to describe the long-term course and consequences of depressive and anxiety disorders in a sample recruited from the community, primary care settings, and specialized mental health care facilities. Persons with a clinically overt primary diagnosis of psychosis, posttraumatic stress disorder, or OCD were not included in the study, as were persons not fluent in the Dutch language. To study OCS, The Young Adult Self-Report Scale for obsessive compulsive symptoms 20 (YASR-OCS) was administered at the 2-year follow-up wave. Therefore, we used this wave as the baseline measurement point for the present study.
Approval of the study was granted by the Ethical Review Boards of all participating centers, and written informed consent was obtained from all participants.
Sample
As OCS were first assessed at the 2-year follow-up, we used this wave as the baseline measurement point for the present study and the 4-year wave of NESDA as the 2-year follow-up measurement of this study. For the present study, all participants who enrolled in both the 2-year and the 4-year follow-up (n = 2402) were included. The attrition rate between baseline and the 2-year wave of NESDA was 13% (n = 385). This attrition was not significantly related to gender and age but to lower level of education (odds ratio [OR], 0.92; 95% confidence interval [CI], 0.98 to 0.95) and to the presence of an anxiety (OR, 1.37; 95% CI, 1.23 to 1.54) and/or depressive disorder (OR, 1.64; 95% CI, 1.41 to 1.90) at baseline.
The attrition rate between the 2-year and 4-year wave of NESDA was 8% (n = 194).
The 24% attrition rate between baseline and the 4-year follow-up (n = 579) was not significantly related to gender and age but to lower level of education (OR, 0.93; 95% CI, 0.89 to 0.97) and to the presence of an anxiety (OR, 1.27; 95% CI, 1.15 to 1.41) and/or depressive disorder (OR, 1.32; 95% CI, 1.1 to 1.6) at baseline.
Participants who had not returned the YASR-OCS questionnaire (n = 270) and those with too many missing data (n = 7) were excluded. Thus, the final sample who completed both time points and returned the YASR-OCS consisted of 2125 participants. Compared with those who were excluded (n = 277), participants who were included (N = 2125) were older (P < 0.001), more frequently female (P = 0.04), less educated (P = 0.002), and had more anxiety and/or depressive disorders (P < 0.001) at our baseline (the 2-year follow-up of NESDA).
Measures
OCS
To assess OCS, the 8-item YASR-OCS was used, which is a subscale of the YASR 20 (see Figure 1 for items). Participants respond on a 3-point scale (0 = not true, 1 = somewhat true or sometimes true, 2 = very true or often true), yielding scores between 0 and 16 on the YASR-OCS. Incidents of missing data were very rare (0.5%) and therefore considered random. These missing data were not imputated. The YASR-OCS has good psychometric properties as a screener of OCS, with well-established cut points for the presence or absence of clinically significant OCS. 21 The internal reliability of the YASR-OCS in our sample was good (Cronbach’s α = 0.83). In line with the literature, OCS were regarded as significantly present with a score of >7 on the YASR-OCS. This cutoff has been previously identified as the best cutoff to predict OCD. 21
Items of the Young Adult Self-Report Scale, obsessive-compulsive symptoms (YASR-OCS 20 ).
Diagnostic Status
To diagnose anxiety and depressive disorders, the Composite International Diagnostic Interview (CIDI), version 2.1, was used, using DSM-IV criteria. The CIDI entails a structured interview with acceptable reliability and validity 22,23 and was administered by trained research staff.
Healthy controls were defined as participants without a lifetime history of a DSM-IV axis I diagnosis of an anxiety or depressive disorder (established using the CIDI). The patient group in this study who were defined as remitted was composed of patients with a lifetime history of an anxiety and/or depressive disorder but with no anxiety or depressive disorder within the past 6 months. The sample was not stratified by an anxiety or depressive disorder in the past, since recent literature shows that diagnostic instability between and within depressive and anxiety disorders is high and recurrence does not solely occur in the specific index disorders. 24 The patient group who were defined as suffering from a “current depressive disorder” contained participants with a diagnosis of a major depressive disorder and/or dysthymia within the past 6 months, and the group with a “current anxiety disorder” contained participants with a diagnosis of panic disorder and/or agoraphobia, social phobia, and/or generalized anxiety disorder, respectively, within the past 6 months. The group defined as “current comorbid anxiety and depressive disorder” contained participants with both a depressive and an anxiety disorder within the past 6 months.
Covariates
All covariates were assessed at ‘baseline’ of the present study (i.e. the two-year follow-up measurement of the NESDA study).
Socio-demographic factors included gender (male/female), age and years of education.
Severity of anxiety and depressive symptoms
Severity of anxiety symptoms was assessed with the Beck Anxiety Inventory (BAI), a widely used 21-item self-report questionnaire. 25 To determine the severity of depressive symptoms the Inventory of Depressive Symptomatology (IDS) was used, a 30-item self-report questionnaire. 26 Both scales have proven to be psychometrically valid and reliable. 27,28
Statistical Analyses
Participants with OCS were compared with those without OCS on sociodemographics and on symptom severity using 2-tailed chi-square statistics for categorical variables and 1-way analysis of variance statistics (ANOVA) for continuous variables. To examine the presence of OCS across diagnostic groups (healthy controls, remitted anxiety and/or depressive disorders, current anxiety disorder, current depressive disorder, current comorbid disorder), 2-tailed chi-square statistics were used. To examine whether the presence of OCS in persons with a current disorder was associated with the severity of these disorders as assessed on the BAI and IDS, 1-way ANOVA statistics were used.
To evaluate the impact of OCS on course trajectories, we defined subsamples. To study the impact of OCS on first onset of anxiety and/or depressive disorders, we used the subsample of healthy controls (n = 469). First onset in the healthy participants was defined as the presence of a diagnosis of anxiety and/or depressive disorder during the 2-year follow-up period. To examine “relapse,” we selected 909 participants who were remitted at first assessment. Relapse was defined as the presence of an anxiety and/or depressive disorder in the past 6 months. To examine “persistence,” participants with a current anxiety and/or depressive disorder at first assessment were selected. Persistence was defined as the 6-month presence of an anxiety and/or depressive disorder at follow-up.
First, chi-square statistics were conducted to examine whether course was more unfavorable in those with OCS versus in those without OCS. Next, bivariate regression analyses were conducted with onset, relapse, and persistence as dependent variables. Independent variables entailed the presence of OCS, gender, age, years of education, and anxiety and depression symptom severity parameters. No other possible confounders were explored. Finally, to assess whether OCS are independently associated with onset, relapse, and persistence of anxiety and/or depressive disorders, multivariate analyses were conducted, including all variables as covariates. P values <0.05 were considered significant. All statistical analyses were conducted with the SPSS statistical package version 20.0 (SPSS Inc., Chicago, IL).
Results
Sample Description
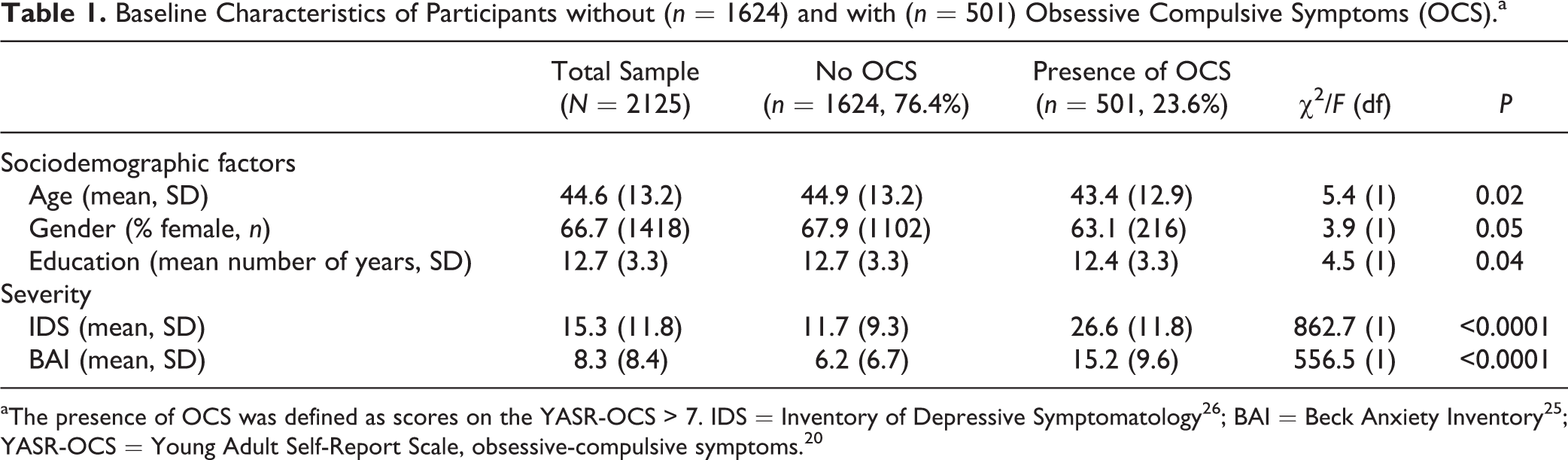
The sample consisted of 2125 participants with an average age of 44.6 years (SD, 13.2), who were predominantly female (66.7%) and had an average of 12.7 years of education (SD, 3.3). The mean IDS score was 15.3 (SD, 11.8), and the mean BAI score was 8.3 (SD, 8.4; see Table 1). Of the total sample, 22.1% (n = 469) were healthy controls, 42.8% (n = 909) had a remitted anxiety and/or depressive disorder, 9.6% (n = 205) had a current depressive disorder, 12.7% (n = 270) had a current anxiety disorder, and 12.8% (n = 272) had a current comorbid anxiety and depressive disorder.
Baseline Characteristics of Participants without (n = 1624) and with (n = 501) Obsessive Compulsive Symptoms (OCS).a
Presence of OCS
Using the predefined threshold on the YASR-OCS, 76.4% of the sample (n = 1624) did not have OCS (YASR-OCS ≤ 7), whereas in the remaining 23.6% (n = 501), OCS were present (YASR-OCS > 7). Participants with OCS were more likely to be male and younger and to report fewer years of education. In addition, the presence of OCS was associated with higher levels of anxiety and depressive symptoms (see Table 1).
The correlations between the YASR-OCS and IDS and between the YASR-OCS and BAI were 0.66 and 0.58, respectively.
Association between Current Presence of OCS and Presence and Severity of Anxiety and/or Depressive Disorders
The presence of OCS was associated with the presence of anxiety and depression; OCS were hardly present in healthy controls, were infrequently present in remitted patients, and were predominantly present in those with current anxiety and/or depressive disorders, χ2: 473.74 (df 4), P < 0.001. Results are presented in Figure 2.
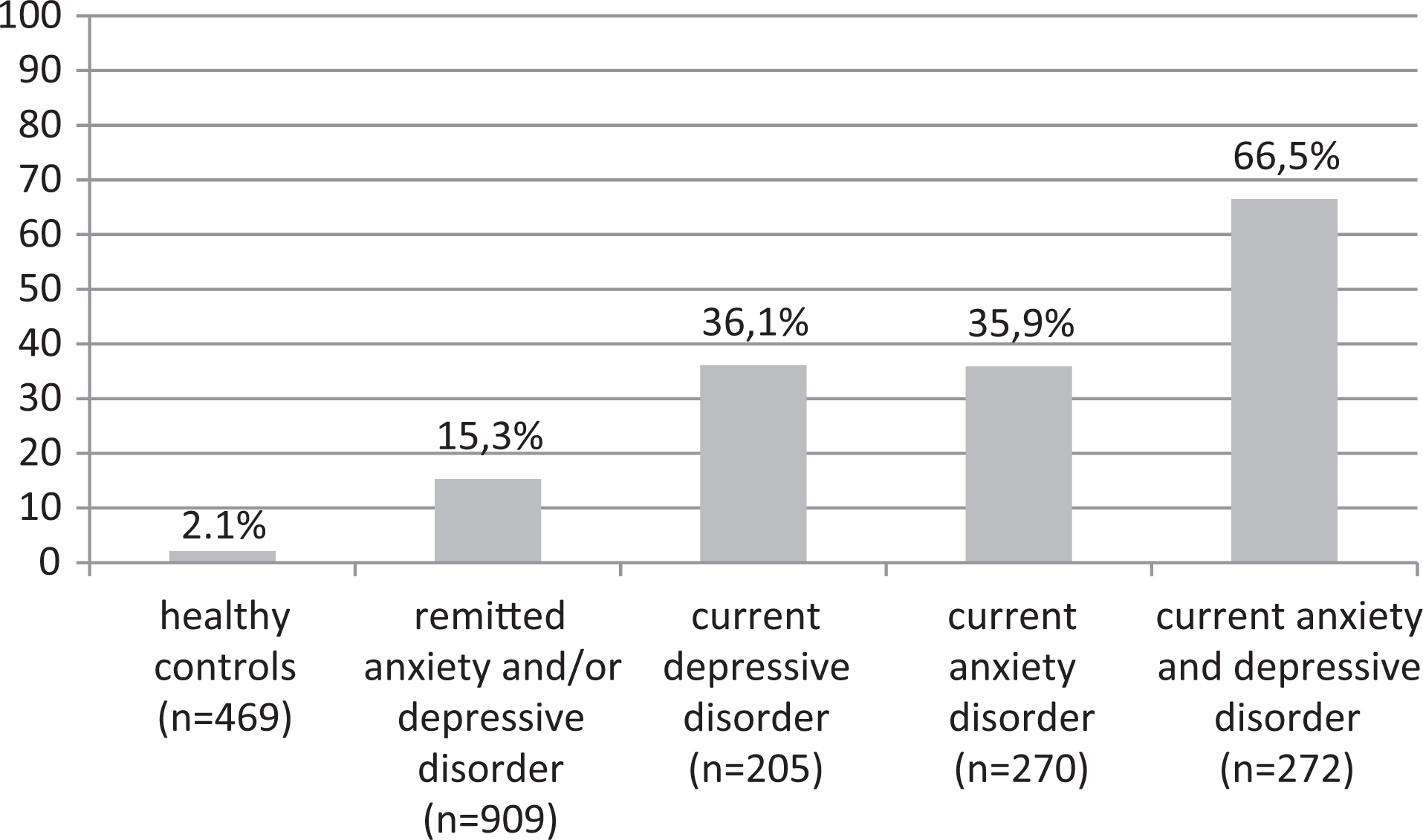
Presence of obsessive-compulsive symptoms (OCS) across healthy controls, participants with a remitted anxiety and/or depressive disorder, and participants with a current anxiety and/or depressive disorder (N = 2125). Presence of OCS was defined as scores on the YASR-OCS > 7. YASR-OCS = Young Adult Self-Report Scale, obsessive-compulsive symptoms. 20 Overall statistics: χ2: 473.74(df = 4), P < 0.001.
More specifically, among participants with a current disorder, the presence of OCS was associated with severity of the current disorder. Thus, in participants with a current depressive disorder, those with OCS had higher mean IDS scores than those without OCS (IDS 26.4 [SD, 11.0] vs 20.3 [SD, 10.8]; F 15.07 [df 1], P < 0.001). Likewise, in participants with an anxiety disorder, those with OCS had higher mean BAI scores as compared with those without OCS (BAI 14.5 [SD, 8.5] vs 11.8 [SD, 8.7]; F 5.95 [df 1], P = 0.02). Also, in participants with a comorbid anxiety and depressive disorder, both IDS and BAI scores were significantly higher in those with OCS as compared with those without OCS (IDS: 33.7 [SD, 11.5] vs 24.7 [SD, 10.7]; F 39.86 [df 1], P < 0.001, and BAI: 20.3 [SD, 10.0] vs 13.4 [SD, 8.4]; F 31.22 [df 1], P < 0.001).
Predictive Value of OCS on First Onset and 2-Year Course Trajectories of Anxiety and Depressive Disorders
First onset of anxiety and depressive disorders at 2-year follow-up occurred in 4.5% (n = 21) of the healthy controls and was associated with presence of OCS. Relapse within 2 years occurred in 19.5% (n = 177) of the participants with a remitted disorder at baseline. Relapse was significantly associated with OCS as well. The baseline disorder persisted in the 2-year follow-up period in 41.0% (n = 84) of participants with a depressive disorder, in 51.1% (n = 138) of those with anxiety disorders, and in 70.6% (n = 192) of the participants with a comorbid anxiety and depressive disorder. Persistence was significantly associated with the presence of OCS above the cut point in participants with a comorbid anxiety and depressive disorder but not in those with a single anxiety or depressive disorder. Results are presented in Table 2.
Impact of Obsessive Compulsive Symptoms (OCS) on the 2-Year Course Trajectory of Healthy Controls and Participants with Remitted or Current Anxiety and/or Depressive Disorders.a
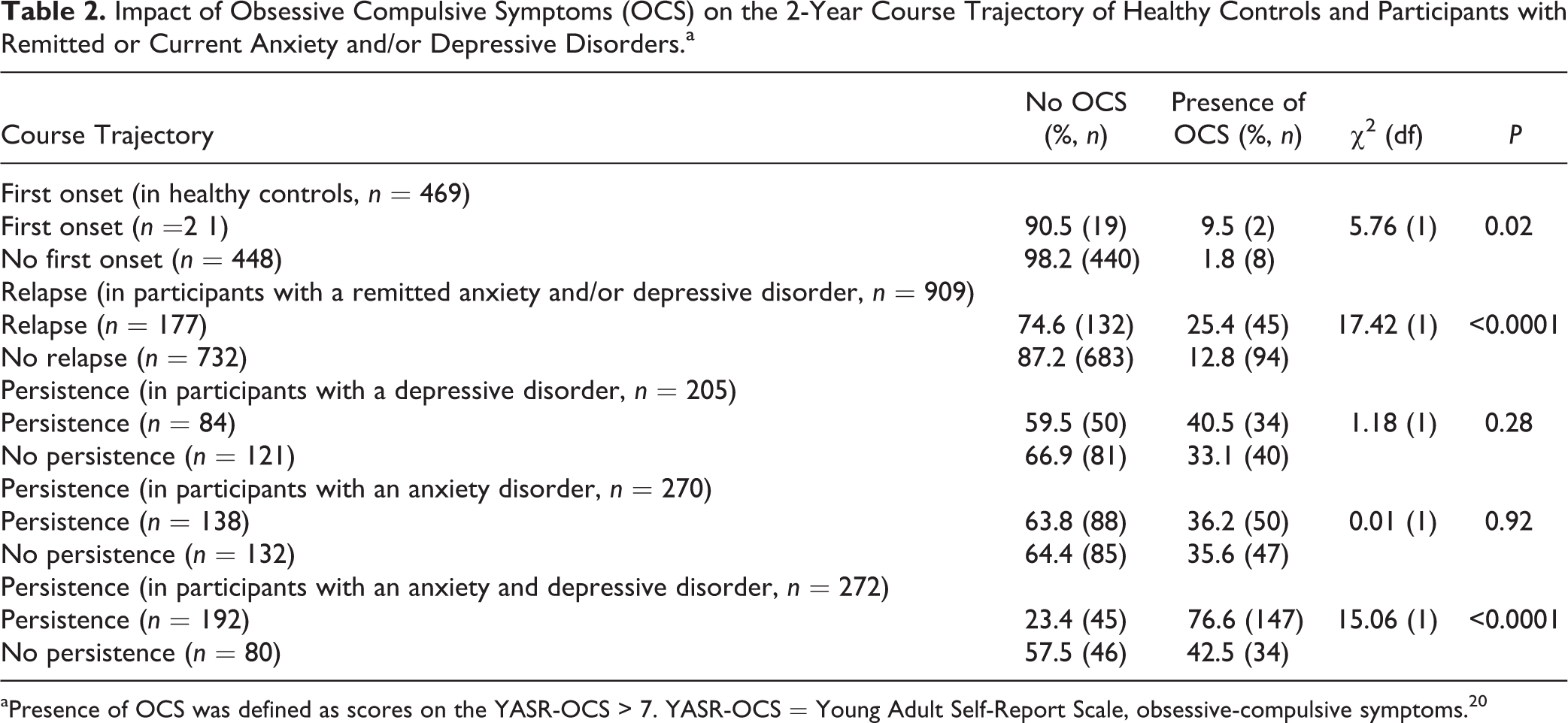
aPresence of OCS was defined as scores on the YASR-OCS > 7. YASR-OCS = Young Adult Self-Report Scale, obsessive-compulsive symptoms. 20
Table 3 presents the association between OCS, sociodemographic factors, symptom severity, and the presence of an anxiety and/or depressive disorder at follow-up. In healthy controls who developed an anxiety and/or depressive disorder (n = 21), only 2 showed OCS above cut point (OR, 5.79; 95% CI, 1.15 to 29.14; see Table 3). Post hoc analysis showed that the 21 participants who developed a disorder showed significantly higher mean YASR-OCS scores at baseline than the healthy controls who did not develop a disorder (mean YASR-OCS score 3.1 vs 1.4; F: 18.02 [df 1], P < 0.0001), suggesting that OCS in healthy controls are associated with development of anxiety or depressive disorders in the 2-year follow-up period.
Predictive Value of Obsessive Compulsive Symptoms (OCS) for First Onset, Relapse, and Persistence of Anxiety and/or Depressive Disorders.a
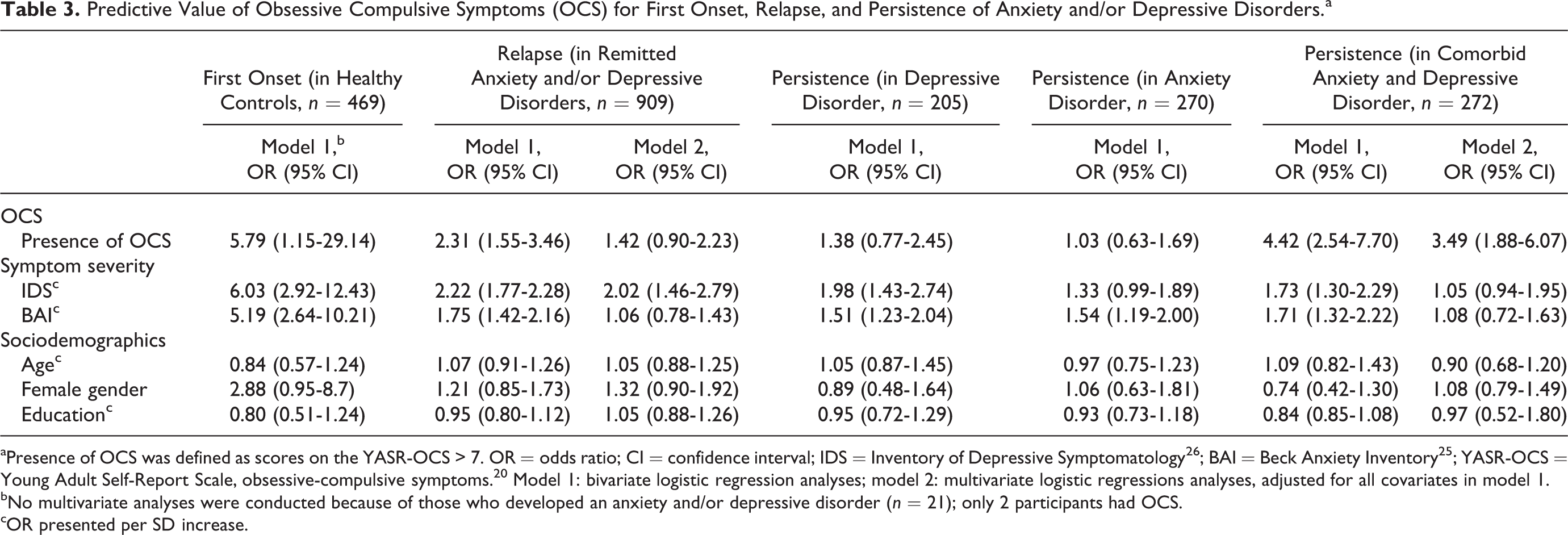
aPresence of OCS was defined as scores on the YASR-OCS > 7. OR = odds ratio; CI = confidence interval; IDS = Inventory of Depressive Symptomatology 26 ; BAI = Beck Anxiety Inventory 25 ; YASR-OCS = Young Adult Self-Report Scale, obsessive-compulsive symptoms. 20 Model 1: bivariate logistic regression analyses; model 2: multivariate logistic regressions analyses, adjusted for all covariates in model 1.
bNo multivariate analyses were conducted because of those who developed an anxiety and/or depressive disorder (n = 21); only 2 participants had OCS.
cOR presented per SD increase.
In participants with a remitted disorder, OCS were significantly associated with relapse (OR, 3.10; 95% CI, 2.13 to 4.50), but the association lost significance after adjusting for severity of anxiety and depressive symptoms.
As mentioned above, in single depressive and anxiety disorders, OCS were not significantly associated with persistence (OR, 1.38; 95% CI, 0.77 to 2.45 and OR, 1.03; 95% CI, 0.63 to 1.69, respectively), but in comorbid anxiety and depressive disorders, they were significantly associated with persistence (OR, 4.42; 95% CI, 2.54 to 7.70). This finding remained significant when adjusting for severity of anxiety and depressive symptoms (OR, 3.49; 95% CI, 1.88 to 6.07).
Discussion
No prior research has systematically examined the impact of comorbid OCS on clinical outcomes in anxiety disorders, and OCS impact has been studied in only one study in depressive disorders. Generally, our findings are in line with previous research indicating that comorbidity in anxiety and depressive disorders in general is associated with severity and chronicity 3 –5,9,29 and, more specifically, in depressive disorders, indicating that comorbid OCS is associated with poorer outcome. 18 Our findings implicate that OCS comorbidity may be a valuable specifier of outcome in both anxiety and depressive disorders, in line with findings of comorbid anxiety symptoms in depression and panic attacks across the full range of psychopathology that predict worse outcome. 14,16 For example, we found that relapse occurred in one-fifth of our sample. Given this high rate, which is consistent with relapse rates found in previous research on anxiety and depression comorbidities, 8,30 identifying patients at high risk for relapse is of utmost importance. Especially in anxiety disorders, predictors of relapse have been scarcely identified. 31 Our finding that OCS predicted relapse in anxiety and depression disordered patients means that standard screening for these patients with obsessive-compulsive symptomatology might be helpful to identify those at a higher risk for relapse. In this exploratory study on the relationship between OCS on one hand and anxiety and depressive disorders on the other, we found that significant OCS were present in a substantial proportion of participants with current anxiety and/or depressive disorders and was moreover associated with higher symptom severity of these disorders. In addition, OCS predicted first onset of anxiety and/or depressive disorder, relapse of anxiety and/or depressive disorders, and persistence in those with a comorbid anxiety and depressive disorder. Our results suggest that OCS does not predict relapse independently of anxiety and depression severity. This can be partially explained by symptom overlap between the measurement instrument for OCS on one hand (YASR-OCS) and anxiety and depression severity on the other; that is, correlations between the YASR-OCS and questionnaires used to assess severity of depression and anxiety were, respectively, 0.66 (between YASR-OCS and IDS) and 0.58 (between YASR-OCS and BAI). One might argue that OCS, anxiety, and depression share symptom overlap and that, as such, comorbid OCS are merely markers of symptom severity, which is by and of itself a predictor of worse outcome, rather than these findings suggesting a specific OCS-based prediction effect of worse outcome. In other words, rather than considering OCD, anxiety disorders, and depression as distinct disorders, which the original definition of comorbidity requires, 32 this type of comorbidity might be regarded as a correlate for severity of the index disorder. However, the finding that OCS predicted persistence in comorbid anxiety and depressive disorder independent of (and maybe even more than) severity of anxiety and depression argues against this line of reasoning and suggests that OCS also have specific unfavorable effects that do not overlap with general aspects of anxiety and depression. One drawback of the YASR-OCS, used to measure OCS, is that this instrument, although accurate in its sensitivity to detect OCS both in children and in adults, 20,21 has little specificity with respect to OC item content. As such, a more specific OC item containing self-report instruments, such as the Obsessive-Compulsive Inventory–Revised, 33 might suffer less from item overlap and be more useful for investigating the specificity of the unfavorable effect of OCS on outcome in anxiety and depressive disorders. In all, these findings of clear associations between OCS, and new onset, relapse, and (in comorbid cases) persistence in anxiety and depressive disorders suggest a role for OCS both as a marker of severity and as a specific OCS effect. With respect to a specific OCS-related effect, whether this is the result of a lack of flexibility to change and—as a consequence—decreased ability to profit from therapy in OCD associated with specific executive and neurobiological dysfunctions has not been addressed in this project. 32 However, future studies on this topic, coupled with intervention strategies that specifically target OC symptoms in anxiety and depressive disordered patients at an early stage of disease development, can direct new treatment avenues.
Several strengths and limitations should be taken into account. Strengths include the large sample size, the well-implemented design of the NESDA study, and the longitudinal design. Three limitations should be acknowledged as well.
First, as OCS were first assessed at the second wave of NESDA, we had no other option than to use this as our baseline measurement. This may have influenced results, as attrition and exclusion rates were somewhat selective.
Second, we assessed OCS with the YASR-OCS and used a cutoff score >7 to define the presence of clinically significant OCS. Because the diagnosis of OCD has not been assessed in NESDA, we cannot be certain whether participants scoring above the threshold on the YASR-OCS had in fact subthreshold symptoms or fulfilled criteria of obsessive-compulsive disorder. However, the cutoff score of the YASR-OCS used in the present study provides a reasonable sensitivity of 82.4% to predict presence of OCD 19 in the current sample. On the other hand, given the specificity of 69.7%, the YASR-OCS has a relatively high chance of false-positive findings. 19 Because persons with a primary diagnosis of OCD were not included in NESDA, we assume that the majority of participants scoring above the threshold had either subthreshold symptoms or had OCD but regarded this as a secondary problem. In all, it seems justified to conclude that a substantial level of OCS has a substantial predictive value. When generalizing these results to populations with comorbid OCD, it is likely that the negative effect of comorbid OCD is even larger than the results presented here.
Third, we used the term persistence to describe an unfavorable course trajectory, defined as the presence of a disorder at 2-year follow-up. This definition has not taken into account the in-between trajectory and—might be—remission proportions in between and therefore should be regarded as a rather rough measure of persistence.
Finally, because of limited numbers of participants with a first onset of an anxiety or depressive disorder, conclusions regarding first onset should be regarded preliminary.
Clinical Implications and Conclusion
OCS frequently co-occur in populations with anxiety and depressive disorders as a primary diagnosis. Although present, OCS might be unnoticed or unreported by patients because the focus of attention is on the primary diagnoses. However, as OCS seem to unfavorably influence course, it seems important to treat these symptoms from the early treatment stages on. What are adequate treatments of comorbid OCS? No pharmacological trials, to our knowledge, have specifically addressed this question. On the contrary, most studies exclude patients with OCS comorbidity. Thus, no evidence-based statements for the pharmacological treatment of comorbidity can be made at this time. There is growing, but contradicting, research on psychological treatment of comorbidity. Some research suggests that by treating the primary diagnosis, comorbid symptoms also decline. 34 –36 Although this might be the case, the presence of residual symptoms (not a full recovery of the comorbid disorder) is an important risk factor for relapse of the comorbid disorder. 37 Other research shows that simultaneous application of more than one disorder-specific cognitive behavioral therapy (CBT) does not seem to enhance treatment outcome. 38 Current research focusses on a new form of CBT: “transdiagnostic treatment.” This form of CBT targets more than one diagnosis by, for example, focusing on regulating emotions. 39 –42
Apart from the discussion of adequate treatment of comorbid OCS, OCS may thus serve as a specifier in clinical practice distinguishing between patients with mild disorders and favorable course trajectories and patients with severe disorders and unfavorable course trajectories. Since patients do not report these symptoms by themselves, the presence of OCS might be easily missed in clinical practice. 43 Clinicians should therefore proactively ask whether OCS are present. Administering a standard self-report questionnaire such as the YASR-OCS might help clinicians in their assessment.
To conclude, knowledge from the present study may add to models for profiling and staging of anxiety and depressive disorders that are currently being developed order to improve clinical prediction and to direct treatment. 44 –47
Footnotes
Acknowledgment
The infrastructure for the NESDA study is supported by participating universities and mental health care organizations (VU University Medical Center, GGZinGeest, Arkin, Leiden University Medical Center, GGZ Rivierduinen, University Medical Center Groningen, Lentis, GGZ Friesland, GGZ Drenthe, IQ Healthcare, Netherlands Institute for Health Services Research [NIVEL], and Netherlands Institute of Mental Health and Addiction [Trimbos]).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.