
Abstract
Objective:
This study prospectively examined maternal biopsychosocial predictors of recovery from comorbid depression and anxiety from 25 weeks’ gestation to 6 years postbirth. Specifically, the study investigated the influence of 1) maternal factors and 2) the child’s behaviours and physical health on the course of the mother’s depressed mood and anxiety.
Methods:
Eighty-six women diagnosed with antenatal depression/anxiety were recruited through the Reproductive Mental Health Program and family practices in Vancouver. Based on the trajectory and status of their symptom remission, participants were categorised into 3 groups: full recovery, partial recovery, and no recovery. The following measures were completed over 6 years: Hamilton Anxiety Rating Scale (HAM-A) and Hamilton Depression Rating Scale (HAM-D) at baseline; Parental Stress Index (PSI) added at 6 months postpartum; Beck Anxiety Inventory (BAI), Beck Depression Inventory II (BDI-II), and Child Behavior Checklist (CBCL) at 3 years postbirth; and HAM-A, HAM-D, MacArthur Health and Behavior Questionnaire (HBQ-P), and PSI at 6 years postbirth.
Results:
Factors that predicted full recovery from depression included the absence of maternal health concerns, low total parental stress, and few child behavioural issues, whereas low levels of spousal stress were a significant factor in achieving full recovery from anxiety.
Conclusion:
A variety of maternal and child-related factors govern full recovery or sustained remission of depression/anxiety in the postpartum up to 6 years postbirth. Early awareness of these predictors could lead to timely interventions, ensuring long-term maternal-child well-being.
Postpartum depression (PPD) is a serious mental health condition that affects new mothers all over the world. Studies show that in developed countries, approximately 10% to 15% of women suffer from PPD after childbirth. 1 Twenty to 60% of these mothers experience comorbid anxiety. 2 –4 These complex disorders have been shown to negatively affect maternal functioning and have detrimental, long-lasting effects on the child’s behaviour and physical health. 5 Specific consequences for the offspring include disturbed social interactions, greater externalising behaviours as children, and increased vulnerability to mental illness as adolescents. 6 Early symptom identification and intervention are essential in ensuring optimal maternal-child well-being. Pharmacotherapy is recommended for moderate to severe postpartum mood/anxiety disorders while psychotherapy is indicated for mild illness. 7,8 Not all women attain full symptom recovery 7 despite timely diagnosis and judicious treatment. 9 To understand this differential treatment response, it is imperative to identify the specific predictors that assist in maintaining sustained remission or full recovery.
To date, most studies have investigated factors that predict PPD; a few have examined predictors of postpartum anxiety; limited knowledge exists on predictive factors that influence comorbid depression/anxiety. 9 A history of psychopathology and psychological distress during pregnancy, 10 low social support, poor marital relationship, 11 and low household income 10 appear to be key factors predicting PPD. Similarly, low maternal education, history of depressed mood, and increased peripartum stress 12 are associated with postpartum anxiety. Understanding potential risk factors associated with comorbid illness helps clinicians predict recovery by screening and identifying mothers at risk. Research is urgently needed in this specific area to prevent the chronicity and functional impairment associated with incomplete recovery.
The current study was undertaken to prospectively investigate the course of a woman’s depressive/anxiety symptoms over a 6-year period postbirth and to determine maternal and child predictors associated with symptom recovery. We expected 1) that maternal and child-related factors would be identified and 2) that these factors would predict both positive and negative trajectories for maternal mood disturbances during postpartum and beyond. Understanding these determinants could lead to the development of a decision-making model that predicts recovery.
Methods
Participants
In this longitudinal cohort study, women were recruited during their second/third trimester of pregnancy from a tertiary care program in Vancouver, British Columbia. Ethics approval was received by University of British Columbia Research Ethics Board and the Children’s and Women’s Health Centre of British Columbia Research Review Committee. Inclusion criteria were as follows: fluent in English, aged 18 to 45 years, physically healthy, diagnosis of comorbid anxiety and depression, and having scores ≥8 on both the Hamilton Anxiety Rating Scale (HAM-A) and Hamilton Depression Rating Scale (HAM-D) either with or without antidepressant treatment. Eligible diagnoses for anxiety: generalised anxiety disorder, panic disorder, obsessive-compulsive disorder, and specific phobia. Eligible diagnoses for depression: major depressive disorder and dysthymia. Exclusion criteria: substance abuse, psychosis, and suicidality. A nurse clinician screened patients (n = 191) for study entry, and the study psychiatrist confirmed diagnosis using HAM-A/HAM-D and by performing a semistructured clinical interview following Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) criteria. A research assistant informed eligible patients about study details and received written informed consent. A total of 110 patients were eligible; 86 completed the study. Patients were followed from their second/third trimester of pregnancy to 6 years postbirth. Reasons for dropout included lost to follow-up, changed mind about study, difficulty attending appointments, and lack of partner support.
Procedure
Following participant consent, women were asked to complete the following forms, validated questionnaires, and rating scales at 4 study visits: Visit 1 (second/third trimester of pregnancy, 25 to 35 weeks’ gestation): HAM-A, HAM-D, and sociodemographic and maternal medical information Visit 2 (6 months postpartum): HAM-A, HAM-D, and Parental Stress Index - Short Form (PSI-SF) Visit 3 (3 years postbirth): At this visit, we used a self-report scale as it was more practical to implement during this 6-year prospective design and would accurately reflect what would occur in clinical practice. Beck Anxiety Inventory (BAI), Beck Depression Inventory II (BDI-II), and Child Behavior Checklist (CBCL). Visit 4 (6 years postbirth): HAM-A, HAM-D, MacArthur Health and Behavior Questionnaire, maternal report (HBQ-P), and Parental Stress Index - Full Length (PSI-FL)
These time points were chosen to capture each phase in the child’s life: infant (6 months postpartum), toddler (3 years postbirth), and school-age child (6 years postbirth).
Study Design
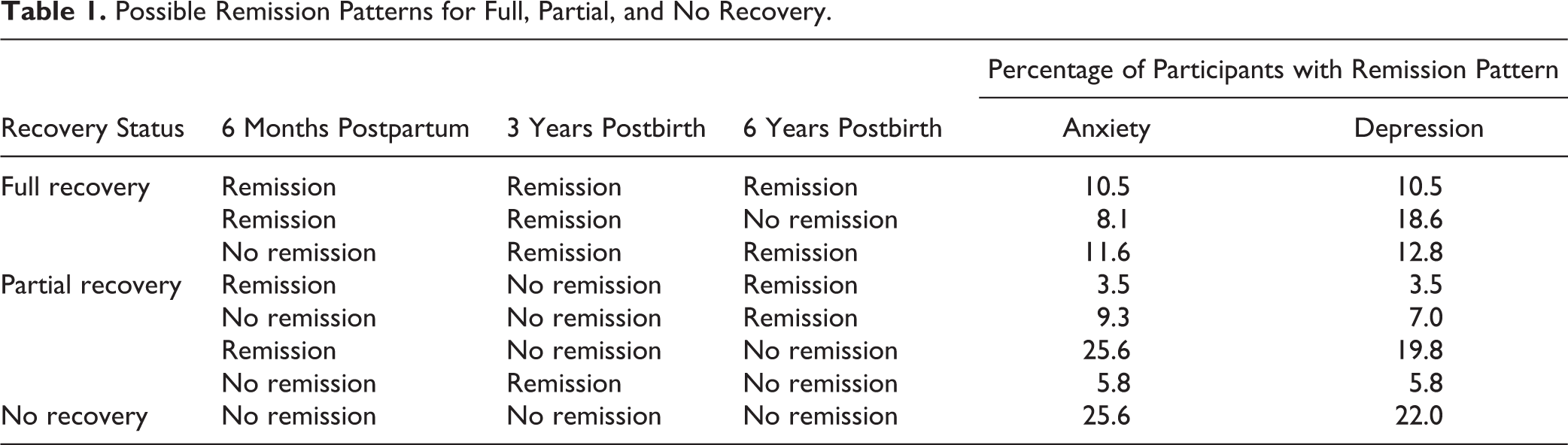
Clinical remission was defined as scores indicating no/minimal depressive or anxiety symptoms at a particular study visit (HAM-D ≤7 and BDI ≤13; HAM-A ≤7 and BAI ≤9). Participants were categorised into 3 groups based on their symptom remission of anxiety and depression over 6 years: full recovery, partial recovery, and no recovery. Full recovery was defined as remissive states at a minimum of 2 consecutive postbirth study visits. No recovery was defined as an absence of remissive states at any of the postbirth study visits. Last, partial recovery was defined as remissive states at 1 or 2 nonconsecutive postbirth visits (see Table 1 for possible remission patterns).
Possible Remission Patterns for Full, Partial, and No Recovery.
Study Variables and Measures
Depression
Two clinical rating scales were used to assess depression, HAM-D and BDI-II. HAM-D is a 21-item clinician-administered depression severity scale defined by a series of symptoms and measures for both psychological and somatic depression. 13 Depression scores from 0 to 7 indicate no/minimal symptoms, 8 to 17 suggest mild depression, 18 to 24 indicate moderate depression, and scores >25 are associated with severe depression. Interrater reliability ranges from 0.84 to 0.90.
BDI-II is a 21-item self-report, multiple-choice questionnaire that measures characteristic attitudes and depression symptoms. Scores ranging from 0 to 13 indicate minimal depression, 14 to 19 indicate mild depression, 20 to 28 suggest moderate depression, and scores >28 are associated with severe depression. The BDI-II has a reliability of α = 0.92.
Anxiety
HAM-A and BAI were used to measure anxiety symptoms. HAM-A is a 14-item clinician-administered anxiety severity scale defined by a series of symptoms and measures for both psychological and somatic anxiety. 13 Scores ranging from 0 to 7 indicate no/minimal anxiety, 8 to 14 suggest mild anxiety, 15 to 23 indicate moderate anxiety, and scores >24 are associated with severe anxiety. Average interrater reliability is 0.89.
BAI is a 21-item self-report, multiple-choice questionnaire that measures the severity of anxiety and describes its emotional, physiological, and cognitive symptoms. 14 Scores from 0 to 9 indicate minimal anxiety, 10 to 16 suggest mild anxiety, 17 to 29 are associated with moderate anxiety, and scores >29 suggest severe anxiety. Internal consistency is 0.92.
Selective serotonin reuptake inhibitor exposure
Information on participants’ selective serotonin reuptake inhibitor (SSRI) treatment at each study visit was obtained from interviews.
Obstetric, gynecologic, and pregnancy data
Type of delivery, birthweight, baby’s sex, and gestational age at birth were obtained from patients. Parity, gravidity, and number of miscarriages were noted.
History of illness
History and family history of psychiatric illness was obtained by the study psychiatrist at the baseline visit. Maternal health problems were collected from self-report.
Parental stress
The PSI is a validated questionnaire that measures the extent of stress experienced by parents. The PSI-FL has 101 items, and the PSI-SF has 36 items. PSI-SF and PSI-FL were used at 6 months postpartum and 6 years postbirth, respectively. Higher PSI scores indicate that parents are experiencing higher levels of stress in their role. 15
Child health and behaviour
The CBCL is a 100-item checklist completed by parents to detect emotional and behavioural problems in children between 1.5 and 5 years. 16 The CBCL gives a total problem score, externalising and internalising scores, and subscale scores. It has shown to have high test-retest reliability (r = 0.85). 16
Measures of child health were obtained from the MacArthur Health and Behavior Questionnaire, maternal report (HBQ-P). 17,18 The HBQ-P is a 175-item questionnaire completed by parents to gather information on their 4- to 8-year-old child’s mental health symptoms, physical health, and social and school functioning. The HBQ-P has strong psychometric properties. 19 –21
Sociodemographic variables
Sociodemographic variables included maternal years of education, age, and marital status.
Statistical Analysis
Descriptive statistics were calculated and compiled for all variables. Potential predictors of membership in the full- and partial-recovery groups for both depression/anxiety were investigated at the bivariate level for inclusion in multivariate prediction models. All predictive models were examined using logistic regression. The full- and partial-recovery groups were compared to the no-recovery groups for both anxiety and depression separately. Variables with a significance of <0.10 were included for analysis in the multivariate prediction model. Imputation using predictive mean matching was performed for variables that had less than 5% of data missing. Variables with a significance of <0.05 were said to show statistical significance in the multivariate model. Analyses were preformed using SPSS version 15.0. 22
Results
Sample Characteristics of Participants with Comorbid Symptoms
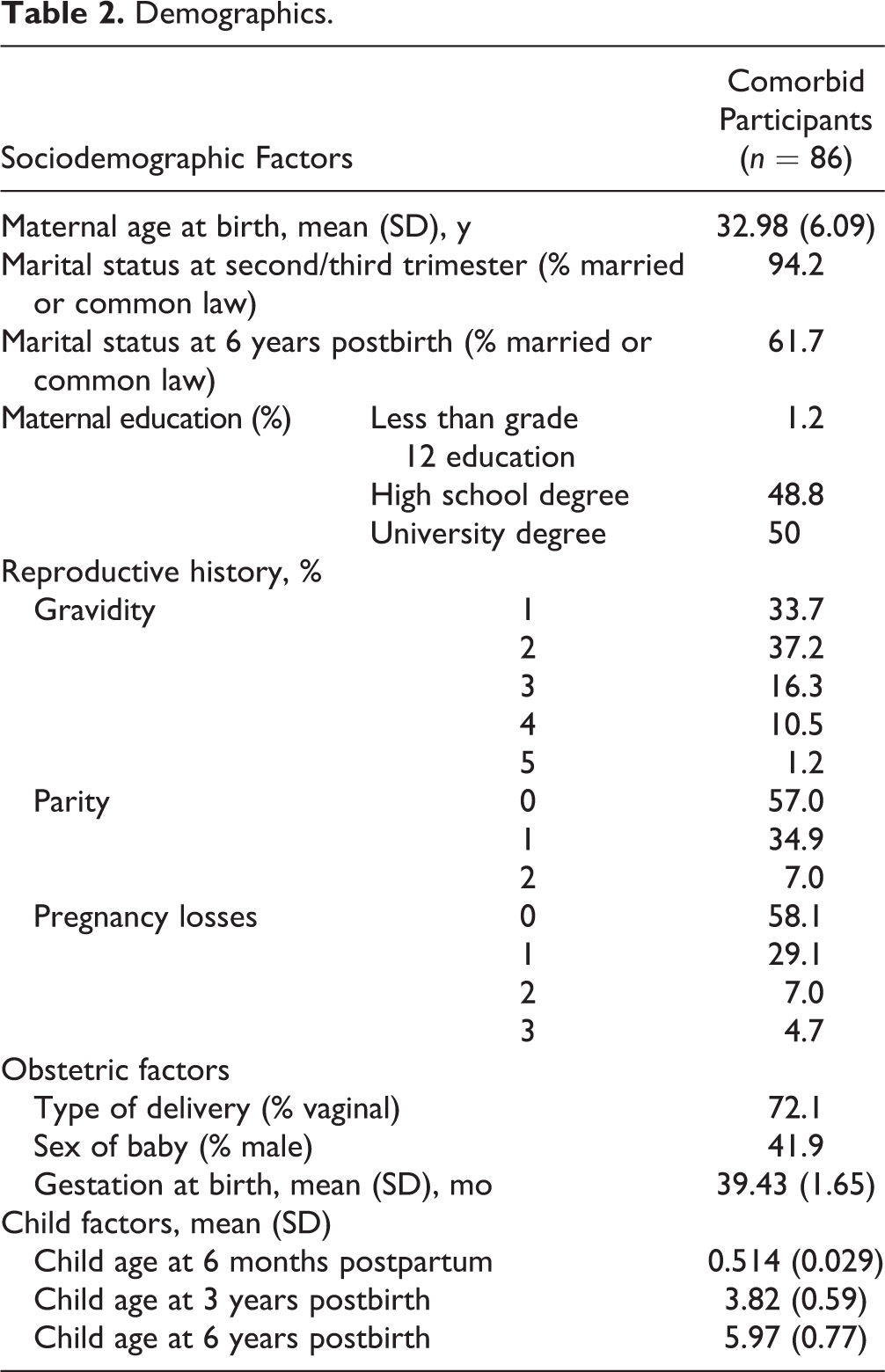
Women were 32.98 years old (standard deviation [SD], 6.09), and most had at least completed high school (98.8%). On average, their newborn’s gestation at birth was 39.43 weeks (SD, 1.65). Most women had vaginal delivery (72.1%). At baseline, 81 women (94.2%) were married or common law, and over the course of the 6-year study, 53 women (61.7%) had this marital status. Thirty-five women (40.8%) had at least 1 miscarriage previously, and for 57.0% of women, the child born during this study was her first child (see Table 2).
Demographics.
The following are our findings for recovery from anxiety symptoms: 26 achieved full recovery, 38 were in partial recovery, and 22 did not recover. With respect to recovery from depressive symptoms, 36 were in full recovery, 31 achieved partial recovery, and 19 participants did not recover. Of the 86 participants in the study, 19 achieved full recovery from both anxiety and depressive symptoms, another 19 participants were in partial recovery from both illnesses, and a total of 10 participants did not recover from either depressive or anxiety symptoms.
Pre- and Postbirth Treatment with SSRIs
Antidepressant treatment was determined at 4 study visits that spanned prenatal and postbirth time points. The following is the percentage of participants taking an SSRI: second/third trimester, 60.5%; 6 months postpartum, 54.7%; 3 years postbirth, 44.2%; and 6 years postbirth, 32.6%. SSRI treatment at 6 months postpartum significantly predicted recovery from anxiety symptoms (P = 0.012) at the bivariate level. When this variable was included in the multivariate model, it did not predict full recovery from anxiety symptoms. Table 3 shows anxiety and depression scores for women with and without SSRI exposure.
Anxiety and Depression Scores Based on SSRI Exposure over Study Period.
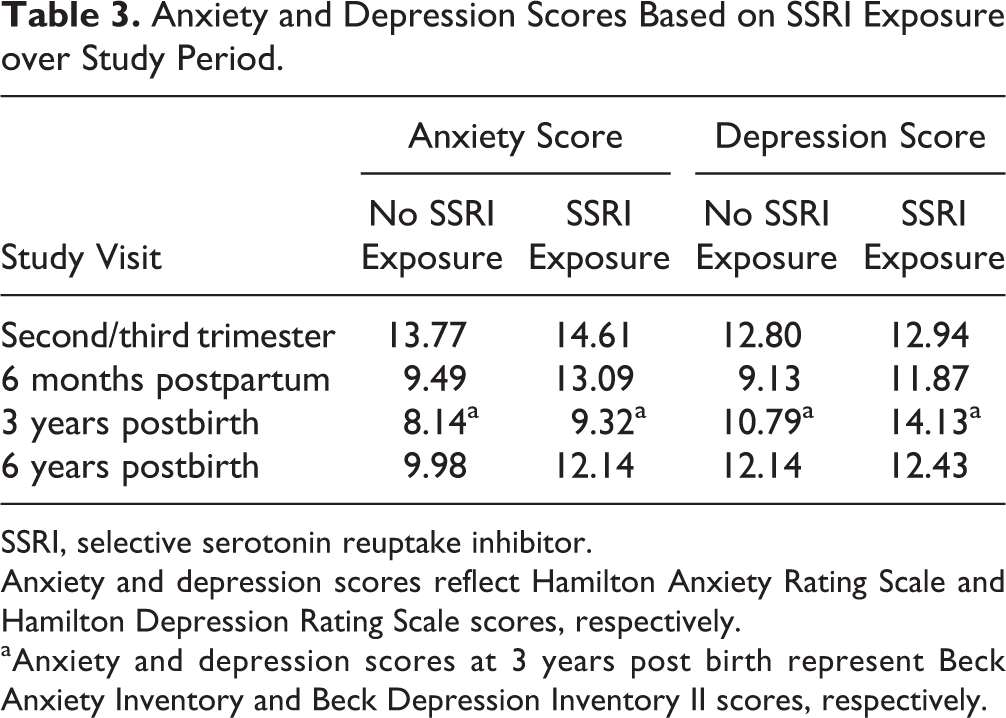
SSRI, selective serotonin reuptake inhibitor.
Anxiety and depression scores reflect Hamilton Anxiety Rating Scale and Hamilton Depression Rating Scale scores, respectively.
aAnxiety and depression scores at 3 years post birth represent Beck Anxiety Inventory and Beck Depression Inventory II scores, respectively.
Bivariate Predictors of Change
Bivariate logistic regression was performed to highlight predictors that play a statistically significant role in a woman being in the full/partial-recovery groups compared to the no-recovery groups.
Child’s externalising and internalising behaviours at 3 years postbirth, child’s chronic medical conditions over 6 years postbirth, total parental stress at 6 months postpartum, spousal stress, and maternal health problems over 6 years postbirth were significant at the 0.10 cutoff for predicting full recovery from depression.
Maternal health problems and a child’s chronic medical conditions over 6 years postbirth were significant at the 0.10 cutoff for predicting partial recovery from depression.
Absence of history of depression and anxiety, absence of family history of anxiety, and low spousal stress at 6 years postbirth were significant at the 0.10 cutoff for predicting full recovery from anxiety.
Absence of family history of anxiety and low levels of spousal stress at 6 years postbirth were significant at the 0.10 cutoff for predicting partial recovery from anxiety.
Multivariate Predictors of Change
Depression
Multivariate logistic regression was performed to test potential predictors of a woman being in the full- or partial-depression recovery groups compared to the no-depression recovery group. For depression, 4 variables were significant at α = 0.05 controlling for the other significant bivariate predictors. Table 4 outlines the factors significant in predicting full and partial recovery from depression.
Factors Predicting Full and Partial Recovery from Depression and Anxiety: Multivariate Model Results.
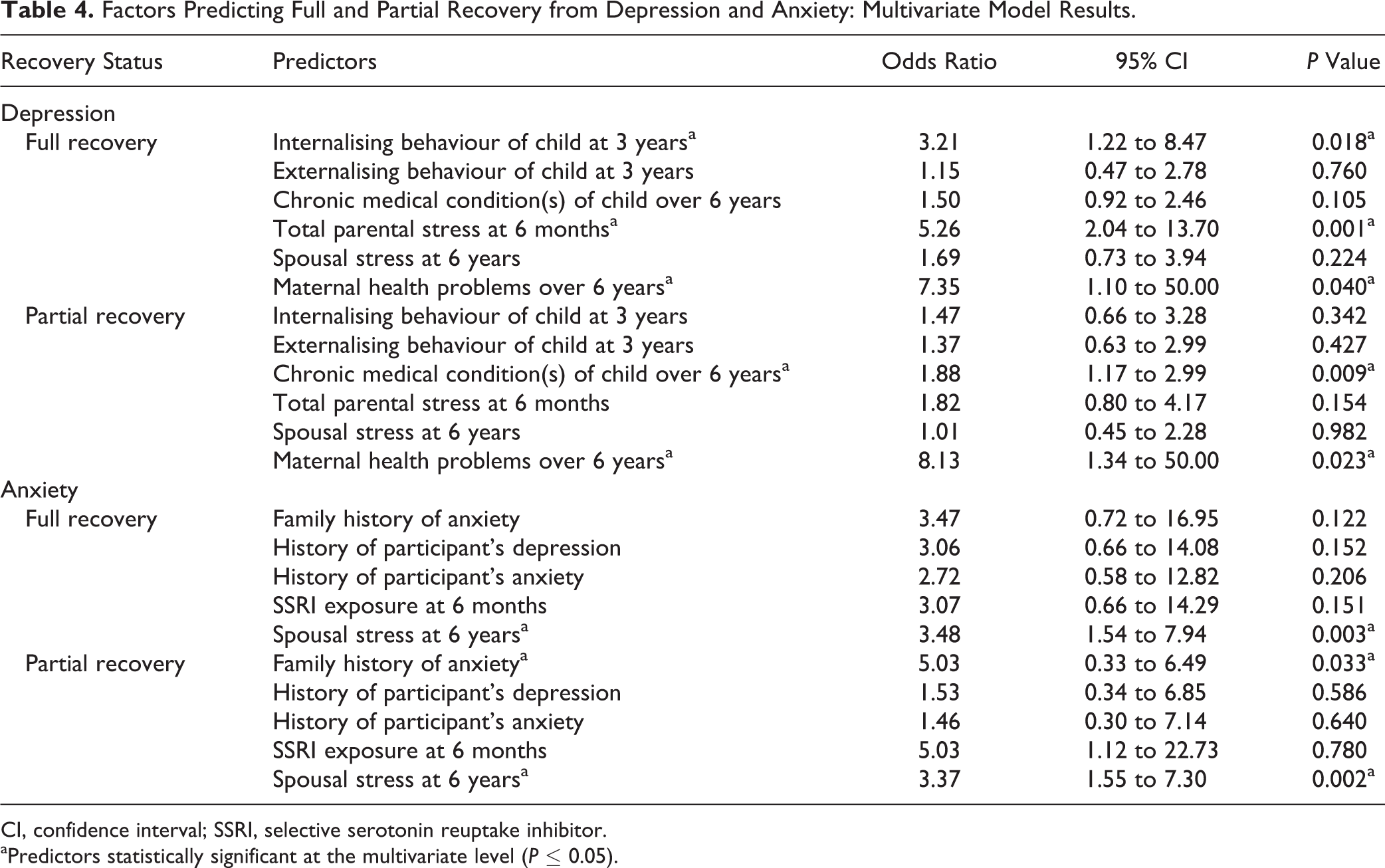
CI, confidence interval; SSRI, selective serotonin reuptake inhibitor.
aPredictors statistically significant at the multivariate level (P ≤ 0.05).
1. Maternal Predictors
Women in this study had a 5.26 times greater chance to fully recover from their depressive symptoms if they had low total parental stress at 6 months postpartum (odds ratio [OR], 5.26; 95% confidence interval [CI], 2.04 to 13.70; P = 0.001). Study participants who did not have any health problems over 6 years postbirth were 7.35 times more likely to achieve full recovery (OR, 7.35; 95% CI, 1.10 to 50.00; P = 0.04) and partial recovery (OR, 8.13; 95% CI, 1.34 to 50.00; P = 0.023) from their depression.
2. Child-Related Predictors
Women in this study were 3.21 times more likely to achieve full recovery from depression over 6 years if their child had low levels of internalising behaviours at 3 years postbirth (OR, 3.21; 95% CI, 1.22 to 8.47; P = 0.018). They were also more likely to achieve partial recovery from depression if their child had fewer chronic medical conditions at 6 years postbirth (OR, 1.88; 95% CI, 1.17 to 2.99; P = 0.009).
Anxiety
Multivariate logistic regression was also used to test predictors of membership in the full- or partial-anxiety recovery groups compared to the no-anxiety recovery group. For anxiety, 3 variables had a significance of 0.05 or below at the multivariate level controlling for the other significant bivariate predictors. Table 4 outlines the factors significant in predicting recovery from anxiety.
3. Maternal Predictors
Women were more likely to be in the full-anxiety recovery group or the partial-anxiety recovery group if they had low spousal stress at 6 years postbirth (OR, 3.48; 95% CI, 1.54 to 7.94; P = 0.003 for full recovery; OR, 3.37; 95% CI, 1.55 to 7.30; P = 0.002 for partial recovery). Study women with an absence of family history of anxiety had a 5.03 times greater chance of being in the partial-recovery group (OR, 5.03; 95% CI, 0.33 to 6.49; P = 0.033).
4. Child-Related Predictors
No child predictors were significantly associated with women achieving either full or partial recovery from anxiety at either the bivariate or multivariate levels (P > 0.05).
Discussion
Our study identified predictors of sustained remission or full recovery from depression/anxiety after childbirth over a 6-year period. We found that low total parental stress at 6 months postpartum, few child internalising behaviours at 3 years postbirth, and an absence of maternal health concerns at 6 years postbirth were significant factors in predicting full recovery from depression over 6 years postbirth. Few chronic medical conditions in the child and absence of maternal health problems predicted partial recovery from depression. With regards to anxiety, low levels of spousal stress at 6 years postbirth was a key predictor of full and partial recovery from anxiety. Absence of family history of anxiety was found to be significant in predicting partial recovery from anxiety. It is important to note that SSRI treatment during pregnancy and postbirth was not a significant predictor of recovery from anxiety/depressive symptoms. However, antidepressant treatment at 6 months postpartum showed significance only at the bivariate level in predicting full recovery from anxiety.
Predicting the course of PPD and anxiety helps assess remission and recovery. This, in turn, helps clinicians plan appropriate interventions. It is important to understand that the common definitions for remission and recovery are based on validated diagnostic scales. 23 Remission has been defined as no/minimal symptoms at a specific moment in time, whereas recovery captures extended or sustained remission. 24 Many researchers suggest that achieving full recovery should be the primary goal of treatment. 25,26 Full recovery has 2 components: symptom improvement and full restoration of functionality. 23 Our study focused on symptom recovery.
In contrast to previous research approaches, participants in this study were categorised into 3 groups based on the course of their symptom remission over 6 years instead of SSRI exposure. 27 We found SSRI treatment, whether it was prenatal or postnatal, was not a predictor of recovery. At visit 1, most women were receiving SSRIs in pregnancy (n = 52), but by the last study visit, only 28 mothers were still on antidepressants. Although pharmacotherapy is often recommended for moderate to severe postpartum mood and anxiety disorders, not all women opt for this treatment modality. Misri et al. 28 suggest that women’s perception of risk associated with pharmacotherapy influences adherence to treatment. Clinicians often hesitate to prescribe antidepressants for breastfeeding mothers due to fear of medication exposure. 29 As a result, clinicians face the dilemma of balancing the overall risk of the illness versus medication exposure to the newborn. 29 Identifying predictors could potentially assist in developing early and appropriate interventions.
In the current study, mothers who had absence of health problems over 6 years postbirth showed an increased chance of achieving both full and partial recovery from depression, compared to mothers who had 1 or more health problems. The connection between long-term maternal physical illness and its impact on mental health has received limited scientific attention. Woolhouse et al., 30 investigating relationships between maternal physical issues and depressive symptoms in the first postpartum year, reported that the prevalence of clinically relevant depressive symptoms increased from 1.9% for women reporting 0 to 2 physical health problems to 11.1% among those with more than 4 health problems. 30 Our findings highlight links between physical illness and depressive symptoms beyond the first year postpartum and offer an important insight into ensuring mental stability by focusing on maintaining physical wellness.
In the present study, mothers reporting lower levels of parenting stress at 6 months postpartum had an increased likelihood of achieving full recovery from depression compared to those reporting higher levels. Parental stress represents the overall level of perceived stress and comprises parental distress, parent-child dysfunctional interaction, and difficult child. 15 Venkatesh et al. 31 found that mothers with higher levels of stress are more likely to have lower levels of self-efficacy and higher levels of anxiety, predisposing them to PPD. Studies have also found the reverse relationship between antenatal depression/anxiety and increased maternal postpartum parenting stress. 27,32 Our findings are consistent with previous reports revealing relationships between parental stress and maternal mood. Studies show psychotherapy 33 and interaction coaching for mothers to be effective in managing parental stress postbirth. 32
Our study reported that a mother has an increased likelihood of achieving full recovery if her child has low levels of internalising behaviours (i.e., emotional reactivity, depression, anxiety, irritability, and withdrawal) at 3 years postbirth. Many studies have found a relationship between PPD and child behaviour. Turney 34 found that mothers with higher levels of depressive symptoms reported more internalising behaviours in their children compared to mothers without. Another study suggested that toddlers exposed to chronic PPD had higher levels of parent-reported behaviour problems. Our finding that low levels of internalising behaviours in a child predict sustained remission adds new knowledge to the existent literature.
We found that mothers who had children with fewer chronic health problems over 6 years postbirth had an increased chance of achieving partial recovery from depression. This is not entirely unexpected given previous studies showing that poor child health can cause maternal distress. 35 To date, no studies have investigated links between a child’s chronic health and its impact on a mother’s recovery from PPD.
The role of spousal stress on recovery from depression and anxiety was also investigated in this study. We found low levels of spousal stress at 6 years postbirth showed full as well as partial recovery from anxiety symptoms. Studies to date have focussed on maternal depression and marital instability. Higher relationship quality appears to be associated with significantly lower odds of depression. 36 Our finding, which links maternal anxiety with spousal stress, underscores the role of partner counselling as an integral part of the intervention postbirth.
In our study, absence of family history of anxiety appeared to play a role in predicting partial recovery from postpartum anxiety but not depression. While the mechanism underlying this association remains unclear, previous research has reported a highly significant relationship between a positive family history of depression and PPD. 37 Studies suggest that patients with a positive family history of depression are more likely to experience early onset depression, increased symptom severity, longer depressive episodes, 38 more Axis I comorbidities (anxiety), 39 and incomplete recovery, 40 pointing to genetic or environmental factors.
We found that mothers’ history of anxiety/depression was not found to be significant in predicting recovery from anxiety/depressive symptoms, contrary to what was expected. Earlier studies found that prior psychiatric illness predicted treatment outcomes in postpartum depressed/anxious women. 41,42 Our findings, which are different, could be due to underreporting of psychiatric history by mothers during their initial assessment. Due to fear of stigma, acceptance of psychiatric illness after a baby’s birth can be distressing and shameful. There is also a possibility that some participants who had a history of depression/anxiety presented with severe illness and subsequently dropped out of the study and were lost to follow-up. These factors could account for the lack of statistical significance in our study.
A number of limitations need mention. The maternal health concerns measure was dichotomous in nature; this could be improved by having more than 2 outcomes in this variable to better understand how the degree of health concerns influences recovery from depression/anxiety. To fully capture all dimensions of recovery, remission along with functional improvement could be measured over time.
Conclusion
Our study findings reveal that absence of maternal health problems, low parental stress, and few child internalising behavioural issues predicted full recovery from depressive symptoms in the mother after childbirth and over a 6-year period. In addition, we found that low levels of spousal stress predicted full recovery from anxiety symptoms over a similar time period. Interestingly, treatment with an SSRI prenatally or postbirth did not predict the clinical course of the disease. Identifying predictors involved in recovery from comorbid psychiatric illness can guide clinicians in planning appropriate and timely interventions. More longitudinal research examining a broader range of predictors is needed, with the ultimate goal being restoration of full functionality and maternal/child wellness.
Footnotes
Author Note
This article was presented as a poster presentation at the University of British Columbia, Annual Department of Psychiatry Research Day, Vancouver, BC, 2016 May 26.
Acknowledgements
We are grateful to Dr. Michael Papsdorf, who assisted with the statistical analysis. We also thank the mothers and children who participated in our research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the following research grants awarded to Dr. Oberlander: MOP 54490 and 57837 from the Canadian Institutes of Health Research and 12-FYO1-30 from the March of Dimes Foundation.