
Abstract
Objective:
Worldwide, there has been substantial controversy with respect to whether military deployment is a risk factor for suicidal behaviour. The present study examined the relationship between lifetime exposure to deployment and deployment-related traumatic events (DRTEs) and past-year suicidal ideation (SI), suicidal plans (SP), and suicidal attempts (SA).
Method:
Data were analysed from the 2013 Canadian Forces Mental Health Survey (8161 respondents; response rate, 79.8%; aged 18-60 years). A total of 12 individual items assessed exposure to DRTEs (e.g., combat, witnessing human atrocities, feeling responsible for the death of Canadian or ally personnel, knowing someone who was injured or killed). We examined each individual DRTE type as well as the number of types of DRTEs in relation to suicidal behaviour.
Results:
Lifetime deployment was not significantly associated with suicidal behaviour. In models adjusted for sociodemographic variables, most of the individual DRTE items and the DRTE count variable were significantly associated with suicidal behaviours (adjusted odds ratio ranged between 1.10 and 5.32). When further adjusting for child abuse exposure, these associations were minimally attenuated, and some became nonsignificant. In models adjusting for mental disorders and child abuse, most DRTEs and number of types of DRTEs became nonsignificant in relation to SI, SP, and SA.
Conclusions:
Active military personnel exposed to increasing number of DRTEs are at increased risk for SI, SP, and SA. However, most of the association between DRTEs and suicidal behaviour is accounted for by child abuse exposure and mental disorders.
Introduction
Some nations have seen substantial increases in the prevalence of suicidal behaviour in active duty military and veterans. 1,2 Suicidal ideation (SI), suicidal plans (SP), and suicidal attempts (SA) are strong risk factors for death by suicide. 3 Recent work has demonstrated a substantial lifetime prevalence of SI (15.4%), SP (6.1%), and SA (3.0%) in the 2013 nationally representative sample of Canadian active military personnel. 4 These rates are very similar to the Canadian general population with lifetime SI (13.3%), SP (4.6%), and SA (3.5%). 4
Although there are many theoretical models that explain suicidal behaviour (Durkheim, 5 Mann et al., 6 Hawton et al., 7 and Zamorski 8 ), Joiner’s interpersonal theory of suicide 9 is particularly relevant among military personnel. Joiner’s theory posits that an individual will die by suicide if he or she has both the desire to die and the acquired ability to carry out suicidal behaviour. He posits that the desire of death develops when the person perceives himself or herself to be a burden on others and/or experiences a sense of loneliness. The acquired ability to attempt suicide occurs through habituation of painful experiences such as previous self-harm behaviour, physical abuse, physical fights, and indirect exposure to death and loss (e.g., physicians and soldiers).
Empirical literature on risk factors for suicidal behaviour among military personnel and veterans can be understood in relation to sociodemographic and military factors, 1,10 predeployment factors (e.g., child abuse exposure), 11 deployment-related trauma (e.g., combat exposure), 12 –14 and postdeployment factors (e.g., mental disorders, poor social supports, and separation from service). 15 –18
There has been substantial controversy with respect to the association between deployment to combat and peacekeeping missions and suicidal behaviour. Many studies have examined an overall deployment variable (e.g., ever deployed vs. never deployed) in relation to suicide risk. With this approach, most studies have found no relationship between deployment and suicidal behaviour. 18,19 A recent meta-analysis of 22 studies found a modest effect, 25% increase in risk, of deployment associated with suicidal behaviour. 20 However, many argue that exposure to traumatic events during deployment (which varies substantially from deployment to deployment and from person to person) is more important to study in relation to suicidal behaviour than a dichotomous (ever vs. never) deployment variable. 21 A smaller number of studies examining exposure to specific events during deployment (e.g., witnessing atrocities and dead bodies) have found a larger association between traumatic events and suicidal behaviour. 20,22,23 In summary, these studies suggest the need to examine in greater detail the types of events experienced by military personnel during deployment to better understand their association with suicidal behaviour.
There are several limitations of the current literature on deployment and suicide risk. First, many studies have not captured details of exposure to specific traumatic experiences during deployment. 1,19 To our knowledge, previous work has not examined deployment history, exposure to specific traumatic events, and increasing number of traumatic events during deployment in relation to suicidal behaviour in the same population. Second, many studies did not assess or adjust for child abuse exposure, which is emerging as an important premilitary risk factor for suicidal behaviour. 11 Third, while some studies have adjusted for mental disorders when examining the association between deployment-related traumatic events (DRTEs) and suicide risk, 2,19 others have not. 12 One could argue that controlling for mental disorders in these models is adjusting for a variable that is part of the causal pathway. For example, DRTEs may increase the likelihood of developing a mental disorder, which in turn increases the risk for suicidal behaviour. However, due to the cross-sectional nature of most studies in the area, it is difficult to test this hypothesis. On the other hand, from a public health perspective, it is also important to know whether DRTEs have an independent effect on suicidal behaviour after adjusting for mental disorders. Such a relationship would suggest the need for postdeployment screening and intervention methods to go beyond screening for mental disorders and also include exposure to DRTEs. Furthermore, it is also possible that DRTEs and mental disorders have a synergistic effect on suicidal behaviour. To our knowledge, no study has examined the interaction between DRTEs and mental disorders in relation to suicidal behaviour.
To address these important gaps in the literature, we analysed data from a nationally representative sample of active military personnel (the 2013 Canadian Forces Mental Health Survey). 4 This in-person interview survey assessed 12 types of potentially traumatic events during deployment, past child abuse experiences, mental disorders, and SI, SP, and SA.
In this study, we examined lifetime deployment, exposure to individual, and increasing number of types of DRTEs in relation to SI, SP, and SA. We hypothesise that certain DRTEs (e.g., witnessing atrocities and death) 13 will remain independently associated with suicidal behaviour even after adjustment for sociodemographic variables, mental disorders, and child abuse exposure. We also hypothesised that there will be a significant interaction between DRTEs and mental disorders, elevating the risk for suicidal behaviour.
Methods
Survey
Data were drawn from the 2013 Canadian Forces Mental Health Survey (CFMHS) (N = 8161, response rate = 79.8%). Detailed methodology of this national survey has been published elsewhere. 4,11,24 The CFMHS comprised a representative sample of the Regular Force military personnel (n = 6692, approximately 46% of whom had deployed in support of the mission in Afghanistan) and a sample of Reserve Force personnel (n = 1469) who deployed in support of the mission in Afghanistan. 24 Reservists who had not deployed in support of the mission in Afghanistan were not included in the survey. The survey was voluntary, and privacy and confidentiality of the respondents are ensured under the Statistics Act. 25 Respondents provided informed consent. The authors obtained approval from Statistics Canada to conduct this analysis.
Measurements
Suicidal behaviours
Suicide-related behaviours consisted of SI, SP, and SA, which were assessed based on past-year and lifetime time frames. Respondents were asked if they had 1) seriously thought about committing suicide or taking their own life, 2) made a plan for committing suicide, or 3) attempted suicide or tried to take their own life. Age of onset data were not available for suicidal behaviour or DRTEs. To address this limitation, and consistent with previous literature, we examined the impact of lifetime DRTEs on past-year suicidal behaviour. 6
Deployment and DRTEs
Lifetime deployment was based on whether the respondent endorsed any deployment (yes or no). There were 3 sections in the survey where participants were asked about DRTEs:
Deployment-specific CFMHS 2013 items
DRTEs included the following: 1) known someone who was seriously injured or killed; 2) found yourself in a life-threatening situation where you were unable to respond because of rules of engagement; 3) ever been injured; 4) ever seen ill or injured women or children who you were unable to help; 5) ever received incoming artillery, rocket, or mortar fire; 6) ever felt responsible for the death of Canadian or ally personnel; 7) ever had a close call (e.g., shot or hit but protective gear saved you); and 8) ever had difficulties distinguishing combatants from noncombatants. These items were selected from a longer combat exposure inventory, 26,27 based on conceptual and empirical considerations. 26 Personnel indicating that they had not ever been deployed were coded as having zero DRTEs.
Lifetime posttraumatic stress items
We also examined items from the traumatic events section of the posttraumatic stress disorder (PTSD) Composite International Diagnostic Interview (CIDI) trauma inventory 28 that were likely to have occurred during deployment: 1) participated in combat, 2) peacekeeping or relief worker in a war zone, and 3) witnessing atrocities or massacres such as dead bodies. These items have been used previously. 12
Deployment-related sexual assault
Lifetime sexual assault was assessed using 2 items also on the PTSD CIDI trauma inventory relating to ever having experienced 1) forced sexual activity or 2) unwanted sexual touching. Those endorsing each of these items were asked if any of the underlying events had occurred while deployed. Endorsing either item was coded as deployment-related sexual assault (yes or no).
We created a count variable (0-12) to examine the impact of increasing number of types of DRTE on the risk for suicidal behaviour. Since this a unique combination of DRTE items, we tested the reliability of the DRTE scale. We found high reliability with an α of >0.8. We also did sensitivity analyses with an 8-item DRTE scale that did not include the 3 PTSD module items and sexual trauma. The results of the 12-item and 8-item scales were consistent.
Child abuse experiences
Items from the Childhood Experiences of Violence Questionnaire (CEVQ) 29 were used to measure physical abuse and exposure to intimate partner violence (IPV). Childhood abuse items pertained to abuse that occurred before the age of 16 years. Binary classifications of child abuse (present/absent) were made based on the CEVQ recommendations: physical abuse was present if 1 or more of 3 variables met the following threshold criteria: 1) being slapped on the face, head, or ears or hit or spanked with something hard 3 times or more; 2) being pushed, grabbed, shoved, or having something thrown at the respondent to hurt him or her 3 times or more; and 3) being kicked, bit, punched, choked, burned, or physically attacked 1 time or more. Exposure to IPV was measured by asking the respondent if he or she had seen or heard parents, stepparents, or guardians hitting each other or another adult in the home 3 times or more. Similar to previous work, 30 sexual abuse was assessed using 2 items and was classified as present if either of the following occurred 1 time or more: 1) attempted or being forced into unwanted sexual activity by being threatened, held down, or hurt in some way and/or 2) sexually touched, meaning unwanted touching or grabbing, kissing, or fondling against the respondent’s will. A respondent was classified as having experienced any child abuse if he or she met the threshold criteria for at least 1 of the 3 types of abuse. 11 A count variable was computed based on the total number of types of abuse experienced (ranging from 0 to 3). 30
Mental disorders
The World Mental Health Survey CIDI 28 for DSM-IV was used to assess the presence of the following lifetime and past-year disorders: depression, generalised anxiety disorder, panic disorder and/or panic attacks, posttraumatic stress disorder, and alcohol abuse or dependence. For this article, we combined all disorders together to create a dichotomous variable to assess the presence of any past-year mental disorder (yes/no).
Sociodemographic covariates
The sociodemographic covariates included age, sex, race, education, household income, marital status, military force type (Regular or Reserve), and military rank category (junior noncommissioned member [NCM], senior NCM, and officer).
Statistical Analysis
To ensure population representation, statistical weights were applied. Bootstrapping was performed for variance estimation to account for the complex sample. First, descriptive statistics were calculated for each variable used in the analysis. Second, based on previous literature suggesting a differential response between sex and DRTE exposure, 31,32 we tested for effect modification between sex and DRTEs. We did not find any of these interaction terms significant in the prediction of suicidal behaviour. Third, a series of separate multivariable logistic regression models were computed to determine if individual DRTEs and number of types of DRTEs increased the likelihood of suicide-related outcomes. Separate regressions were conducted for lifetime deployment, each DRTE, and the DRTE count variable. In the first adjusted models (adjusted odds ratio [AOR]–1), we included sociodemographic variables, including age, sex, race, education, household income, marital status, military force type, and military rank. In the second adjusted models (AOR-2), we included all variables in AOR-1 and added a count variable of child abuse experiences. In the third adjusted models (AOR-3), we included all variables in AOR-1 and AOR-2 and added the dichotomous any past-year mental disorder variable. Finally, we tested for interactions between the DRTE count variable and mental disorders in relation to suicidal behaviour.
Results
Table 1 shows the prevalence of all the variables in the sample, including sociodemographic variables, DRTEs, child abuse experience, and mental disorders. Among the DRTEs, exposure to combat, known someone seriously injured or killed, and received incoming artillery, rocket, or mortar fire were the 3 most common DRTEs, while sexual trauma during deployment was the least common DRTE.
Prevalence and Means for the Independent and Dependent Variables in the Sample (N = 8161).a
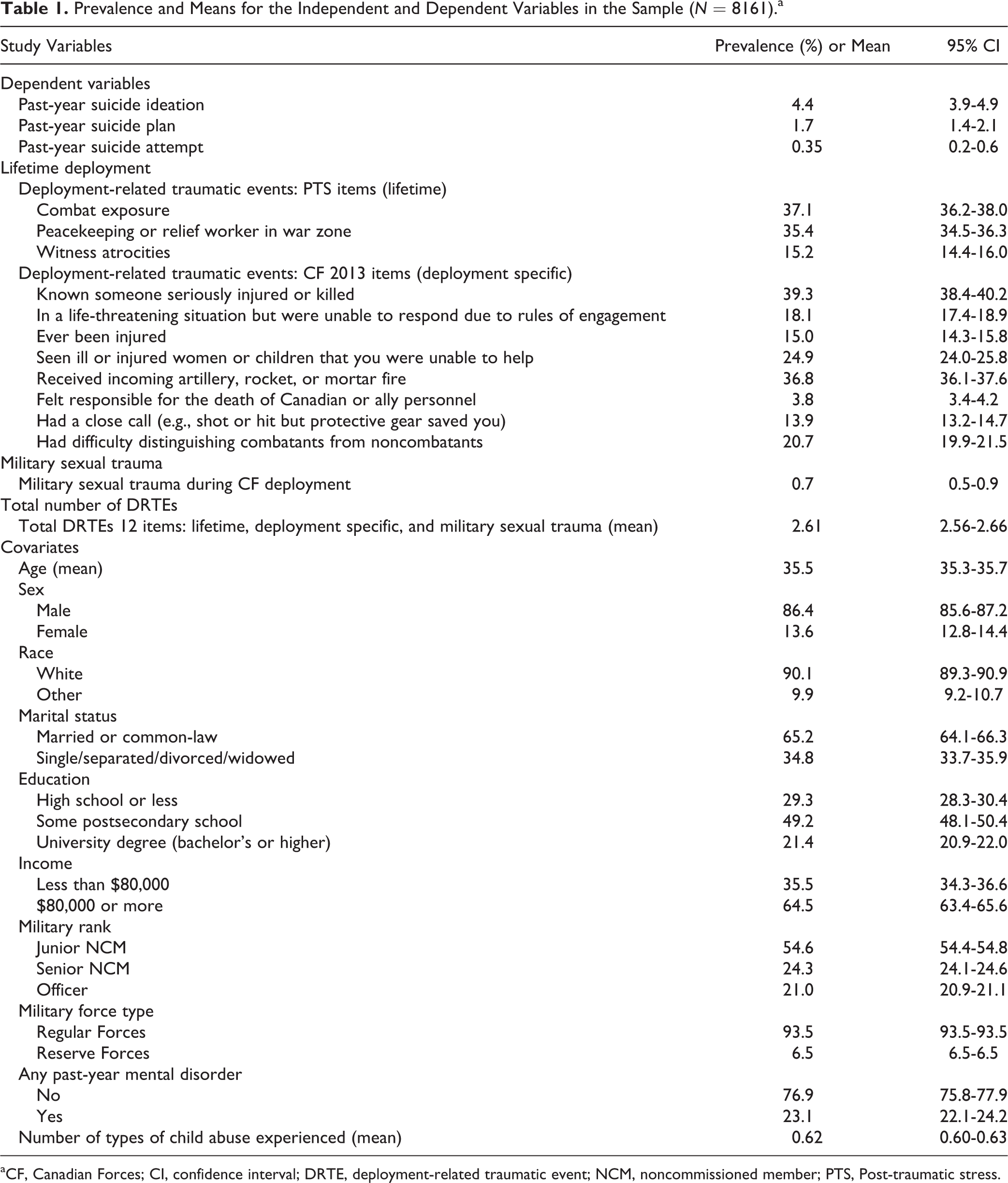
aCF, Canadian Forces; CI, confidence interval; DRTE, deployment-related traumatic event; NCM, noncommissioned member; PTS, Post-traumatic stress.
Table 2 presents the regression models for lifetime deployment and individual DRTEs in relation to past-year SI. Lifetime deployment was not significantly associated with SI in any of the 3 models. In models adjusting for sociodemographic variables (AOR-1), all the individual DRTEs, with the exception of sexual trauma, were independently associated with SI (AOR between 1.31 and 2.92). In models that added child abuse exposure (AOR-2), 6 of the 12 DRTEs items became nonsignificant (AOR between 1.40 and 2.51). In AOR-3, adjusting for any mental disorder, all the DRTEs with the exception of one (“felt responsible for death of Canadian or ally personnel”) became nonsignificantly associated with SI. The DRTE count variable was significantly associated with SI in AOR-1 and AOR-2 but became nonsignificantly associated with SI in AOR-3.
Lifetime Deployment and Deployment-Related Traumatic Events and Past-Year Suicide Ideation.a
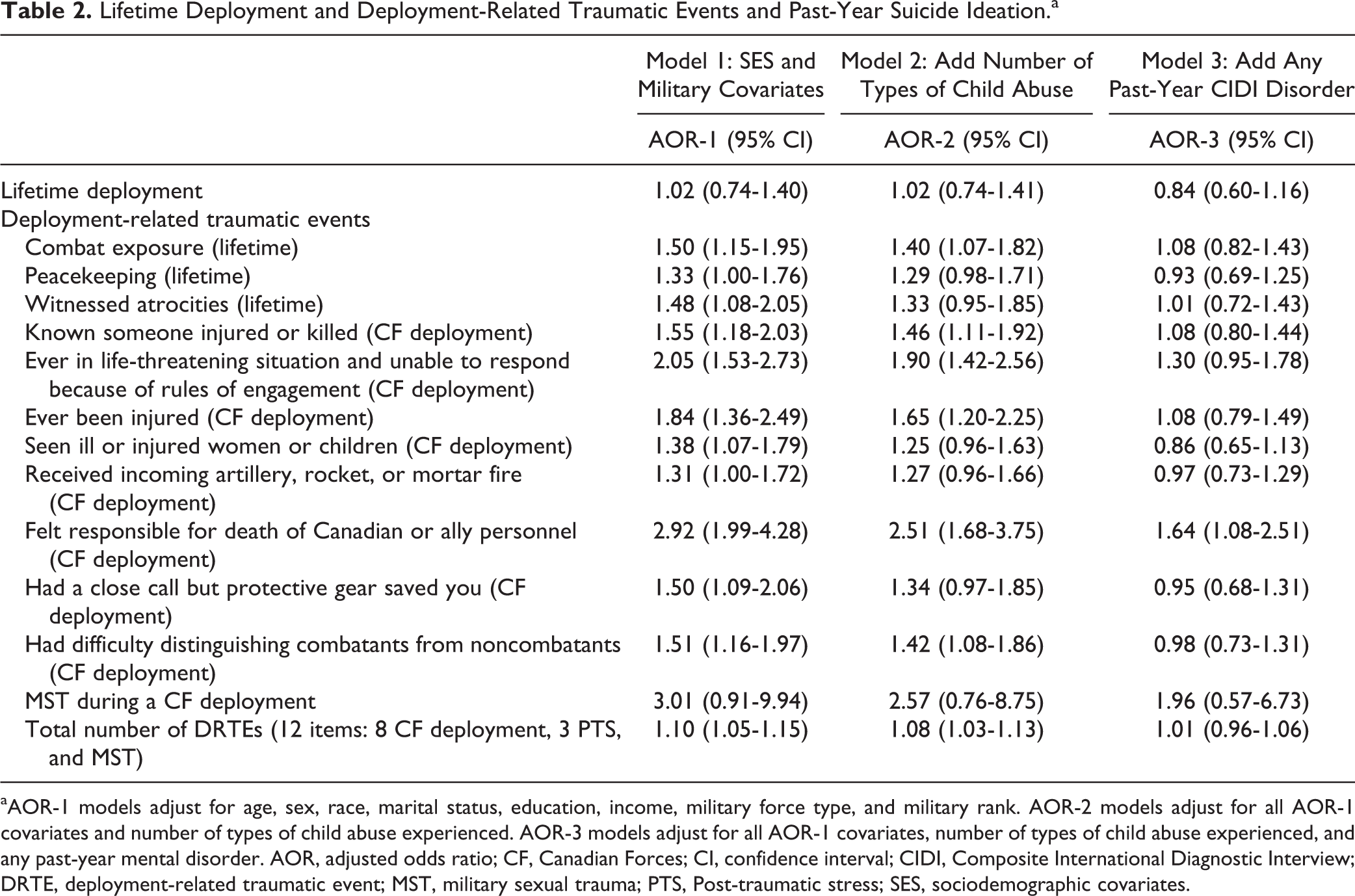
aAOR-1 models adjust for age, sex, race, marital status, education, income, military force type, and military rank. AOR-2 models adjust for all AOR-1 covariates and number of types of child abuse experienced. AOR-3 models adjust for all AOR-1 covariates, number of types of child abuse experienced, and any past-year mental disorder. AOR, adjusted odds ratio; CF, Canadian Forces; CI, confidence interval; CIDI, Composite International Diagnostic Interview; DRTE, deployment-related traumatic event; MST, military sexual trauma; PTS, Post-traumatic stress; SES, sociodemographic covariates.
Table 3 presents the relationship between lifetime deployment and individual DRTEs and past-year SP. Lifetime deployment was not significantly associated with SP in any of the 3 adjusted models. There was insufficient power to test the relationship between deployment-related sexual assault in relation to SP. In AOR-1 models, all the individual DRTEs were significantly associated with SP (AOR between 1.76 and 3.59). In AOR-2 models, where child abuse exposure was included, most of the DRTEs remained significantly associated with SP (AOR between 1.54 and 2.81). However, in AOR-3 models, where any mental disorder was included, all the DRTEs became nonsignificant. The DRTE count variable was significantly associated with SP in AOR-1 and AOR-2 but became nonsignificantly associated with SP in AOR-3.
Deployment and Deployment-Related Traumatic Events and Past-Year Suicide Plans.a
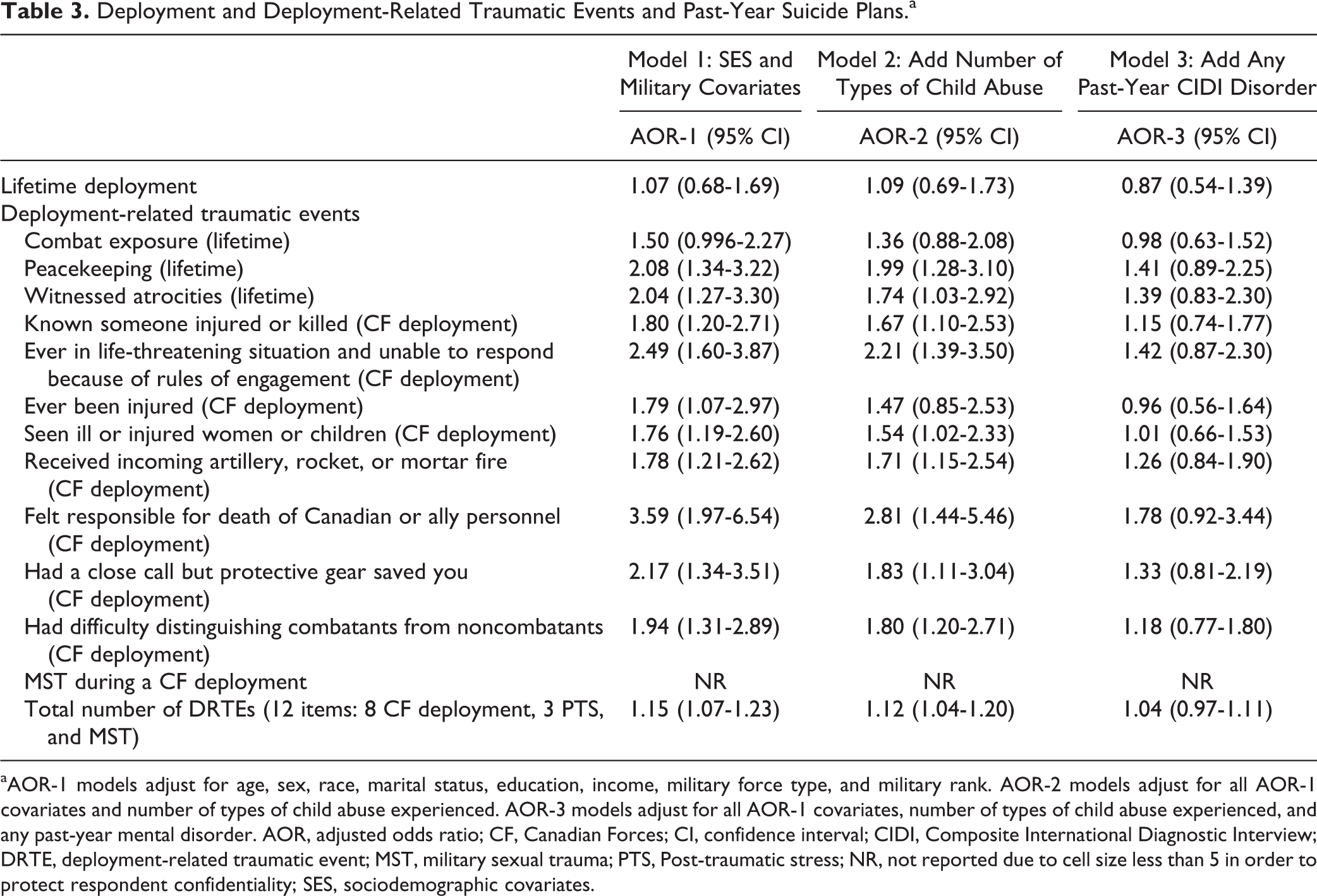
aAOR-1 models adjust for age, sex, race, marital status, education, income, military force type, and military rank. AOR-2 models adjust for all AOR-1 covariates and number of types of child abuse experienced. AOR-3 models adjust for all AOR-1 covariates, number of types of child abuse experienced, and any past-year mental disorder. AOR, adjusted odds ratio; CF, Canadian Forces; CI, confidence interval; CIDI, Composite International Diagnostic Interview; DRTE, deployment-related traumatic event; MST, military sexual trauma; PTS, Post-traumatic stress; NR, not reported due to cell size less than 5 in order to protect respondent confidentiality; SES, sociodemographic covariates.
Table 4 presents the relationship between lifetime deployment and individual DRTEs and past-year SA. Lifetime deployment was not associated with SA in any of the 3 models. In AOR-1, 7 of the 12 DRTE items were independently associated with SA (AOR between 1.92 and 5.32). In AOR-2, only 4 of the 12 items were significantly associated with SA (AOR between 2.81 and 5.07). In AOR-3, only “being unable to respond to a life-threatening situation because of rules of engagement” remained significantly associated with SA. The DRTE count variable was significantly associated with SA in AOR-1 and AOR-2 but became nonsignificantly associated with SA in AOR-3.
Deployment-Related Traumatic Events and Past-Year Suicide Attempts.a
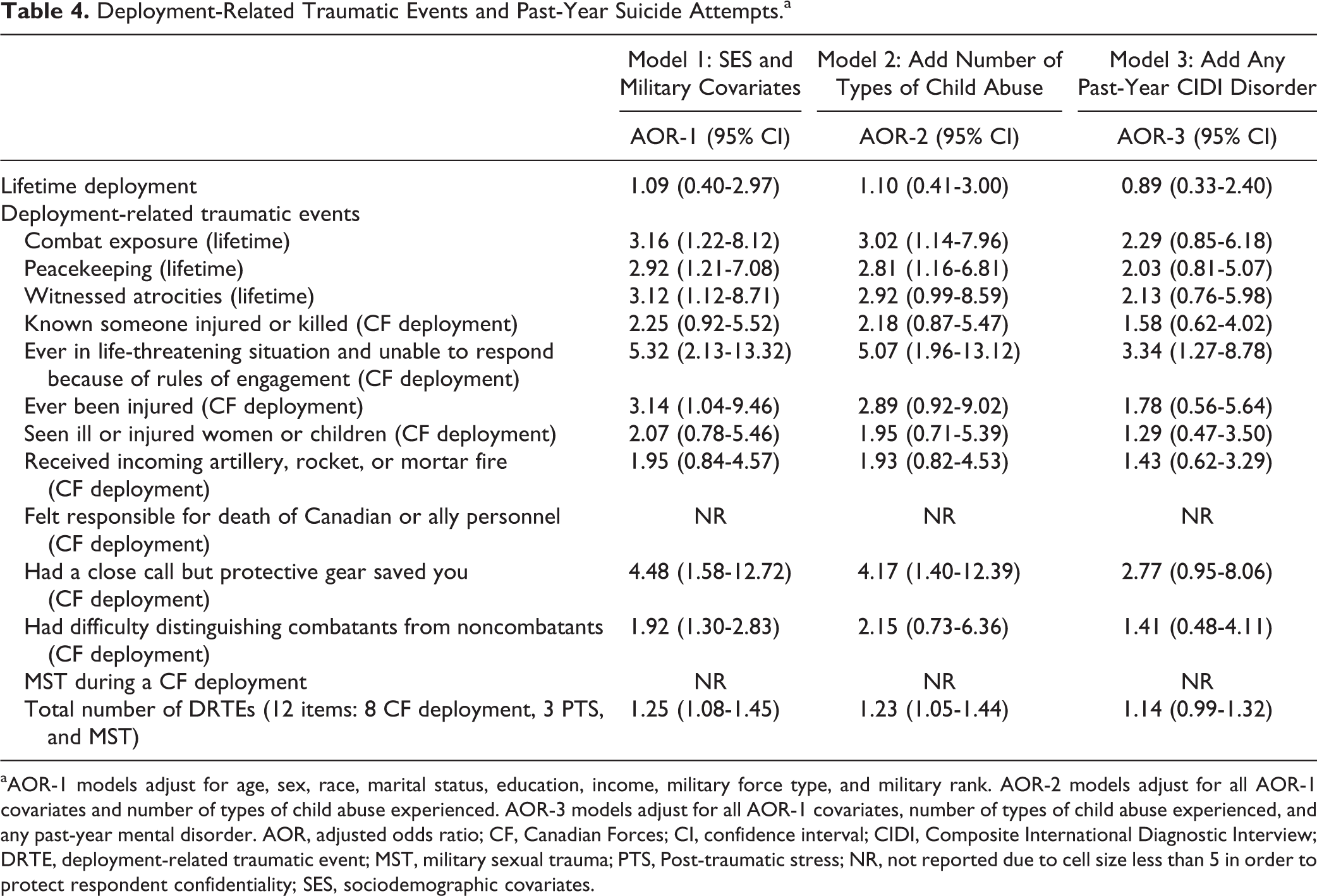
aAOR-1 models adjust for age, sex, race, marital status, education, income, military force type, and military rank. AOR-2 models adjust for all AOR-1 covariates and number of types of child abuse experienced. AOR-3 models adjust for all AOR-1 covariates, number of types of child abuse experienced, and any past-year mental disorder. AOR, adjusted odds ratio; CF, Canadian Forces; CI, confidence interval; CIDI, Composite International Diagnostic Interview; DRTE, deployment-related traumatic event; MST, military sexual trauma; PTS, Post-traumatic stress; NR, not reported due to cell size less than 5 in order to protect respondent confidentiality; SES, sociodemographic covariates.
We also tested interaction terms between mental disorders and the DRTE count variable for each suicidal behaviour. There was no significant interaction between number of types of DRTEs and mental disorders for the outcomes of SI and SP. There was not enough power to test the interactions between number of types of DRTEs and mental disorders for SA.
Discussion
The present study provides important new information on the controversial relationship between deployment and suicidal behaviour. There are 4 key findings from this research. First, lifetime history of deployment was not significantly associated with past-year SI, SP, and SA. Second, we found a relationship between exposure to multiple individual DRTEs and number of types of DRTEs and SI, SP, and SA. Third, child abuse and DRTEs were significantly correlated, but the relationships between DRTEs and suicidality persisted even after adjustment for child abuse. Fourth, we demonstrated that most of the relationship between individual DRTEs and suicidal behaviour was accounted for by mental disorders. To our knowledge, this is the most comprehensive and in-depth examination of the impact of specific traumatic events during deployment in relation to SI, SP, and SA.
Our findings are consistent with previous literature in this area showing that exposure to traumatic events during deployment has greater explanatory value for suicidal behaviour than an omnibus “ever deployed” variable. 21 Similar to the established dose-response relationship between deployment experiences and posttraumatic stress disorder and other mental disorders, 33,34 this study underscores that a similar dose-response relationship exists between deployment experiences and suicidal behaviour. We also found that certain DRTEs had stronger associations with suicidal behaviour than others. Military personnel who reported being responsible for the death of a Canadian ally or being unable to respond to a life-threatening situation because of rules of engagement were at substantially higher odds of reporting suicidal behaviour. These particular events might be especially stressful in creating anxiety and guilt that might increase the risk of SI, SP and SA. These findings provide empirical support for Joiner’s interpersonal theory of suicide where exposure to death may be an important part of the development of suicidal behaviour. 35
In this study, we also demonstrated the importance of adjusting for the effects of child abuse experiences in examining the relationship between DRTE and suicidal behaviour. Early experiences of trauma are well known to increase the vulnerability to both mental disorders and suicidal behaviour. 34,36 Our previous work has shown that military personnel have a high prevalence of child abuse exposure, which is strongly associated with suicidal behaviour. 11 It is important to underscore that many of the specific DRTEs and the DRTE count variable remained significantly associated with suicidal behaviour in models adjusted for child abuse exposure. Child abuse exposure also remained significantly associated with suicidal behaviour. These findings support the importance of a dose-response relationship between DRTEs and suicidal behaviour among military personnel. However, the association between number of DRTEs and suicidal behaviour became nonsignificant when adjusting for mental disorders.
Previous studies in the literature have sometimes adjusted for the effects of mental disorders, 19 while others have not. 12 Thus, our study is consistent with earlier work that has found a significant relationship between DRTEs and suicidal behaviour without accounting for the effects of mental disorders. Furthermore, most studies that have adjusted for the effects of mental disorders have found small or nonsignificant relationships between deployment and suicide. Future studies could consider examining whether specific mental disorders mediate the relationship between DRTEs and suicidal behaviour.
The findings of this study need to be considered in the context of several strengths and limitations. The strengths include the use of 1) a large, contemporary, representative sample; 2) state-of-the-art epidemiological methods using the World Health Organization CIDI 28 ; and 3) use of a broad list of DRTE items.
There are 5 major limitations of the current study. First, the survey was a cross-sectional design that did not assess information related to the age of onset of the deployment, mental disorders, and suicidal behaviour. To address this issue, similar to previous work, 12 we used lifetime DRTEs with past-year suicide-related outcomes. We also adjusted for mental disorders during the past year. It would have been ideal to have age of onset of mental disorders, traumatic events, and suicidal behaviour such that we could explore the temporal relationships between these 3 variables. Our current study is limited by the fact that mental disorders and suicidal behaviour could have had their onset prior to the deployment. Second, the current survey used a single-item measure of suicide attempt. Some of the analysis was limited by power, especially with the SA outcomes. We did not have detailed information about the number and lethality of SA. Although the item used in the current survey is part of the CIDI used worldwide, 37 recent work is showing that a single-item measure of suicide attempts may have limited reliability and validity. 38,39 For example, in 1 study, only 60% of people who endorsed a single item of “Have you ever attempted suicide?” were classified as having a history of suicide attempt based on follow-up questions. 38 Third, the composite DRTE measure was uniquely created from several items assessed in the survey. Although we found high reliability of the scale and the items have face validity, the items do not measure severity and perceived threat during exposure to the DRTE. Perceived threat during exposure to trauma has been strongly associated with subsequent mental health problems. 40 Fourth, we also were not able to account for the effects of other adult traumatic events because it was not clear whether the traumatic event reported occurred during deployment. Finally, the findings of this study may not be generalizable to deaths by suicide. We want to highlight that in our study, and in other studies, SA and suicide deaths have a low prevalence. So, although the AORs in this study were not significant, many AORs were greater than 2.0, showing that the data may not have enough power to accurately examine these outcomes. To address these limitations, there is a need for longitudinal mental health survey research with more detailed assessment of DRTEs, perceived threat during exposure to DRTEs, and temporal information about the onset of mental disorders, DRTEs, and suicidal behaviour.
Clinical and Policy Implications
This study adds important new information on the relationship between deployment and DRTEs and suicidal behaviour. Although deployment itself is not associated with suicidal behaviour, increasing levels of exposure of DRTEs is associated with suicidal behaviour. Predeployment resilience training strategies that improve the capacity of military personnel to face DRTEs may reduce suicidal behaviour. Cognitive processing therapy and prolonged exposure therapy have been shown to be effective in reducing acute stress disorder symptoms 41 and PTSD symptoms. 42 Conceptually, these psychological interventions could be adapted for use during the deployment phase. However, there is no strong, empirical literature to support overall resilience training 43 or predeployment resilience training. 44 We suggest that early recognition of exposure to DRTEs during and after deployment may reduce the risk of postdeployment mental disorders and suicidal behaviour.
Conclusions
Serving military personnel exposed to increasing number of types of DRTEs are at increased risk for SI, SP, and SA. There is also variability of the relationship between some individual DRTEs and the risk for suicidal behaviour. These findings suggest the potential importance of early recognition and treatment of military personnel exposed to high levels of DRTEs and postdeployment mental disorders. Indeed, the Canadian Armed Forces has educational and screening programs that assess both deployment-related trauma and mental disorders in place for that very reason.
Footnotes
Acknowledgements
Statistics Canada collected and provided the data for academic purposes, but the analyses are the sole responsibility of the authors. The opinions expressed do not represent the views of the Department of National Defence (Canada), the Canadian Armed Forces, or Statistics Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the Government of Canada and a CIHR Foundation Grant 333252 (Sareen).