
Abstract
Antipsychotics are necessary for many older adults to treat major mental illnesses or reduce distressing psychiatric symptoms. Current controversy exists over the role of antipsychotics in the management of neuropsychiatric symptoms (NPS) in persons with dementia. Although some NPS may be appropriately and safely treated with antipsychotics, a fine balance must be achieved between the benefits of these medications, which are often modest, and adverse events, which may have significant consequences. Approximately one-third of all persons with dementia are currently prescribed antipsychotic medications, and there is significant variation in the use of antipsychotics across care settings and providers. Reducing the inappropriate or unnecessary use of antipsychotics among persons with dementia has been the focus of increasing attention owing to better awareness of the potential problems associated with these medications. Several approaches can be used to curb the use of antipsychotics among persons with dementia, including policy or regulatory changes, public reporting, and educational outreach. Recently, there has been encouraging evidence of a downward trend in the use of antipsychotics in many long-term care settings, although prescribing rates are still higher than what is likely optimal. Although reducing the inappropriate use of antipsychotics is a complex task, psychiatrists can play an important role via the provision of clinical care and research evidence, contributing to improved care of persons with dementia in Canada and elsewhere.
There are increasing numbers of older adults in Canada, and an aging population will result in a greater proportion of persons with dementia. A doubling of dementia prevalence is anticipated in the future, with more than 1 million persons with dementia living in Canada by 2030. 1 Neuropsychiatric symptoms (NPS), also known as behavioural and psychological symptoms of dementia or responsive behaviours, affect 80% of all persons with dementia. 2 NPS include a variety of symptoms, some of which can result in significant distress for individuals with dementia or those around them. Although nonpharmacological treatments are recommended as first-line treatments for NPS, 3 –6 these approaches are not always effective, and research evidence on these approaches may not be readily translated to clinical practice because of the limited availability of resources in many regions. 7
Given the high prevalence of NPS, it is not surprising that psychotropic medication use is common among persons with dementia, with atypical antipsychotics being the most extensively studied class of medications. Guideline recommendations suggest that some atypical antipsychotics can be considered for the treatment of agitation, aggression, and psychosis that is severe, persistent, and either results in significant distress for the patient or poses a safety risk for the persons with dementia or those around them. 3,4,6 The clinical benefits of antipsychotics for NPS are modest, 8 and the types of NPS that respond to antipsychotics are limited. 9 Furthermore, the use of antipsychotics in persons with dementia is associated with increased risks of mortality, 10 stroke, 11 and more common side effects such as falls, 12 sedation, 8 and cognitive decline. 13
Despite these concerns, upward of 20% to 30% of persons with dementia are currently prescribed antipsychotic medications. 14 There is wide variation in the use of antipsychotics across long-term care (LTC) facilities beyond what can be explained by differences in underlying resident characteristics, 15,16 and variability in antipsychotic prescribing rates is associated with individual family physicians 17 and psychiatrists, 18 suggesting that antipsychotics may be used inappropriately in many instances. Other factors associated with increased use of antipsychotics include larger size of LTC facilities 16,19 and urban location of LTC facilities. 15,19 LTC facilities in which caregivers perceive lower access to recreational activities, less perceived availability of LTC staff, and less staff engagement with residents also have increased rates of antipsychotic use. 19 Antipsychotic prescribing in LTC is also highly correlated with other measures of quality of care such as overall mortality. 20 Inappropriate use of antipsychotics in LTC settings has recently become a focus of public scrutiny in Canada and has been the subject of numerous media reports. 15,21,22 Choosing Wisely, an international initiative to reduce ineffective or harmful health care interventions, has identified antipsychotic use among persons with dementia as one of its major recommendations for the care of older adults. 23
In this article, we review the patterns of antipsychotic use among persons with dementia and discuss factors associated with variation in antipsychotic use. We then provide an overview of strategies that have been adopted to minimize inappropriate prescribing. Our review will conclude with recent trends in antipsychotic use and initiatives that are under way in Canada to reduce inappropriate prescribing.
Antipsychotic Use in Dementia
Prevalence of Antipsychotic Use in Dementia
We completed a systematic review and meta-analysis to estimate the prevalence of antipsychotic use among persons with dementia. The electronic databases MEDLINE and Embase from inception until January 2014 were searched using standardized key words and medical subject headings to identify relevant studies. We included only studies that examined study populations with dementia diagnosed using standardized diagnostic criteria and that also reported on the proportion of the study sample who received antipsychotic medications. Information on study country, setting (community compared with LTC), and severity of dementia were extracted from studies. Random-effects meta-analysis was undertaken using the statistical program R to determine the pooled estimates of antipsychotic prescribing among individuals with dementia, and subgroup analyses were undertaken to evaluate factors associated with antipsychotic prescribing.
A total of 45 studies reported on the prevalence of antipsychotics among persons with dementia 16,24 –68 (Table 1), with 43 studies containing sufficient information to be included in a meta-analysis. In the meta-analysis of these studies, the pooled prevalence of any antipsychotic use among persons with dementia was 27.5% (95% CI 25.7% to 29.3%, P < 0.0001). There was evidence of significant statistical heterogeneity in the prevalence of antipsychotics reported in these studies (Q = 16 930, P < 0.0001, I 2 = 99.8%). There were significant differences in antipsychotic prescribing among studies with community-based samples when compared with LTC (Figure 1). In subgroup analyses, studies conducted in community settings (N = 11) had a lower prevalence of antipsychotic use when compared with LTC settings (N = 21; 12.3% compared with 37.5%; Q = 61.77, P < 0.0001). There was increasing prevalence of antipsychotic use with increasing severity of dementia from a rate of 6.7% reported in one study of mild dementia, 12.2% in studies with moderate dementia (N = 5), and 45.1% in studies involving severe dementia (N = 3; Q = 32.89, P < 0.0001).
Studies evaluating antipsychotic prescribing rates among persons with dementia.
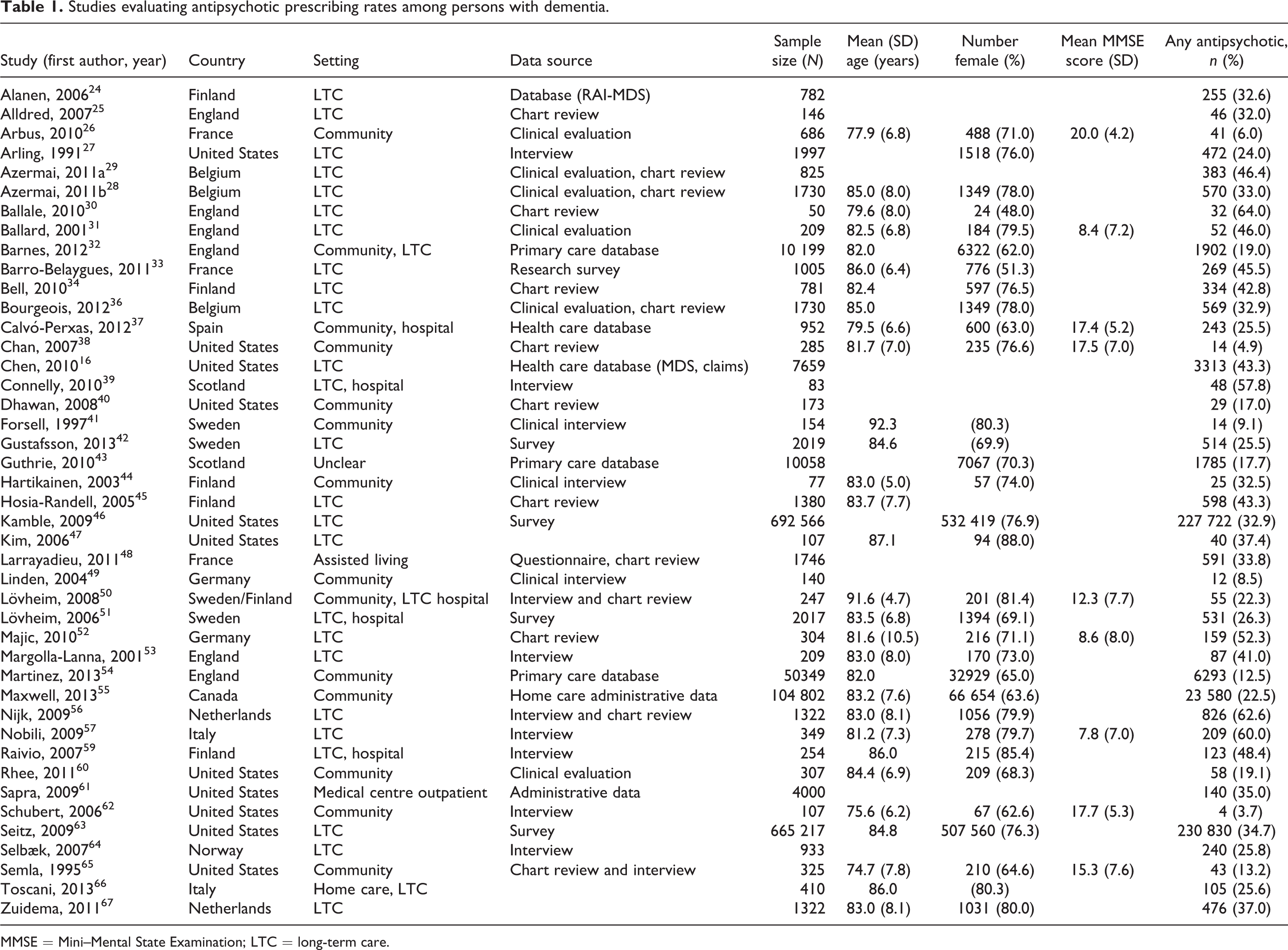
MMSE = Mini–Mental State Examination; LTC = long-term care.
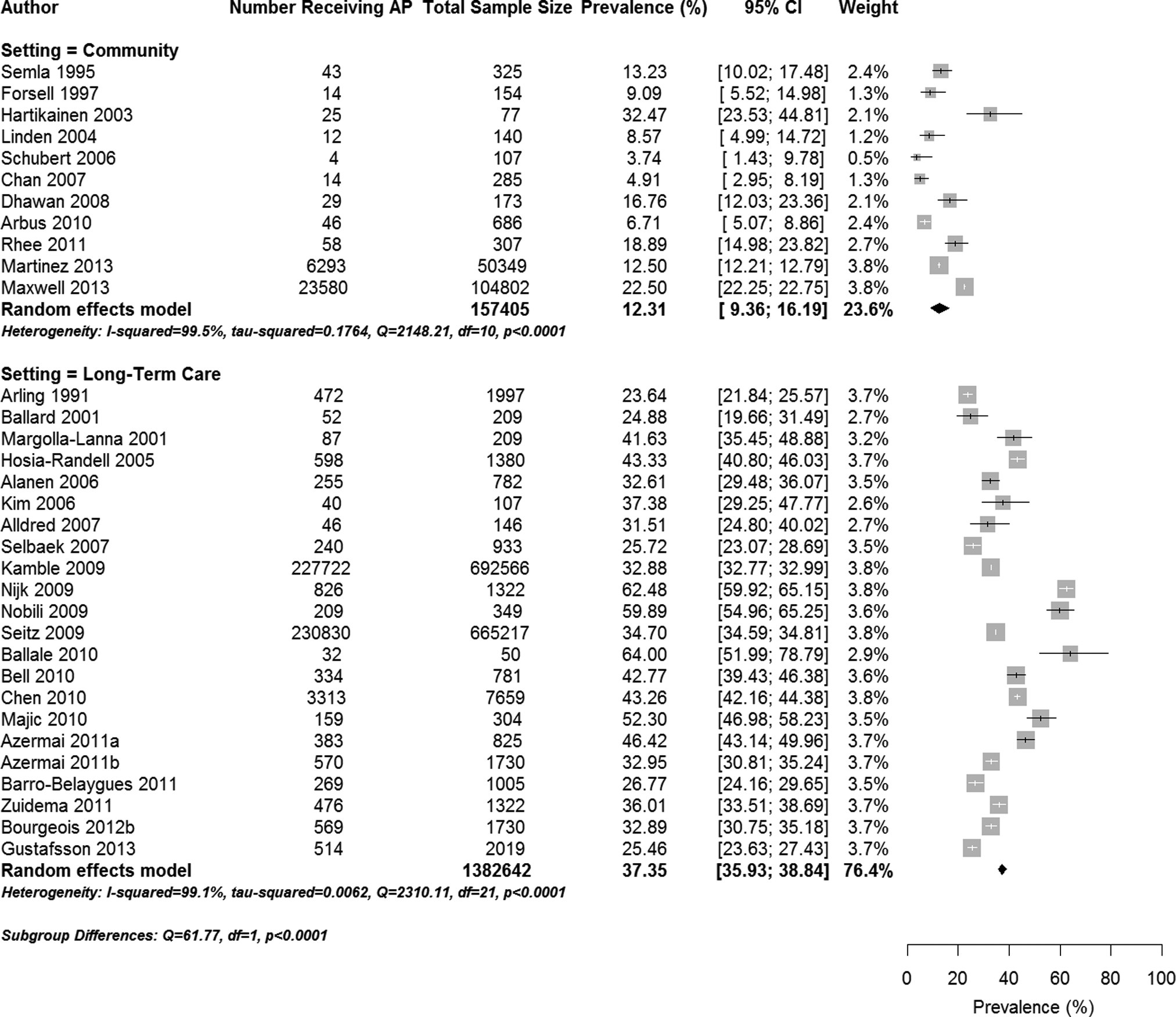
Forest plot of the prevalence of antipsychotic prescribing in community and long-term care settings.
Trends in Antipsychotic Use
Meta-regression was used to examine whether there have been changes in antipsychotic prevalence over time in the studies included in our review. We observed a small but significant reduction in the prevalence of antipsychotics in community settings (β = –0.06, P < 0.0001) and a small increase in antipsychotic prescribing rates reported over time from studies conducted in LTC (β = 0.03, P < 0.0001).
Analysis of antipsychotic prescribing over time within health regions is encouraging, with recent studies generally showing reductions. Analysis of data reported to the Canadian Institute of Health Information (CIHI) between 2001 and 2007 found a 37.7% prevalence of antipsychotic use among all older adults in LTC. In the time periods preceding and following Health Canada warnings about antipsychotics in 2005, there was an overall increase in the use of antipsychotics in Ontario, but the rate of increase in the use of antipsychotics decreased following the warnings when compared with the time period immediately preceding them. 69,70 Updated information on antipsychotic use in LTC using the CIHI indicator have shown reductions in inappropriate antipsychotic use from 2010 and 2015 71 (Figure 2).
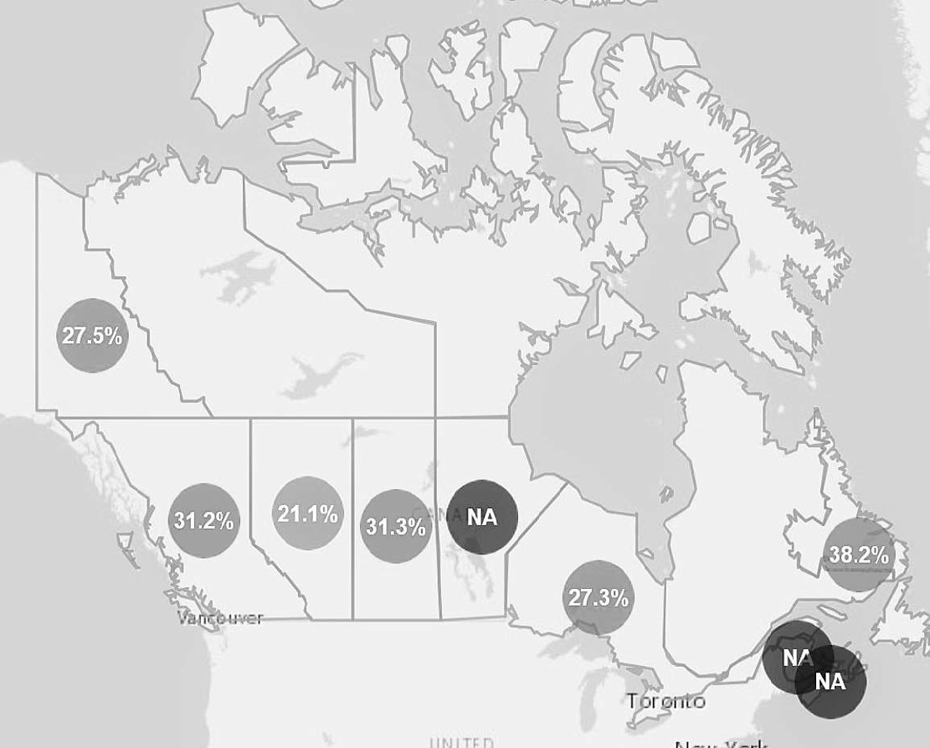
Provincial rates of inappropriate prescribing of antipsychotics in long-term care in Canada using Canadian Institutes of Health Information Indicator. NA = not applicable due to data not being available. All numbers indicate provincial average of antipsychotic indicator across all reporting long-term care sites within each province. Reprinted with permission from the Canadian Institutes of Health Information Indicator, available at www.yourhealthsystem.cihi.ca, accessed August 23, 2016.
Antipsychotic prescribing rates in US LTC homes have decreased significantly since rates approaching 50% were observed in the mid-1990s, 72,73 and reductions among persons with dementia in US outpatient settings have also been observed. 74,75 Similar reductions in antipsychotic use have been observed over time in the United Kingdom 76 and France, 77 whereas a study of antipsychotic trends in Germany did not find significant reductions in use among persons with dementia. 78 In studies that have evaluated outcomes potentially related to lower antipsychotic use, other psychotropic medication or restraint use has generally not increased, 72,74,79,80 although a few have documented small increases in the use of antidepressants. 76,81,82 This is in keeping with several large-scale studies indicating that antipsychotics can be successfully discontinued in most individuals without significant worsening of behavioural symptoms. 83,84 Risk factors for relapse following antipsychotic discontinuation include greater severity of NPS at the time of antipsychotic initiation 83 and shorter duration of antipsychotic treatment when compared with chronic use. 85 Together, these findings are encouraging, although current rates are still higher than what is likely optimal in many settings.
Measuring Appropriateness of Antipsychotic Prescribing
Crude rates of antipsychotic prescribing do not provide any information on the potential appropriateness of use, and antipsychotic prescribing rates are commonly adjusted to account for differences in patient characteristics between facilities. The inappropriate use of antipsychotics indicator is calculated by CIHI using data that are routinely collected and reported by approximately 57% of all LTC facilities in Canada 71 using the number of individuals receiving an antipsychotic on 1 or more days within the 7 days preceding their most recent LTC assessment, divided by the total number of individuals in the facility or region who do not meet exclusion criteria. 86 The CIHI indicator excludes individuals with schizophrenia, Huntington’s disease, those with active delusions or hallucinations, and those at the end of life (all potential indications for antipsychotics). To compare rates across facilities or regions, adjustments are made for heterogeneity in underlying clinical populations and for differences in age, severity of dementia (as measured by the Cognitive Performance Scale), and agitation. 87,88 The CIHI indicator is currently publicly reported for all LTC facilities in Ontario, Alberta, British Columbia, and the Yukon, with partial reporting in Newfoundland, Nova Scotia, and Manitoba. In the most recent data, the overall rate of potentially inappropriate prescribing of antipsychotics among reporting LTC homes is 27.5% (Figure 3). Reporting of the CIHI indicator is limited to LTC facilities; data from community, hospital, or other settings are not reported on.
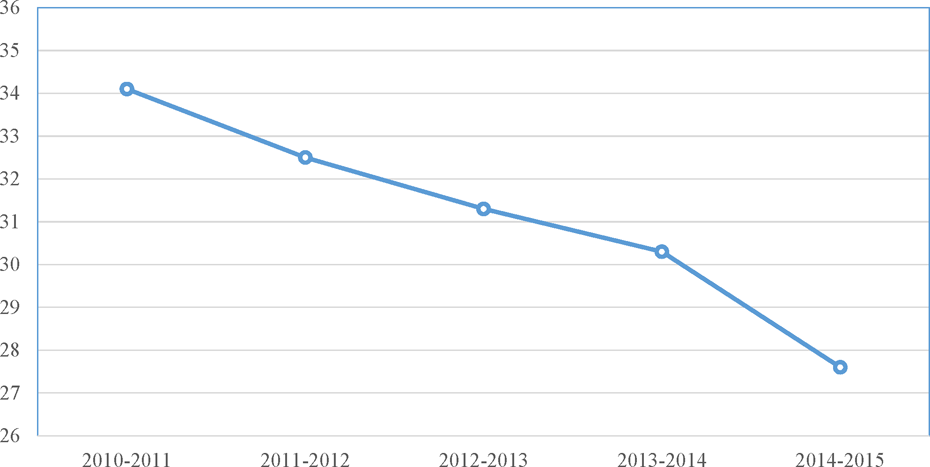
Trends in rates of inappropriate antipsychotic use in long-term care facilities in Canada using the Canadian Institutes for Health Information (CIHI) Inappropriate Use of Antipsychotics Indicator. Rate reflects the average rate of inappropriate antipsychotic use of all long-term care facilities reporting to CIHI. Adapted from the Canadian Institutes of Health Information Indicator, available at http://www.yourhealthsystem.cihi.ca, accessed April 26, 2016.
There are significant limitations to the CIHI indicator when applied at an individual level. Some potential indications for antipsychotics among people with dementia, most importantly significant symptoms of aggression, are not captured in the exclusion criteria for the CIHI indicator. The CIHI indicator lists only schizophrenia as a mental health exclusion criterion, whereas other mental health conditions such as bipolar disorder and major depression may also be appropriate indications for antipsychotics in older adults. Given that there are appropriate indications for antipsychotic use in some instances, a proportion of individuals who are receiving antipsychotics appropriately will be misidentified on the CIHI indicator. Polypharmacy, either with multiple antipsychotics or antipsychotics in combination with other psychotropics, is common in LTC settings 20,82 but also not captured by the CIHI indicator.
Approaches to Reduce Inappropriate Antipsychotic Use
Several approaches have been employed to reduce inappropriate antipsychotic use among persons with dementia. These strategies can include policy or regulatory approaches, public reporting, and interventions directly targeting health care providers. We review the history and the strengths and limitations of each in the remainder of this review.
Policy and Regulatory Approaches
Administrative approaches, including policy change and the use of legislation, have the potential to broadly affect prescribing practices. The United States and United Kingdom are among the first jurisdictions to implement national policy approaches aimed at reducing unnecessary use of antipsychotics. Although other countries have since implemented similar policies, a broad regulatory framework has yet to be developed in Canada.
In response to concerns regarding poor quality care in nursing homes in the United States, including high rates of antipsychotic use 89 and recommendations from an Institute of Medicine study, 90 the United States enacted legislation to improve care in nursing homes in the Federal Nursing Home Reform Act from the Omnibus Budget Reconciliation Act of 1987, referred to as OBRA-87. 91 For residents with dementia and NPS, OBRA-87 recommended a trial of nonpharmacological approaches, review, and dose reductions after 6 months of treatment 89 and limited the appropriate use of antipsychotics to individuals with psychotic disorders or severe agitation. 92
New care standards following OBRA-87 were enforced beginning in 1990. Early studies during this time period found relative reductions in antipsychotic prescribing rates of 32% to 36%. 79,93 Several subsequent studies demonstrated relative reductions in antipsychotic use by approximately 30% in most regions. 94 Prescribing patterns for other categories of psychotropic medications remained relatively stable overall, although some studies found small increases in the use of anxiolytics and antidepressants. 79,80,89,92,95 Although OBRA-87 did lead to early reduction of antipsychotics in LTC, most studies have questioned the impact on overall quality of care. 96 Rates increased again in subsequent years, possibly because of the availability of atypical antipsychotics and expanded indications for their use, 97,98 although the use of antipsychotics did decline specifically among those with dementia. 98,99
In the United Kingdom, the Department of Health in collaboration with the Alzheimer’s Society created a dementia strategy in 2009. 100 Appropriate antipsychotic use was included within the strategy’s initiatives to improve overall care in LTC. 100 The strategy recommended national efforts be made to reduce the use of antipsychotics in persons with dementia across care settings by creating structures for auditing of antipsychotic use, skills development in primary care and LTC, and improved access to mental health services support. 101 Following introduction of the strategy, statistics from the National Health Service demonstrated a 10% absolute reduction in antipsychotic prescribing in community-based settings from 2006 (17% prescribing rate) to 2011 (7% prescribing rate), despite increasing numbers of individuals with dementia. 102 Antipsychotic prescribing rates in LTC settings have not been reported to date.
Public Reporting
Public reporting of quality information, such as inappropriate antipsychotic use, may result in improvements via several proposed mechanisms. Public availability of this information allows the public to select for better performance and for government and other funders to allocate resources or determine accreditation based on quality of care. 103 This selection process can increase demand for high-quality care, motivating providers to improve the care they deliver. 104 Other rationales have been proposed, including public reporting as a tool for regulation, as in the case of OBRA-87, or as a method for ensuring individual and organizational accountability. 105
In general, public reporting alone has mixed effects on quality of care. Reporting may stimulate quality improvement activities; however, relatively few studies have focused on its effect on clinical outcomes. 106 There is evidence suggesting that public reporting may be more effective in influencing changes at organizational and administrative levels, rather than at the level of individual providers or patients. 105,107
Starting in 2015, CIHI has provided publicly reported antipsychotic prescribing at the level of individual LTC facilities and by health regions in Canada (available at http://yourhealthsystem.cihi.ca/hsp/indepth#). In the United States, an antipsychotic indicator similar to the CIHI indicator is reported. 108 –110 Unlike the CIHI indicator, the presence of delusions or hallucinations is not an exclusion criteria, whereas bipolar disorder is. 109 The US Centers for Medicare and Medicaid Services has been publicly reporting information on LTC quality indicators since 2002, although public reporting of antipsychotics began only in 2012. 108 In 2012, a national, multidimensional initiative to reduce the unnecessary use of antipsychotics was implemented, including public reporting of antipsychotic rates (LTC facility level information is available at https://www.medicare.gov/nursinghomecompare/search.html). 108,111 This initiative proposed an initial goal of 15% relative reduction in antipsychotic prescribing rates from a baseline rate of 23.9% to 20.3%. 110 The most recent information on antipsychotic prescribing in US LTC facilities reported a rate of 17.4% at the end of 2015. This has prompted development of new benchmarks to reduce antipsychotic use to 16.7% by the end of 2016. 73 Comparison between LTC facilities included and excluded in this reporting indicated that during and following implementation of public reporting, the proportion of residents using antipsychotic medications declined in all facilities, but the difference in the short term was significantly larger (approximately 40% greater reduction) in those required to publicly report. 108,111 However, all facilities eventually experienced similar decreases, suggesting that public reporting broadly incentivized changes in prescribing. 108 Of note, the use of all psychoactive medications declined during this time, with no significant difference between reporting and nonreporting facilities. 108
Educational Approaches to Reducing Antipsychotic Use
In addition to systems-level approaches to reducing inappropriate antipsychotic use such as policy or public reporting, there is increasing evidence for a variety of approaches focused on individual health care providers. A recent systematic review by Coon et al 112 identified 22 studies that have been used to reduce inappropriate antipsychotic use in LTC settings. The quality of studies included in this review varied, as did the components and duration of the interventions, which precluded a meta-analysis. Most studies in the review examined educational strategies (n = 11) directed at LTC staff or physicians. Most high-quality studies in this review demonstrated absolute reductions in antipsychotic use of 12% to 20%. Educational in-reach approaches involving education and individual patient review (n = 6) were also largely effective in reducing antipsychotic use in studies that evaluated these approaches. Multicomponent interventions (n = 5), which variably included elements such as education, prescribing audit and feedback, and medication review by interdisciplinary teams, all showed consistent reductions in antipsychotic prescribing, although only 1 study was a randomized controlled trial. The long-term effects of these interventions beyond the implementation period were evaluated in only 4 studies, with mixed results on the sustainability of improvements noted following implementation.
A recent well-designed, randomized controlled trial evaluated the impact of medication review, social interaction, or exercise in 16 LTC facilities in the United Kingdom. 113 All participating LTC homes received education on person-centered approaches to care. Eight homes were randomized to receive each of the 3 interventions, with most facilities receiving more than 1. Antipsychotic review was associated with a 50% reduction in antipsychotic use. However, antipsychotic review in isolation was associated with a worsening of overall NPS when compared with antipsychotic review in the presence of the social interaction intervention. Exercise was also associated with overall improvements in NPS. This study demonstrates that although significant decreases in antipsychotics can be achieved with educational approaches, in the absence of improved access to nonpharmacological treatments, there may be detrimental effects of reducing antipsychotics on NPS.
Future Directions to Improve Antipsychotic Prescribing in Canada
Initiatives to Reduce Inappropriate Use of Antipsychotics in Canada
There are currently no national regulatory or policy strategies in Canada related to reducing inappropriate use of antipsychotics. Public reporting of the CIHI inappropriate use of antipsychotic indicator is now available for approximately half of all LTC facilities in Canada, although at this time it is difficult to assess the impact of this initiative on prescribing rates. Several provinces and health regions in Canada have initiated widespread programs to reduce inappropriate use of antipsychotics. Of these programs, the Appropriate Use of Antipsychotics initiative in Alberta 114 is the most extensive antipsychotic reduction intervention in Canada to date. The program, initiated in 2011, includes both policy and regulatory approaches involving a provincial clinical guideline 115 and program implementation including staff education, use of person-centered approaches to reduce NPS, and monthly interdisciplinary team rounds to support reduction or discontinuation of antipsychotics 114 (additional details are available at http://www.albertahealthservices.ca/scns/auatoolkit.aspx). The most recent information available in Alberta demonstrates a current inappropriate antipsychotic prescribing rate of approximately 18%. 71 Alberta currently has the lowest provincial average for antipsychotic prescribing, likely reflecting the initial impact of this initiative. Other initiatives currently under way in Canada include the Canadian Foundation for Healthcare Improvement Reducing Antipsychotic Medication Use Collaborative, involving more than 200 LTC facilities across Canada, 116 the Call for Less Antipsychotics in Residential Care program in British Columbia, 117 and the Ontario Ministry of Health and Long-Term Care Appropriate Prescribing Demonstration Project in Ontario. 87,118 Health Quality Ontario has recently developed draft quality standards for behavioural symptoms of dementia, establishing several process indicators to improve prescribing, documentation, and review of psychotropic medications. 119
Areas for Future Research
Although there is emerging evidence that a number of strategies can reduce inappropriate antipsychotic use in dementia, several areas require further research and evaluation. The optimal rate of antipsychotic use in dementia has not been determined. Based on changes in prescribing rates observed in which widespread initiatives for reducing antipsychotics have been implemented (such as the United States and Alberta), rates of inappropriate antipsychotic prescribing below 20% are likely feasible in many regions provided that similar processes to support reductions are available. Health Quality Ontario has proposed a provincial benchmark of 19% for performance on the CIHI potentially inappropriate antipsychotic prescribing indicator (N. Degani, manager, Health System Performance, e-mail message, August 17, 2016). Although reductions in antipsychotic use are possible within most LTC settings through modifying prescribing practices and existing care processes, the impact of factors such as the physical design of LTC facilities or changes to staffing models have not been examined in detail. There is also significant variation in antipsychotic prescribing in acute care, where antipsychotic rates may be as high or higher than those reported in LTC 120,121 and uncertainty regarding the prevalence of their use in other care settings where dementia is common, such as assisted living or supportive housing. Although some nonpharmacological strategies have proven effective in research studies, their feasibility in real-world settings and long-term efficacy have not been established, access to effective nonpharmacological approaches for NPS needs to be improved, 122 and the development of safe and effective pharmacological treatments for NPS is necessary. The outcomes associated with the prescribing of multiple antipsychotics or combinations of antipsychotics with other psychotropic medications also require future study.
We have attempted to provide an overview related to the prescribing of antipsychotics among persons with dementia and a summary of evidence-based strategies to reduce inappropriate use of antipsychotics. However, this is not a systematic review and as such may not include all the strategies that can address this complex topic. In general, the literature on optimal strategies for reducing inappropriate use of antipsychotics in dementia is relatively sparse and mostly from settings outside of Canada.
Conclusions
Antipsychotic use among persons with dementia is common and higher than what is indicated in many circumstances. Both broad, systems-level approaches and provider-level interventions have a role in reducing inappropriate use of antipsychotics. It is encouraging that rates of antipsychotics appear to be decreasing with time, but sustained effort will be needed to maintain current gains, and additional work is required to further reduce antipsychotics to more optimal levels of prescribing. Reaching desired goals for antipsychotic use in dementia care will require collaboration among psychiatrists, health care funders and regulators, fellow physicians, and front-line staff across a variety of health care settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Julia Kirkham is supported by an Interdisciplinary Fellowship Program Award through the Canadian Frailty Network. Dr Seitz receives consulting fees funding from Cancer Care Ontario in his role as the Provincial Medical Lead for Dementia Capacity Planning in Ontario. Dr. Rochon is the Retired Teachers of Ontario Chair in Geriatric Medicine at Women’s College Research Institute and the University of Toronto.
Funding
The author(s) declared receipt of the following financial support for the research, authorship, and/or publication of this article: This review was supported through research funding provided through the Canadian Institutes of Health Research through the Canadian Consortium on Neurodegeneration in Aging.