
Abstract
Objective:
To measure service use and costs associated with health care for patients with mental health (MH) and substance use/addiction (SA) problems.
Methods:
A 5-year cross-sectional study (2007-2012) of administrative health care data was conducted (average annual sample size = 123,235 adults aged >18 years who had a valid Ontario health care number and used at least 1 service during the year; 55% female). We assessed average annual use of primary care, emergency departments and hospitals, and overall health care costs for patients identified as having MH only, SA only, co-occurring MH and SA problems (MH+SA), and no MH and/or SA (MH/SA) problems. Total visits/admissions and total non-MH/SA visits (i.e., excluding MH/SA visits) were regressed separately on MH, SA, and MH+SA cases compared to non-MH/SA cases using the 2011-2012 sample (N = 123,331), controlling for age and sex.
Results:
Compared to non-MH/SA patients, MH/SA patients were significantly (P < 0.001) more likely to visit primary care physicians (1.82 times as many visits for MH-only patients, 4.24 for SA, and 5.59 for MH+SA), use emergency departments (odds, 1.53 [MH], 3.79 [SA], 5.94 [MH+SA]), and be hospitalized (odds, 1.59 [MH], 4.10 [SA], 7.82 [MH+SA]). MH/SA patients were also significantly more likely than non-MH/SA patients to have non-MH/SA-related visits and accounted for 20% of the sample but over 30% of health care costs.
Conclusions:
MH and SA are core issues for all health care settings. MH/SA patients use more services overall and for non-MH/SA issues, with especially high use and costs for MH+SA patients.
The critical role of mental health (MH) in overall health is well recognized, 1 including a mental health action plan developed by the World Health Organization 2 ; however, the extent that mental health contributes to use of general health care services remains unclear. Even less is known regarding co-occurring mental health and substance use/addiction (SA) problems and how they are related to health service use.
Several studies have found that frequent emergency department users may be more likely to have MH and/or SA (MH/SA) problems compared to less frequent users. 3 –7 However, most of these studies used small samples from a single hospital or community, and a recent review 8 concluded that findings depend on factors such as location of the health care setting. Evidence also indicates high rates of MH and SA problems among frequent users of other medical services (e.g., primary care). 9,10 Again, these studies used small samples from a single clinic or practice. One exception was a study of all health care users in British Columbia, 11 which found that frequent health care users were more likely than less frequent users to be diagnosed with a psychosocial condition (including both MH and SA); however, this study did not determine whether services used were for psychosocial versus other health conditions.
The present research advances knowledge through 4 methodological enhancements to research in this area. First, we used a large random sample of health care users to assess a broad range of medical services used by persons who have MH/SA problems. This allowed a more complete picture of service use by persons with MH/SA problems than obtained with previous studies examining only one type of service.
Second, we compared health care use patterns for persons with MH, SA, and co-occurring MH and SA (MH+SA) problems. MH and SA problems commonly co-occur, 12 –14 affecting service needs and use. 15 –21 Although some research has examined outcomes for persons with co-occurring MH and SA, 22 no studies of general health care use have systematically compared use for persons with MH problems only, SA only, MH+SA, and no MH/SA problems.
Third, we assessed whether persons with MH/SA problems used health care services for MH/SA needs or for other health issues. People who have MH/SA disorders are at higher risk of physical health problems and are more likely to incur intentional and unintentional injuries. 1,9,23 –26 They may also require more extensive treatment for physical health problems 27 –30 compared to persons who do not have MH/SA disorders. MH/SA problems can also hamper help seeking, diagnosis, and treatment, 1,31 possibly resulting in greater severity of physical health problems. Thus, to better understand why people with MH or SA problems are heavier users of medical services, it is important to examine the extent of service use for both MH/SA and non-MH/SA health problems.
Finally, we estimated overall medical service costs associated with MH/SA problems. Other than 2 studies comparing costs for psychiatric patients with and without co-occurring substance use disorders, 17,18 little is known about the health care costs for MH/SA versus non-MH/SA patients and the extent that costs are associated with MH or SA only versus co-occurring MH and SA problems.
Objectives
The objectives of this research were to estimate use of different medical services by persons who have MH/SA problems, including visits to primary care physicians, emergency departments visits, hospitals admissions, and total health care costs; compare health care use by persons with MH only, SA only, and MH+SA problems to a common control group of persons with no MH/SA problems; and assess the extent that services used by MH, SA, and MH+SA patients addressed MH/SA versus non-MH/SA problems.
Methods
We used a 5-year cross-sectional study design to examine 12-month health care utilization among persons categorized as having MH only, SA only, and both MH and SA (MH+SA) problems compared to individuals not identified as having MH or SA problems (non-MH/SA). This design allowed us to focus on patients with current MH or SA problems (i.e., met criteria for MH or SA within a 12-month timeframe) with replications across multiple years to increase robustness of findings. We selected a random sample of 200,000 Ontario residents who had a valid health insurance card (with universal health care, this includes almost all residents of Ontario; population 13.6 million) for each fiscal year (beginning on April 1 of each year), starting with 2007. We excluded 40,849 individuals (averaged across the 5 years) who did not use any of the health services included in the study and 35,915 individuals (averaged across the 5 years) who were younger than 19 years of age (the legal age for alcohol consumption in Ontario). The resulting average sample size across the 5 years was 123,235 (55% female).
We used the administrative health databases at the Institute for Clinical Evaluative Sciences (ICES) where patient-level records pertaining to provincially funded medical services are linked anonymously using unique encrypted identifiers. Specifically, we included: inpatient service utilization from the Canadian Institute for Health Information (CIHI), Discharge Abstract Database (DAD), and the Ontario Mental Health Reporting System (OMHRS) database (OMHRS records all hospitalizations in Ontario in psychiatric-designated beds); emergency department visit information from the CIHI National Ambulatory Care Registration System (NACRS) database; and physician visit data from the Ontario Health Insurance Plan (OHIP) database. We used the Ontario Drug Benefits (ODB) database to capture methadone use for opioid maintenance treatment (benefits available to persons aged 65+, on social assistance, etc.; http://www.health.gov.on.ca/en/public/programs/drugs/programs/sdp.aspx). Demographic information was obtained from the Registered Persons Database (RPDB). The study was approved by the Centre for Addiction and Mental Health Research Ethics Board.
Case Ascertainment
Patients were classified as MH if they met at least one of the following criteria: 1) a mental health–related discharge diagnosis from a general hospital bed (ICD-10 codes F20-F69), 2) a mental health–related diagnosis from a psychiatric hospital bed (DSM-IV codes 295-298, 311, 300, or 301), 3) a mental health– or self-harm–related emergency department (ED) visit (ICD-10 codes F20-F69, X60-X84), or 4) an OHIP billing claim for a mental health–related primary care physician or psychiatrist visit (based on a validated algorithm developed by Steele et al. 32 ). Dementia and delirium were excluded because they involve medical as well as psychiatric illnesses that often result in placement in long-term care. Childhood disorders, including mental retardation/developmental delay and autism, were also excluded.
SA case criteria included at least one of the following: 1) a substance-related discharge diagnosis from a general hospital bed (ICD-10 codes F10-F19, F55), 2) a substance-related diagnosis from a psychiatric hospital bed (DSM-IV code 303 or 304), 3) a substance-related ED visit (ICD-10 codes F10-F19, F55), 4) an OHIP billing claim with a substance-related diagnosis (DSM-IV code 303 or 304), or 5) an ODB claim for methadone (only 15 SA cases were uniquely identified by this criterion).
Persons were further categorized as MH only, SA only, MH+SA, or non-MH/SA for comparison of service use patterns.
Outcomes
For each of the 4 patient categories (MH only, SA only, MH+SA, non-MH/SA), we calculated the average number of primary care physician visits, ED visits, and hospitalizations (both MH/SA and non-MH/SA related) across the 5 years. We determined whether each visit/hospitalization was for MH/SA using the same criteria used for case ascertainment. Visits coded MH/SA may have also involved non-MH/SA diagnoses or treatments in addition to MH/SA, while those coded “non-MH/SA” included only visits that did not involve any MH or SA. We measured annual total costs (in Canadian dollars) for all services delivered to each person and paid for by the health care system using the algorithm developed by Wodchis et al. 33 and commonly used for cost analyses. 34 This algorithm includes measuring the cost of services based on individual utilization and associated fees paid by the government. When individual costs are not available (e.g., for institutional settings), it allocates institutional costs to individual visits or admissions. Thus, costs include the 3 main outcomes for the present study as well as any other costs billed to the health care system.
Statistical Analyses
Descriptive statistics were computed for each outcome across the 4 MH/SA groups and averaged across the 5 years. Negative binomial regression models were used to compare groups for number of primary care visits per person for the final year of the sample (2011-2012). These analyses model the log of the expected count (i.e., number of visits) as a linear function of the predictor variables. The coefficients obtained were exponentiated to obtain rate ratios and confidence intervals. ED visits and hospitalizations were converted to dichotomous variables (1 = any visit/hospitalization, 0 = no visit/hospitalization) because of their highly skewed distributions and were regressed onto the categorical variable reflecting the 4 MH/SA groups using logistic regression. All regression models adjusted for age and sex. Although we present regression results for 2011-2012 in this article, separate regression models were calculated for each year and showed similar findings. Data were analyzed using SAS Version 9.2 (SAS Institute, Cary, NC, USA).
Results
Table 1 shows demographic characteristics and overall costs for each group averaged across the 5 years. Similar results were found for each year, reflecting no major changes in the health care system during that period. As shown in the table, more women than men were in the MH group, while more men than women were in the SA and MH+SA groups. Average age for the MH group was similar to the non-MH/SA group (about 48-49 years); however, SA patients were about 5 years younger and MH+SA patients about 7 years younger than those in the non-MH/SA group. About 20% of the sample met criteria for MH/SA, with most classified as MH problems only (18%) and less than 2% having service use involving SA (0.71% SA and 0.90% MH+SA). Per capita costs were about double for MH-only and SA-only patients compared to non-MH/SA patients and more than 3 times for MH+SA patients. Overall, MH/SA patients accounted for over 30% of total health care costs.
Sex, Age, and Health Care Costs for Patients Identified as Having Mental Health Problems Only (MH), Substance Use/Addiction Problems Only (SA), Both MH and SA Problems (MH+SA), or No MH- or SA-Related Medical Service Use (Non-MH/SA).
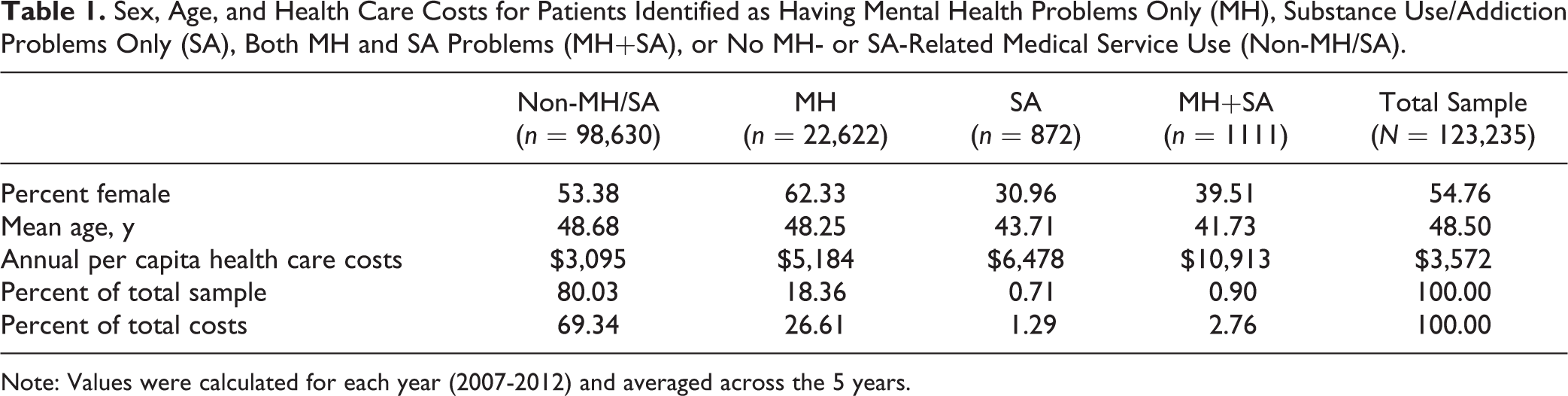
Note: Values were calculated for each year (2007-2012) and averaged across the 5 years.
Number of Primary Care Physician Visits, ED Visits, and Hospital Admissions
Mean numbers of primary care physician visits, ED visits, and hospital admissions for MH, SA, MH+SA, and non-MH/SA patients averaged over the 5 years are shown in Figures 1 to 3, respectively. Rate and odds ratios of service use for MH, SA, and MH+SA compared to non-MH/SA patients and results of statistical significance tests, controlling for sex and age, are shown in Table 2.
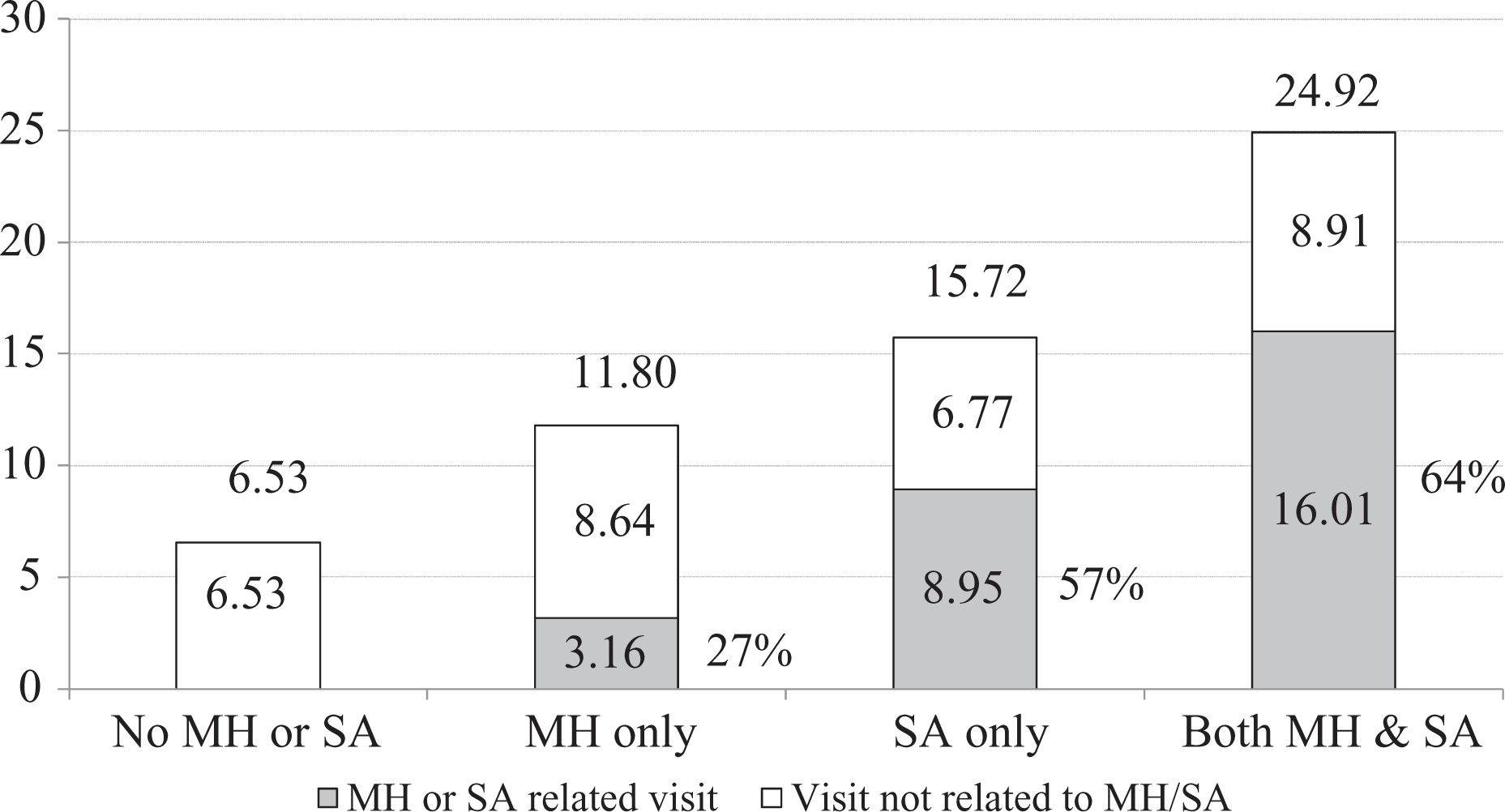
Annual mean number of primary care physician visits by patients identified as having mental health problems only (MH), substance use/addiction problems only (SA), or both MH and SA problems (MH+SA) compared to patients who did not use services for MH or SA (No MH/SA). The median and mode for number of visits for each group (averaged across the 5 years) were 4.0 and 1.0 (respectively) for no MH or SA, 6.8 and 2.2 for MH only, 9.0 and 4.4 for SA only, and 14.4 and 5.6 for MH+SA. Of the 16.01 MH- or SA-related visits by the MH+SA group (shown as the dark part of the bar), 12.32 were recorded as SA and 3.69 recorded as MH.
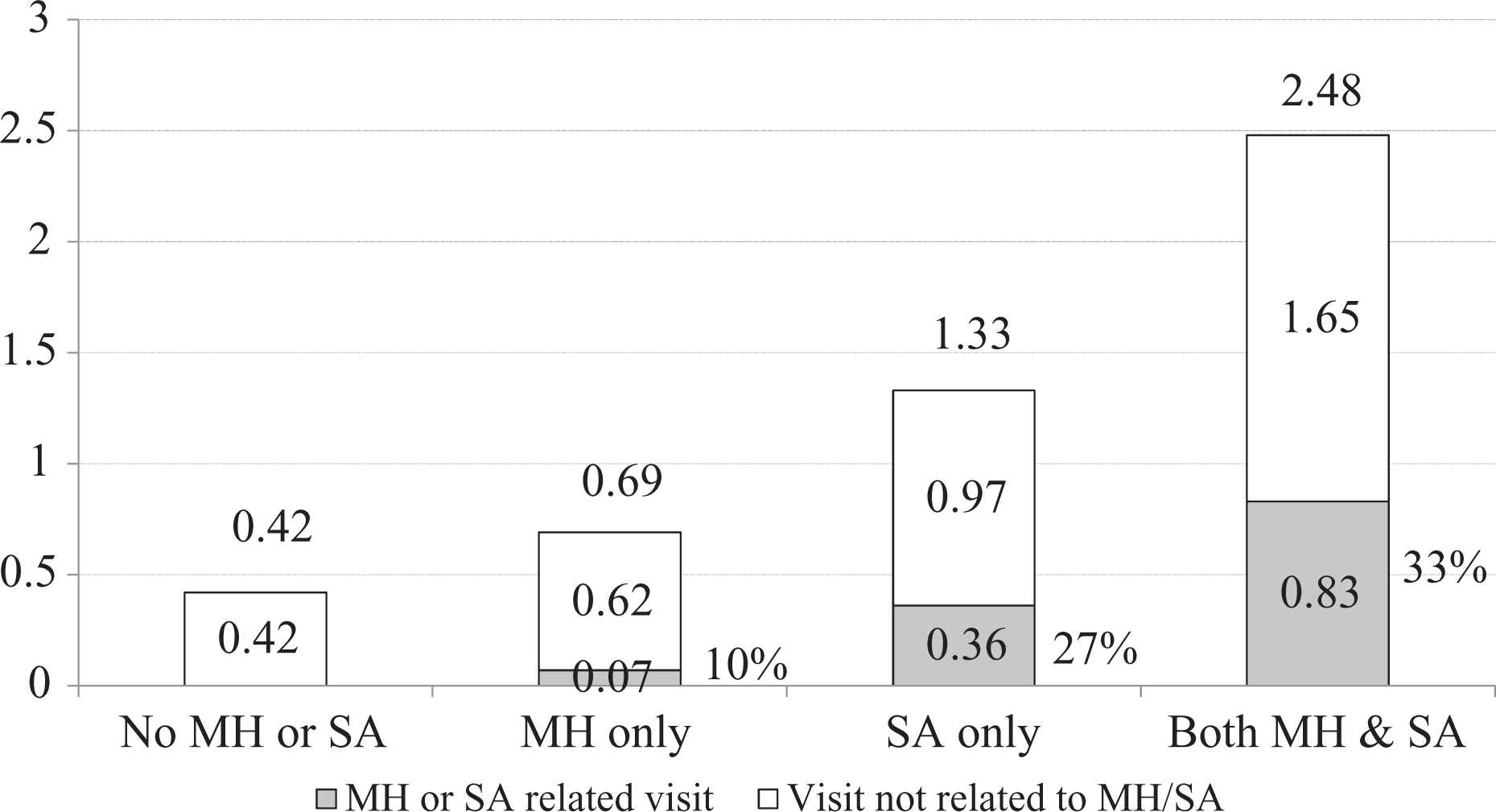
Annual mean number of emergency department visits by patients identified as having mental health problems only (MH), substance use/addiction problems only (SA), or both MH and SA problems (MH+SA) compared to patients who did not use services for MH or SA (No MH/SA). The percent reporting 1 or more emergency department visits for each group (averaged across the 5 years) was 25.5 for no MH or SA, 33.0 for MH only, 55.1 for SA only, and 65.2 for MH+SA. For MH+SA patients, .53 of the .83 MH/SA visits were recorded as SA and .40 as MH (some patient visits were recorded as both MH and SA related).
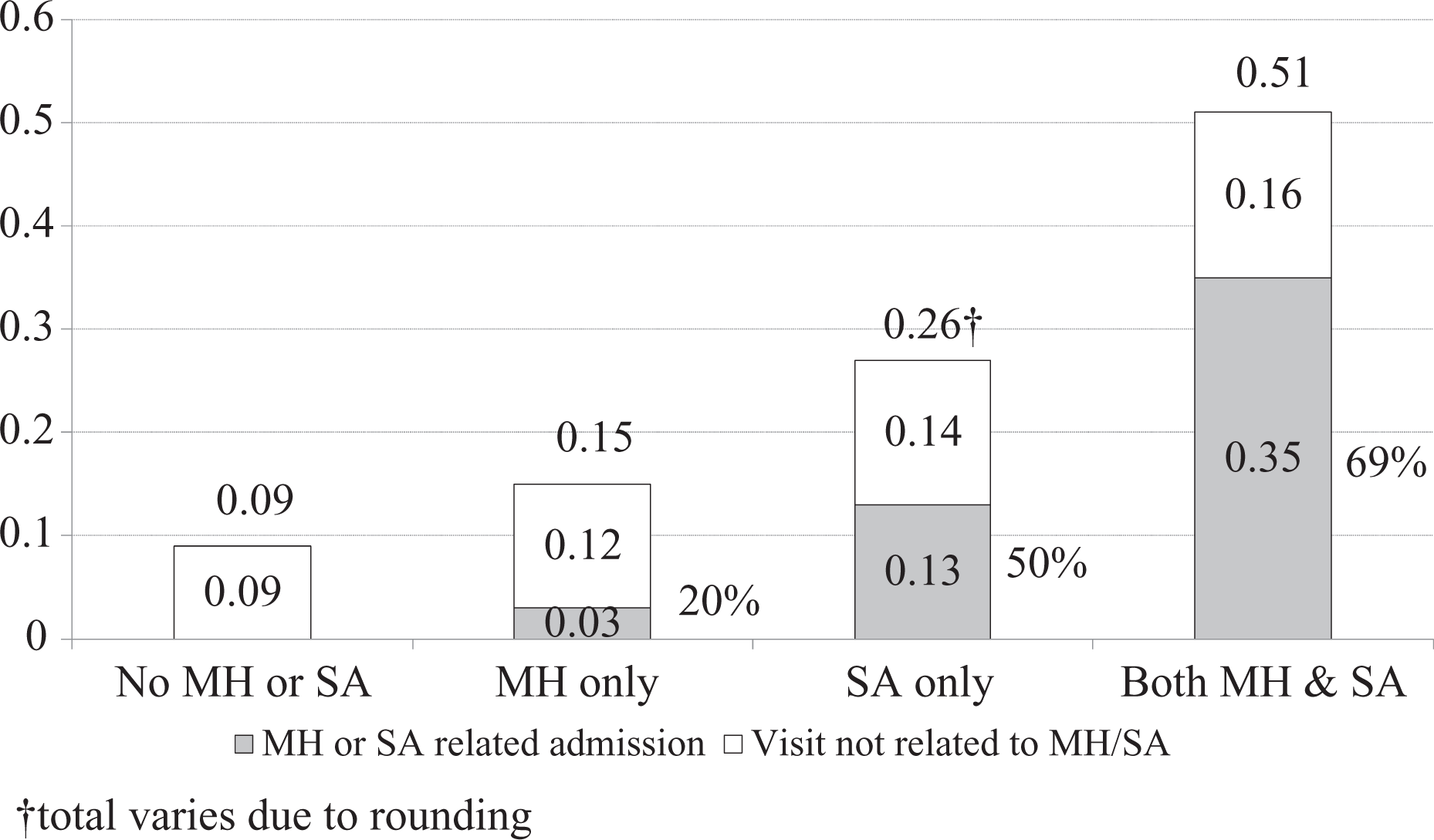
Annual mean number of hospitalizations by patients identified as having mental health problems only (MH), substance use/addiction problems only (SA), or both MH and SA problems (MH+SA) compared to patients who did not use services for MH or SA (No MH/SA). The percent reporting 1 or more hospitalizations for each group (averaged across the 5 years) was 7.0 for no MH or SA, 10.7 for MH only, 18.0 for SA only, and 28.8 for MH+SA. For MH+SA patients, .20 of the .35 hospitalizations for MH or SA were recorded as related to SA and .24 related to MH (some hospitalizations were recorded as both MH and SA).
Health Service Utilization by Mental Health Problems Only (MH), Substance Use/Addiction Problems Only (SA), or Both MH and SA Problems (MH+SA) Compared to Patients Who Did Not Use Services for MH or SA (Non-MH/SA).
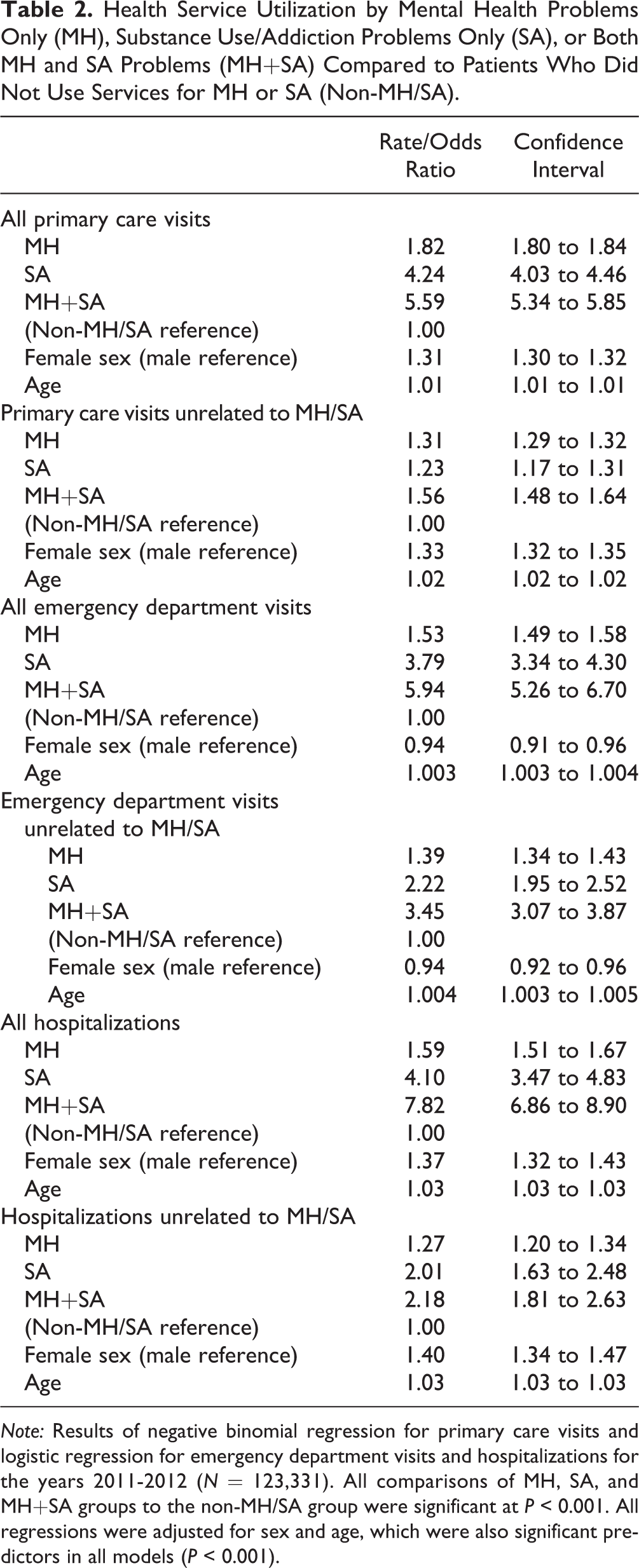
Note: Results of negative binomial regression for primary care visits and logistic regression for emergency department visits and hospitalizations for the years 2011-2012 (N = 123,331). All comparisons of MH, SA, and MH+SA groups to the non-MH/SA group were significant at P < 0.001. All regressions were adjusted for sex and age, which were also significant predictors in all models (P < 0.001).
Each bar in Figure 1 shows the total annual mean number of visits to a primary care physician by whether the person was classified as MH, SA, MH+SA, or non-MH/SA. As shown in Figure 1, MH+SA patients visited primary care physicians most often (annual mean of 24.92 visits) followed by SA (15.72), MH (11.80), and non-MH/SA (6.53). Most visits for MH+SA and SA patients were for MH/SA reasons (64% and 57%, respectively—shown as the grey part of the bar), whereas only 27% of visits were for MH for patients in the MH group.
Figure 2 shows that MH+SA patients visited the emergency department most frequently (mean of 2.48 visits per year), followed by SA (1.33 visits), MH (0.69 visits), and non-MH/SA (0.42 visits). For all MH/SA groups, a third or less of visits related to MH/SA (10% for MH, 27% for SA, and 33% for MH+SA).
The results shown in Figure 3 for hospitalizations indicate the same pattern, with most frequent hospitalizations by MH+SA patients, followed by SA, MH, and non-MH/SA. For MH, most hospitalizations were not related to MH (20% related to MH). However, 50% of hospitalizations of SA patients were related to SA, and 69% of MH+SA were related to MH/SA.
Table 2 shows the regression results comparing MH/SA groups to non-MH/SA patients for 2011-2012 adjusting for sex and age (results were similar for other years; not shown). Analyses indicated that all MH/SA groups were significantly different from the non-MH/SA group at the P < 0.001 level for all comparisons. Consistent with results shown in the figures, overall rate and odds ratios controlling for sex and age were highest for MH+SA patients, followed by SA and MH across all 3 types of service use. For example, compared to non-MH/SA patients, MH+SA patients visited a primary care physician more than 5 times as often, were almost 6 times as likely to use the ED, and almost 8 times as likely to be hospitalized.
For analyses restricted to non-MH/SA visits, all rate and odds ratios were attenuated but remained significant, with more frequent visits/hospitalizations for MH, SA, and MH+SA patients (P < 0.001) than for non-MH/SA patients in all models. However, attenuation was more pronounced for primary care physician visits and hospitalizations than for ED visits, especially for the SA and MH+SA groups. For example, the rate ratio for MH+SA (compared to non-MH/SA) was reduced from 5.59 for all primary care physician visits to 1.56 when analyses were restricted to non-MH/SA visits, whereas the odds ratio for ED visits decreased from 5.94 to 3.45.
Discussion
Analyses of health care records of primary care visits, ED visits, and hospitalizations from a large representative sample provide several new insights into use of general medical services by patients with MH/SA problems. First, the present findings provide clear evidence that individuals with MH/SA problems are more frequent users of all types of medical services. Per capita use was highest for patients with MH+SA problems, followed by SA only and MH only, and lowest for those without MH/SA problems. Second, costs associated with service use were higher for those with co-occurring MH+SA problems compared to SA-only and MH-only groups. This confirms other evidence that patients with MH+SA problems have more complex needs and are high users of health services. 16 –21,35 Thus, it is critical that professionals providing general medical services have training and capacity to ensure adequate care for persons with MH/SA problems, especially given findings by Wang et al. 36 that persons with serious mental illness who were treated only in the general medical sector were less likely to receive minimally adequate care compared to those receiving specialist care.
Only a small proportion of cases were identified as SA—less than 2% of the sample (including both SA and MH+SA cases); yet, according to 2013 survey data, 13.7% of Ontario adults reported hazardous or harmful drinking, and 6.6% reported symptoms of alcohol dependence in the past year 37 (using the Alcohol Use Disorders Identification Test [AUDIT 38 ]). Thus, it is likely that not all patients who actually had SA problems were identified. Underidentification may have been due to SA problems being generally underidentified by medical staff. 39 As well, even when the role of SA is identified, it may not be recorded in medical records (e.g., emergency treatment for an injury that is alcohol related). Also, stigma associated with SA may cause people with SA problems to avoid doctors 40 or not reveal alcohol problems to medical professionals. Of note, the MH+SA group was larger than the SA-only group. This may reflect the high rate of co-occurring MH problems among persons with SA problems, 12 –14 greater likelihood of identification because of more frequent contact with the system, or greater opportunity for SA problems to be identified when MH problems are treated.
The high number of primary care visits by persons with MH/SA problems confirms that family doctors play a major role in care for persons with MH problems. 41 –43 North American studies suggest that this role has been increasing, 43,44 with 1 study in Manitoba 43 finding that 24% of services provided by family doctors were for psychosocial conditions. We cannot know from the present data the extent that patients see family doctors instead of or in addition to using mental health and substance use specialty services. However, given the relatively high use of primary care services and related costs for MH/SA problems, it is crucially important that primary care physicians know not only how to address MH 24 and SA problems 39 but also how to link patients with other specialized services, 45 including psychiatrists 46 and MH/SA specialty services in the community. 2,47 It is also important to explore and evaluate efforts to coordinate care between primary care physicians and other MH/SA services through collaborations and partnerships. 48 –53
The high use of ED services by people with MH/SA problems, especially those with co-occurring MH+SA problems, suggests that it is important for future research to ascertain the extent that such use reflects unavoidable need for emergency services versus system factors such as insufficient local specialist services for MH/SA, 54 including a lack of 24-hour access to MH and SA counselling 55 ; poor access to psychiatrists and other counselling services to manage MH problems before they reach a crisis 46,56,57 ; poor health-related attitudes and values 58 ; low use of preventive health services by some heavy drinkers 59 ; or poverty and other social determinants that may lead to use of emergency services in the absence of access to more suitable services. 25,60 –62
Patients with MH/SA problems also made more visits for non-MH/SA reasons (physical health) compared to non-MH/SA cases, and this was especially true for ED visits. This finding is consistent with evidence that people with MH/SA problems tend to experience more health problems generally and more intentional and unintentional injuries than do people with no MH/SA problems 1,9,23,24,26 Most notably, two-thirds of ED visits by patients with MH+SA problems were recorded as non-MH/SA related. The high rate of non-MH/SA emergency department visits may be reflective of the high prevalence of medical comorbidity in this patient population 1,23,24 ; however, it is also possible that the links between MH/SA and illness/injury are sometimes missed or not recorded by attending physicians. 63 Further investigation is needed to assess the extent that MH/SA problems are recognized 64 and treated effectively 65 at EDs.
Strengths and Limitations
Strengths of the present analyses include a broad approach to identifying users of the system based on a large general population sample of patients who used physician/hospital services across the province as opposed to data from a single health care provider as in most previous studies; examination of a broad range of services, including primary care, hospitalizations, and ED, as well as total costs; comparison of patients classified into 4 groups using standard criteria (MH only, SA only, MH+SA, and non-MH/SA); and assessment of service use for both MH/SA versus non-MH/SA reasons.
A limitation of the study is that administrative data may include diagnoses that are incomplete or inconsistently reported. As well, MH/SA problems may be underidentified in general medical settings given that many people with MH/SA problems do not receive treatment for these problems. 66 Also, we have no information about the rate of MH/SA problems among those who were excluded because they did not use any general medical services during the study period. As discussed above, underidentification may be especially true for SA problems. Specifically, the Steele et al. 32 algorithm that we used has been validated for identifying MH cases generally (with SA codes subsumed under MH); however, no separate validation was done for SA codes. In addition, while the relatively large proportion of MH cases (over 18%) suggests that a broad range of MH problems (from minor to severe) were included in the sample, it is possible that SA cases included only those with severe SA problems. Thus, comparisons of rates of service use for MH versus SA should be interpreted with caution. Despite possible underidentification of SA, separating SA only from co-occurring MH+SA patients provides important new knowledge absent from previous studies that compared MH+SA to MH only but not to SA only.
Finally, although the findings are consistent with evidence from the United States and elsewhere, another limitation of this study is that data are from a single Canadian province with a publicly funded health care system and may not be fully generalizable to other types of health systems.
Conclusion
It is clear that primary care physicians and other medical/hospital workers play a major role in assisting persons who have mental health and substance use/addiction problems. As such, MH/SA is not a specialty health issue but rather a core health issue that affects all health service environments. 1 Therefore, it is critical that health professionals in these environments have core competencies 59 relating to MH and SA identification, prevention, and treatment, as well as an understanding of interrelationships and interactions of physical health with MH/SA to ensure that persons with MH/SA problems receive appropriate and comparable quality of care to those who do not have these problems. 1,67,68 Also needed in these settings is sound knowledge of the larger network of services to make appropriate referrals and linkages with other nonmedical and medical specialist service providers. Improved knowledge and system-wide communication and coordination between general medical 45 and specialist services 55,69 would improve integration of services for people who have complex needs relating to MH or SA, especially co-occurring MH and SA disorders, 70,71 and thus may reduce system inefficiencies and the overall burden on the health system.
Footnotes
Author Note
The opinions, results, and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by the ICES or the Ontario MOHLTC is intended or should be inferred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Partnership for Health Systems Improvement Grant from the Canadian Institutes of Health Research (267416). This study was also supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC).