
Abstract
Background:
Six recent randomised control trials (RCTs) have suggested that supervised injectable heroin (SIH) can be effective in patients who persist in street heroin use during methadone treatment. However, short-term randomised control trials have limitations in assessing the effectiveness of treatments for addictive disorders, which are chronic and relapsing disorders of motivation. These RCTs particularly fail to capture the process of the SIH treatment and the diversity of influence and change over time.
Method:
This narrative review is based on the analysis of published data. Conclusions are drawn from a process of reflection informed by experience in delivering one of the published trials, subsequent experiences in varying the way SIH is delivered, and through consideration of possible mechanisms of action of SIH.
Observations:
Many long-term, socially marginalised and demoralised people who are addicted to heroin experience few rewards from the stability afforded by methadone treatment. Supervised injected heroin is sufficiently reinforcing for many of these individuals to attend daily and participate in highly structured treatment. With an adequate daily dose of supervised methadone to avoid withdrawal dysphoria, occasional diamorphine injections—not necessarily twice daily, or even every day—is enough to hold people in treatment. Participation was associated with reduced amounts of non-prescribed drug use, a gradual change in self-image and attitude, and for some subjects, a movement towards social reintegration and eventual withdrawal from SIH.
Conclusions:
Prescribed heroin is sufficiently motivating to hold a proportion of recidivist addicts in long-term treatment. Participation in structured treatment provides respite from compulsive drug use, and a proportion of subjects develop sufficient rewards from social reintegration to successfully withdraw from treatment. Such change, when it occurs, is slow and stuttering.
Introduction
Following the rapid rise in heroin addiction in many Western countries in the 1990s, there was renewed interest in prescribing diamorphine (pharmaceutical heroin) as a way to ameliorate the devastating effects of heroin addiction. Randomised controlled trials (RCTs) comparing the effectiveness of Supervised Injectable Heroin (SIH) to oral methadone were undertaken in Switzerland, 1 the Netherlands, 2 Spain, 3 Germany, 4,5 the UK 6 and Canada. 7 A meta-analysis of the 6 RCTs concluded that, among people who had failed to respond to methadone treatment, SIH was more effective than methadone in suppressing street heroin use. 8
In general, these positive findings have not persuaded policy makers to support many existing programs or roll-out the treatment more widely. 9 This is not surprising. The finding that people prescribed high-dose pharmaceutical heroin used less street heroin is not a strong argument that treatment is effective (or even that SIH is “treatment” at all). Most observers would require improvements in health, quality of life, and social reintegration to accept that a treatment is worthwhile. However, in comparing SIH with oral methadone treatment, it is not possible to blind either participants or staff to the treatment allocation, and self-reported mood, quality of life and social functioning are susceptible to bias, compromising the value of self-report. Even before the RCTs were conducted, it was assumed that prescribing SIH is motivational, attracting participation by offering access to their drug of choice, and it was anticipated that subjects randomised to the control group might be more likely to drop out or experience resentful demoralisation, which would make meaningful evaluation difficult. 10
This was confirmed in some of the RCTs. For example, in the German trial, 31% of control subjects dropped out early, compared with 2% of those randomised to SIH; thereafter, retention was almost identical in the 2 groups (p57). 4 In addition, the greatest self-reported improvements on the Global Severity Index of the SCL-90 occurred while subjects awaited group allocation and receipt of the first dose of medication (p80). 4 Clearly, such an improvement cannot be attributed to the effects of heroin as medication.
Retention data from the German trial suggest that, in addition to subject disappointment, staff attitudes may have been another source of bias. Retention in the heroin arm was broadly comparable across 6 locations in the German study, ranging from 59% to 85% (mean, 67%) retained at 12 months. However, methadone retention differed widely, from 21% retained in one centre to more than 80% in another. The investigators commented that one clinic “managed to maintain the attractiveness of methadone treatment” (p58). 4 Treatment works better when staff believe in it, 11 and it is possible that staff in some centres were enthusiastic about diamorphine treatment and felt that subjects in the control condition had missed out, and this may have contributed to the higher drop-out rates. These findings support the suggestion that rules of evidence designed to test the effectiveness of medications may be inappropriate when assessing complex interventions for the motivational disorder of addiction. 12
Recent research on psychological and self-help approaches to addiction have moved from searching for evidence that interventions “work” to asking questions of the mechanisms by which they contribute to change, and for which individuals and in what contexts different treatments can be helpful. 13,14 This more nuanced approach seems better suited to assessing SIH as a form of treatment than is undertaking clinical trials comparing SIH to a treatment known to have previously failed in the target population.
This paper is based on our experience of delivering SIH, first as a research trial, and then for several years as a clinical service. The paper explores the mechanisms of action of SIH, and proposes that the reported evidence from RCTs, showing better results from SIH than from oral methadone, may actually understate the effectiveness of this modality of treatment for many participants. The paper reviews aspects of the clinical trials that shed light on how prescribed heroin works, and uses clinical experience to suggest how supervised injectable heroin can contribute to recovery from addiction.
Evidence from Published Trials
Did Prescribed Injectable Heroin Attract and Retain in Treatment Otherwise Hard to Engage Heroin Users?
Despite confirmation that participants who enrolled in the trials were seeking diamorphine, and tended to drop out if randomised to methadone, SIH trials struggled to attract participants into treatment. Far from being a “honey pot” to draw in people who wanted heroin, the Swiss, German, Spanish, the UK and North American trials all reported recruitment problems, and needed to extend the period of recruitment and (or) failed to reach target numbers. Likewise, SIH trials failed to attract new, previously “unreached” people to treatment; in the German study, one arm of the trial set out to recruit people not currently in treatment, but only 3% of recruits had no prior treatment history. 4
Did SIH Reduce the Use of Non-prescribed Drugs?
Attracting and retaining participation in treatment is not in itself a positive outcome; 10 at best, retention is a proxy measure of outcome. The critical outcome is a reduction in the use of non-prescribed drugs, as reduction in street drug use is generally a prerequisite to improving physical and mental health and restoring impaired social role. 15 Evidence from all clinical trials was consistent: prescribed, high-dose pharmaceutical heroin helped subjects reduce or cease their use of street heroin. 8 However, the results of the 6 RCTs found little difference in cocaine and other street drug use between SIH and control subjects. Such drug use compromises the effectiveness of treatment in promoting social reintegration.
Does SIH Facilitate Social Integration?
Waldorf and Biernacki 16 refer to the ‘inter-world’ inhabited by a heroin user in treatment as no longer part of the drug scene but not part of mainstream society either. Many SIH subjects fit that description, ceasing illicit use but not finding any social role or affiliation. In part, this reflects a wider social problem in the UK, and probably in any high income country with a welfare system—the emergence of a long-term unemployed underclass that is supported by welfare but impoverished, demoralised, and often lacking a social role. Achieving stable housing, re-establishing relationships with family, and re-entry into the workforce are changes that contribute to the slow process of consolidation of a non-addict identity. In all trials, there was little evidence of improved social functioning in SIH subjects compared with controls.
However, clinical trials may underestimate the potential effectiveness of SIH. During the trials, subjects on SIH and those on methadone received the same psychosocial support (or, in the case of the German trial, were randomly allocated to 1 of 2 structured programs of psychosocial support). During the trial phase, case workers did not use the motivational salience of SIH to steer subjects away from other drugs. In our clinic, outside of the trial context, we began informing patients that ongoing receipt of SIH was contingent on ceasing benzodiazepine and cocaine use. Some patients were prescribed reducing dosages of benzodiazepine to withdraw safely. Our perception is that the motivational salience of access to prescribed heroin was enough for many patients to cease benzodiazepine and cocaine use, something not tested in the clinical trials.
The Evolution of SIH in the London Clinic
Structured Treatment
SIH is a highly structured treatment, and it became increasingly structured over time at the South London clinic (Table 1). The basic behavioural structure was daily attendance and ritualised administration. During SIH, and for the first months of treatment, patients attended twice daily, 7 days per week. On arrival at the clinic, patients checked in with the receptionist, then sat in the waiting room until called through individually for their dosages. On entering the injecting room, they identified themselves to the 2 nurses, who would verify their identity and visually confirm that the patient was not intoxicated. Nurses drew up the prescribed dose of heroin, while patients washed their hands thoroughly, then swabbed down the proposed injecting site. Nurses then passed the loaded syringe to the patient to inject themselves. Following injection, patients then disposed of the used equipment, swabbed down all surfaces, and spoke briefly with nurses to confirm that they were not intoxicated. Once daily, patients were given a dose of oral methadone, taken under observation. Patients then left the clinic. Urine toxicology was performed about fortnightly, on a day chosen at random.
Timeline of SIH in the UK
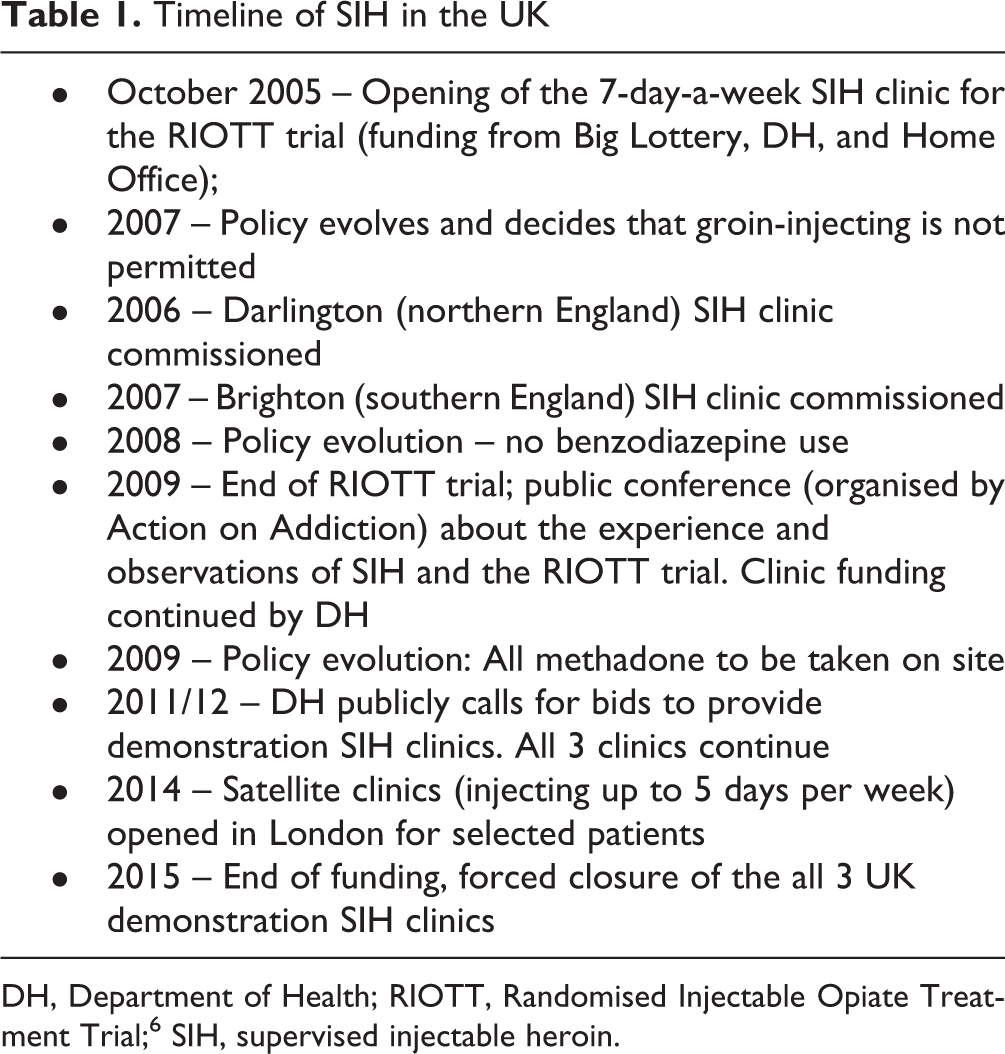
DH, Department of Health; RIOTT, Randomised Injectable Opiate Treatment Trial; 6 SIH, supervised injectable heroin.
Clinic policies, designed and progressively revised to minimize risks, formed the core of the structure. Our observation was that patients misusing benzodiazepines or alcohol were at increased risk of post-injection hypoxia. They also tended to be more behaviourally chaotic. In patients known to misuse alcohol, a breathalyser was used to confirm that breath alcohol was at an acceptable level prior to receiving heroin. Mortality is increased when benzodiazepines are co-prescribed with opioid substitution treatment 17 or with opioid analgesics, 18 and, over time, the clinic adopted a “no benzodiazepine” policy. Patients who appeared intoxicated would have an on-the-spot urine dipstick test prior to dosing. If they tested positive for benzodiazepines, no injectable drugs would be dispensed, and people would receive oral methadone only on that day.
Rules around injecting were developed to minimize vein damage. Patients were allowed a maximum of 3 attempts to find a vein, and were discouraged from “digging” to find IV access. Groin injecting was not permitted. 19 In practice, most patients moved to injecting intramuscularly. The result was marked improvement in injecting-related abscesses and ulcers, which were common at the initiation of SIH.
The cognitive component of the structure included clear objectives of treatment: reduction and cessation of non-prescribed drug use, attention to physical and mental health, and assistance to promote social reintegration (such as obtaining stable housing, participating in training courses). Patients had fortnightly clinical reviews with key workers, and medical reviews every 3 months or more frequently if there were issues of medical or psychiatric comorbidity.
The Impact of Structure
As noted above, recruitment difficulties were seen in all published trials of SIH, and this emphasizes an important aspect of diamorphine treatment—the ambivalence heroin addicts feel toward structured treatment. From our experience in the South London clinic, most patients missed 2 to 3 appointments before eventually presenting. Before joining the SIH program, most people seeking SIH were homeless, received low doses of methadone, and attended treatment erratically. People with few social supports or without a meaningful social role or identity other than “addict” often saw little meaning in the concept of “recovery” and found little appeal in treatment. 20 Many at presentation were “hopeless”—without hope or expectation that life could be different. Several patients presented in the anticipation of “free heroin”; their continued access to heroin was sufficient motivation to attend and comply with clinic requirements.
Transition in identity and outlook is central to recovery from drug dependence—a process characterized by Marie Nyswander as the transition “from drug addict to patient”. The rituals of daily attendance, compliance with clinic rules about hand washing and vein care, post-injection monitoring, regular urine toxicology, and frequent clinical review; these elements contributed to making heroin injecting a ‘treatment’ rather than access to free drugs. Diamorphine is enough incentive for some people who are dependent on heroin to accept rules and structure. Our observation was that for most (not all) patients, participation in treatment was associated with a gradual change in outlook, attendance and presentation.
Doses
Because of the short half-life of heroin and its active metabolites, subjects in the SIH trials were also provided with oral methadone to avoid the emergence of withdrawal. In the South London clinic, during the RCT, methadone doses were moderate (40 to 60 mg) and were given to take home and consume in the evenings to avoid withdrawal overnight. However, in the post-trial phase of treatment, which ran for 6 years, we experimented with approaches to medication. The critical change was switching from providing methadone to take home, to giving all methadone as supervised, on-site doses.
From the time this policy was introduced, there were no further instances of post-injection respiratory depression requiring intervention over the next 6 years. We assumed that people had sought to increase the effect of diamorphine by omitting all or part of their methadone, keeping tolerance low to experience a greater effect from diamorphine. Following that observation, we implemented a policy of increasing methadone dosages, so that everyone was taking at least 60 mg/day in addition to diamorphine. The intention was to minimize withdrawal dysphoria. Monitoring confirmed that patients on high-dose methadone and diamorphine still experienced a prompt physiological response to the intramuscular injection of heroin, and that tolerance induced by methadone was partial rather than complete. 21
Frequency of Injecting
With an adequate dose of supervised methadone to avoid withdrawal, the role of prescribed heroin was to provide intermittent reward, and this did not always need to be daily. Once stabilised on high-dose heroin—typically, 200 mg twice daily, along with 80 to 100 mg oral methadone—and no longer using street heroin, many patients were happy to reduce the frequency of injecting and reduce the heroin dosage. Several patients initiated the reduction in dosage and frequency within a few months, mostly to free themselves from the requirement to attend the clinic twice daily. Many patients dropped rapidly to 100 mg heroin once daily, sometimes to 100 mg thrice weekly.
Use of Long-acting Medications other than Methadone
Some patients were recruited on the grounds that they were non-responders to methadone. We explored the use of slow-release oral morphine as an alternative. A report of patient responses has been published. 22 A few patients on buprenorphine were also commenced on injectable drugs. They reported a gratifying effect of injecting diamorphine but had poor control of withdrawal when the diamorphine injections wore off, and all were eventually transferred to methadone. For patients on buprenorphine, injectable buprenorphine may warrant consideration in those continuing to inject street drugs.
Summary
Until the 1970s in the UK, prescribing heroin was the most common approach for the treatment of heroin addiction. The rationale for such prescribing was straightforward—it was a humane response to people who found themselves in a predicament. There remains a common assumption that if heroin is wanted, prescribing it under controlled conditions, as a stable dosage, can minimize the damage done by addiction.
To the extent that the problems of people addicted to heroin are merely their addiction to heroin, providing a stable supply may well be the main function of prescribing opioids—whether diamorphine, methadone or buprenorphine—to manage addiction. On occasion, there are individuals who remain high-functioning and socially integrated while maintained on prescribed IV heroin without supervision. 23 However, the challenge facing communities is not the few high-functioning addicts but the larger cohort of demoralised and socially marginalised heroin users who see little benefit in the stability offered by conventional treatments. Recent trials of SIH have targeted these “hard to reach” people: those who are less able to take advantage of the respite from addiction offered by methadone or drug-free treatment. SIH offers these people enough reinforcement to participate in structured treatment. It requires skilled and supported staff, a treatment ethos that focuses on supporting social reintegration.
Structured treatment was necessary to minimize the risks of overdose and diversion; however, it probably also has a therapeutic element. Redefining heroin as medication—ritually administered with an emphasis on safety and hygiene—promoted a change in identity and outlook. Indirect evidence from the RCTs suggest the importance of structure, because participating generally had a beneficial effect, regardless of the group to which subjects were allocated. For example, in the Swiss RCT, more than half the “methadone non-responders” initially randomised to oral methadone did well and declined the option of transferring to diamorphine when the 6 months of randomised treatment was completed; 1 methadone non-responders had become methadone responders. Highly structured treatment and monitoring provided in RCTs may explain why methadone became more effective in this previously refractory group.
Structured methadone treatment produces better outcomes than unstructured treatment. 24 If methadone were delivered in small, well-staffed clinics rather than low-cost, industrial-scale dispensing operations, an uncertain number of “methadone treatment non-responders” might become methadone responders. However, this does not mean there is no place for SIH. There will continue to be people who fail to respond to methadone treatment, and the evidence from RCTs is sufficient: SIH is more effective than optimised methadone treatment for people persisting in heroin use despite treatment. Our hypothesis is that SIH is effective because heroin is one of the few things able to motivate some individuals who have experienced long-term and demoralising social exclusion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JS is a researcher and clinician and has worked with a range of treatment and rehabilitation service providers. He has contributed to the work of various governmental and non-governmental organisations and has been awarded project grant support and (or) honoraria and (or) consultancy funds from the Department of Health, NTA (National Treatment Agency), PHE (Public Health England), Home Office, NICE (National Institute for Health and Clinical Excellence), and EMCDDA (European Monitoring Centre for Drugs and Drug Addiction) as well as research grants from (last 3 years) NIHR (National Institute on Health Research), MRC (Medical Research Council) and Pilgrim Trust. He has also worked with pharmaceutical companies to seek to identify new or improved treatments (including, last 3 years, Martindale, Reckitt-Benkiser, Lundbeck, MundiPharma, Viropharma, Rusan/iGen) and he and his employer (King’s College London) have been awarded honoraria, travel and (or) consultancy funds. His employer (King’s College London) is registering intellectual property on an innovative development in this area with which JS is involved, and JS has been named on a patent registration by a Pharma company as inventor of a potential novel overdose resuscitation product. A fuller account of JS’s interests is given on his personal web-page of the Addictions Department of King’s College London at ![]() .
.
JB has held consultancy agreements with Reckitt-Benckiser, Britannia pharmaceuticals and Martindale Pharma, and was awarded research funds by Reckitt-Benckiser. He was awarded speaker’s and hospitality funds by Indivior, Martindale and Mundipharma.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.